
Abstract
Poor relationship quality can increase an individual’s psychological distress. There is substantial debate regarding the influence of relationship quality for men and women. Some have found that women’s psychological distress is affected more by poor relationship quality compared to men. Others have found that psychological distress is equally affected for men and women, but it may look different—depressive symptoms for women and total alcohol consumption for men. In this study we examined how men and women differed in changes in relationship quality and changes in psychological distress. Then, we examined how changes in one manifestation of psychological distress and changes in relationship quality were related and how this association differed for men and women. Women reported lower initial relationship quality and total alcohol consumption but higher initial depressive symptoms. Men and women only differed on changes in total alcohol consumption, with women decreasing less than men over 25 years. Finally, both changes in total alcohol consumption and changes in depressive symptoms were related to changes in relationship quality for women, but not men. The reverse direction did not differ by gender, although change in depressive symptoms was related to change in relationship quality. Implications for future research are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Married individuals, compared to their nonmarried peers, tend to have greater mental health, longer life expectancy, and fewer reports of substance use (e.g., Proulx et al. 2007; Waite and Gallagher 2000; Umberson et al. 2006). Despite this prominent finding, it is also true that individuals in low quality relationships experience increased psychological distress compared to single individuals, divorced individuals, and individuals in higher quality relationships (Hawkins and Booth 2005). Therefore, it appears that the quality of one’s romantic relationship may be more influential on individual mental health rather than one’s relationship status.
Gender may moderate the association between relationship quality and psychological distress, with men benefiting more from marriage than women and women experiencing more psychological distress from lower quality relationships than men (Gove 1972). Most studies operationalized psychological distress as depression and critics argued that these studies examined gendered manifestations of psychological distress (e.g., Hill and Needham 2013). This perspective suggests that men and women similarly experience effects of low relationship quality through psychological distress; however, men manifest distress symptoms through behavior (e.g., alcohol consumption) whereas women manifest distress symptoms through internalization and affect (e.g., depression, anxiety; Williams 2003). Such a supposition tends to be better established theoretically than empirically as studies operationalizing psychological distress through gendered manifestations reported mixed findings (Pateraki and Roussi 2013). One possible explanation for these mixed findings is that research has yet to examine how change in total alcohol consumption and depression are influenced by change in relationship quality over time; that is, examining the association between dynamic rather than static variable measurements.
In longitudinal studies, relationship quality and psychological distress are typically measured statically whereby measures of relationship quality at one time point influence psychological distress at a later time point. Alternatively, if change is being measured, scholars have examined how a static measure of an independent variable at one time point influences change in a dependent variable (i.e., the slope). However, these static measures do not capture the natural change in an individual’s interpersonal and intrapersonal characteristics whereby change in one variable may influence similar or opposing change in another. What has yet to be examined in longitudinal studies of romantic relationships and mental health is how changes in relationships quality may influence changes in individual psychological distress. This study sought to examine how gender and change in relationship quality influence change in total alcohol consumption and depression simultaneously over a 25 year period using a series of latent growth curve models.
Gender and Psychological Distress
Gender and psychological distress both have socially constructed meanings, wherein that which is considered “feminine,” “masculine,” or “psychologically distressed” can change depending on context or over time depending on cohort. Also, the boundaries regarding behaviors that are considered to be “masculine” or “feminine” have blurred over the past century (Kite 2001). Therefore, examining the intersection of gender and mental health may be much like trying to examine a moving target as the meanings of each are continuously changing due to their socially constructed meanings.
As an interpersonal factor, psychological distress is difficult to directly measure and measurable manifestations of psychological distress must be assessed. When examining how psychological distress relates to romantic relationships, scholars have commonly defined it as depressive symptoms (e.g., Beach 2001; Whisman 2001). There are many critiques of the literature that focused on depression as a manifestation of psychological distress. These critiques suggest that depression is a gendered expression of psychological distress. When an individual experiences psychological distress, affective manifestations (e.g., depression, anxiety) are more socially acceptable for women whereas behavioral manifestations (e.g., antisocial behaviors, substance use) are more socially acceptable for men (Williams 2003). Supporting this argument, depression is more often diagnosed among women (Bruce and Kim 1992) whereas problematic total alcohol consumption is more common among men (Dawson et al. 2007). However, some scholars have found that men and women experience depression and total alcohol consumption to the same extent (Hill and Needham 2013). Among older couples, gender differences tend to be observed less frequently (Levenson et al. 1993) indicating that perhaps gendered expressions of psychological distress decrease with age. Taking into account these findings, this study focused on multiple manifestations of psychological distress (e.g., depression, total alcohol consumption) and how these manifestations may differ by gender.
Gender, Relationship Quality, and Psychological Distress
Research regarding the moderating influence gender has on the association between relationship quality and psychological distress have found mixed findings. Some of these mixed findings have been attributed to a possible cohort effect (Proulx et al. 2007) and differences between longitudinal and cross-sectional studies (Pateraki and Roussi 2013). Others have contended that studies operationalize psychological distress in accordance with a socially constructed bias towards women (i.e., depression), thus skewing the results toward findings that women experience more distress (Williams 2003). Therefore, it is important to understand the role of gender when examining relationship quality and psychological distress conceptualized as depressive symptoms or total alcohol consumption.
Depressive Symptoms
In a review of multiple cross-sectional studies, Gove (1972) found that women experienced more depression than men in marital relationships, but not in any other relationship form. This finding led Gove to conclude that men benefit from marriage more than women in terms of psychological distress and was among the first to examine how marital status and psychological distress may be moderated by gender. More recent meta-analytic studies have focused on relationship quality and found that the relationship between psychological distress and relationship quality are stronger for women compared to men (Proulx et al. 2007; Whisman 2001); that is, women’s psychological distress, compared to men, is affected more by the quality of the relationship. However, in both meta-analyses psychological distress was conceptualized as depression, neglecting more traditional masculine manifestations of psychological distress (e.g., total alcohol consumption). Christian et al. (1994) found that components of low marital quality influenced depression for both husbands and wives; however, gender moderated this relationship. Specifically, lower problem-solving abilities, increased partner aggression, unemployment, and lower spousal assertiveness were related to more depressive symptoms among women whereas only lower problem-solving abilities were related to depressive symptoms among men. Because these studies were cross-sectional, findings may reflect temporal disturbances in marital quality and not how consistent marital quality across time may influence individual psychological distress over time.
When examining the interaction of these factors longitudinally, there are inconsistent findings regarding gender as a moderator of the interaction of relationship quality and depression. Some studies have found no gender difference between relationship quality and depression over time (e.g., Hill and Needham 2013). Kurdek (1998) found that later in the relationship (four years of marriage) marital quality was linked to depressive symptoms for men but the opposite was true for women with depression symptoms being linked to marital quality. More specifically, men’s depression symptoms at Time 2 were influenced by Time 1 marital quality, whereas with women this path was not significant.
Overall, relationship quality is related to depression and this association is stronger for women than for men in cross-sectional studies. However, over time there is less consistency regarding the association between relationship quality and depression and whether this association differs by gender. It has been speculated that this longitudinal inconsistency might be due to spouses becoming less gendered in their expression of psychological distress over the course of their marriage (Levenson et al. 1993). Also, most studies examine the interaction of relationship quality and psychological distress over a period of less than five years (e.g., McNulty et al. 2008). Therefore, examining the association between relationship quality and psychological distress, specifically depression, over 10 or more years may better explain whether and how gender moderates this relationship over time.
Total Alcohol Consumption
When examining how gender moderates the association between relationship quality and psychological distress, it is important to consider gendered manifestations of psychological distress. Williams (2003) suggested that studies focusing on depression may incorrectly assert that marital quality affects women more than men because men tend to externalize psychological distress whereas women tend to internalize distress.
In general, problematic total alcohol consumption in romantic relationships is related to lower relationship quality (Leonard and Eiden 2007; Marshal 2003) and men tend to drink alcohol more frequently than women (Wilsnack et al. 2000). However, there is evidence that gender differences exist in the association between total alcohol consumption and relationship quality. In a longitudinal study, Cranford et al. (2011) found gender differences when considering the influence of an alcohol disorder on relationship quality. Specifically, in a dyadic analysis, men’s total alcohol consumption was not related to their own or their partner’s marital quality nine years later, but women’s total alcohol consumption was directly related to her and her partner’s later marital quality. Additionally, in daily reports, women tended to drink alcohol more than men after reporting relational difficulties (Levitt and Cooper 2010) Conversely, couples with an alcoholic wife reported higher relationship satisfaction compared to couples with an alcoholic husband (Noel et al. 1991) indicating that the gender of the individual with alcoholism may influence the romantic relationship differently. Taken together, it is unclear how change in total alcohol consumption in relation to change in relationship quality over time differs by gender.
Current Study
The association between relationship quality and psychological distress has been found consistently; as relationship quality decreases, psychological distress increases (Hawkins and Booth 2005; Pateraki and Roussi 2013; Proulx et al. 2007). However, there have been mixed findings as to whether this interaction is the same for both men and women in marital relationships, with some scholars finding differences (Proulx et al. 2007; Simon 2002) and others reporting no differences (Hill and Needham 2013). An absence of gender differences are more often found in longitudinal studies perhaps because cross-sectional studies are only capturing momentary fluctuations in marital quality and psychological distress. Also, absence of gender differences in longitudinal studies might be due to relationship duration, as older couples’ gender roles become less distinctive (Levenson et al. 1993). However, no study was found that simultaneously examined how gender influences changes in relationship quality and changes in manifestations of psychological distress. The present study sought to examine how gender influences change in these two constructs by testing:
-
a.
How is gender is related to changes in total alcohol consumption and relationship quality while controlling for depressive symptoms and initial total alcohol consumption and relationship quality?
-
b.
How is gender related to changes in depressive symptoms and relationship quality while controlling for total alcohol consumption and initial depressive symptoms and relationship quality?
As previously stated, there is some inconsistency as to how relationship quality influences psychological distress over time. Another possible explanation for these discrepancies is that psychological distress is most commonly measured as depressive symptoms (e.g., Beach 2001; Kurdek 1998; Whisman 2001) which is considered a socialized feminine manifestation of psychological distress and thus biasing these findings. Others have suggested that total alcohol consumption is a socialized masculine manifestation of psychological distress (Hill and Needham 2013; Williams 2003). Therefore, it is important to consider both manifestations of psychological distress to determine how changes in relationship quality may influence psychological distress. Although there are some studies that have examined manifestations of total alcohol consumption and depressive symptoms (Simon 2002), no studies were found that examined one manifestations of psychological distress while controlling for the other. The present study sought to further answer:
-
c.
How does gender moderate the association between changes in relationship quality and total alcohol consumption while controlling for depressive symptoms and initial relationship quality and total alcohol consumption?
-
d.
How does gender moderate the association between changes in relationship quality and depressive symptoms while controlling for total alcohol consumption and initial relationship quality and depressive symptoms?
Method
Procedures
The Americans’ Changing Lives (ACL) survey is an ongoing research project conducted by the University of Michigan, Institute for Social Research, Survey Research Center. The ACL consists of five waves of survey data collected over 30 years (Wave 1 [W1] = 1986; Wave 2 [W2] = 1989; Wave 3 [W3] = 1994; Wave 4 [W4] = 2002; Wave 5 [W5] = 2011). These data are part of a larger study that examines how a range of activities and social relationships influence individual productivity and how individuals adapt to stress and life events that could influence individual health and effective functioning. Data were collected through face-to-face survey interviews by trained interviewers (for more information see the project website: http://www.isr.umich.edu/acl/).
Participants
Participants from W1 of the ACL were sampled using a multistage stratified area probability of individuals ages 25 or older within the U.S. (N = 3617). African Americans and individuals over age 60 were over sampled at W1. For all subsequent waves an attempt was made to contact all respondents from previous waves: W2 = 2867, W3 = 2559, W4 = 1785, W5 = 1313. Most attrition was due to participant mortality rather than nonresponse. At W5, 46.3% of participants were considered “missing deceased” and 17.4% were considered “missing nonresponders.” Inclusion criteria for the current study limited participants to those who reported being married or in a romantic relationship at W1, which resulted in the removal of 42.9% of participants. The final sample included: W1 = 2066, W2 = 1693, W3 = 1586, W4 = 1183, and W5 = 1125.
Participants were mostly women (56.3%) with the majority reporting as White (72.3%), followed by Black (24.1%), and Native American, Asian, and Hispanic were approximately 1% each. At W1 participants were on average 52 years old (SD = 16.34, range = 25–92). Participants were married or partnered for an average of 27 years (SD = 17, range = < 1–67 years). Participants’ marital status ranged from 67.4% at W1 to 97.3% at W5 and those reporting as cohabiting ranged from 3.0% at W1 to 32.6% at W5. In waves 2–5, those who reported being divorced ranged from 5.4 to 12.1% respectively. Participants who reported being widowed ranged from < 1% in W1 to 22.8% in W5. On average, one child lived in the participant’s household and number of children ranged from 0 to 8 children across all waves.
Variables
Gender
Gender was assess at W1 and was coded as (0) Men and (1) Women.
Relationship Duration
Relationship duration was considered a time invariant variable and was assessed once at W1. This variable was included to control for relationship differences that may be accounted for by the length of the relationship. Assessment of relationship duration used two questions. First, married participants responded to the question: “For how many months or years have you been married to your partner?” Second, non-married participants living with their romantic partner responded to the question: “For how many months or years have you been living with your partner?” Responses were combined and coded as the total number of years together.
Children in the Home
This was a time invariant variable measured at W1. The number of children was assessed by the original data by adding “the number of children the individual has who live elsewhere” to “the number of children living inside the home.” “The number of children living elsewhere” was truncated at 8 children, so number of children at the high end of the range is not exact. Responses ranged from (0) no children to (8) 8 or more children.
Relationship Status
This variable was considered a time variant variable and was included in the model for every wave of data collection. This variable was assessed using a single item: “Are you currently married, separated, divorced, widowed, never married?” This item was recoded into four dichotomous variables: Married ([0] all else, [1] married); cohabiting ([0] all else, [1] cohabiting); divorced ([0] all else, [1] divorced); and widowed ([0] all else, [1] widowed).
Relationship Quality
This variable was measured using four items: (a) Marital satisfaction (“Taking all things together, how satisfied are you with your marriage/ relationship?”) with response options ranging from (0) Completely satisfied to (4) Not at all satisfied; (b) marital conflict (“How often would you say the two of you typically have unpleasant disagreements or conflicts?”) with response options ranging from (0) Daily or almost daily to (6) Never; (c) marital dissatisfaction (“Taking everything into consideration, how often do you feel bothered or upset by your marriage/relationship?”) with response options ranging from (0) Almost always to (4) Never; and (d) spousal support (“How much does your (husband/wife/partner) make you feel loved and cared for?”) with response options ranging from (0) A great deal to (4) Not at all. These items were assessed at all waves of data collection and recoded so that items were scaled in a similar manner, wherein higher scores indicated greater relationship quality. Scale reliability was acceptable for each wave of the study (W1: α = 0.76, W2: α = 0.79, W3: α = 0.78, W4: α = 0.77, W5: α = 0.80). Mean scores for relationship quality are presented in Table 1 by gender.
Depressive Symptoms
This variable was measured using an 11-item scale based on the Center for Epidemiologic Studies Depression (CESD; Radloff 1977) scale. Participants’ response options to items (e.g., “I felt sad” and “I felt that people disliked me”) ranged from (0) Never or hardly ever to (3) Most of the time. Scale reliability was acceptable for each wave of the study (W1: α = 0.81, W2: α = 0.82, W3: α = 0.83, W4: α = 0.81, W5: α = 0.85). All items were summed to create a single score where higher scores indicated greater depressive symptoms. This measure was assessed during every wave of the study. Mean scores for depressive symptoms for each wave were are presented in Table 1 by gender.
Total Alcohol Consumption
This variable was measured using three items developed and calculated by the ACL team: (a) “Do you typically drink alcohol?” (0 = No, 1 = Yes), (b) “During the last month, on how many days did you drink?” ([0] none to [31] 31 days), and (c) “On days that you drink, how many cans of beer, glasses of wine, or drinks of liquor do you usually have?” ([0] 0 drinks to [20] 20 drinks). The ACL team combined the items by multiplying these questions together to produce number of drinks per month. Number of drinks per month had a possible range of 0–600. This final count item was recoded into bins of 10 drinks so that scores ranged from (1) 1 to 10 drinks to (20) 200+ drinks. Scores of 200+ drinks were recoded into bins of 100 drinks so that 201 to 300 drinks are coded as 21. This item was assessed at every wave. The average drinks are in Table 1 by gender; the median number of drinks reported at each month were: W1: Median = 4 drinks (men), 0 drinks (women), W2: Median = 2 drinks (men), 0 drinks (women), W3: Median = 3 drinks (men), 0 drinks (women), W4: Median = 1 drink (men), 0 drinks (women), and W5: Median = 0 drinks (men), 0 drinks (women).
Analytic Strategy
Latent Growth Curve Modeling (LGCM) was used to assess how relationship quality, depressive symptoms, and total alcohol consumption changed over time, and how these relationships were moderated by gender (McArdle and Hamagami 1992). These models assessed for change in two constructs simultaneously and controlled for the mutual influence of each construct. Analyses for these models were conducted using Mplus (Muthén and Muthén 1998–2012). To assess model fit for the LGCM, the comparative fit index (CFI), the Tucker-Lewis index (TLI), and the root mean square of error approximation (RMSEA) were evaluated if the χ2 test was significant. A model was determined to be of adequate fit to the data if the χ2 value was small and non-significant, the CFI and TLI values were > 0.95, and the RMSEA was < 0.05 (Kline 2011).
All analyses were conducted in Mplus using TYPE = COMPLEX. The TYPE = COMPLEX accounts for stratification, clustering, and sampling weights, all of which were developed by the ACL (House 2014) and used in these analyses. This approach utilized these sampling features to compute standard errors and χ2 tests of model fit. To examine gender as a moderator, a grouping variable was used and a series of Wald χ2 fit tests were conducted to determine if constraining the model to be equal on a single path for men and women significantly improved the model-data fit. Wald χ2 difference tests were conducted within Mplus using the DIFFTEST function (Muthén and Muthén 1998–2012). A significant test (p < .05) indicates that men and women differed on the tested path.
Results
Initial Statistical Analyses
All analyses were completed using Mplus 7.0 (Muthén and Muthén 1998–2012). Missing values were handled using full information maximum likelihood estimation (FIMLE), which assumes that data are missing at random. When the covariates related to the missing pattern are included in the model, FIMLE produces less biased and more reliable parameter estimates compared to conventional methods (e.g., list-wise deletion, multiple imputation; Allison 2003). Type of missing (i.e., missing nonresponders and missing deceased) differed on key demographic variables (e.g., socioeconomic status, race/ethnicity, age). Therefore, a series of t tests and χ2 tests were conducted to determine the demographic variables related to missingness. Statistically significant variables were included in the final models to help explain data patterns missing at random with full information maximum likelihood in Mplus. A few of the control variables were correlated with other variables of interest. Results of the correlation analyses ranged from r = − .48 to .43 across the five waves examined. Control variables were included in the model as missing auxiliary (AUXILIARY = (m) ×) variables to reduce bias in estimated parameters and dealing with missingness (Muthén and Muthén 1998–2012).
The primary statistical assumption for path analysis is normal distribution as problems with dependence, multicollinearity, or equality of variance are handled by this statistical method. Skewness and kurtosis are reported in Table 1 for all variables of interest. The distribution of total alcohol consumption was highly skewed and kurtotic; therefore, due to limitations in the statistical software, these variables were run using MLR, which can better estimate non-normality compared to the maximum likelihood estimator. In some waves, the depressive symptoms variable was slightly skewed and kurtotic; thus, caution is warranted when interpreting these variables as normally distributed. Bivariate correlations were also examined for men and women and presented in Table 2. For men and women, relationship quality was related to depressive symptoms at every wave of data collection but only some waves for alcohol. Similarly, depressive symptoms was only sometimes correlated with alcohol consumption.
How Is Gender Related to Change?
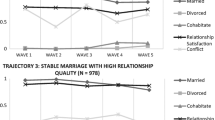
The first aim of the present study was to determine how gender was related to changes in total alcohol consumption and relationship quality while controlling for depressive symptoms, initial total alcohol consumption, and relationship quality. Using latent growth curve modeling across the five study waves we first examined changes in total alcohol consumption and relationship quality when controlling for depressive symptoms. The model-data fit was acceptable: χ2(44) = 128.97, p = 1.85; CFI = 0.98; TLI = 0.98; RMSEA = 0.034 [95% CI = 0.027–041]. In Table 3, model results are presented, including unstandardized slopes and intercepts of total alcohol consumption and relationship quality along with unstandardized regression coefficients and effect sizes for gender. Additionally, changes in relationship quality and total alcohol consumption for men and women are reported. Further, we sought to examine how gender was related to changes in depressive symptoms and relationship quality while controlling for total alcohol consumption, initial depressive symptoms, and relationship quality. The model-data fit was acceptable: χ2(44) = 215.35, p = 1.39; CFI = 0.96; TLI = 0.95; RMSEA = 0.048 [95% CI = 0.042–0.054]. In Table 3, model results are presented, including unstandardized slopes and intercepts of depressive symptoms and relationship quality, covariances among the slopes and intercepts, and unstandardized regression coefficients and effect sizes for gender. Changes in relationship quality and depressive symptoms for men and women are shown in Fig. 1.

Depiction of change in relationship quality, alcohol use, and depression for men and women across the five study waves
Gender as a Moderator?
The third aim of the present study sought to identify if gender moderated the association between changes in relationship quality and total alcohol consumption while controlling for depressive symptoms, initial relationship quality, and total alcohol consumption. To examine this, we used gender as a grouping variable and Wald χ2 difference tests to examine if the paths between psychological distress and relationship quality were different for men and women. First, we examined total alcohol consumption, and the model-data fit was acceptable: χ2(83) = 200.14, p = .10 RMSEA = 0.041 [95% CI = 0.034–0.048]. The Wald test of parameter constraints indicated that men and women did not differ on the influence of changes in relationship quality on changes in total alcohol consumption [χ2(1) = 1.28, p = .26] and this path was not significant for either gender (B = 0.001, p = .98). However, the reverse was not true. That is, men and women did differ on the influence of changes in total alcohol consumption on changes in relationship quality [χ2(1) = 2.79, p = .09]. For women, the influence of changes in total alcohol consumption trended toward being negatively related to change in relationship quality (B = − 0.14; p = .09). However, for men, changes in total alcohol consumption did not influence changes in relationship quality (B = − 0.001; p = .89).
Lastly, the present study sought to determine if gender moderated the association between changes in relationship quality and depressive symptoms while controlling for total alcohol consumption, initial relationship quality, and depressive symptoms. The model-data fit was acceptable: χ2(79) = 222.31, p = 1.45 with a non-significant statistic indicating we could not reject the null hypothesis that the data fit the model. The Wald test of parameter constraints indicated that men and women did not differ on the influence of changes in relationship quality on changes in depressive symptoms [χ2 (1) = 1.84, p = .17) and the path for both was significant (B = − 3.35, p < .001). However, the influence of changes in depressive symptoms on changes in relationship quality did differ for men and women [χ2(1) = 4.67, p = .03). For men, influence of changes in depressive symptoms on changes on relationship quality was not significant (B = − 0.03, p = .32) but for women this relationship was significant (B = − 0.15, p < .05). This finding indicated that for women, changes in depressive symptoms over time can affect changes in relationship quality, but changes in relationship quality does not affect changes in depressive symptoms for men or women.
Discussion
Individuals in low quality relationships tend to report greater psychological distress compared to their single or happily married peers (Hawkins and Booth 2005). According to Proulx et al. (2007), it is critical to examine how psychological distress and relationship quality change over time and how gender may moderate that change. Scholars have also found that women tend to experience more psychological distress from poor relationship quality than their male partners (Gove 1972). However, critics have countered that depressive symptoms, a female gendered manifestation of psychological distress, is often used to measure psychological distress rather than a male gendered manifestation of psychological distress (e.g., total alcohol consumption; Hill and Needham 2013). Further complicating matters, it appears that marital quality may follow a linear decline over time; however, individual well-being waxes and wanes depending on contextual and emotional changes (Davila et al. 2003; Kurdek 1998). To begin to tease apart this complex relationship, we examined two models to examine: (a) how gender was related to changes in relationship quality and depressive symptoms while controlling for total alcohol consumption and (b) how gender was related to changes in relationship quality and total alcohol consumption while controlling for depressive symptoms.
When examining if total alcohol consumption was a manifestation of psychological distress, gender was significantly related to relationship quality at W1 but not related to changes in relationship quality across the five waves. Women tended to report lower relationship quality at W1 compared to men, but men and women changed similarly in relationship quality over time. Women reported less total alcohol consumption at W1 but decreased in total alcohol consumption more slowly than men over time. Despite this slower decline, women’s total alcohol consumption remained constantly lower than men’s across all five time points. The model examining depressive symptoms as a manifestation of psychological distress indicated that gender was significantly related to relationship quality and depressive symptoms at W1 but not to change in the two variables across the 25 year period. Although men and women differed in their initial reports of relationship quality and depressive symptoms, they changed at the same rates in both variables. These findings are consistent with previous studies in that relationship quality appears to decline in a linear fashion (Davila et al. 2003) and some have found that relationship satisfaction does differ by gender, with women reporting lower relationship satisfaction (Proulx et al. 2007). However, this study advances the understanding of changes in relationship quality and psychological well-being by indicating that men and women do not differ in their declines in relationship satisfaction or depressive symptoms over time.
Next, this study examined how gender moderated the relationship between changes in psychological distress and changes in relationship quality. For women, changes in total alcohol consumption and changes in depressive symptoms were negatively related to changes in relationship quality, but this pattern was not found for men. For both men and women changes in relationship quality was negatively related to changes in depressive symptoms in the same magnitude of influence. Meaning, for women, but not for men, changes in psychological distress can influence changes in their reports of relationship quality. As one’s psychological distress can be influenced by many contextual factors (e.g., work stress, parenting demands, and social network strain), for women, changes in relationship quality may be sensitive to dyadic as well as contextual stressors. However, for men and women changes in relationship quality was related to changes in depressive symptoms as previously found by other scholars (e.g., Beach 2001). This finding indicates that both men and women are susceptible to the negative effects of poor relationship quality; however, changes in a woman’s relationship quality may be susceptible to individual, dyadic, and contextual factors.
There have been mixed results on the influence of relationship quality and psychological distress, wherein some studies reported gender differences (Proulx et al. 2007) and others did not (Hill and Needham 2013). Scholars have posited that gender differences are due to men and women expressing their psychological distress differently. Although these findings dispute the gendered manifestations of psychological distress assertion in that women’s depressive symptoms and total alcohol consumption were related to changes in relationship quality, but not for men, it does lend support to other scholars’ (e.g., Pateraki and Roussi 2013) findings that relationship quality and psychological distress are more strongly related to relationship quality for women than for men.
Limitations
Although this study has a number of strengths, it is important to consider the limitations that warrant caution when interpreting these findings. First, although an attempt was made to reduce bias in the non-normality of total alcohol consumption, caution should be taken when interpreting the results of the LGCM and gender as a moderator. Further, the majority of the participants reported high relationship quality and low total alcohol consumption (ceiling and floor effects). Although these reports could be due to the face-to-face interviews and participants’ social desirability bias, these results may not be generalizable to individuals who report marital distress, or high alcohol consumption. Additionally, it is important to consider the average age of the sample at W1 was quite high (M = 52 years) and the findings may not be relevant to younger married individuals or younger cohorts. Finally, there were few Latino individuals included in the study; therefore, caution should be taken when generalizing findings to Latino populations.
Future Research and Implications
For practitioners working with couples or individuals with relational concerns, it seems that changes in women’s psychological distress may influence changes in their perceived relationship quality. This may be an indication of the efficacy of some cognitive behavioral therapies (CBT; see Beck 2011), which focus on thought processes before changing behavioral patterns for individuals experiencing relational and psychological distress. Further, these findings begin breaking down the assumptions of some therapeutic models such as the marital discord model, which states that marital quality influences change in depression (Beach et al. 1990). For men there appears to be other factors that influence change in relationship quality and psychological distress. Further investigation is recommended before disregarding these therapeutic models.
As mentioned earlier, gender differences tend to be observed less frequently among older couples (Levenson et al. 1993). Perhaps gendered expressions of psychological distress decrease with age. Although it is beyond the scope of the present study, future research may benefit from examining age as a moderator of the gender effects found in the present study.
It is well known that relationship quality is an important correlate with psychological distress, above and beyond relationship status. As relationship quality is a variable amenable to change, perhaps psychological distress can indirectly benefit from changes in relationship quality. Recently implemented two-session brief interventions working with moderately happy couples, like the individuals in this study, have shown improvements in individual well-being, relationship quality, and parenting confidence in follow-up surveys (Gordon et al. 2014). Brief interventions such as these should be considered because the focus is placed on improving relationship health as a means of indirectly improving individual and child well-being.
References
Allison, P. D. (2003). Missing data techniques for structural equation modeling. Journal of Abnormal Psychology, 112(4), 545–557. https://doi.org/10.1037/0021-843x.112.4.545.
Beach, S. R. H. (2001). Marital and family processes in depression: A scientific foundation for clinical practice. Washington, DC: American Psychological Association.
Beach, S. R. H., Sandeen, E. E., & O’Leary, K. D. (1990). Depression in marriage: A model for aetiology and treatment. New York, NY: The Guilford Press.
Beck, J. S. (2011). Cognitive behavior therapy: Basics and beyond. New York: Guilford Press.
Bruce, M. L., & Kim, K. M. (1992). Differences in the effects of divorce on major depression in men and women. The American Journal of Psychiatry, 149, 914–917. http://psycnet.apa.org/psycinfo/1992-43181-001.
Christian, J. L., O’Leary, K. D., & Vivian, D. (1994). Depressive symptomatology in maritally discordant women and men: The role of individual and relationship variables. Journal of Family Psychology, 8, 32–42. https://doi.org/10.1037/0893-3200.8.1.32.
Cranford, J. A., Floyd, F. J., Schulenberg, J. E., & Zucker, R. A. (2011). Husbands’ and wives’ total alcohol consumption disorders and marital interactions as longitudinal predictors of for a stress generation model. Journal of Personality and Social Psychology, 73, 849–861. https://doi.org/10.1037/0022-3514.73.4.849.
Dawson, D. A., Grant, B. F., Chou, S. P., & Stinson, F. S. (2007). The impact of partner alcohol problems on women’s physical and mental health. Journal of Studies on Alcohol and Drugs, 68, 66–75. http://psycnet.apa.org/psycinfo/2006-23097-009.
Davila, J., Karney, B. R., Hall, T. W., & Bradbury, T. N. (2003). Depressive symptoms and marital satisfaction: Within-subject associations and the moderating effects of gender and neuroticism. Journal of Family Psychology, 17, 557–570. https://doi.org/10.1037/0893-3200.17.4.557.
Gordon, K. C., Kasting, A., Wischkaemper, M., Hawrilenko, K., Roberson, M., Gray, P. N. E., T., & Cordova, J. (2014). Strengthening relationships through a two-session community intervention. Poster presented at the Administration for Children and Families Grantee Showcase in Washington, D.C.
Gove, W. R. (1972). The relationship between sex roles, marital status, and mental illness. Social Forces, 51, 34–44. https://doi.org/10.1093/sf/51.1.34.
Hawkins, D. N., & Booth, A. (2005). Unhappily ever after: Effects of long-term, low-quality marriages on well-being. Social Forces, 84, 451–471. https://doi.org/10.1353/sof.2005.0103.
Hill, T. D., & Needham, B. L. (2013). Rethinking gender and mental health: A critical analysis of three propositions. Social Science & Medicine, 92, 83–91. https://doi.org/10.1016/j.socscimed.2013.05.025.
House, J. S. (2014). Americans’ Changing Lives: Waves I, II, III, IV. and V, 1986, 1989, 1994, 2002, and 2011. Inter-university consortium for political and social research. Ann Arbor, MI. https://doi.org/10.3886/ICPSR04690.v7.
Kite, M. E. (2001). Changing times, changing gender roles: Who do we want women and men to be? In R. K. Unger (Ed.), Handbook of the psychology of women and gender (pp. 215–227). Hoboken, NJ: Wiley.
Kline, R. B. (2011). Principles and practice of structural equation modelling. New York, NY: Guilford Press.
Kurdek, L. A. (1998). Relationship outcomes and their predictors: Longitudinal evidence from heterosexual married, gay cohabiting, and lesbian cohabiting couples. Journal of Marriage and the Family, 60, 553–568. https://doi.org/10.2307/353528.
Leonard, K. E., & Eiden, R. D. (2007). Marital and family processes in the context of total alcohol consumption and alcohol disorders. Annual Review of Clinical Psychology, 3, 285–310. https://doi.org/10.1146/annurev.clinpsy.3.022806.091424.
Levenson, R. W., Carstensen, L. L., & Gottman, J. M. (1993). Long-term marriage: Age, gender, and satisfaction. Psychology and Aging, 8, 301–313. https://doi.org/10.1037/0882-7974.8.2.301.
Levitt, A., & Cooper, M. L. (2010). Daily total alcohol consumption and romantic relationship functioning: Evidence of bidirectional, gender-, and context-specific effects. Personality and Social Psychology Bulletin, 36(12), 1706–1722.
Marshal, M. P. (2003). For better or for worse? The effects of total alcohol consumption on marital functioning. Clinical Psychology Review, 23(7), 959–997.
McArdle, J. J., & Hamagami, F. (1992). Modeling incomplete longitudinal and cross-sectional data using latent growth structural models. Experimental Aging Research, 18, 145–166. https://doi.org/10.1080/03610739208253917.
McNulty, J. K., O’Mara, E. M., & Karney, B. R. (2008). Benevolent cognitions as a strategy of relationship maintenance: “Don’t sweat the small stuff"… But it is not all small stuff. Journal of Personality and Social Psychology, 94, 631–646. https://doi.org/10.1037/0022-3514.94.4.631.
Muthén, L. K., & Muthén, B. O. (1998–2012). Mplus User’s Guide. Seventh Edition. Los Angeles: Muthén & Muthén.
Noel, N. E., McCrady, B. S., Stout, R. L., & Fisher-Nelson, H. (1991). Gender differences in marital functioning of male and female alcoholics. Family Dynamics of Addiction Quarterly, 1, 31–38.
Pateraki, E., & Roussi, P. (2013). Marital quality and well-being: The role of gender, marital duration, social support and cultural context. A Positive Psychology Perspective on Quality of Life: Social Indicators Research Series, 51, 125–145. https://doi.org/10.1007/978-94-007-4963-4_8.
Proulx, C. M., Helms, H. M., & Buehler, C. (2007). Marital quality and personal well-being: A meta-analysis. Journal of Marriage and Family, 69, 576–593. https://doi.org/10.1111/j.1741-3737.2007.00393.x.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401.
Simon, R. W. (2002). Revisiting the relationships among gender, marital status, and mental health. American Journal of Sociology, 107, 1065–1096. https://doi.org/10.1086/339225.
Umberson, D., Williams, K., Powers, D. A., Liu, H., & Needham, B. (2006). You make me sick: Marital quality and health over the life course. Journal of Health and Social Behavior, 47, 1–16.
Waite, L. J., & Gallagher, M. (2000). The case for marriage: Why married people are happier, healthier and better off financially. New York: Doubleday.
Whisman, M. A. (2001). The association between depression adn marital dissatisfaction. In S. R. H. Beach (Ed.), Marital and family processes in depression: A scientific foundation for clinical practice (pp. 3–24). Washington, DC: American Psychological Association.
Williams, K. (2003). Has the future of marriage arrived? A contemporary examination of gender, marriage, and psychological well-being. Journal of Health and Social Behavior, 44, 470–487. https://doi.org/10.2307/1519794.
Wilsnack, R. W., Vogeltanz, N. D., Wilsnack, S. C., & Harris, T. R. (2000). Gender differences in total alcohol consumption and adverse drinking consequences: Cross-cultural patterns. Addiction, 95(2), 251–265.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Roberson, P.N.E., Lenger, K.A. & Olmstead, S.B. Examining How Romantic Relationship Quality Influences Individual Psychological Distress Over Time for Men and Women. J Adult Dev 25, 259–269 (2018). https://doi.org/10.1007/s10804-018-9290-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10804-018-9290-4