
Abstract
This investigation is a secondary analysis of data from a randomized control trial of the PLAY Home Consultation Intervention Program which was conducted with 112 preschool children with Autism Spectrum Disorders and their parents (Solomon et al. in J Dev Behav Pediatr 35:475–485, 2014). Subjects were randomly assigned to either a community standard (CS) treatment group or to the PLAY Project plus CS Treatment (PLAY). PLAY subjects received monthly parent–child intervention sessions for 1 year during which parents learned how to use the rationale and interactive strategies of the Developmental, Individual-differences, Relationship-based (DIR) intervention model (Greenspan and Weider in The child with special needs: encouraging intellectual and emotional growth. DeCapo Press, Cambridge, MA, 1998) to engage in more responsive, affective and less directive interactions with their children. This investigation examined whether PLAY intervention effects on parents’ style of interacting with their children as well as on children’s social engagement mediated the effects of PLAY on children’s autism severity as measured by ADOS calibrated severity scores. Regression procedures were used to test for mediation. There were two main findings. First the effects of PLAY on children’s social engagement were mediated by the increases in parental responsiveness and affect that were promoted by PLAY. Second, the effects of PLAY on the severity children’s Social Affect disorders were mediated by changes in parental responsiveness and affect; however, the effects of Responsive/Affect were mediated by the impact these variables had on children’s social engagement. Results are discussed in terms of contemporary models of developmental change including the developmental change model that is the foundation for DIR.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The PLAY Project [(PLAY)—Play and Language for Autistic Youngsters] is a relationship based early intervention (RBI) that is designed to enhance children’s developmental functioning and decrease their autistic characteristics by teaching parents to routinely engage in social, play and communicative interactions that are characterized by high levels of responsiveness and affect and moderate to low levels of directiveness. PLAY has operationalized the Developmental, Individual-differences, Relationship-based (DIR) intervention model developed by Greenspan and Wieder (1997, 1998) by adapting DIR theory and principles into a structured home visiting intervention that includes coaching, modeling, and video feedback related to parents’ use of PLAY methods, techniques, and activities.
A randomized control trial (RCT) of PLAY was conducted with 112 preschool aged children with diagnoses of Autism Spectrum Disorder (ASD) and their parents (Solomon et al. 2014). Subjects were randomly assigned to a community standard (CS) intervention plus PLAY versus a CS intervention only. Over the course of 1 year, PLAY consultants made monthly 3 h home visits during which they coached parents on the use of PLAY strategies. In addition, a 15 min video of representative play interaction was recorded and analyzed. This analysis was used to develop a written plan describing methods, techniques, and activities to foster parents’ interactional abilities and promote their children’s development.
Pre-post comparisons indicated that compared to CS mothers, PLAY mothers’ interactions with their children became more responsive and affective and less directive. In addition, PLAY children’s interactions were marked by a significant increase in social engagement. Although, group differences on standardized language and certain developmental measures were not significant, there were significant group differences on children’s Autism Diagnostic Observation Schedule (ADOS-G). PLAY children were more than twice as likely as CS children to improve their ADOS-G diagnostic classification.
While results from this study indicated that PLAY was causally related to improvements in children’s autism classification, this study did not delineate the mechanisms that were the basis for these changes. That is, changes in autism classification could have been caused by one or all of the changes in parent interactive style that were promoted by PLAY, or by the effects of PLAY on children’s social engagement. Information about the actual mechanisms that contributed to children’s changes are important not only for improving the efficiency of PLAY, but also for identifying processes that may be helpful for improving the effectiveness of other interventions for young children with autism (Aldred et al. 2012).
Parenting Style and Developmental Change
PLAY is based upon the transactional model of development (Sameroff 2010) which asserts that the quality and frequency of interactions that take place between parents and children are the primary mechanism for developmental change. The focus of PLAY on encouraging high levels of responsiveness and affect is consistent with descriptive research studies which have reported that parental responsiveness, particularly as assessed by measures of contingency, reciprocity, affect and non-directiveness, is associated with optimal levels of child development and social emotional functioning (Warren and Brady 2007; Mahoney and Nam 2011). These findings have not only been reported for typically developing children but also for children with a range of developmental risks and disabilities including autism (McDuffie and Yoder 2010; Siller and Sigman 2002, 2008).
PLAY encourages parents to use interactional methods and strategies to enhance their children’s engagement in social interaction. It is organized around the Functional Emotional Developmental Levels (FEDL) as described by Greenspan and Weider (1998) which is used to guide the principles and practices of intervention plans. PLAY asserts that the increases in children’s functional emotional development which parents promote through social engagement not only address children’s social deficits but also enhance the learning processes that are the foundations for their developmental learning.
Causal Analyses of Relationship Based Interventions (RBI)
Several investigations have reported that RBI interventions are effective at promoting various domains of development for children with a variety of disabilities including ASD (c.f., Mahoney and Nam 2011; McCollum and Hemmeter 1997; Trivette 2003). Similar to results reported in the PLAY RCT, many of these studies have reported significant improvements in parents’ responsive interactive style as well as increases in children’s social engagement. However, the majority of these studies have failed to examine how intervention changes for parents and children are causally associated with improvements in children’s development and functioning. Such analyses are critical for addressing questions and concerns about the underlying logic models of RBIs, particularly because of the marked differences of this approach from the evidenced based behavioral interventions that dominate contemporary early intervention practice for children with ASD.
Recently, two investigations reported mediational analyses that examined potential causal pathways for RBIs. In an evaluation of a social pragmatics communication intervention, Aldred et al. (2012) reported that changes in parental responsiveness partially mediated intervention effects on children’s ADOS communication and social domain algorithm. Karaaslan and Mahoney (2015) investigated child development outcomes from an RBI called Responsive Teaching [RT (Mahoney and MacDonald 2007)]. A two-step mediation analysis indicated that although changes in parental responsiveness mediated the effects of RT on child development, the effects of responsiveness were mediated by intervention changes in children’s engagement. Thus although RT promoted developmental change by promoting highly responsive parental interactions, it was the effects of this style of interaction on children’s engagement that was directly associated with children’s developmental improvements.
Autism Severity
All subjects in the original PLAY RCT were assessed with the ADOS-generic (ADOS-G) to determine their diagnostic classification. After pretest data collection had been completed, the revised ADOS-2 was published (Lord et al. 2012). This version includes an algorithm for standardized calibrated severity scores (CSS) which minimize the effects of several child characteristics that are not defining characteristics of autism such as children’s age, language ability and race. However, since the PLAY randomization was initially done using diagnostic classifications that were based on research derived cut points for the ADOS-G (Lord et al. 1994), replacing ADOS-G scoring with the CSS algorithm would have invalidated the initial randomization because many participants would have been in different diagnostic groups or would have been disqualified from the study. As a result, CSS scores were not used for that study and children were classified as having autism or ASD both at pre and post intervention based upon the ADOS-G criteria.
Even though standardized CSS scores provide a more reliable and valid index of autism severity, these scores still pose challenges to assessing changes in severity over time because they combine symptoms from the Social Affect (SA) and Restricted and Repetitive Behavior (RRB) domains of the ADOS. These domains are not only purported to be independent dimensions of autism, but may also have unique developmental trajectories that respond differently to psychosocial or medical interventions. To address this problem, Hus et al. (2014) recently developed separate algorithms for calibrating CSS scores for each of these ADOS domains that can be used to evaluate changes in these two components of autism.
Purpose and Hypotheses
The purpose of this investigation was to conduct secondary analyses of the data from the PLAY RCT (Solomon et al. 2014) to investigate the mechanisms underlying PLAY treatment effects on children’s autism severity as measured by SA and RRB CSS scores. To conduct this analysis we first re-examined the effects of PLAY on autism severity as measured by CSS scores. We then investigated whether significant changes in children’s autism severity as measured by CSS scores were mediated both by the intervention changes in parents’ style of interaction as well as by children’s social interactive engagement.
Four hypotheses were tested in this study. First we hypothesized that the PLAY effects on children’s autism severity that were observed using ADOS-G criteria would continue to be evident using Social Affect and Restrictive and Repetitive Behavior CSS scores. Second, since PLAY intervention strategies were designed specifically to enhance children’s social engagement, we hypothesized that intervention changes in parents’ style of interaction would mediate PLAY effects on children’s social engagement. Third, consistent with results reported by Aldred et al. (2012), we hypothesized that improvements in children’s autism severity would be mediated by the changes in parents’ style of interaction, particularly as reflected by increases in responsiveness. Fourth, as postulated by Greenspan and Weider (1997) we hypothesized that the effects of parenting style on children’s autism severity would be mediated by PLAY intervention effects on children’s social engagement.
Methods
Subjects
Families were recruited from April 2010 to June 2012 through local physician offices in four cities in the U.S. (Detroit, MI; Peoria-Bloomington, IL: Billings, MT; Evansville, IN), and referred for enrollment to four Easter Seals sites in those cities, respectively. Two consecutive cohorts participated for 1 year each. Inclusion criteria were age 3:0–5:11 (actual 2 years 8 months–5 years 11 months) at the time of intervention; previous clinical diagnosis of Pervasive Developmental Disorder (PDD) according to DSM-IV criteria, and meeting criteria for autism or ASD on the Autism Diagnostic Observation Schedule (ADOS) (Lord et al. 2000) and Social Communication Questionnaire (SCQ) (Rutter et al. 2003). Exclusion criteria included a diagnosis of Asperger’s Disorder (due to the low incidence of this condition at this age), genetic disorders, severe medical conditions, a parent with severe psychiatric disorder or cognitive impairment, and/or families in which English was not the primary language. The Peabody Picture Vocabulary Test—Fourth Edition (Dunn and Dunn 2007) was used to screen parents for cognitive functioning that would permit understanding of the intervention processes, with a minimum requirement of 6th-grade vocabulary. Easter Seals administrators obtained written informed consent. Of the 148 families screened, 128 met criteria and chose to participate, but only 112 completed the study.
Table 1 displays child and family demographic characteristics by group for subjects who completed the study. At baseline, children’s average age was around 50 months (range 32–71 months). In accordance with the prevalence of autism, the majority of children were male. About one-quarter were African-American, Asian, and/or Hispanic. Most were from two-parent families, with more than half reporting family incomes under $60,000 (U.S. median income in 2011 was $51,100). Most primary parents (responsible for participating in the intervention) were mothers. About half of primary parents had Bachelor’s degrees.
Randomization
De-identified demographic and diagnostic data for enrolled families were sent to an independent research team for randomization to community-standard intervention (CS) or PLAY plus CS. Randomization occurred within sites using a matched-pair design with primary blocking variables of age (≤4.49 vs. ≥4.5 years), ADOS-G related autism categories (autism vs. autism spectrum) and child gender. Each group was allocated 64 families. Retention over the study year was 89.0 % of PLAY families and 85.9 % of control families for a total of 112 families. Retained and non-retained families did not differ significantly on any demographic or outcome variables.
Intervention Procedures
The PLAY Project Home Consultation (PLAY) program is a well-established clinical model (Solomon et al. 2007) that operationalizes the DIR theoretical framework (Greenspan and Weider 1998). PLAY typically supplements existing services (e.g. special education, language and occupational therapies, and/or ABA/behavioral interventions) but has also been implemented as a primary intervention for children with ASD under 3 years of age.
Treatment Group Six PLAY consultants who were occupational therapists, language therapists, or special educators and employed by Easter Seals were trained to certification. Consultants provided the standard PLAY Project intervention consisting of a 3-h home visit monthly for 12 months (M visits = 11.5, SD = .8). Before the first visit, parents received written and DVD-based training materials that described PLAY principles, methods, activities, and techniques. During all subsequent visits, consultants obtained a 15-min representative sample of coached parent play and consultant modeling during the visit. Parents learned to sensitively interpret the child’s subtle and hard to detect cues, respond contingently to the child’s intentions, and effectively engage the child in reciprocal exchanges. Parents were also taught to provide appropriate developmental challenges to promote progress in the child’s functional development as defined by Greenspan and Weider’s six functional emotional developmental levels (Greenspan and Weider 1998). A written video analysis, sent between visits, reviewed the parent–child video interactions, summarized the child’s developmental profile, and recommended methods and techniques for improvement. The program was revised over time to address the child’s evolving developmental profile. Consultants were available between visits as needed by email or phone. Families were encouraged to engage their child in 15–20-min play sessions and throughout daily routines for a total of 2 h/day. Parents completed monthly logs of time spent using PLAY methods with their child as well as hours of CS interventions.
Control Group CS children participated in special education public pre-school (12 h/week on average), as well as approximately 100 h/year of private speech and language therapies. Participation in other intensive interventions (i.e., at least 10 h/week) made families ineligible because of the potential confound with PLAY; one family from each group was removed for this reason. Two families from the CS group chose to pay for PLAY services and were dropped from the study.
Measures
Data were collected prior to randomization and 12 months later. Easter Seals site administrators collected demographic data for the child and family at the screening visit including age, gender, race, and family composition. ADOS evaluators were trained to research reliability. The ADOS was administered in Easter Seals offices and evaluators who were blinded to intervention status. In addition, they did not have any other involvement with the families outside of the assessment process including the provision of intervention services. Other parent-report measures were completed by parents in the home, collected and reviewed for accuracy at Easter Seals offices. All observations were video recorded in the home, then scored by raters blinded to group and time assignment.
Autism Severity
The ADOS-G (Lord et al. 2000) assesses social and communication behaviors representing ASD and was administered by independent assessors in ES offices. Assessors administered either Module 1, for children who used little or no phrase speech, or Module 2, for children who used phrase speech but did not speak fluently. Seventy participants were administered ADOS Module 1 and 26 were administered Module 2 at both pre- and post-test. The remaining 16 participants were administered Module 1 at pre-test and Module 2 at post-test.
For this study, autism severity was calibrated from the raw totals of the ADOS SA and RRB domains. CSS (Hus et al. 2014) are based upon a 10 point scale: scores from 1 to 3 are in the “Nonspectrum” range; 4–5 are in the “ASD” range; and 6–10 in the “Autism” range. CSS scores are reported to be less influenced by child characteristics such as verbal IQ, nonverbal IQ, age and race than raw domain scores (Hus et al. 2014).
Parent and Child Interaction
Children and their mothers were video recorded while playing together for 7½ min with a set of developmentally appropriate toys at the beginning and completion of intervention. Mothers were instructed to play with their children as they typically do. Videotapes of these observations were coded two times by trained independent observers who were blinded to treatment allocation or to the time of the observation (i.e., pre/post). The Maternal Behavior Rating Scale (MBRS) was used to assess parents’ style of interaction; the Child Behavior Rating Scale (CBRS) was used to assess children’s interactive engagement.
Maternal Behavior Rating Scale
The MBRS (Mahoney 2008) is a 12 item global rating scale that assesses parents’ style of interacting with their children. This scale has been used extensively in research with parents of young children with disabilities and developmental risks, including children with autism (Diken and Mahoney 2013). Results from this research indicate that MBRS ratings of parents’ interactive style are associated with children’s rate of developmental growth (e.g., Mahoney et al. 1985; Kim and Mahoney 2005) and are sensitive to the effects of parent-mediated interventions (e.g., Karaaslan and Mahoney, 2015; Mahoney and Powell 1988; Mahoney and Perales 2003, 2005). The MBRS assesses four interactive style dimensions: Responsive/Child Oriented (3 items, α = .87 at baseline, .91 at follow-up); Affect/Animation (5 items, α = .85 at baseline, .89 at follow-up); Achievement Orientation (2 items, α = .22 at baseline, .58 at follow-up); and Directiveness (2 items, α = .64 at baseline, .53 at follow-up). Interrater reliability was assessed through intraclass correlations (ICCs) for 20 % of videos randomly selected and distributed over the time of the study. ICCs were .64 for Responsiveness/Child Oriented, .70 for Affect/Animation, .73 for Achievement Orientation, and .61 for Directiveness,
Child Behavior Rating Scale
The CBRS (Mahoney and Wheeden 1999a, b) includes seven global items that assess children’s engagement in social interaction. This scale has been used extensively in research with young children with disabilities including autism (Diken and Mahoney 2013) to assess children’s interactive behavior with their mothers and other adults (e.g., Kim and Mahoney 2005; Mahoney et al. 2007). It has been reported to be sensitive to the effects of RBI interventions (e.g., Mahoney and Perales 2003, 2005). The CBRS is comprised of 7 items that assess two interactive style dimensions for children: Attention (4 items, α = .88 at baseline, .89 at follow-up) and Initiation (3 items, α = .70 at baseline, .83 at follow-up). Interrater reliability was assessed through intraclass correlations (ICCs) for 20 % of videos randomly selected and distributed over the time of the study. ICCs for CBRS scales were .75 for Attention and .77 for Initiation.
Social Functioning
Functional Emotional Assessment Scale
The FEAS (Greenspan et al. 2001) is an observational instrument that was designed to assess children’s social emotional functioning. The FEAS has six levels and 34 items based on Greenspan’s six functional developmental levels (FDL) which assess the quality of children’s social engagement. They progress from simple attention (FDL 1) and engagement (FDL 2), to two-way, purposeful reciprocal exchanges (FDL 3), to problem solving gestures (FDL 4), and then the consistent use of words (FDL 5) leading to rich pretend play, emotional thinking, and complex interaction (FDL 6). Items are rated as 0 (not at all or very brief), 1 (present some of the time, observed several times), or 2 (consistently present, observed many times). Ratings were summed to compute scores. Higher raw scale scores indicate greater social emotional development.
A 15 min parent child observation conducted exclusively for the FEAS was video recorded at pre- and post-intervention. Children’s behavior was coded by raters blind to group allocation and assessment time. Internal consistency of the FEAS was .99 at pre-test and .95 at post-test. ICCs for interrater reliability for videos randomized over time were .95.
Results
Preliminary Analyses
A multivariate analysis of variance was conducted to investigate changes in ADOS CSS measures over intervention (Table 2). Results from this analysis indicated that while both groups of children showed significant decreases in autism severity during the course of intervention (p < .001), the overall effect of PLAY on total ADOS CSS scores was not significant (p > .05). However, univariate analyses indicated that PLAY resulted in a significant reduction of SA severity scores (p < .05) but not RRB scores.
Based upon these results, the following analyses examined whether the improvements in children’s SA characteristics observed in the PLAY RCT were mediated by the changes in parenting style and child social engagement that also occurred during intervention. For these analyses we created the variable SA improvement [(SA2 − SA1) × (−1)]. In addition, we used Time 2 measures to reflect changes in parenting style and child engagement that occurred during intervention, since these measures reflect the level of these behaviors as observed at T1 in addition to the behavioral changes that occurred during intervention.
Correlations were computed to examine the relationship between parenting style and child engagement with SA Improvement as well as the inter-relationships among these variables. As indicated on Table 3, two of the four MBRS variables, responsive and affect, as well as children’s CBRS and the FEAS total scores were significantly correlated with SA Improvement (ps <.01). There was a strong correlation between the two child variables (rCBRS-FEAS = .72, p < .01), suggesting that these variables assessed a common underlying construct. Each of these child variables was significantly associated with all of the MBRS subscales (ps <.01) with the exception of achievement.
These results were used to reduce the number of variables to be included in the mediation analyses. First, the MBRS ‘achievement’ and ‘directiveness’ subscale scores were eliminated because of their nonsignificant associations with SA Improvement. Second, the MBRS ‘responsive’ and ‘affect’ subscale items were reduced to a single variable using a principle component analysis. As depicted on Table 4 this component, Responsive/Affect, accounted for 67 % of the variance of these items and loaded positively on all responsive and affect scale items.
Tests for Mediation
Because of the strong correlation between the CBRS and FEAS, separate mediational analyses were conducted with these two social engagement measures. The first set of analyses examined whether the effects of PLAY on children’s social engagement were mediated by parents’ Responsive/Affect component at Time 2 using the Baron and Kenny (1986) test for mediation. This approach tests whether the proposed mediator mediates the effect of the Treatment (PLAY) on the outcome (CBRS/FEAS). Table 5 reports a sequence of multivariate regression analyses testing this effect. Step 1 tests the effects of PLAY on the CBRS (Step 1a) and FEAS (Step 1b); Step 2 tests the effects of PLAY on the mediator, Responsive/Affect. Step 3 tests the effects of PLAY on the outcomes, CBRS (Step 3a) and FEAS (Step 3b), in the presence of the mediator, Responsive/Affect.
Results from these analyses indicated the following. First, (Step 1a) there was a large effect of Treatment on CBRS [B = .77 (.16), p = .000] and (Step 1a) a moderate effect of PLAY on FEAS [B = 6.11 (2.25), p = .008]. Second, (Step 2) there was a large effect of Treatment on the hypothesized mediator, Responsive/Affect [B = 1.01 (.16), p = .000]. Third, simultaneous entry of the hypothesized mediator, Responsive/Affect, and Treatment into the model predicting CBRS (Step 3a) produced a reduction in the coefficient of the Treatment effect on CBRS which was non-significant. Similarly entry of the hypothesized mediator and Treatment into the model predicting FEAS (Step 3b) produced a reduction in the coefficient of the Treatment effect on FEAS which was also non-significant. Overall, results reported in Step 3 are consistent with the hypothesis that Responsive/Affective mediated the effects of Treatment on children’s social engagement. 93 % of the Treatment effect on CBRS is explained by the change in Responsive/Affect; while 84 % of the Treatment effect on FEAS is explained by the change in Responsive/Affect.
The second set of analyses examined whether the effects of PLAY on children’s Social Affect were mediated by parents’ Responsive/Affect as well as by children’s social engagement. Using the Baron and Kenny (1986) approach, we conducted a two-step mediational analyses in which we first tested the mediating effects of Responsive/Affect and we next examined the simultaneous mediating effects of Responsive/Affect and children’s social engagement as assessed either by the CBRS or the FEAS on SA Improvement.
Table 6 reports the sequence of multivariate regression analyses that were used to test this effect. Step 1 tests the effects of Treatment on SA Improvement. Step 2 tests the effects of Treatment on the first mediator, Responsive/Affect. Step 3 tests the effects of Treatment on the second mediator, child social engagement as assessed by the CBRS (3a) or the FEAS (3B). Step 4 tests the effects of Treatment on SA Improvement in the presence of the mediator Responsive/Affect. Step 5 tests for the effects of Treatment on SA Improvement in the presence of two potential mediators, Responsive/Affect and child engagement.
Results indicated: (Step 1) a small effect of Treatment on SA Improvement [B = 1.54 (.79), p = .042]; (Step 2) a large effect of Treatment on the first hypothesized mediator, Responsive/Affect [B = 1.05 (.16), p = .000]; and (Step 3) large effects of Treatment on the second hypothesized mediator child social engagement as measured both by the CBRS [B = .77 (.16), p = .000] and FEAS [B = 6.11 (2.25), p = .008]. (Step 4) Simultaneous entry of the hypothesized mediator Responsive/Affect and Treatment into the model predicting SA Improvement indicated that Responsive/Affect was a significant mediator that resulted in a substantial reduction in the coefficient of the Treatment effect on SA Improvement. (Step 5) Simultaneous entry of the two hypothesized mediators Responsive/Affect and Child Engagement indicated that children’s social engagement significantly reduced the effects of both Treatment and Responsive/Affect on SA Improvement. More than 90 % of the coefficient effects of both Treatment and Responsive/Affect were mediated by the CBRS; while 78 % of the coefficient effects for Treatment and 55 % of the effects of Responsive/Affect were mediated by the FEAS. For both sets of Step 5 analyses, neither the effects of Treatment nor Responsive/Affect were significant indicating that PLAY intervention effects on SA Improvement were mediated by Treatment effects on children’s social engagement.
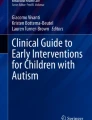
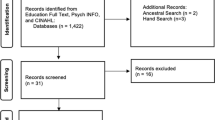
Figures 1 and 2 summarize the findings reported above. As indicated on both figures results from mediational analyses indicated that the intervention effects of PLAY were compatible with each of the three hypothesized mediational effects. First intervention changes in parents’ style of interaction (i.e., Responsive/Affect) mediated PLAY effects on children’s social engagement as measured either by the CBRS (Fig. 1) or the FEAS (Fig. 2)]. Second, PLAY effects on children’s SA Improvement were mediated by intervention changes in Responsive/Affect (Note this effect is indicated by Betas having a superscript of 2). Third, the effects of Responsive/Affect on SA Improvement were mediated by intervention changes in children’s social engagement as measured both by the CBRS (Fig. 1) or FEAS (Fig. 2) (Note: this effect is indicated by Betas having a superscript of 3). These results depict a model of developmental change in which the changes in parents’ interactive style (i.e., Responsive/Affect) that were promoted by PLAY were indirectly associated with improvements in children’s Social Affect because of the impact that Responsive/Affect had on children’s social engagement as assessed either by the CBRS (Fig. 1) or FEAS (Fig. 2).

Summary of meditational analyses of treatment effects on CBRS and social affective improvement. 1Beta without potential mediators; 2Beta with one mediator (responsive/non-direct component); 3Beta with two mediators (responsive/non-direct component and CBRS); *p < .01; **p < .001

Summary of meditational analyses of treatment effects on FEAS and social affective improvement. 1Beta without potential mediators; 2Beta with one mediator (responsive/non-direct component); 3Beta with two mediators (responsive/non-direct component and FEAS); *p < .01; **p < .001
Discussion
This secondary analysis was conducted to investigate two issues related to the effects of the PLAY Project on autism severity. First, it reexamined the PLAY RCT using ADOS CSS to determine the effects of PLAY on the severity of children’s SA and RRB disorders. Second, it conducted mediation analyses to determine the mechanisms by which PLAY resulted in reductions in autism severity. In general, there were two major findings from this investigation.
Severity of Autistic Characteristics
Although the original PLAY RCT indicated that PLAY resulted in significant improvements in children’s ADOS-G autism classification (Solomon et al. 2014), analyses using ADOS CSS scores provided a different and perhaps more accurate picture of PLAY intervention effects. PLAY did not result in an overall reduction in autism severity as measured by CSS scores. However, this was primarily attributable to the finding that PLAY had no effect on the severity of children’s RRBs. Nonetheless, there was a significant effect of PLAY on the severity of children’s SA disorders, and the magnitude of this effect was comparable to the size of the effect of PLAY previously reported for children’s ADOS-G classification (Solomon et al. 2014).
Insofar as CSS scores are less affected by non-autistic characteristics of children such as their age and language ability than are ADOS-G diagnostic criteria, differences between PLAY Treatment effect findings using CSS versus the ADOS_G criteria are compatible with criticisms that ADOS-G classifications may be unduly affected by characteristics of children that are not specifically associated with autism. Nevertheless, the contrasting PLAY effects for children’s SA as versus their RRB disorders not only refines our understanding of the effects of PLAY, but also reinforces the notion that autism is a complex disability that likely includes two or more semi-autonomous behavioral disorders which may have unique developmental trajectories and responses to treatment (Hus et al. 2014).
DIR was predicated on the notion that SA disorders constitute the primary, or core, characteristic of autism. Consistent with this notion DIR intervention strategies were designed primarily to address children’s social affect disorders. While DIR postulated that RRB disorders should improve as children make social affect improvements, the developers of this intervention emphasized the need for multiple complementary interventions, including social-behavioral and occupational therapy as well as pharmacological treatments, to adequately address the full scope of behavioral disorders associated with autism. Clearly results from this investigation underscore the possibility that RRB disorders require a different type of treatment protocol than do SA disorders.
Mechanism of Developmental Change
Despite the increasing evidence that RBIs can be effective at addressing the developmental needs of children with disabilities, there has long been skepticism regarding the value of this approach for children with autism. This skepticism has been fueled, in part, by the widespread belief that children with autism require directive interaction/instructional procedures to encourage them to perform, or attempt, behaviors that are contrary to their basic tendencies, as in the case of social engagement (Stahmer et al. 2005; Wong et al. 2014). It is further supported by evidence from descriptive studies which indicate that parents tend to be highly directive when their autistic children are not engaged in social interaction. Many interpret these findings as indicating that by becoming more directive parents are making necessary and appropriate accommodation to their children’s resistance to social interaction (e.g., Adamson et al. 2004; Kasari et al. 1988).
It is in this context that findings from our mediation analysis take on great importance. First, despite the propensity of children with autism to avoid or resist social interaction, parental interactions that were characterized by high levels of responsiveness/affect were strongly associated with children becoming more actively engaged in social interaction. In fact the parents who achieved the highest levels of responsiveness/affect by the end of intervention had children who displayed the highest levels of engagement. In addition, while our results indicated that parental directiveness was not associated with the quality of children’s engagement, still correlations indicating that the parents with the highest levels of directiveness displayed the lowest levels of responsiveness, seem to contradict the belief that directiveness is an effective or necessary interactive strategy for promoting children’s social engagement.
Results indicating that the effects of the Responsive/Affect interactive style promoted by PLAY on children’s SA disorders was mediated by the impact of this style of interaction on children’s social engagement are entirely consistent with the DIR theory which is the foundation for the PLAY. Given the apparent effectiveness of this interactive style at promoting children’s social engagement, it is not surprising that parents who routinely use this interactive style during daily routines and activities are actually teaching their children to develop the habit of social interaction. Over time this interactive pattern enhances children’s social competence thereby reducing the severity of their social affect disorders.
How Study Results Apply to CS Subjects and Others
Although the focus of this investigation was on the subjects who received PLAY, it is important to note that our findings also pertain to parents and children in the control group. SA improvements were not only observed for 74 % of the PLAY children, but for 51 % of the CS children as well. Since CS subjects did not receive PLAY or any other parent-mediated intervention, the design of this study points to the possibility that the improvements made by these subjects might be attributed to factors such as special education/related services, maturation, or to ADOS measurement error. While we are unable to rule out these factors, results from our mediation analyses indicate that the same pattern of improvements in parenting style and children’s social engagement that were associated with PLAY intervention effects also mediated the SA improvements made by CS children.
That is, even though pre–post changes in Responsive/Affect and child engagement were not significant for the CS group, there was considerable within group variability on these variables. More than 40 % of CS parents increased their Responsiveness/Affect, while 36 % of their children increased their social engagement as measured both by the FEAS and the CBRS. Our mediation analyses indicated that the effects of both Responsive/Affect and children’s social engagement on SA Improvement were substantially greater than were the treatment effects of PLAY. These results indicate that the changes made by CS subjects in Responsive/Affect and children’s social engagement were also associated with the SA improvements made by CS children.
Insofar as parental Responsive/Affect and child engagement can vary in other interventions for young children with ASD, results from this study raise the possibility that the mechanisms of developmental change identified in this study might be universal phenomena that affect children’s SA disorders across all interventions. This possibility points to the need for future research that examines whether or how parenting style and children’s social engagement are associated with child outcomes attained in any intervention, regardless of the types of procedures that are used and whether or not parents are actively involved.
Practical Implications
Since the SA improvements made by PLAY children were associated with improvements in social engagement that were promoted by increases in their parents’ Responsive/Affect, one of the major impediments to children benefitting from PLAY was the failure of their parents’ to make these interactive changes. Yet, the question remains why this might have occurred.
Parents’ failure to make the changes recommended in PLAY could be associated with a host of factors including: the way interventionists present information; parents having difficulty following through with PLAY suggestions either due to challenges associated with interacting with their children or other life circumstances; parents not believing that PLAY information and strategies were relevant to addressing their children’s developmental needs; as well as parents’ convictions that the manner they currently interact with their children is more beneficial than the recommendations provided in PLAY. Improvements in the efficiency of PLAY not only requires that professionals carefully monitor the effects of PLAY strategies on parents’ interactive style throughout the course of intervention, but also depends upon the development and evaluation of innovative methods for teaching PLAY strategies and encouraging parents to incorporate these strategies into their routine interactions with their children.
Limitations of Study
The PLAY RCT had a number of strengths, including a large sample from diverse communities, as well as a rigorous research design which included strong measures of fidelity of implementation which underscore the validity of the original findings. Although we concur that the CSS may provide a more accurate measure of autism severity than the ADOS-G, it is important to recognize that this assertion remains to be empirically evaluated. Post hoc changes in the primary study outcome measure to reassess original data is a significant limitation of this study, particularly insofar as it may have compromised our randomization procedures. As a result, future RBI research is needed which uses the CSS both to randomize subjects to treatments and to determine the replicability of results reported from this investigation.
References
Adamson, L. B., Bakeman, R., & Deckner, D. F. (2004). The development of symbol-infused joint engagement. Child Development, 75, 1171–1187.
Aldred, C., Green, J., Emsley, R., & McConachie, H. (2012). Brief report: Mediation of treatment effect in a communication intervention for pre-school children with autism. Journal of Autism and Developmental Disorders, 42, 447–454.
Baron, R. M., & Kenny, D. A. (1986). The moderator mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology, 31, 1173–1182.
Diken, O., & Mahoney, G. (2013). Interactions between Turkish mothers and preschool children with autism. Intellectual and Developmental Disabilities, 51, 190–200.
Dunn, L. M., & Dunn, D. M. (2007). Peabody picture vocabulary test (4th ed.). Circle Pines, MN: American Guidance Service.
Greenspan, S., DeGangi, G., & Wieder, S. (2001). Functional Emotional Assessment Scale. Bethesda, MD: Interdisciplinary Council on Developmental and Learning Disorders.
Greenspan, S. I., & Weider, S. (1998). The child with special needs: Encouraging intellectual and emotional growth. Cambridge, MA: DeCapo Press.
Greenspan, S. I., & Wieder, S. (1997). An integrated developmental approach to interventions for young children with severe difficulties in relating and communicating. Zero to Three, 17, 5–18.
Hus, V., Gotham, K., & Lord, C. (2014). Standardizing ADOS domain scores: Separating severity of social affect and restricted and repetitive behaviors. Journal of Autism and Developmental Disorders, 44, 2400–2412.
Karaaslan, O. & Mahoney, G. (2015). Mediational analyses of the effects of responsive teaching on the developmental functioning of preschool children with disabilities. Journal of Early Intervention, 37, 286–299.
Kasari, C., Sigman, M., Mundy, P., & Yirmiya, N. (1988). Caregiver interactions with autistic children. Journal of Abnormal Child Psychology, 16, 45–56.
Kim, J. M., & Mahoney, G. (2005). The effects of relationship focused intervention on Korean parents and their young children with disabilities. Research in Developmental Disabilities, 26, 101–201.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., et al. (2000). The autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30, 205–223.
Lord, C., Rutter, M., DiLavore, P. C., Risi, S., Gotham, K., & Bishop, S. (2012). Autism diagnostic observation schedule (2nd ed.). Torrance, CA: Western Psychological Services.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24, 659–685.
Mahoney, G. (2008). The Maternal Behavior Rating Scale-Revised. Cleveland, OH: Case Western Reserve University.
Mahoney, G. J., Finger, I., & Powell, A. (1985). The relationship between maternal behavioral style to the developmental status of mentally retarded infants. American Journal of Mental Deficiency, 90, 296–302.
Mahoney, G., Kim, J. M., & Lin, C. S. (2007). The pivotal behavior model of developmental learning. Infants and Young Children, 20, 311–325.
Mahoney, G., & MacDonald, J. (2007). Autism and developmental delays in young children: The Responsive Teaching curriculum for parents and professionals. Austin, TX: PRO-ED.
Mahoney, G., & Nam, S. (2011). The parenting model of developmental intervention. In R. M. Hodapp (Ed.), International review of research on mental retardation (Vol. 41, pp. 73–125). New York, NY: Academic Press.
Mahoney, G., & Perales, F. (2003). Using relationship-focused intervention to enhance the social-emotional functioning of young children with autism spectrum disorders. Topics in Early Childhood Special Education, 23(2), 77–89.
Mahoney, G., & Perales, F. (2005). A comparison of the impact of relationship-focused intervention on young children with pervasive developmental disorders and other disabilities. Journal of Developmental and Behavioral Pediatrics, 26, 77–85.
Mahoney, G., & Powell, A. (1988). Modifying parent–child interaction: Enhancing the development of handicapped children. Journal of Special Education, 22, 82–96.
Mahoney, G., & Wheeden, C. A. (1999a). The effect of teacher style on interactive engagement of preschool-aged children with special learning needs. Early Childhood Research Quarterly, 14, 51–68.
Mahoney, G., & Wheeden, C. A. (1999b). The effect of teacher style on interactive engagement of preschool-aged children with special learning needs. Early Childhood Research Quarterly, 14, 51–68.
McCollum, J. A., & Hemmeter, M. L. (1997). Parent–child interaction intervention when children have disabilities. In M. J. Guralnick (Ed.), The effectiveness of early intervention (pp. 549–576). Baltimore: Brookes.
McDuffie, A., & Yoder, P. (2010). Types of parent verbal responsiveness that predict language in young children with autism spectrum disorder. Journal of Speech, Language, and Hearing Research, 53, 1026–1039.
Rutter, M., Bailey, A., Berument, S. K., et al. (2003). Social Communication Questionnaire (SCQ). Los Angeles, CA: Western Psychological Services.
Sameroff, A. (2010). A united theory of development: A dialectic integration of nature and nurture. Child Development, 81, 6–22.
Siller, M., & Sigman, M. (2002). The behaviors of parents of children with autism predict the subsequent development of their children’s communication. Journal of Autism and Developmental Disorder, 32, 77–89.
Siller, M., & Sigman, M. (2008). Modeling longitudinal change in the language abilities of children with autism: Parent behaviors and child characteristics as predictors of change. Developmental Psychology, 44, 1691–1704.
Solomon, R., Necheles, J., Ferch, C., et al. (2007). Pilot study of a parent training program for young children with autism: The PLAY project home consultation program. Autism, 11, 205–224.
Solomon, R., Van Egeren, L., Mahoney, G., Quon-Huber, M., & Zimmerman, P. (2014). PLAY Project home consultation intervention program for young children with autism spectrum disorders: A randomized controlled trial. Journal of Developmental and Behavioral Pediatrics, 35, 475–485.
Stahmer, A. C., Collings, N. M., & Plankos, L. A. (2005). Early intervention practices for children with autism: Descriptions from community providers. Focus on Autism and Other Developmental Disabilities, 20, 66–79.
Trivette, C. (2003). Influence of caregiver responsiveness on the development of children with or at-risk for developmental disabilities. Bridges, 1, 1–13.
Warren, S. F., & Brady, N. C. (2007). The role of maternal responsivity in the development of children with intellectual disabilities. Mental Retardation and Developmental Disabilities Research Reviews, 13(4), 330–338.
Wong, C., Odom, S., Hume, K., Cox, A. W., Fettig, A., Kucharczyak, S., et al. (2014). Evidence based practices with children, youth and young adults with autism spectrum disorder. Chapdpcel Hill, NC: Frank Porter Graham Publications.
Acknowledgments
This investigation was supported by a National Institute of Mental Health (NIMH) and Small Business Innovation Research (SBIR) grant (Grant No. 2 R44 MH078431-02A1). It is a secondary analysis of a previously published investigation: “Solomon R, Van Egeren L, Mahoney G, Quon-Huber M, Zimmerman P. (2014). PLAY Project Home Consultation Intervention Program for Young Children with Autism Spectrum Disorders: A Randomized Controlled Trial. Journal of Developmental and Behavioral Pediatrics, 35(8): 475–485”.
Author Contributions
RS conceived the randomized control trial and directed all aspects of the original study including the study design, subject recruitment and randomization, intervention, assessments, and data management. GM conceptualized this secondary analysis, conducted data analyses, and drafted the manuscript. Both authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mahoney, G., Solomon, R. Mechanism of Developmental Change in the PLAY Project Home Consultation Program: Evidence from a Randomized Control Trial. J Autism Dev Disord 46, 1860–1871 (2016). https://doi.org/10.1007/s10803-016-2720-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-016-2720-x