
Abstract
There is a dearth of research that focuses on social intervention efforts for adults on the autism spectrum with intellectual disability and limited conversational language. Using a multiple baseline experimental design, this pilot investigation of the Socialization Knowledge for Individuals with Limited Language (SKILL) program evaluated a novel peer-facilitated group program specifically designed to target social interaction skills for this population. Findings from five pilot participants yielded evidence of social improvements across specific verbal skills (on-topic conversational contributions and responses) and nonverbal behaviors (eye-contact, active listening), as evidenced by coded social conversation probes and parent-report measures. These findings demonstrate the promise of a socialization intervention for a population that has historically been neglected in the social intervention research literature.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Adults on the autism spectrum with co-occurring intellectual disability (ID) are critically underrepresented in the autism intervention literature (Siegel 2018). Adults with ID have only been included in approximately 6% of published studies (Russell et al. 2019) yet are estimated to represent 30–40% of all individuals on the autism spectrum (Maenner 2020). This exclusion neglects a sizable portion of the autism population in need of targeted intervention and support (Shattuck et al. 2012; Stedman et al. 2019; Totsika et al. 2010).
In spite of the growing recognition of the importance of social skill training for autisticFootnote 1 individuals at all levels of intellectual functioning, very few autistic adults with ID have regular access to evidence-based programs that target specific social competencies and promote continued social development into adulthood (Dudley et al. 2019; Gotham et al. 2015). This lack of programming that provides engaging social interactions, goal-setting, and opportunities for social-emotional growth may be associated with emotional and behavioral challenges over time (Duncan et al. 1999; Matson and Shoemaker, 2009; Taylor et al. 2015) and poorer life outcomes (Howlin et al. 2004; Shattuck et al. 2012). Social skill interventions for this population should address the unique learning considerations of individuals severely affected in both cognitive and language domains (Stedman et al. 2019), while including effective components to foster measurable skill acquisition, increased quality of life, and meaningful relationships in supported living or employment contexts (Walsh et al. 2019).
Promoting Social Functioning
To facilitate meaningful and relevant social gains, a growing body of evidence suggests that psychosocial interventions for autistic adults must target a broad array of demonstrable social competencies (Pallathra et al. 2018). These social competencies may include verbal and nonverbal strategies that convey social interest and sustain an interaction, along with skills to recognize emotions and respond appropriately (Mazefsky et al. 2013; Walton and Ingersoll, 2013). The existing intervention literature provides several promising strategies for targeting and improving social functioning in adults on the autism spectrum, including socially motivating programming, experiential learning, and visual learning strategies. A multi-faceted program that combines these key elements may promote social skill development for autistic adults with ID and limited conversational language:
Motivation
To develop a context conducive to learning new social behaviors, social motivation is a crucial programmatic consideration. Social motivation is linked to a willingness to engage with others in the context of social learning activities, which in turn determines the effectiveness of the delivered lesson and associated rate of skill acquisition (Pallathra et al. 2018; Vernon et al. 2018). There is existing evidence in the child-focused autism literature that socially motivating activities promote language and social development within the context of intervention efforts (e.g., DiStefano et al. 2016; Ingersoll and Wainer 2013; Vernon et al. 2019). Specific motivational strategies that are associated with these gains include the use of experiential learning activities, thematic interests, visual aids, and supportive group contexts that incorporate both social instruction and practice with same-aged peers (Barry et al. 2003; Gates et al. 2017; Harrop et al. 2019; Pallathra et al. 2019). Among autistic adults with co-occurring ID, a motivating group socialization context may promote the development of social communication and interaction skills (Walsh et al. 2018).
Experiential Learning
Past research supports the positive benefits of a hands-on, experiential learning (a “learn by doing” approach) to promote social communication gains for autistic adults with co-occurring ID (Carminati et al. 2007; Ryan et al. 2019; Walsh et al. 2018, 2019). In an experiential learning context, competencies are acquired through immersion in a natural or quasi-natural social learning context (e.g., engagement with peers) and subsequent feedback on one’s performance. This model is conceptualized to enhance a didactic learning setting in which skills are formally taught through structured lessons. As one example, Ryan and colleagues (2019) demonstrated the efficacy of behavioral skills training in increasing appropriate nonverbal conversation skills for six autistic adults with co-occurring ID using live modeling, practice, and in vivo feedback.
Peer-Mediated Intervention (PMI)
In an experiential learning context, the use of same-aged, typically-developing peer facilitators has been demonstrated to facilitate social interaction gains through instruction, modeling, and therapeutic encouragement during group sessions (Chang and Locke 2016; Płatos and Wojaczek 2018; Vernon et al. 2018). Recent research found that PMI improved the social skill generalization outcomes of a video-based group intervention for four autistic adolescents with ID (Stauch et al. 2018). The addition of PMI may have enhanced social skill gains by providing individualized learning experiences in the context of a standardized intervention curriculum. When peers are assigned to a single participant for the duration of treatment, they may tailor their approach to the participant’s learning needs by modifying their tone, affect, language, or speech rate, for instance (Dyson et al. 2019). The familiarity and comfort with a peer facilitator may also enhance social motivation (Thompson et al. 2020).
Visual and Video-Based Learning
To further engage participants and build social motivation, visual modeling provides a concrete, dynamic representation of target social skills. For autistic adults, visual learning is often a relative strength (Corbett and Abdullah 2005). There is growing evidence that video modeling is effective for teaching social communication skills and facilitates skill acquisition and maintenance (Hume et al. 2009). For autistic adults with co-occurring ID, video-modeling has been used to improve social perception skills (Stauch et al. 2018) and to enhance social behaviors in a vocational setting (Walsh et al. 2018). Similarly, autistic adolescents and adults with ID demonstrated improvements in social ability, engagement, and functional communication following the TEACCH program, which relies heavily on visual modeling (Siaperas and Beadle-Brown 2006). These benefits may be enhanced by using visual checklists in a video modeling context to promote generalization of social skills (Spriggs et al. 2015).
Current Study
The Socialization Knowledge for Individuals with Limited Language (SKILL) Program is a group intervention designed to target social competencies in autistic adults with co-occurring ID and limited functional language. The SKILL Program combines motivational, experiential, peer-mediated, and visual components into a single intervention model that has been specifically designed for this population.
The primary aim of this investigation was to explore the feasibility, acceptability, and preliminary efficacy of the SKILL Program. We hypothesized that the program elements would lead to favorable indications of treatment acceptability. It was also hypothesized that participants’ trajectories of social skill use would improve over time, as assessed by analysis of filmed social conversations and parent-report standardized survey measures. Given the complex developmental profiles of this under studied population, targeted treatment efforts were used to address both global and participant-specific verbal and nonverbal competencies associated with social functioning. Specifically, it was anticipated that all participants would improve in their use of on-topic (contextually appropriate) verbal contributions to an unfolding social conversation (the primary behavior of interest). Additionally, it was anticipated that individuals would improve in specific social competencies identified as a primary concern for each person, which spanned verbal (conversational contributions) and non-verbal (active listening and eye-contact) skill domains. For adults who received social communication interventions throughout their childhood, the ultimate goal of this trial was to demonstrate that a continued focus on social interaction practice and goal-setting is valuable to families and can yield meaningful social improvements over time.
Method
Participants
Participants were recruited via targeted social media advertisements and emails to autism center mailing lists. Inclusion criteria included: (a) verification of ID (FSIQ < 70), (b) limited language use (receptive and expressive vocabulary standard scores < 70; confirmation of limited fluent language use in conversation probes, defined as a lack of full sentence language use or near-exclusive use of highly scripted/perseverative language); (c) at least some use of multiple-word phrase speech (i.e. not completely nonverbal); (d) confirmation of Autism Spectrum Disorder (ASD) diagnosis based on existing records. The mean age of the five participants was 21.0 years (SD = 3.2) and all were male (See Table 1 for more detailed demographic information and a summary of each participant’s observed language use).
Research Design
A concurrent multiple baseline across participants design was used to examine the preliminary efficacy of the 10-week group SKILL program. Since participants were not receiving interventions targeting key SKILL social interaction domains at the time of recruitment, they were assigned to one of three baseline conditions within a single intake session. Participants completed two, four, or six baseline unstructured social interaction probes (described in Measures) at intake prior to the start of the program. These videotaped naturalistic social interaction samples were collected for all participants at intake (2, 4, or 6 conversations), every 2 weeks before the group SKILL session (2 conversations), and post-intervention (2 conversations). This project received Institutional Review Board (IRB) approval and was conducted at a North American university.
Procedure
Social Facilitator Recruitment and Training
University undergraduate students (86.3% self-identified female) were recruited to serve as social facilitators for the SKILL program. These facilitators received a 5-h initial training on working with autistic adults with co-occurring ID, basic group facilitation skills, and goals of the pilot program. The social facilitators also participated in weekly 1-h supervision meetings for ongoing clinical supervision and discussion of the curriculum. A clinical psychology doctoral student and licensed clinical psychologist jointly conducted all training sessions and oversaw all weekly group treatment sessions.
Participant Screening
A phone screen was conducted with the participant’s parent to determine initial eligibility, followed by in-person eligibility assessments with the parent and participant at intake. The phone screen questions were standardized to provide initial verification of limited language use (e.g., mean length of utterances, spontaneous vs. prompted language use).
Intake Sessions
Each participant completed a single intake session which consisted of: (a) obtaining informed consent from legal guardians and assent from each dependent adult; (b) completing 2, 4, or 6 filmed unstructured social interaction probes with different typically-developing peers to obtain authentic first encounters; (c) completing one filmed standardized social interaction probe; (d) completing a standardized cognitive assessment; (e) completing standardized language assessments. During this time, parents completed survey measures and, in conjunction with their designated peer facilitators, identified a primary social goal related to one of the key intervention domains to serve as their child’s social interaction skill target.
Participant Characterization Measures
Cognitive Ability
The Kaufman Brief Intelligence Test, Second Edition (KBIT-2) provides measures of verbal and nonverbal intelligence and a composite IQ score (Kaufman, 1990). The KBIT-2 was used in the current study to provide confirmation of existing records of IQ < 70 for all participants.
Autism Symptomatology
In addition to confirmation of ASD diagnoses with existing records, parents completed a questionnaire to provide additional information about autism symptoms and social functioning in daily life. The Social Responsiveness Scale, Second Edition, Informant Report (SRS-2A; Constantino and Gruber 2012) is a 65-item informant-report rating scale with a high internal consistency (alpha) of 0.90-0.95 that measures reciprocal social behavior, social use of language, and other behaviors characteristic of ASD as they occur in natural social settings.
Adaptive Functioning
The Parent/ Caregiver rating form of the Vineland Adaptive Behavior Scales, Third Edition (Vineland-3; Sparrow et al. 2016) provides an Adaptive Behavior Composite score comprised of standard scores across three domains: daily living, communication, and socialization adaptive domains. The Vineland-3 has shown high internal consistency of 0.90-0.98 for the comprehensive rating form (Spriggs et al. 2015).
Receptive Vocabulary
Receptive vocabulary skills were assessed using the Peabody Picture Vocabulary Test, 5th Edition (PPVT-5). The PPVT-5 is an individually administered assessment of receptive language that contributes useful information for identifying and quantifying language ability. The PPVT-5 has shown high internal consistency (0.96–0.97) and test–retest reliability (corrected r = 0.84) for adults in the 18–25 age range (Williams and Williams 2007). Research supports the utility of the PPVT as a proxy for verbal IQ across individuals with ASD of varying ages and cognitive abilities (Krasileva et al. 2017).
Expressive Vocabulary
Expressive vocabulary skills were assessed using the Expressive Vocabulary Test, Third Edition (EVT-3). The EVT-3 is an individually administered assessment of expressive language and word retrieval in which individuals are presented with drawings depicting a range of content areas and parts of speech. The EVT-3 has shown high internal consistency (0.95-0.97) and test–retest reliability (corrected r = 0.90) for adults in the 18–25 age range (Dunn and Dunn 2007). Both the PPVT-5 and the EVT-3 have been shown to discriminate between typically developing individuals and those with ASD (Dunn and Dunn 2007; Williams and Williams 2007).
Social Conversation Data Collection
Unstructured Social Interaction Probes
Live peer interaction may be the most direct means to observe and code the use of behaviors associated with social competence and success (Ko et al. 2019). To examine individual trajectories of social skill use, participants completed 3-min unstandardized, “get-to-know-you” conversations with young adult peers at intake, every 2 weeks before the weekly treatment sessions, and post-treatment. In order to obtain an authentic first social encounter, these typically-developing peers were untrained, uncoached, and unaware of the project aims or hypotheses. Additionally, novel sets of typically-developing peers were recruited for unstructured conversations at each time point. Participants engaged in separate conversations with an equal number of unfamiliar males and females in a quiet room at each time point.
Standardized Social Interaction Probes
Once at intake and once post-treatment, participants also engaged in a standardized conversation (3–5 min) with the same trained typically-developing peer who was not involved in design or implementation of the treatment. This peer used a standardized script in order to specifically elicit certain social initiations and responses to open-ended questions and leading statements. This conversation procedure was developed by the research team to serve as a standardized counterpart to the unstructured conversation samples (see Ratto et al. 2011 for an analogous structured conversation outcome measure).
SKILL Program Overview
The SKILL program consisted of 10 weekly 90-min sessions that followed an established curriculum based on empirically-based strategies for social interaction skill acquisition, mastery, and generalization (Table 2). While all participants completed the same group curriculum, peer facilitators incorporated individualized social skill practice in the key intervention domains (conversational contributions, active listening, eye-contact) for each participant (in a format similar to the START program described in Vernon et al. 2018).
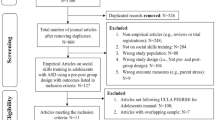
Each session consisted of an individual check-in session, group socialization time, interactive social skill practice, a social activity, a second social skill practice, and an individual check-out session (Fig. 1). The SKILL program model valued experiential learning through instruction, modeling, rehearsal, and feedback in each session (Leaf et al. 2015). Weekly homework assignments were given to the parent and participant to encourage continued practice and generalization of skills to the home or community environments.

SKILL program weekly session timeline
Session Materials
Each week, peer facilitators used a visual schedule and visual checklists to depict the structure and goals of each session. Existing research supports the use of participant interests in intervention efforts (Harrop et al. 2019), and the visual checklists were individualized to include motivating thematic interests (e.g., a picture of a favorite cartoon character to attract participant interest).
SKILL Program Weekly Session Format
Individual Check-In Session (10 min)
Parents and participants first completed an individual check-in session with their designated peer facilitator. Given that parent training is a fundamental component of comprehensive intervention (National Research Council 2009), this time was allotted to provide an opportunity for the peer facilitator to provide psychoeducation on social skill goals, review the participant’s homework, discuss social successes and challenges, and address questions and concerns. Each family also discussed progress regarding their individual social skill goals. Lastly, facilitators primed participants for the upcoming session content and group activities.
Group Introduction Phase
Socialization Time (10 min) The first phase of the group session consisted of socialization time with snacks and facilitated discussion. Peer facilitators guided discussion using visual prompts and checklists. Recognizing that emotional awareness is a key social intervention component (Mazefsky and White 2014), facilitators incorporated emotion recognition into this phase by using feelings charts and emotion thermometers to help participants label their feelings.
Group Interactive Game (10 min) Following socialization time, facilitators introduced an ice-breaker game relevant to the weekly social skill topic to foster learning and social connectedness. For example, music was incorporated as an autism therapy aid (Sharda et al. 2018) to practice greetings in an interactive activity that incorporated music, movement, and greetings practice.
Interactive Social Skill Practice
Target Skill Video I (10 min) The facilitators next initiated an interactive lesson of the week’s social skill topic. The topic was introduced via video modeling, a teaching strategy that has contributed to social skill gains for autistic adults with co-occurring ID (Stauch et al. 2018; Walsh et al. 2018). Twenty videos (two videos per intervention session) were created by study investigators to teach the social skill topic of the week. Each video was intended to model individual components of each target skill (e.g., components of an appropriate greeting) to enhance learning. The target social skill was first modeled (two actors greet each other), then one actor was filmed enacting the skill (waving at the camera and saying “hello”) in slow motion before the same interaction was displayed again. At the start of each video, popular media movie and television show video clips with characters demonstrating the target skills were included to enhance participant engagement (Harrop et al. 2019). We repeated Target Skill Video I twice sequentially in each session to foster learning.
Target Skill Practice (10 min) Next, two group facilitators completed a live scripted role-play to further demonstrate the social skill topic. Given the importance of incorporating family voices into the intervention development process (Nicolaidis et al. 2011; Fletcher-Watson et al. 2019), the role-plays following the video model honored parent suggestions to repeatedly model target skills in different formats. The role-plays were accompanied by simple images that were presented by a facilitator during the dialogue (e.g., a picture of a handshake when the actors were greeting each other). After introduction to the topic, peer facilitators continued to model the skill (Bandura 1979; Vernon et al. 2018) and participants practiced imitating the skill in small break-out groups.
Outdoor Social Activity (10 min)
The group then transitioned into a structured group social activity outside. The social activity phase was designed to sustain attention and motivation, and to promote social bonding and teamwork. Activities varied each week based on the weekly target skill in order to practice the social skill in novel ways.
Interactive Social Skill Practice Part II
Target Skill Video II (10 min) The group phase concluded with a second topic video (played twice) and live scripted role-play using accompanying visuals. Target Skill Video II provided multiple exemplars of the weekly topic to facilitate comprehension and mastery. This approach has been used successfully with individuals with ASD and ID to promote success in related contexts (Murphy and Barnes-Holmes 2017). For the “Greetings & Goodbyes” lessons, the second video demonstrated the goodbye, while the first video demonstrated the greeting. The video series was intended to foster learning by presenting target social skills in incremental steps (Pallathra et al. 2018).
Target Skill Practice II with Summary (10 min) Once the second video and live role-play were completed, the facilitators led a second round of small group practice that included imitation and practice of the skills demonstrated in the second video. Lastly, the group reviewed key take-aways from the session and participants completed a final practice of the target social interaction skill.
Family Check-Out Sessions (10 min)
In order to embrace a participatory model that was adaptive and responsive to family needs (Nicolaidis et al. 2011; Fletcher-Watson et al. 2019), we conducted family check-out meetings after each session and a final group debriefing session at the termination of the SKILL program. In the weekly check-out, facilitators reviewed the participant’s progress during the group session and summarized homework goals for the upcoming week. A written summary of the current topic was provided to the family, along with a framework for introducing the homework social interaction and a checklist to indicate the dates that they practiced the target social skill (goal of 5 times) over the week. Families were also provided with additional copies of materials used during group sessions (e.g., a visual checklist for question-asking) to aid practice at home.
Post SKILL Trial Debriefing Session
At the conclusion of the 10-week SKILL program, all parents and participants were invited to return for a final session to complete follow-up measures and provide oral and written feedback about the intervention. The feedback discussion covered a range of topics including the utility of the video models (sample videos were provided), input on the strategies for teaching social skills, methods to address individual participant needs in the group setting, and the structure of homework assignments. All responses were recorded.
Dependent Measures
Feasibility Measures
Fidelity of Implementation and Attendance Each facilitator completed a fidelity checklist during every group session to monitor adherence to the intervention protocol, including both the schedule and timing of activities. Facilitators also recorded weekly attendance and homework completion (completed, partial completion, not completed) on a checklist. Homework completion was assessed through parent completion of the homework handout indicating the date that they practiced the target social interaction skill with their child over the past week (completed = 5 times, partial completion < 5 times, not completed = did not practice). For adults with limited ability to self-report, weekly attendance rates were an important indicator of their willingness and desire to return to group weekly, per parent report.
Treatment Satisfaction At the conclusion of the SKILL program, parents completed a 10-item Treatment Satisfaction Scale developed for the current study to obtain their impressions of the overall impact of the intervention. The first 6-items were rated on a 5-point scale (e.g., 1 = not helpful/ no benefit, 5 = very helpful/ beneficial) and included items such as “looking back on the program as a whole, please rate how helpful you thought the program was for child.” The remaining items consisted of open-ended questions on components of the program that were most helpful, least helpful, and suggestions for future groups.
Unstructured and Standardized Social Interaction Probes Coding Procedure
Research assistants completed video coding of the unstructured and standardized conversations in random order. All coders were naïve to the study hypotheses, time-point, and study design. Prior to video coding, each coder was extensively trained (to a criterion of at least 90% agreement on all dependent measures). Dependent variables were transcribed and coded using Datavyu software (Datavyu Team 2014). Transcription occurred in order to facilitate the coding process and to provide total speaking durations for the peer and participant during the conversations. Of the 78 standardized and unstructured conversations over the course of the study, 31 (39.7%) of the files were coded by two independent coders for the purpose of inter-rater reliability (IRR), reported below. IRR for eye-contact was assessed using a two-way random, consistency, average measures intraclass-class correlation (ICC).
Group Social Conversation Primary Measure: On-Topic Contributions
On-topic contributions were assessed for all participants during the unstructured and the standardized social interaction probes collected independently of the treatment sessions. All speech produced by the participant during these conversations received a speaking code. Speaking behaviors were further categorized as questions or comments. Questions were defined as inquires intended to elicit a response from the peer. Comments were defined as a verbal statement made immediately following a peer’s verbal statement or question, including minimal verbal encouragers (e.g., “mmm-hmm”). Kappa for identifying question or comment was 0.89, consistent with very strong agreement.
Participant questions and comments were then categorized as contextually on-topic or off-topic using previous peer statements. On-topic questions involved asking a question related to the discussion topic or questions in the spirit of a “get-to-know-you” conversation. On-topic comments were statements directly related to the current topic of conversation. In contrast, off-topic questions or comments were unrelated to the current discussion topic and were not introduced with sufficient context (e.g., If a peer was talking about a favorite restaurant and then the participant randomly referenced their favorite movie). Off-topic also included repeating the peer’s statement (immediate echolalia) and conversational scripting (delayed echolalia), defined as repeating a line to oneself that was not in response to the peer’s question or comment (e.g., repeating a favorite movie line). Kappa for categorizing language as on-topic or off-topic was 0.68, indicating substantial agreement.
Analytic approach For the multiple baseline unstructured conversations, percent of time spent on-topic was calculated by dividing the sum of on-topic conversational contributions by the participant’s total speaking duration to yield a percentage. We present these values for each unstructured conversation throughout treatment and report individual means and ranges at baseline, midpoint, and post-treatment. For the standardized conversations collected once pre- and once post-treatment, on-topic contributions were calculated by summing on-topic comments in response to an established number of conversation bids. A Wilcoxon signed rank test (with continuity correction for small samples) in R was used to compare on-topic contributions during standardized conversations from pre- to post-treatment.
Individualized Social Conversation Measures
Individual social skill measures were collected during the unstructured social interaction probes with typically-developing peers at intake, every 2 weeks before the treatment session, and post-treatment. In addition to the common group social conversation measure (on-topic contributions), social skill targets were selected for each participant at intake that reflected the primary social skill vulnerability of each individual. These individualized targets, related to the core verbal and nonverbal social interaction skill domains previously highlighted in this paper, are summarized below:
Active Listening (Participants 1 and 3) For Participants 1 and 3, there were reported and observed challenges with demonstrating appropriate social engagement with conversational partners, linked to limited use of active listening skills. Active listening was defined as showing appropriate interest while the peer was speaking by engaging in all of the following behavioral indicators: sitting and facing the peer, making eye-contact with the peer, and not talking while the peer was talking. Percent listening behaviors was calculated as the sum of the participant’s time spent listening divided by the peer’s total time spent vocalizing. Kappa for categorizing speaking or listening behaviors was 0.91, indicating very strong agreement.
On-topic Questions (Participant 2) In addition to the group goal of increasing the percent of on-topic contributions, Participant 2 required targeted practice with on-topic question asking. At the start of the intervention, Participant 2 almost exclusively asked scripted questions related to his preferred interests in movies and superheroes, and he demonstrated limited regard for the conversation topic or learning more about the peer’s interests. Targeted practice with Participant 2 focused on increasing his on-topic questions (e.g., “how are you?”). On-topic question asking was calculated by summing the on-topic questions during each conversation.
Eye Contact (Participant 4) Participant 4 made limited eye-contact with social partners at the start of the intervention, so peer facilitators worked to increase his nonverbal engagement during social conversations. Eye contact was a continuous variable that was categorized as directing gaze toward the peer’s face. It was coded on a continuous basis to capture subtle shifts in gaze. Eye contact coding was deemed reliable if the onset and offset times for both coders were within 2 s of each other. Percent eye-contact was calculated as the sum of the participant’s eye-contact duration divided by the conversation duration. The resulting ICC for eye contact was in the good range, ICC = 0.70 (Cicchetti, 1994).
Speaking Duration (Participant 5) While Participant 5 provided brief on-topic conversational contributions at baseline, these were generally short phrase responses and thus, the amount that he spoke was minimal relative to his conversation partners. Specialized practice with Participant 5 targeted his speaking duration during conversations to develop more balanced conversations. Percent speaking duration was calculated by summing the length of questions and comments divided by the total speaking duration (participant and peer) to yield a percentage.
Parent-Report Measures
Parent-report measures were administered at intake and post-treatment. The following survey domains were selected to provide more global impressions of reciprocal social communication skills and social engagement, along with social-emotional regulation skills in daily life.
Social Communication and Interaction The Total Social Communication and Interaction (SCI) standard score of the SRS-2A (Constantino and Gruber 2012) is made up of four subtests: Social Awareness, Social Cognition, Social Communication, and Social Motivation. The SCI t-score indicates an individual’s degree of difficulty with social understanding and interaction that may interfere with everyday social interactions (M = 50, SD = 10). A Wilcoxon signed rank test (with continuity correction for small samples) in R was used to compare parent-reported SCI scores from pre- to post-treatment.
Adaptive Socialization Skills The Socialization adaptive domain of the Vineland-3 (Sparrow et al. 2016) is composed of three subdomains: Interpersonal Relationships (skills used to establish and maintain friendships), Play and Leisure Time (skills related to engaging in age-appropriate individual and group activities), and Coping Skills (skills related to self-regulation and behavioral flexibility). The mean for the Vineland-3 socialization domain is 100 (SD = 15).
Social Motivation and Competency The Social Motivation Competency Scale (SMCS) is a rating scale developed by our research team for use in a previous study of a socialization intervention for adolescents (Vernon et al. 2018). Items pertaining to social comfort, conversation skill use, empathy, friendships, appropriate behavior, social contact, and social interest are rated by caregivers on 1–5 Likert scales.
Emotion Regulation The Emotion Dysregulation Inventory (EDI; Mazefsky et al. 2018) is a caregiver-report survey that is designed to capture emotional distress and problems with emotion regulation across a range of functioning in ASD. The EDI Reactivity scale captures emotional reactions through endorsements of the severity of problem behaviors (Not at All—Very Severe). The EDI has been found to have good reliability in samples of adults across the spectrum of ASD (α = 0.94; Conner et al. 2018).
Results
Feasibility
Adherence to the weekly session protocol (percentage of objectives completed) was 96.8% on average (range: 82.6–100%). The mean attendance rate for all five participants was 96.0%. Three of the five participants attended all 10 sessions, while two participants missed one session each. The majority of participants completed weekly homework assignments (session means: completed = 62.8%, partial completion = 11.6%, not completed = 27.9%).
Treatment Acceptability
The mean rating for helpfulness of the intervention content (on a scale of 1 = “not helpful/ no benefit” to 5 = “very helpful/ very beneficial”) across all 10 sessions was 4.50 (SD = 0.50), and the helpfulness of the homework for providing skills to practice at home was rated 4.17 on average (SD = 1.46). The family that ranked the helpfulness of the homework the lowest (Participant 2) rarely completed homework throughout the intervention. On a 5-point Likert scale (1 = “not at all” to 5 = “extremely”), participants’ perceived enjoyment of the social group (M = 4.17, SD = 0.90) and the likelihood of recommending the program to another family (M = 5.00) were both rated highly by parents. Parents also endorsed that participation in the group was meaningful to their families (M = 4.67, SD = 0.75). In contrast, parents provided lower ratings in response to a question regarding their satisfaction with available community services to support their child’s social communication development, not including the SKILL program (M = 2.83, SD = 1.57).
Social Conversation Outcomes
Group Social Conversations Primary Measure: On-Topic Contributions
Unstructured Conversations For the 3-min multiple baseline unstructured conversations, there were individual gains in the percent of time on-topic from baseline to post-intervention (Fig. 2). On-topic conversational contributions increased from pre- to post-treatment for Participant 1 (pre M = 14.75%, range: 0.98–28.51%; post M = 33.83%, range: 21.62–46.03%), Participant 2 (pre M = 68.81%, range: 66.40–71.22%; post M = 74.32%, range: 67.44–81.21%), Participant 3 (pre M = 40.50, range: 22.90–61.46%; post M = 72.69%, range: 60.51–84.88%), and Participant 4 (pre M = 9.76%, range: 0.00–40.34%; post M = 20.39%, range: 10.40–30.37%). Participant 5 spent the majority of conversations on-topic at baseline (pre M = 97.65%), and he remained consistent throughout treatment (post M = 96.55%).

On-topic conversational contributions
Standardized Conversations In addition to the unstructured conversations, all participants completed one standardized conversation pre-treatment and one post-treatment. The standardized conversations included an intentional number of conversation bids to explore the frequency of on-topic responses. For the structured conversations, there was a 10.0 mean increase in the number of on-topic responses to conversation bids from pre-treatment (M = 10.4, SD = 3.1) to post-treatment (M = 20.4, SD = 4.2) for all participants (Wilcoxon Signed Ranks Test, V = 1, p = 0.06, d = 2.7; Fig. 3).

Mean number of on-topic responses from baseline to post-intervention during standardized conversation protocol. Note: The blue line indicates the mean and standard error from pre- to post-treatment for all participants (n = 5)
Individualized Social Conversation Measures
Active Listening (Participant 1 and Participant 3) Participants 1 and 3 demonstrated low initial levels of active listening behaviors while the peer was speaking (1 M = 20.53%, range: 0.00–41.07%; 3 M = 13.25%, range: 1.40–37.11%). After targeting this skill in the first four weeks of the intervention, Participant 1’s listening behaviors increased at midpoint (M = 35.53%, range: 1.51–69.55%) and continued to increase through the end of the intervention (M = 45.53%, range: 37.75–53.32%). Participant 3’s listening behaviors remained consistent at midpoint (M = 11.75%, range: 5.84–17.65%) and increased post-treatment (M = 36.24%, range: 21.20–51.28%; Fig. 4).

Individualized social interaction skill targets
On-Topic Questions (Participant 2) Participant 2 demonstrated low frequency of on-topic question asking at baseline (M = 4.0, range: 4.0). Over the course of treatment, Participant 2’s number of on-topic questions increased from midpoint (M = 13.5, range: 12.0–15.0) to post-intervention (M = 14.0, range: 13.0–15.0; Fig. 4).
Eye Contact (Participant 4) At baseline, Participant 4’s eye-contact during conversations was limited (M = 5.07%, range: 0.09–11.03%). Participant 4’s eye-contact increased at the midpoint (M = 9.08%, range: 4.28–13.88%) and slightly decreased from midpoint to post-intervention (M = 6.29%, range: 3.15–9.43%; Fig. 4). Consistent with increased active listening skills, both Participant 1 and Participant 3 also exhibited gains in eye-contact from baseline (1 M = 35.44%, range: 29.86–41.03%; 3 M = 7.35%, range: 3.70 – 15.63%) to post-intervention (1 M = 50.41%, range: 45.03–55.79%; 3 M = 27.01%, range: 20.11–33.91%).
Speaking Duration (Participant 5) At baseline, Participant 5 provided few conversational contributions relative to the total speaking duration (M = 21.98%, range: 15.35–28.21%). Participant 5’s speaking contributions remained relatively consistent at midpoint (M = 21.75%, range: 13.00–30.50%) and increased post-intervention (M = 37.10%, range: 28.33–45.86%; Fig. 4).
Parent Social Survey Measures
For the survey data, average change scores and associated effect sizes are summarized in Table 3.
SRS-2 SCI
There were significant improvements on the SRS-2 Social Communication Index (Wilcoxon Signed Ranks Test, V = 10, p < 0.05). When comparing pre-intervention and post-intervention means for the parent-reported SRS-2 SCI, four Participants (1, 3, 4, 5) experienced a reduction in their total score, indicating a decrease in their endorsement of social communication challenges. Participant 2 experienced a negligible change in score. The mean change in the SRS-2 SCI score was -3.5 (range of -5 to -3).
Vineland-3 Socialization Domain
The parent-reported Vineland-3 Socialization domain scores demonstrated an increase in scores in three Participants (1, 3, 5), which is indicative of the desired increase in socialization. Participant 2 and Participant 4’s scores remained the same. The mean change in the Vineland-3 Socialization score from pre-intervention to post-intervention was 8.0 (range of −8 to 17).
SMCS
A comparison of the pre-intervention and post-intervention scores of the parent-reported SMCS were indicative of social increases in four Participants (1, 3, 4, 5). Participant 2 experienced a negligible change in score. The mean change in the SMCS score was 6.25 (range of 2 to 8).
EDI – Reactivity Scale
A comparison of the parent-reported EDI—Reactivity scores demonstrated a decrease in scores in three Participants (1, 2, 4), indicative of the desired decrease in poorly regulated negative emotional reactions. Participants 3 and 5 experienced slight increases in scores. The mean change in the EDI—Reactivity score from pre-intervention to post-intervention was −1.5 (range of −7.9 to 4.5).
Discussion
This pilot investigation of the SKILL program aimed to assess the feasibility, acceptability, and preliminary efficacy of a novel social competence intervention for adults on the autism spectrum with co-occurring ID and limited functional language. Using a multiple baseline design, we explored social communication gains through coded social behaviors during filmed conversation probes and complementary parent-survey measures. Initial findings support feasibility of implementation and acceptability of the program to adults on the autism spectrum and their families, as measured through weekly fidelity checklists, treatment satisfaction ratings, and attendance tracking. Findings from filmed social conversations demonstrate developing improvements in verbal (on-topic conversational contributions) and nonverbal (eye-contact, active listening) social competencies following participation in the SKILL program. These findings provide preliminary evidence that the SKILL program enhances social communication skills that are critical to social functioning and lay the foundation for continued research into evidence-based treatment strategies for this under served population.
Social Communication Outcomes
We examined a key social interaction skill as our primary group outcome measure—on-topic conversational contributions—in both unstructured conversations and standardized conversations. With the exception of Participant 5, who upon further analysis was already found to make on-topic contributions at baseline (albeit with significant response latency), all participants increased their use of on-topic conversational contributions during unstructured conversations at the end of treatment. Given that some participants trended positive during baseline in the on-topic variable, future investigations will ensure that there is a steady or declining trend at baseline. During standardized conversations, participants also demonstrated a notable increase in on-topic responses to conversation bids, suggesting that the SKILL program may improve participants’ ability to provide contextually appropriate responses.
All participants demonstrated evidence of emerging but meaningful individualized social improvements after completion of the SKILL curriculum. Participant 1, who exhibited few active listening behaviors at the start of the intervention, demonstrated appropriate listening behaviors approximately half of the time when peers spoke to him at the end of the trial. Participant 2 almost exclusively asked scripted questions related to his preferred interests at baseline, so it was notable that he asked more diverse, on-topic questions post-intervention. Participant 3 increased his use of active listening behaviors by sitting and facing the peer, making eye-contact, and not speaking while the peer was speaking post-intervention, which indicated marked improvement from his tendency to disengage during conversations at baseline. Participant 4 evidenced improvements in nonverbal engagement with increased eye contact over the course of treatment. Finally, Participant 5 expanded beyond his typical brief responses and ultimately increased his frequency of conversational contributions to yield more balanced conversations with peers. These individual trajectories of social skill development resulting from participation in the SKILL program suggest that this comprehensive package with individualized components may be effective in targeting a range of social vulnerabilities (Kasari et al. 2018).
On parent-report measures of social functioning, parents reported an upward trajectory of social communication growth that could be strengthened with prolonged treatment duration. Specifically, the majority of parents reported reductions in social communication challenges and corresponding increases in adaptive socialization skills. With regard to poorly regulated emotional responses, some parents reported a decrease in emotional reactivity. While emotion regulation skills were not a primary outcome of this study, this finding lends support for further exploration of strategies to target challenging social behaviors in the context of social intervention efforts for this population. Taken together, the SKILL program results demonstrate the promise of a group social communication intervention for autistic adults who are severely affected in cognitive and language domains.
Limitations and Future Directions
This pilot investigation was intended to assess the feasibility, acceptability, and preliminary efficacy of a manualized intervention package for a small cohort of autistic adults with ID and limited language. The presented data reveal promising gains in core social interaction skills. While large treatment effects were not consistently obtained, it is important to interpret these gains in light of the complex characterization profiles and developmental histories of the selected participants. These are autistic individuals with ID and limited language use who have been exposed to a variety of behavioral and educational interventions over their entire lifespan. The goal of this trial was not to create transformational change in participant social profiles, but rather to demonstrate that continued social improvement is still possible for this population. The ability to “move the needle” is a critical first step in this line of research. The next step is to explore sustained use of these strategies in a longer, more intensive format to create more impactful, generalized improvements to social functioning.
Additional research studies are needed to validate these preliminary findings and to address limitations of the pilot study. In order to control for participant maturation, attention, and expectancy effects, a randomized clinical trial (RCT) with a control group is needed to further evaluate the efficacy of the SKILL program. To address minimal diversity amongst pilot participants, the RCT should include a more diverse group of males and females from a range of socioeconomic and racial/ethnic backgrounds to increase the generalizability of our findings. To enhance our baseline characterization of this population, we plan to include a more comprehensive battery of assessments targeted toward individuals with limited language to more thoroughly characterize participants and measure improvements. Modifications to our characterization battery will include the Adapted ADOS (Bal et al. 2020) as a clinician-administered measure of autism symptomatology for minimally-verbal adults. Finally, more work is needed to understand the nuances of social engagement and motivation for autistic individuals with ID (Neuhaus et al. 2019). To capture social motivation as a possible predictor of individual difference in response to SKILL, we will include the Stanford Social Dimensions Scale (SSDS), a parent-report measure of this construct (Phillips et al. 2019).
Future investigations with this understudied population will continue to evaluate the optimal treatment duration to maximize social improvements. To this end, we plan to incorporate standardized checklists for peer facilitators to code participants’ social skill acquisition during the final practice in each session. To monitor the generalization of social skills, it would also be useful to teach and measure these variables in novel settings, including at home, school, residential living, or vocational settings (Walsh et al. 2018).
Furthermore, to better understand mechanisms of action and the nuances of social skill improvements, future studies should consider the use of available technologies and analytic techniques. Automated computational linguistic and computer vision tools will enable us to capture verbal (language characteristics, acoustics) and nonverbal (facial expressions) social competencies with greater granularity than manual behavior coding (e.g., Parish-Morris et al. 2018). Additionally, psychophysiological measures of arousal (heart rate, skin conductance) may provide insights into underlying mechanisms driving social engagement and avoidance (e.g., Dijkhuis et al. 2019). To systematize a personalized approach to the SKILL program based on these variables, future investigations may employ adaptive treatment designs, such as the Sequential Multiple Assignment Randomized Trial (SMART) design, to tailor intervention content to individual profiles of needs and abilities (Kasari et al. 2018).
Conclusion
In determining meaningful and relevant outcomes for this population, it is important to consider quality of life variables for autistic adults with ID and their families. Schalock and colleagues’ (2002) review of quality of life for individuals with ID notes that emotional well-being, social inclusion, personal development, and self-determination are all important domains of well-being. Further examination of social skills that are likely to promote enhanced quality of life may guide our work in choosing meaningful social goals for autistic adults with ID and limited functional language. Finally, more research is needed to understand this population’s complex, nuanced treatment needs, and to target implementation and dissemination barriers to address a critical gap in adult services nationwide.
Notes
This manuscript uses both Identity-first and Person-first language, consistent with practices among autistic-self advocates and community stakeholders (Kenny et al. 2016).
References
Bal, V. H., Maye, M., Salzman, E., Huerta, M., Pepa, L., Risi, S., et al. (2020). The Adapted ADOS: A new module set for the assessment of minimally verbal adolescents and adults. Journal of Autism and Developmental Disorders, 50(3), 719–729.
Bandura, A. (1979). Self-referent mechanisms in social learning theory. American Psychologist, 34(5), 439–441. https://doi.org/10.1037/0003-066X.34.5.439.b.
Barry, T. D., Klinger, L. G., Lee, J. M., Palardy, N., Gilmore, T., & Bodin, S. D. (2003). Examining the effectiveness of an outpatient clinic-based social skills group for high-functioning children with autism. Journal of Autism and Developmental Disorders, 33(6), 685–701. https://doi.org/10.1023/B:JADD.0000006004.86556.e0.
Chang, Y.-C., & Locke, J. (2016). A systematic review of peer-mediated interventions for children with autism spectrum disorder. Research in Autism Spectrum Disorders, 27, 1–10. https://doi.org/10.1016/j.rasd.2016.03.010.
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment, 6(4), 284–290. https://doi.org/10.1037/1040-3590.6.4.284.
Conner, C. M., White, S. W., Beck, K. B., Golt, J., Smith, I. C., Mazefsky, C. A. (2018). Improving emotion regulation ability in autism: The Emotional Awareness and Skills Enhancement (EASE) program. Autism: The International Journal of Research and Practice, 1362361318810709. https://doi.org/10.1177/1362361318810709
Corbett, B. A., & Abdullah, M. (2005). Video modeling: Why does it work for children with autism? Journal of Early and Intensive Behavior Intervention, 2(1), 2–8. https://doi.org/10.1037/h0100294.
Constantino, J. N., & Gruber, C. P. (2012). Social responsiveness scale: SRS-2. Torrance, CA: Western Psychological Services.
DiStefano, C., Shih, W., Kaiser, A., Landa, R., & Kasari, C. (2016). Communication growth in minimally verbal children with ASD: The importance of interaction. Autism Research: Official Journal of the International Society for Autism Research, 9(10), 1093–1102. https://doi.org/10.1002/aur.1594.
Dudley, K. M., Klinger, M. R., Meyer, A., Powell, P., & Klinger, L. G. (2019). Understanding service usage and needs for adults with asd: the importance of living situation. Journal of Autism and Developmental Disorders, 49(2), 556–568. https://doi.org/10.1007/s10803-018-3729-0.
Duncan, D., Matson, J. L., Bamburg, J. W., Cherry, K. E., & Buckley, T. (1999). The relationship of self-injurious behavior and aggression to social skills in persons with severe and profound learning disability. Research in Developmental Disabilities, 20(6), 441–448. https://doi.org/10.1016/S0891-4222(99)00024-4.
Dunn, L. M., & Dunn, D. M. (2007). Peabody Picture Vocabulary Test—Fourth Edition PPVT4. Bloomington, MN: NCS Pearson.
Dijkhuis, R. R., Ziermans, T., van Rijn, S., Staal, W., & Swaab, H. (2019). Emotional arousal during social stress in young adults with autism: Insights from heart rate, heart rate variability and self-report. Journal of autism and developmental disorders, 49(6), 2524–2535.
Dyson, M. W., Chlebowski, C., & Brookman-Frazee, L. (2019). Therapists’ adaptations to an intervention to reduce challenging behaviors in children with autism spectrum disorder in publicly funded mental health services. Journal of autism and developmental disorders, 49(3), 924–934.
Fletcher-Watson, S., Adams, J., Brook, K., Charman, T., Crane, L., Cusack, J., et al. (2019). Making the future together: Shaping autism research through meaningful participation. Autism, 23(4), 943–953. https://doi.org/10.1177/1362361318786721.
Carminati, G., Gerber, F., Baud, M. A., & Baud, O. (2007). Evaluating the effects of a structured program for adults with autism spectrum disorders and intellectual disabilities. Research in Autism Spectrum Disorders, 1(3), 256–265. https://doi.org/10.1016/j.rasd.2006.11.001.
Gates, J. A., Kang, E., & Lerner, M. D. (2017). Efficacy of group social skills interventions for youth with autism spectrum disorder: A systematic review and meta-analysis. Clinical Psychology Review, 52, 164–181. https://doi.org/10.1016/j.cpr.2017.01.006.
Gotham, K., Marvin, A. R., Taylor, J. L., Warren, Z., Anderson, C. M., Law, P. A., et al. (2015). Characterizing the daily life, needs, and priorities of adults with autism spectrum disorder from Interactive Autism Network data. Autism, 19(7), 794–804. https://doi.org/10.1177/1362361315583818.
Harrop, C., Amsbary, J., Towner-Wright, S., Reichow, B., & Boyd, B. A. (2019). That’s what I like: The use of circumscribed interests within interventions for individuals with autism spectrum disorder. A systematic review. Research in Autism Spectrum Disorders, 57, 63–86. https://doi.org/10.1016/j.rasd.2018.09.008.
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry, 45(2), 212–229. https://doi.org/10.1111/j.1469-7610.2004.00215.x.
Hume, K., Loftin, R., & Lantz, J. (2009). Increasing independence in autism spectrum disorders: A review of three focused interventions. Journal of Autism and Developmental Disorders, 39(9), 1329–1338. https://doi.org/10.1007/s10803-009-0751-2.
Ingersoll, B., & Wainer, A. (2013). Initial efficacy of project ImPACT: A parent-mediated social communication intervention for young children with ASD. Journal of Autism and Developmental Disorders, 43(12), 2943–2952. https://doi.org/10.1007/s10803-013-1840-9.
Kasari, C., Alexandra, S., & Wendy, S. (2018). SMARTer approach to personalizing intervention for children with autism spectrum disorder. Journal of Speech, Language, and Hearing Research, 61(11), 2629–2640. https://doi.org/10.1044/2018_JSLHR-L-RSAUT-18-0029.
Ko, J. A., Miller, A. R., & Vernon, T. W. (2019). Social conversation skill improvements associated with the Social Tools And Rules for Teens program for adolescents with autism spectrum disorder: Results of a randomized controlled trial. Autism, 23(5), 1224–1235. https://doi.org/10.1177/1362361318808781.
Krasileva, K. E., Sanders, S. J., & Bal, V. H. (2017). Peabody picture vocabulary test: Proxy for verbal iq in genetic studies of autism spectrum disorder. Journal of Autism and Developmental Disorders, 47(4), 1073–1085. https://doi.org/10.1007/s10803-017-3030-7.
Kaufman, A. S. (1990). Kaufman brief intelligence test: KBIT. Circle Pines, MN: AGS, American Guidance Service.
Leaf, J. B., Townley-Cochran, D., Taubman, M., Cihon, J. H., Oppenheim-Leaf, M. L., Kassardjian, A., et al. (2015). The Teaching interaction procedure and behavioral skills training for individuals diagnosed with autism spectrum disorder: A review and commentary. Review Journal of Autism and Developmental Disorders, 2(4), 402–413. https://doi.org/10.1007/s40489-015-0060-y.
Maenner, M. J. (2020). Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016 (p. 69). Surveillance Summaries: MMWR.
Matson, J. L., & Shoemaker, M. (2009). Intellectual disability and its relationship to autism spectrum disorders. Research in Developmental Disabilities, 30(6), 1107–1114. https://doi.org/10.1016/j.ridd.2009.06.003.
Mazefsky, C. A., Day, T. N., Siegel, M., White, S. W., Yu, L., Pilkonis, P. A., et al. (2018). Development of the Emotion Dysregulation Inventory: A PROMIS®ing Method for Creating Sensitive and Unbiased Questionnaires for Autism Spectrum Disorder. Journal of Autism and Developmental Disorders, 48(11), 3736–3746. https://doi.org/10.1007/s10803-016-2907-1.
Mazefsky, C. A., Herrington, J., Siegel, M., Scarpa, A., Maddox, B. B., Scahill, L., et al. (2013). The Role of Emotion Regulation In Autism Spectrum Disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 52(7), 679–688. https://doi.org/10.1016/j.jaac.2013.05.006.
Mazefsky, C. A., & White, S. W. (2014). Emotion Regulation: Concepts & Practice in Autism Spectrum Disorder. Child and Adolescent Psychiatric Clinics of North America, 23(1). https://doi.org/10.1016/j.chc.2013.07.002
Murphy, C., Barnes-Holmes, P. M. D. (2017). Teaching important relational skills for children with Autism spectrum disorder and intellectual disability using freely available (GO-IRAP) software. Austin Journal of Autism & Related Disabilities, 3(2).
National Research Council (US) and Institute of Medicine (US) Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth, and Young Adults: Research Advances and Promising Interventions. (2009). Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities (M. E. O’Connell, T. Boat, & K. E. Warner, Eds.). National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK32775/
Neuhaus, E., Webb, S. J., & Bernier, R. A. (2019). Linking social motivation with social skill: The role of emotion dysregulation in autism spectrum disorder. Development and psychopathology, 31(3), 931–943.
Nicolaidis, C., Raymaker, D., McDonald, K., Dern, S., Ashkenazy, E., Boisclair, C., et al. (2011). Collaboration strategies in nontraditional community-based participatory research partnerships: lessons from an academic-community partnership with autistic self-advocates. Progress in Community Health Partnerships, 5(2), 143–150. https://doi.org/10.1353/cpr.2011.0022.
Pallathra, A. A., Calkins, M. E., Parish-Morris, J., Maddox, B. B., Perez, L. S., Miller, J., et al. (2018). Defining behavioral components of social functioning in adults with autism spectrum disorder as targets for treatment. Autism Research, 11(3), 488–502. https://doi.org/10.1002/aur.1910.
Pallathra, A. A., Cordero, L., Wong, K., & Brodkin, E. S. (2019). Psychosocial interventions targeting social functioning in adults on the autism spectrum: A literature review. Current Psychiatry Reports. https://doi.org/10.1007/s11920-019-0989-0.
Parish-Morris, J., Sariyanidi, E., Zampella, C., Bartley, G. K., Ferguson, E., Pallathra, A. A., Bateman, L., Plate, S., Cola, M., Pandey, J., Brodkin, E. S., Schultz, R. T., Tunç, B. (2018). Oral-Motor and Lexical Diversity During Naturalistic Conversations in Adults with Autism Spectrum Disorder. Proceedings of the Fifth Workshop on Computational Linguistics and Clinical Psychology: From Keyboard to Clinic, 147–157. https://doi.org/10.18653/v1/W18-0616
Phillips, J. M., Uljarević, M., Schuck, R. K., Schapp, S., Solomon, E. M., Salzman, E., et al. (2019). Development of the Stanford Social Dimensions Scale: initial validation in autism spectrum disorder and in neurotypicals. Molecular autism, 10(1), 1–16.
Płatos, M., & Wojaczek, K. (2018). Broadening the scope of peer-mediated intervention for individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 48(3), 747–750. https://doi.org/10.1007/s10803-017-3429-1.
Ratto, A. B., Turner-Brown, L., Rupp, B. M., Mesibov, G. B., & Penn, D. L. (2011). Development of the contextual assessment of social skills (cass): A role play measure of social skill for individuals with high-functioning autism. Journal of Autism and Developmental Disorders, 41(9), 1277–1286. https://doi.org/10.1007/s10803-010-1147-z.
Russell, G., Mandy, W., Elliott, D., White, R., Pittwood, T., & Ford, T. (2019). Selection bias on intellectual ability in autism research: A cross-sectional review and meta-analysis. Molecular Autism, 10(1), 9. https://doi.org/10.1186/s13229-019-0260-x.
Ryan, G., Brady, S., Holloway, J., & Lydon, H. (2019). Increasing appropriate conversation skills using a behavioral skills training package for adults with intellectual disability and autism spectrum disorder. Journal of Intellectual Disabilities, 23(4), 567–580. https://doi.org/10.1177/1744629517750744.
Schalock, R. L., Brown, I., Brown, R., Cummins, R. A., Felce, D., Matikka, L., et al. (2002). Conceptualization, measurement, and application of quality of life for persons with intellectual disabilities: Report of an international panel of experts. Mental Retardation, 40(6), 457–470. https://doi.org/10.1352/0047-6765(2002)040<0457:CMAAOQ>2.0.CO;2.
Sharda, M., Tuerk, C., Chowdhury, R., Jamey, K., Foster, N., Custo-Blanch, M., et al. (2018). Music improves social communication and auditory–motor connectivity in children with autism. Translational Psychiatry, 8(1), 1–13. https://doi.org/10.1038/s41398-018-0287-3.
Shattuck, P. T., Narendorf, S. C., Cooper, B., Sterzing, P. R., Wagner, M., & Taylor, J. L. (2012). Postsecondary Education and Employment Among Youth With an Autism Spectrum Disorder. Pediatrics, 129(6), 1042–1049. https://doi.org/10.1542/peds.2011-2864.
Siaperas, P., & Beadle-Brown, J. (2006). A case study of the use of a structured teaching approach in adults with autism in a residential home in Greece. Autism, 10(4), 330–343. https://doi.org/10.1177/1362361306064433.
Siegel, M. (2018). The severe end of the spectrum: Insights and opportunities from the autism inpatient collection (AIC). Journal of Autism and Developmental Disorders, 48(11), 3641–3646. https://doi.org/10.1007/s10803-018-3731-6.
Sparrow, S. S., Cicchetti, D. V., Saulnier, C. A. (2016). Vineland Adaptive Behavior Scales-Third Edition (Vineland-3).
Spriggs, A. D., Knight, V., & Sherrow, L. (2015). Talking picture schedules: Embedding video models into visual activity schedules to increase independence for students with ASD. Journal of Autism and Developmental Disorders, 45(12), 3846–3861. https://doi.org/10.1007/s10803-014-2315-3.
Stauch, T. A., Plavnick, J. B., Sankar, S., & Gallagher, A. C. (2018). Teaching social perception skills to adolescents with autism and intellectual disabilities using video-based group instruction. Journal of Applied Behavior Analysis, 51(3), 647–666. https://doi.org/10.1002/jaba.473.
Stedman, A., Taylor, B., Erard, M., Peura, C., & Siegel, M. (2019). Are children severely affected by autism spectrum disorder underrepresented in treatment studies? An analysis of the literature. Journal of Autism and Developmental Disorders, 49(4), 1378–1390. https://doi.org/10.1007/s10803-018-3844-y.
Taylor, J. L., Henninger, N. A., & Mailick, M. R. (2015). Longitudinal patterns of employment and postsecondary education for adults with autism and average-range IQ. Autism, 19(7), 785–793. https://doi.org/10.1177/1362361315585643.
Team, D. (2014). Datavyu: A video coding tool. Databrary Project, New York University. http://datavyu.org.
Thompson, C., McDonald, J., Kidd, T., Falkmer, T., Bölte, S., Girdler, S. (2020). “I don’t want to be a patient”: Peer mentoring partnership fosters communication for autistic university students. Scandinavian Journal of Occupational Therapy, 1–16.
Totsika, V., Felce, D., Kerr, M., & Hastings, R. P. (2010). Behavior problems, psychiatric symptoms, and quality of life for older adults with intellectual disability with and without autism. Journal of Autism and Developmental Disorders, 40(10), 1171–1178. https://doi.org/10.1007/s10803-010-0975-1.
Vernon, T. W., Holden, A. N., Barrett, A. C., Bradshaw, J., Ko, J. A., McGarry, E. S., et al. (2019). A pilot randomized clinical trial of an enhanced pivotal response treatment approach for young children with autism: The PRISM model. Journal of Autism and Developmental Disorders, 49(6), 2358–2373. https://doi.org/10.1007/s10803-019-03909-1.
Vernon, T. W., Miller, A. R., Ko, J. A., Barrett, A. C., & McGarry, E. S. (2018). A randomized controlled trial of the social tools and rules for teens (START) program: An immersive socialization intervention for adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 48(3), 892–904. https://doi.org/10.1007/s10803-017-3380-1.
Walsh, E., Holloway, J., & Lydon, H. (2018). An evaluation of a social skills intervention for adults with autism spectrum disorder and intellectual disabilities preparing for employment in ireland: A pilot study. Journal of Autism and Developmental Disorders, 48(5), 1727–1741. https://doi.org/10.1007/s10803-017-3441-5.
Walsh, E., Holloway, J., Lydon, H., McGrath, A., & Cunningham, T. (2019). An exploration of the performance and generalization outcomes of a social skills intervention for adults with autism and intellectual disabilities. Advances in Neurodevelopmental Disorders, 3(4), 372–385. https://doi.org/10.1007/s41252-019-00125-x.
Walton, K. M., & Ingersoll, B. R. (2013). Improving social skills in adolescents and adults with autism and severe to profound intellectual disability: A review of the literature. Journal of Autism and Developmental Disorders, 43(3), 594–615. https://doi.org/10.1007/s10803-012-1601-1.
Williams, K. T., Williams, K. T. (2007). EVT-2: Expressive vocabulary test. Pearson.
Acknowledgements
The authors would like to acknowledge our dedicated team of behavior coders and peer facilitators who made this research possible. We are also grateful for the commitment and input from our participating families.
Funding
University of California Santa Barbara, Academic Senate Grant (PI: Vernon).
Author information
Authors and Affiliations
Contributions
Author Contributions
EF conceived of the study along with TV, facilitated its design and coordination, collected the data, performed the statistical analysis, interpreted the data, and drafted the manuscript. KD contributed to study design and coordination, data collection, and manuscript development. JL assisted with writing scripts perform reliability checks, creating variables for behaviorally-coded data, and analyzing the data. KH contributed to the development of behavior-coding schemes, developing a coding manual, and training new coders. HF assisted with the development of behavior-coding procedures, data interpretation, and the preparation of figures for the manuscript. AM participated in study design, coordination, and data collection. TV participated in the design and coordination of the study, collected data, assisted with interpretation of the data, and revised the manuscript critically. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Consent to Participate
Informed consent was obtained from legal guardians and assent was obtained from all adults included in the study.
Consent to Publish
Participants signed informed consent regarding publishing their data.
Ethics Approval
Approval was obtained from the ethics committee of University of California, Santa Barbara. The authors certify that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ferguson, E.F., Drapalik, K.N., Liang, J. et al. Social Interaction Skill Intervention for Autistic Adults with Intellectual Disability and Limited Language: A Pilot of the SKILL Program. J Autism Dev Disord 51, 1641–1657 (2021). https://doi.org/10.1007/s10803-020-04659-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-020-04659-1