
Abstract
Higher-functioning participants with and without autism spectrum disorder (ASD) viewed a series of face stimuli, made decisions regarding the affect of each face, and indicated their confidence in each decision. Confidence significantly predicted accuracy across all participants, but this relation was stronger for participants with typical development than participants with ASD. In the hierarchical linear modeling analysis, there were no differences in face processing accuracy between participants with and without ASD, but participants with ASD were more confident in their decisions. These results suggest that individuals with ASD have metacognitive impairments and are overconfident in face processing. Additionally, greater metacognitive awareness was predictive of better face processing accuracy, suggesting that metacognition may be a pivotal skill to teach in interventions.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is characterized by impairments in social communication and interaction, as well as restricted and repetitive behaviors and interests (American Psychiatric Association 2013). While much research has examined social impairments in ASD (e.g., Baron-Cohen et al. 2001; Hileman et al. 2011), only two research studies have assessed metacognitive awareness of social impairments in ASD (Sawyer et al. 2014; Wilkinson et al. 2010). Metacognitive awareness of social impairments may be a critical first step for successful social skill interventions (e.g., Verhoeven et al. 2012). In order to show substantial social skill improvements, it may be necessary for individuals to monitor their social performance, recognize when they are uncertain about a social situation or have made a mistake in a social situation, and act appropriately to gather more information about the social situation or acknowledge and make amends for any social mistakes that occurred during that social situation. Given the sparse research in this area, the goal of the current study was to examine metacognitive awareness of social impairments in ASD. Specifically, we examined metacognitive awareness of face processing in higher-functioning children and adolescents with ASD.
Metacognition
There are two distinct components of metacognition: knowledge of cognition and regulation of cognition (e.g., Jacobs and Paris 1987; Schraw 1998; Schraw and Dennison 1994). Knowledge of cognition is the ability to appraise one’s own cognition and is further divided into declarative knowledge (knowing about learning techniques and one's abilities), procedural knowledge (knowing how to employ learning techniques), and conditional knowledge (knowing why and when to employ learning techniques; e.g., Jacobs and Paris 1987; Schraw 1998; Schraw and Dennison 1994). Regulation of cognition is the ability to manage and control one’s cognitive learning and performance. Regulation of cognition can be further divided into at least three skill sets: planning (selecting learning techniques and allocating resources appropriately to reach a cognitive goal), monitoring (being aware of and assessing one’s learning and performance), and evaluation (analyzing one’s performance and learning efficiency after a task; e.g., Jacobs and Paris 1987; Schraw 1998; Schraw and Dennison 1994). The current study focuses on the regulation of cognition, specifically monitoring one’s performance on a face processing task.
Metacognition and Performance
Several studies have shown that metacognition is predictive of cognitive performance, at least partially independent of intelligence (e.g., van der Stel and Veenman 2008, 2010). Many of these studies, using different cognitive tasks (e.g., math problem solving, foreign language achievement) and different populations (e.g., secondary school students, adult learners of English), have assessed the contributions of both intelligence and metacognition to cognitive performance and have found metacognition to be a stronger predictor of performance than intelligence (e.g., Pishghadam and Khajavy 2013; Veenman et al. 2005; Veenman and Spaans 2005).
The research literature on metacognition of social skills is less well-established than the research literature on metacognition of cognitive skills. Several studies show that individuals with typical development display metacognitive awareness of face processing, as indicated by the relation between confidence ratings and accuracy on face processing tasks (e.g., Kelly and Metcalfe 2011; Watier and Collin 2011, 2012). In their study, Kelly and Metcalfe (2011) further showed that, on one of two face processing tasks given to university students, better metacognitive awareness was associated with better performance. Thus, although the literature in this area is limited, the initial research suggests that metacognition may be predictive of performance on social information processing tasks, just as metacognition is predictive of performance on cognitive tasks.
Metacognition in Autism Spectrum Disorder
Given that metacognition shows significant relations with both cognitive and social performance, metacognition may be a promising intervention platform for individuals with ASD and may be particularly relevant to examine in ASD. While the initial studies in this area examined metacognition in participants with ASD and a comorbid intellectual disability (e.g., Farrant et al. 1999a, b), more recent studies have examined metacognition in higher-functioning individuals with ASD (Grainger et al. 2014; Sawyer et al. 2014; Wilkinson et al. 2010; Wojcik et al. 2011, 2013; 2014).
Several of these recent studies examine metacognition in response to nonsocial stimuli in higher-functioning individuals with ASD, with some studies suggesting intact metacognition (Wojcik et al. 2011, 2013, 2014) and other studies suggesting impaired metacognition (Grainger et al. 2014; Wojcik et al. 2013). For example, Wojcik et al. (2011) administered a series of tasks that involved following instruction sequences to higher-functioning children and adolescents with and without ASD. There were no differences in the abilities of individuals with and without ASD to accurately judge their performance on this task, suggesting intact metacognition in ASD. Conversely, Grainger et al. (2014) presented word pairs to higher-functioning adults with ASD and asked them to predict whether they would later recognize the missing target word. Participants with ASD predicted their memory performance above chance, but their predictions were less accurate than those of participants with typical development, suggesting impaired metacognition in ASD.
Studies by Wilkinson et al. (2010) and Sawyer et al. (2014) are of particular relevance to the current paper because they examine metacognition in response to social stimuli, specifically faces, in higher-functioning individuals with ASD. In Wilkinson et al. (2010), higher-functioning children, adolescents, and adults with and without ASD studied a series of faces, completed a recognition task in which they identified each face as new or old, and rated their confidence in their memory judgment for each face. Compared to children and adolescents with typical development, those with ASD were less accurate when “certain” and more accurate when “guessing” in their face processing decisions, indicating a weaker relation between confidence and accuracy and less well developed metacognitive skill in children and adolescents with ASD. Adults with ASD showed more evidence of differential face processing accuracy across confidence ratings than children and adolescents with ASD, which may indicate that metacognitive awareness improves with age. Sawyer et al. (2014) asked higher-functioning adults with and without ASD to complete a social task in which they selected emotions corresponding to face stimuli and a nonsocial task in which they selected answers corresponding to general knowledge questions. On each task item, participants were asked to decide how confident they were that they had selected the correct answer and whether or not to submit their answer to contribute to their overall performance score. Across both tasks, participants with and without ASD did not show significant differences in the relation between confidence and accuracy. However, participants with ASD showed marginal impairments in metacognitive control (i.e., withholding incorrect responses and submitting correct responses) on the emotion recognition task and were significantly more likely to submit all answers across both tasks, further suggesting impairments in metacognitive control. Overall, while the current research on metacognition in ASD is mixed, both studies that have examined metacognition of social stimuli, specifically faces, in ASD have shown some evidence of impairments in this area, particularly for children and adolescents (Sawyer et al. 2014; Wilkinson et al. 2010).
Face Processing in Autism Spectrum Disorder
The research literature suggests that individuals with ASD have impairments in their ability to process faces (see Harms et al. 2010 for a review). Many of these studies specifically suggest that individuals with ASD have difficulty recognizing emotions from faces (e.g., Baron-Cohen et al. 2001; Celani et al. 1999; Wallace et al. 2008); however, it is important to note that such impairments are not always seen on simple face processing tasks with higher-functioning individuals with ASD (e.g., Castelli 2005; Jones et al. 2011; Tracy et al. 2011).
There are several classic findings within the face processing and ASD literature that have been replicated across multiple studies, and two of these findings have particular relevance for the current study. The first finding suggests that individuals with ASD are better able to process inverted faces and/or show less decline in processing inverted versus upright faces compared to individuals with typical development. This finding has been supported by the behavioral (e.g., Hobson et al. 1988), eye-tracking (e.g., Falck-Ytter 2008), and electrophysiological (e.g., Hileman et al. 2011) research literature. Individuals with ASD may process faces in a more piecemeal fashion while individuals with typical development may process faces in a more holistic fashion. As such, face inversion may disrupt the face processing abilities of individuals with typical development to a greater extent than it disrupts the face processing abilities of individuals with ASD. The second finding of particular relevance to the current study suggests that individuals with ASD do not attend as closely to the eye region of the face and/or have more difficulty processing the eye region of the face compared to individuals with typical development (e.g., Baron-Cohen et al. 2001; Klin et al. 2002; Pelphrey et al. 2002). Individuals with ASD may rely on the mouth region for face processing to a greater extent than individuals with typical development (e.g., Klin et al. 2002; Neumann et al. 2006; Spezio et al. 2007).
Current Study
The primary goal of the current study was to assess metacognition of social stimuli, specifically metacognition of facial affect judgments, in higher-functioning children and adolescents with ASD. It is important to examine metacognition in later childhood and adolescence as this is a sensitive period in the development of metacognitive skills (e.g., Paulus et al. 2014; von der Linden and Roebers 2006; Weil et al. 2013). Similarly, it is important to examine metacognition in higher-functioning individuals with ASD as preliminary research suggests that metacognition and self-awareness may support intervention efficacy for individuals with ASD (e.g., Verhoeven et al. 2012).
Only two previous studies have examined metacognition of social stimuli in higher-functioning individuals with ASD (Sawyer et al. 2014; Wilkinson et al. 2010), so this study significantly extends our understanding of metacognition of social stimuli, specifically faces, in ASD. Additionally, only one study has previously examined metacognition of facial affect in ASD (Sawyer et al. 2014). The Sawyer et al. (2014) study examined metacognition of facial affect in adults with ASD, and to the authors’ knowledge, the current study is the first to examine metacognition of facial affect in children and adolescents with ASD. Finally, while Sawyer et al. (2014) examined whether overall task performance differed between participants who showed some metacognitive control on the emotion recognition task (i.e., withheld at least one response) and participants who did not show any metacognitive control (i.e., submitted all responses), the current study is the first to examine the relation between overall task performance and metacognitive monitoring (i.e., the within-person correlation between confidence and accuracy) in ASD. Metacognitive control, or the process of acting on one’s metacognitive skill, is contingent upon effective metacognitive monitoring, or the ability to discriminate between correct and incorrect decisions (Sawyer et al. 2014).
Considering the previous two studies on metacognition of face processing in ASD (Sawyer et al. 2014; Wilkinson et al. 2010), we hypothesized that metacognition would be impaired in participants with ASD compared to participants with typical development. In accordance with the metacognition and performance literature (e.g., Kelly and Metcalfe 2011; Pishghadam and Khajavy 2013; Veenman et al. 2005; Veenman and Spaans 2005), we further hypothesized that better metacognitive monitoring on the face processing task would be associated with better performance.
The secondary goal of the current study was to assess face-processing ability in higher-functioning children and adolescents with ASD when the face was revealed in a piecemeal fashion. By revealing the face in a piecemeal fashion, participants with and without ASD were constrained to use similar face processing styles, as each element of the face was likely processed in the order in which it was revealed. To the authors’ knowledge, this is one of the first studies (e.g., Wallace et al. 2008) to compare face processing in individuals with and without ASD by revealing the face in a piecemeal fashion, such that face processing style and scanpath are constrained to be relatively similar between diagnostic groups.
In congruence with the classic face processing literature (e.g., Baron-Cohen et al. 2001; Celani et al. 1999; Wallace et al. 2008), we hypothesized that participants with ASD would be less accurate in determining facial affect than participants with typical development. However, we also took note of the mixed literature in this area, such that several studies examining face processing in higher-functioning individuals with ASD have not found a significant impairment in emotion recognition ability (e.g., Castelli 2005; Jones et al. 2011; Tracy et al. 2011). Furthermore, we hypothesized that participants with ASD would be more accurate in processing inverted faces compared to participants with typical development (e.g., Falck-Ytter 2008; Hileman et al. 2011; Hobson et al. 1988) and participants with typical development would be more accurate in processing faces in which the eye region was revealed before the mouth region compared to participants with ASD (e.g., Baron-Cohen et al. 2001; Klin et al. 2002; Pelphrey et al. 2002).
Methods
Participants
Participants in this study were part of a larger study on self-monitoring in children and adolescents (ages 8–16 at time of enrollment) with ASD or typical development. For the larger study, participants with ASD were recruited from the University of Miami / Nova Southeastern University Center for Autism and Related Disabilities, and participants with typical development were recruited from local schools. In the initial screening for this study, participants were excluded from participation if they had a history of seizures, a genetic condition (e.g., Down Syndrome), a reading level below the second grade, psychotic symptoms, a previously abnormal EEG, or if they were nonverbal. Additionally, participants with ASD were required to have an ASD diagnosis from a community mental health professional, and participants with typical development could not have received such a diagnosis.
Thirty-two participants with ASD and 31 participants with typical development were recruited from the larger study to participate in the current study. All participants had to have a verbal IQ ≥ 70, as assessed by the Wechsler Intelligence Scale for Children—Fourth Edition (WISC-IV; Wechsler 2003). Additionally, all participants had to show variability in their confidence judgments on the face processing task administered in this study; participants who responded with the same degree of confidence to all face stimuli were excluded from the sample. As the current literature suggests that screening instruments may be less sensitive in identifying higher-functioning participants with ASD (e.g., Eaves et al. 2006; Papanikolaou et al. 2009; Schanding et al. 2012), participants with ASD were required to meet 2 of the following 3 diagnostic criteria: ≥7 on the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2002), ≥13 on the Social Communication Questionnaire (SCQ; Rutter et al. 2003), and ≥13 on the Autism Spectrum Screening Questionnaire (ASSQ; Ehlers et al. 1999). Participants with typical development were excluded from the sample if they met any of these cutoff scores. Due to these criteria, six participants were excluded from the sample: 4 participants with typical development met the diagnostic cutoff criteria for ASD on one measure and 2 participants with ASD did not show variability in their confidence judgments on the face processing task. In addition, a third participant with ASD was excluded from the sample, as this participant repeatedly requested to guess the affect of the face very early during the face stimulus presentation (only 1–2 segments of the face revealed) and as there was a related experimenter error in administering the study procedure.
Participants with z-scores greater than |3| on overall task confidence or overall task accuracy were considered to be outliers and excluded from the sample (e.g., Osborne 2010; Osborne and Overbay 2004). Z-scores were first computed for participants’ overall task confidence, and one participant with typical development was excluded from the sample. Z-scores were next computed for participants’ overall task accuracy, and one participant with ASD was excluded from the sample. Finally, the four oldest female participants with typical development were excluded from the sample for matching purposes.
The final sample for this study was composed of 28 participants with ASD (24 males) and 22 participants with typical development (16 males). Given that participants with ASD had to meet 2 of 3 diagnostic criteria, 25 participants met criteria on the ADOS, 26 participants met criteria on the SCQ, and 27 participants met criteria on the ASSQ. There were no significant differences between diagnostic groups on age, t(48) = 1.62, p = 0.11, verbal IQ, t(48) = 1.67, p = 0.10, performance IQ, t(48) = −0.64, p = 0.52, or gender distribution, χ 2 (1, N = 50) = 1.30, p = 0.25. See Table 1.
Measures
The following diagnostic and cognitive assessments were completed by participants as part of the larger study.
Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2002 ) In this semi-structured observational assessment, participants are evaluated in the areas of communication, reciprocal social interaction, imagination and creativity, and stereotyped behaviors and restricted interests. The ADOS has high reliability and validity and uses an algorithm that is both specific and sensitive in identifying individuals with ASD (Lord et al. 2000). In this study, ADOS Modules 3 (n = 15) and 4 (n = 35) were administered to participants.
Autism Spectrum Screening Questionnaire (ASSQ; Ehlers et al. 1999 ) In this 28-item questionnaire, parents rate their child’s behaviors as being the same, somewhat different, or different from the behaviors of other children. This measure has been validated against other assessments of behavioral disorders and shows good reliability (Ehlers et al. 1999).
Social Communication Questionnaire, Lifetime Form (SCQ; Rutter et al. 2003 ) In this questionnaire, parents report on their child’s reciprocal social interaction, communication, and repetitive and stereotyped patterns and behaviors. The SCQ was developed from the 40 critical items of the Autism Diagnostic Interview (ADI; Lord et al. 1994), has been validated by high correlations with the ADI, and shows good reliability (Berument et al. 1999).
Wechsler Intelligence Scale for Children–IV (WISC-IV; Wechsler 2003 ) Participants completed an abbreviated version of the WISC-IV (Vocabulary and Similarities Scales to index Verbal IQ, Block Design and Matrix Reasoning Scales to index Performance IQ). The WISC IV shows stable test–retest reliability and has been validated through associations with other intelligence scales (Williams et al. 2003).
Stimuli
The stimuli used in the current study were 56 color photographs of faces from the NimStim Face Stimulus Set (Tottenham et al. 2009). The face stimuli were divided into fourteen segments, with one segment containing the eye region of the face and another segment containing the mouth region of the face. Each face stimulus was presented in a piecemeal fashion, with one segment of the face stimulus revealed every second. Thus, after 14 s, all 14 segments of the face were revealed.
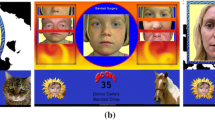
Faces varied on three key dimensions: affect, orientation, and order in which the facial features were revealed. Face stimuli depicted seven different emotions (angry, disgust, fear, happy, neutral, sad, and surprised), and each emotion was depicted eight times. Half of the face stimuli had an upright orientation, and half of the face stimuli had an inverted orientation. For half of the faces, the eyes were revealed early (the fourth segment) in the piecemeal process and the mouth was revealed late (the eleventh segment) in the piecemeal process (i.e., ‘eyes early’ faces). This order was reversed for the other half of the faces, such that the mouth was revealed early and the eyes were revealed late (i.e., ‘mouth early’ faces). See Fig. 1.

The piecemeal presentation of an upright face stimulus in which the mouth is revealed early and the eyes are revealed late. This face stimulus expresses the emotion fear
Procedure and Task
Participants completed two face processing tasks: a passive face processing task in which EEG/ERP data were collected (see Hileman et al. 2011) and an active face processing task in which behavioral data were collected. The current paper presents the results of the active face processing task.
In this task, face stimuli were presented in two blocks (upright faces and inverted faces) using PowerPoint software. The order in which the blocks were presented was counterbalanced across participants. Participants were asked to view the face stimuli as they were revealed and to guess the emotion of each stimulus as quickly and accurately as possible. When participants were ready to guess the emotion of a face, they were asked to pause the PowerPoint presentation with the computer mouse,Footnote 1 tell their affect selection to the experimenter, and indicate how confident they were in their affect selection on a scale from 1 (very unconfident) to 5 (very confident). Although these data are not presented in the current study, the face stimulus was then revealed in whole and participants had the opportunity to change or keep their current affect selection. If participants changed their affect selection, they were asked to provide a confidence rating for their new affect selection.
Data Analyses
Given that 50 participants viewed 56 faces, 2800 face trials were expected to be included in the data analyses. However, 99 trials were excluded: 38 trials were not completed (one participant was unable to finish the experimental protocol) and 61 trials were excluded due to equipment and/or experimenter error. Thirty-two participants had one or more trial excluded, and 2701 individual trials across participants were ultimately included in the data analyses.
Hierarchical Linear Modeling
Since face trials were nested within participants, two-level Hierarchical Linear Modeling (HLM) was used to analyze the data, with stimulus-specific variables (e.g., confidence, orientation) evaluated at Level 1 of the model and participant-specific variables (e.g., diagnosis, age) evaluated at Level 2 of the model. The estimation method used for these analyses was restricted maximum likelihood, and accuracy of affect selection was the dependent variable. As accuracy was a dichotomous variable (0 = inaccurate, 1 = accurate), a Bernoulli distribution was used. The unit-specific models without robust standard errors were interpreted. As suggested by Enders and Tofighi (2007), Level 1 variables were centered differently in the HLM model, depending on the research question. When assessing the main effects of Level 1 variables or interaction effects between Level 1 and Level 2 variables, Level 1 variables were centered within clusters (CWC). When assessing the main effects of Level 2 variables, Level 1 variables were centered at the grand mean (CGM).
As recommended by Raudenbush and Bryk (2002), a “step up” strategy was used for model building, rather than a “saturated” strategy. At each step of the model building process, a fixed effect and/or variance component was tested, such that only significant or marginally significant (p < 0.10) effects/components were retained in the model. In the first step of the model building process, fixed effects and variance components at Level 1 were examined. The variance component for the intercept and the effects of confidence (CWC), orientation (0 = upright, 1 = inverted), order in which the facial features were revealed (0 = ‘eyes early’ faces, 1 = ‘mouth early’ faces), and number of face segments revealed when the affect was selected (CWC) and their corresponding variance components were respectively assessed.
In the second step of the model building process, fixed effects for the intercept at Level 2 were examined. As Level 2 main effects were assessed in this step, non-dichotomous Level 1 variables that were retained in the model were CGM (Enders and Tofighi 2007). The effects of diagnosis (0 = typical development, 1 = ASD), age (CGM), verbal IQ (CGM), and gender (0 = male, 1 = female) were respectively assessed.
In the remaining steps of the model building process, fixed effects for the slopes for each of the Level 1 variables were examined. The effects of Level 2 variables (diagnosis, age, verbal IQ, and gender) on the slopes for each of the Level 1 variables (confidence, orientation, order of facial features, and number of face segments) that were retained in the model were respectively assessed. The model continued to be built in a stepwise fashion such that the fixed effects for the slopes were examined and finalized one by one, in the same order in which the Level 1 variables were entered into the model. As interaction effects between Level 1 and Level 2 variables were assessed in these steps, non-dichotomous Level 1 variables that were retained in the model were CWC (Enders and Tofighi 2007).
After the model was built, two final models were run. In Model 1, non-dichotomous Level 1 variables that were retained in the model were CWC.Footnote 2 This model was used to interpret the main effects of Level 1 predictors and the interaction effects between Level 1 and Level 2 predictors. In Model 2, non-dichotomous Level 1 variables that were retained in the model were CGM. This model was used to interpret the main effects of Level 2 predictors.
Hierarchical Linear Regression
In order to assess whether metacognition was associated with performance on the face processing task, overall task accuracy and metacognition were calculated for each participant. Overall task accuracy was operationalized as the number of face trials in which the participant correctly selected the affect out of the total number of face trials. Overall task metacognition was operationalized as the within-person Goodman–Kruskal gamma correlation between confidence and accuracy on all face trials (see Nelson et al. 2004 for a discussion on the use of this correlation in the metacognition literature). A hierarchical linear regression was conducted, such that overall task accuracy was the dependent variable, diagnostic group (0 = typical development, 1 = ASD), gender (0 = male, 1 = female), age (centered), and verbal IQ (centered) were entered as predictors in the first model, and overall task metacognition (centered) was entered as an additional predictor in the second model. All predictors in the first model were theoretically meaningful predictors, and thus these predictors were retained in the second model, regardless of their significance in the first model.
Results
See Table 1 for descriptive statistics for participants with and without ASD on overall task accuracy, confidence, number of face segments revealed when the facial affect was selected, and metacognition.
Hierarchical Linear Modeling
See Table 2 for a summary of Models 1 and 2. The results for the variance components are reported in Table 2, but these results are not discussed in the text. In addition, in order to simplify the text, the results are reported without explicitly indicating the variables that are controlled for in their interpretation. See Table 2 for a list of variables that are included in the models and are thus controlled for in the interpretation of the following effects.
Model 1
Participants were more likely to be correct in their affect selection when they had greater confidence in their affect selection, t(48) = 7.07, p < 0.01. This effect was qualified by an interaction between confidence and diagnostic group, t(48) = −3.46, p < 0.01, such that confidence was a stronger predictor of accuracy for participants with typical development than for participants with ASD. These results indicate that participants with typical development showed greater metacognitive awareness (i.e., a stronger relation between confidence and accuracy) on the face processing task than participants with ASD. See Fig. 2.

Predicted accuracy of affect selection across confidence levels for participants with ASD and typical development
Participants were less likely to be accurate in their affect selection on inverted faces compared to upright faces, t(2645) = −9.82, p < 0.01. Participants were also more likely to be correct in their affect selection of ‘mouth early’ faces compared to ‘eyes early’ faces, t(2645) = 2.49, p = 0.01. This effect was qualified by a marginal interaction between order of facial features and age, t(2645) = 1.70, p = 0.09, such that older participants showed a greater advantage in processing ‘mouth early’ faces than younger participants. See Fig. 3.

Predicted accuracy of affect selection across participant ages for ‘eyes early’ and ‘mouth early’ faces
Model 2
Participants with a higher verbal IQ were more likely to be correct in their affect selection, t(2645) = 2.77, p = 0.01.
Hierarchical Linear Regression
The first model marginally predicted task accuracy, F(4, 45) = 2.47, p = 0.06. The second model, ΔF(1, 44) = 3.15, p = 0.08, marginally predicted task accuracy above and beyond the first model. Thus, the second model was retained as the final model and predicted 24 % of the variance in task accuracy. In this model, participants with a higher verbal IQ, t(44) = 2.56, p = 0.01, and participants with an ASD diagnosis, t(44) = 2.15, p = 0.04, were significantly more accurate on the face processing task, and participants with greater overall task metacognition, t(44) = 1.78, p = 0.08, were marginally more accurate on the face processing task. Interestingly, diagnostic group was not a significant predictor of task performance in the first model, t(45) = 1.56, p = 0.13, and became a significant predictor of task performance in the second model, which controlled for the effects of overall task metacognition. See Table 3.
Post Hoc Analyses of Confidence Ratings
Given that there was a significant difference in the relation between confidence and accuracy for participants with and without ASD, we conducted a series of post hoc analyses to determine whether there were significant differences in how participants with and without ASD utilized the confidence scale. For each participant, we calculated the percentage of trials for which the person endorsed each confidence rating (1–5). A MANCOVA was used to evaluate the effects of diagnostic group (ASD vs. typical development) on the five dependent variables: percentage of ‘1’, ‘2’, ‘3’, ‘4’, and ‘5’ confidence ratings. Age, verbal IQ, and gender were included as covariates in the analyses. The MANCOVA assumption of parallel regression slopes was examined by testing for an interaction between diagnostic group and each of the covariates. The interaction effects did not reach significance, suggesting that the effects of the covariates were similar across diagnostic groups. Thus, the assumption of parallel regression slopes was met, and the interaction terms were removed from further analyses. As verbal IQ and gender did not have significant effects in any of the subsequent analyses, they were removed as covariates.
There was a significant multivariate effect for diagnostic group, F(4, 44) = 4.11, p = 0.01, η 2 p = 0.27, and age, F(4, 44) = 3.33, p = 0.02, η 2 p = 0.23. As such, the univariate main effects were examined for these variables. There was a significant effect of diagnostic group on percentage of ‘3’ confidence ratings, F(1, 47) = 10.92, p < 0.01, η 2 p = 0.19, and ‘4’ confidence ratings, F(1, 47) = 4.15, p = 0.05, η 2 p = 0.08, such that participants with typical development utilized these confidence ratings more often than participants with ASD. There was also a significant effect of diagnostic group on percentage of ‘5’ confidence ratings, F(1, 47) = 9.97, p < 0.01, η 2 p = 0.18, such that participants with ASD utilized this confidence rating more often than participants with typical development. See Fig. 4. Examining the univariate effects of age, there was a significant effect of age on percentage of ‘1’ confidence ratings, F(1, 47) = 8.27, p = 0.01, η 2 p = 0.15, such that younger participants utilized this confidence rating more often than older participants. There was also a marginal effect of age on percentage of ‘3’ confidence ratings, F(1, 47) = 3.78, p = 0.06, η 2 p = 0.07, such that older participants utilized this confidence rating more often than younger participants.

The percentage of responses given by participants with typical development and ASD for each confidence rating
Post Hoc Analyses of Number of Face Segments Revealed
Although number of face segments revealed did not have an effect on face processing accuracy in the final model, it did have a marginal effect on face processing accuracy during the model-building process. As such, we conducted a series of post hoc analyses to determine whether participants with typical development and ASD differed in the average number of face segments revealed when guessing the affect of the face stimuli. An ANCOVA was performed with diagnostic group (ASD vs. typical development) as the between-subjects variable and age, gender, and verbal IQ as covariates. The assumption of parallel regression slopes was examined by testing for an interaction between diagnostic group and each of the covariates. The interaction effects did not reach significance, such that the assumption was met and the interaction terms were removed from further analyses. As none of the covariates had a significant effect in subsequent analyses, they were removed as covariates. In the final analysis, there was a significant effect of diagnostic group on number of face segments revealed, F(1, 48) = 13.84, p < 0.01, η 2 p = 0.22, such that participants with ASD waited until more face segments were revealed before guessing the affect of the face compared to participants with typical development.
Summary of Results
Confidence in one’s face processing decision significantly predicted accuracy across all participants, but the relation between confidence and accuracy was stronger for individuals with typical development than individuals with ASD. All participants were more likely to be accurate when processing upright faces compared to inverted faces, and all participants, particularly older participants, were more likely to be accurate when processing ‘mouth early’ faces compared to ‘eyes early’ faces. Participants with a higher verbal IQ had greater accuracy on the face processing task. Overall, greater task metacognition marginally predicted better task performance, above and beyond the effects of diagnostic group, gender, age, and verbal IQ. Better task performance was also significantly associated with a higher verbal IQ and an ASD diagnosis. Participants with ASD more frequently used the ‘5’ (very confident) rating and less frequently used the ‘4’ (confident) and ‘3’ (somewhat confident, somewhat unconfident) ratings compared to participants with typical development. Younger participants more frequently used the ‘1’ (very unconfident) rating and marginally less frequently used the ‘3’ rating compared to older participants. Finally, in comparison to participants with typical development, participants with ASD waited until more face segments were revealed before guessing the affect of the face.
Discussion
Effects of Participant Characteristics on Performance
In this study, higher verbal IQ was associated with greater accuracy on the face processing task. This result is consistent with previous literature indicating that better emotion recognition ability is associated with higher IQ scores (e.g., Golan and Baron-Cohen 2006; Jones et al. 2011; Pallett et al. 2014; Wright et al. 2008). Although face processing is often referred to as an effortless and automatic process for individuals with typical development (e.g., Meaux et al. 2014; Remington et al. 2012), this result indicates that cognitive resources were implicated and utilized in the current face processing task. As this face processing task involved identifying the emotions of 56 faces as quickly and accurately as possible and as the piecemeal presentation of the face stimuli disrupted holistic face processing strategies, performance on this task may have demanded cognitive resources (e.g., ability to process information quickly, ability to sustain attention to task stimuli) to a greater extent than face processing in a naturalistic setting. In addition, participants with a higher verbal IQ may have been helped by the use of inner speech, or internal self-talk, to guide and regulate their behavioral choices on this face processing task.
In the HLM analysis, there were no direct effects of diagnostic group, age, or gender on face processing accuracy. While we had predicted that individuals with typical development would be more accurate on this task than individuals with ASD, the current null finding fits well with more recent literature suggesting that higher-functioning individuals with ASD are proficient at simple face processing tasks (e.g., Castelli 2005; Jones et al. 2011; Tracy et al. 2011). In addition, this null finding may be partially due to the piecemeal presentation of faces in the current study; this presentation style may have conferred a face processing advantage on participants with ASD, who tend to use more piecemeal face processing strategies, and a face processing disadvantage on participants with typical development, who tend to use more holistic face processing strategies (e.g., Dawson et al. 2005).
Although diagnostic groups did not differ in face processing accuracy, individuals with ASD did wait until more face segments were revealed before selecting an affect, suggesting that they may require more processing time and/or more facial cues to achieve the same face processing accuracy as individuals with typical development. Given that more processing time and more facial cues were confounded in this study design, it is not clear how each of these factors uniquely affected and contributed to face processing for individuals with ASD. Previous research has both indicated that individuals with ASD may experience delays in face processing (e.g., Batty et al. 2011; Hileman et al. 2011; O’Connor et al. 2005) and may perform better on face processing tasks that provide more facial cues (e.g., O’Connor et al. 2007; Wilson et al. 2007), such that both of these factors may have influenced face processing in the current study. Overall, the lack of diagnostic group differences on face processing accuracy indicates that determining facial affect, at the time selected by the participant, was of similar difficulty for both participants with and without ASD; as such, any diagnostic group differences in metacognition on this task cannot be attributed to differences in task difficulty.
Effect of Confidence on Performance: Examining Metacognition
Across all participants, greater confidence was associated with greater accuracy. Age, verbal IQ, and gender did not have a significant effect on the relation between confidence and accuracy. However, diagnosis did have a significant effect, such that participants with typical development had a stronger relation between confidence and accuracy than participants with ASD, and diagnosis was therefore included as a predictor of this relation in the final HLM model. This result is consistent with our hypothesis and replicates the results of Wilkinson et al. (2010). While Sawyer et al. (2014) did not find a differential relation between confidence and accuracy across diagnostic groups, the authors did find diagnostic group differences in participants’ use of metacognitive control (i.e., submitting correct responses and withholding incorrect responses). Together, these studies suggest that metacognition of face processing, specifically facial affect, is impaired in individuals with ASD, and this impairment may be reflective of a broader impairment in social metacognition or domain general metacognition in ASD.
Interestingly, even though the HLM analysis indicated that participants with and without ASD did not have any differences in accuracy on the face processing task, participants with ASD did have more difficulty monitoring their performance on this task. This result was also observed in the Wilkinson et al. (2010) study and is reminiscent of neuroimaging findings in which individuals with and without ASD have similar behavioral performance on face processing tasks but different neural activation patterns (e.g., Wang et al. 2004; Weng et al. 2011). Even when individuals with and without ASD do not show behavioral differences in face processing accuracy, there seem to be important neural and metacognitive differences in face processing between these two groups.
A metacognitive impairment in face processing in ASD, or a more general metacognitive impairment in social processing in ASD, may make it difficult for individuals with ASD to detect when a face processing or social processing error has been made. If a person is unaware that a social error has been made (e.g., monopolizing a conversation), that person is unlikely to change his/her behavior or make amends for the error (e.g., ask the other person questions about his/her interests, apologize to the other person). In addition, when a person is unaware that a social error has been made, that person is likely to continue making the same social error over and over again.
Although individuals with ASD showed impairments in metacognition on this task, it is important to note that metacognition was not absent for individuals with ASD. Individuals with ASD did show a relation between confidence and accuracy, albeit a reduced relation compared to individuals with typical development. Furthermore, in this task, the face stimuli were slowly revealed in a piecemeal fashion, and participants were asked to guess the emotion of each face stimulus as quickly and accurately as possible. Thus, participants were required to continually monitor their awareness of the emotion of the face and decide when they had gathered enough information to make a decision regarding that emotion. As participants with typical development and ASD did not show any differences in face processing accuracy on this task, it suggests that participants with ASD were sufficiently aware of their social cognitive processing to ascertain when they were ready to make a decision regarding affect. Indeed, participants with ASD tended to wait longer to make a decision regarding affect than participants with typical development.
Post hoc analyses were conducted to determine how participants utilized the confidence ratings for this task. While participants with and without ASD did not show any differences in accuracy on this task, participants with ASD were significantly more confident in their performance. Overconfidence may cause individuals with ASD to devote less effort and attention to a task, as they are already confident in their performance on that task; the allocation of fewer cognitive resources to the task may therefore lead to underperformance on the task (e.g., Dunlosky and Rawson 2012; Stone 1994). Furthermore, overconfidence in performance can lead to a greater sense of failure and dissatisfaction with negative outcomes (McGraw et al. 2004). Individuals with ASD are at risk for elevated internalizing problems (e.g., Hammond and Hoffman 2014; Hurtig et al. 2009; Simonoff et al. 2008), and individuals who are overconfident in their social performance may be at greater risk for depression and/or anxiety if they experience social rejection. As such, overconfidence in ASD may have negative effects above and beyond impaired metacognition.
Age also influenced how participants utilized the confidence ratings for this task. While age did not affect accuracy, younger participants were significantly less confident in their performance than older participants. Younger participants have less experience processing faces than older participants, so it is likely that this effect is reflective of face processing expertise. In general, individuals with a lot of experience on a given task (i.e., experts) are more confident in their performance than individuals with a little experience on that task (i.e., novices; Hallin et al. 2009).
Effects of Face Stimulus Characteristics on Performance
We hypothesized that participants with typical development would be less accurate in processing inverted faces and more accurate in processing ‘eyes early’ faces compared to participants with ASD. Neither of these diagnostic group effects were observed in the current study. All participants, regardless of diagnostic group, were more accurate in processing upright faces compared to inverted faces and ‘mouth early’ faces compared to ‘eyes early’ faces. As face stimuli were revealed in a piecemeal fashion, all participants may have engaged in piecemeal face processing, regardless of their intuitive face processing style. Given that face processing styles and scanpaths were constrained to be relatively similar across participants with and without ASD, diagnostic group differences that may have otherwise existed may have been obscured on this task. For example, if the face stimuli had not been revealed in a piecemeal fashion, individuals with typical development may have used a more holistic face processing style, potentially leading to greater accuracy in processing upright faces and less accuracy in processing inverted faces. The face stimuli used in this task were static and depicted simple emotions; inversion and order of facial features may have yielded differential diagnostic group effects on more complex face processing tasks.
In the literature, the eye region of the face is generally considered to be more important for face processing than the mouth region of the face (e.g., Baron-Cohen et al. 1997; Pelphrey et al. 2002). Thus, in the current study, it was surprising to find that all participants were more accurate in processing ‘mouth early’ faces than ‘eyes early’ faces. This result is consistent with a recent study (Blais et al. 2012) which indicates that the mouth region of the face is more informative than the eye region for processing basic emotions. The eye region of the face may be most important for processing complex facial expressions, such that participants may have been more accurate in processing ‘eyes early’ faces if more complex facial expressions had been used in this task. However, the mouth region may be most important, yet underappreciated, for processing basic facial expressions. Additionally, this study suggests that the mouth region of the face may become easier to process with development, such that older children and adolescents are better able to extract affective information from the mouth region of the face than younger children.
As the mouth region of the face may be more informative for processing simple facial expressions than the eye region (Blais et al. 2012) and as individuals with ASD seem to have a propensity toward mouth processing (e.g., Klin et al. 2002; Neumann et al. 2006; Spezio, et al. 2007), it may be useful to develop face processing interventions for individuals with ASD that primarily focus on the mouth region of the face. Although such an intervention approach may be unorthodox, the mouth region of the face is arguably just as or more informative than the eye region of the face and appears to be a natural area of focus for individuals with ASD. In an eye-tracking study, Klin et al. (2002) found that greater fixation on the mouth region of the face was associated with more social adaptation and less autistic social impairment, suggesting that the ability to process emotions from the mouth region of the face is associated with positive social skills in individuals with ASD. Furthermore, Tanaka et al. (2010) demonstrated that the ability to process emotions from the mouth region of the face is amenable to intervention in children and adolescents with ASD.
Relation Between Metacognition and Performance
Greater metacognition on the face processing task predicted better performance on this task, above and beyond the effects of diagnostic group. This result is consistent with our hypothesis, as well as the literature on metacognition and performance (Kelly and Metcalfe 2011; Pishghadam and Khajavy 2013; Veenman et al. 2005; Veenman and Spaans 2005), and highlights the importance of attending to individual differences in metacognition across individuals with typical development and ASD. Given the results of this study, metacognition appears to be a stronger predictor of face processing ability than diagnostic group. This result is reminiscent of the cognitive performance literature (Pishghadam and Khajavy 2013; Veenman et al. 2005; Veenman and Spaans 2005), in which metacognition often emerges as a stronger predictor of cognitive performance than intelligence. Together, these studies underscore the importance of metacognition in predicting social and cognitive performance; individual differences in metacognition appear to be a key predictor of individual differences in performance that should be considered alongside other more intuitive predictors of performance, such as diagnostic group and intelligence.
Interestingly, diagnostic group did not emerge as a significant predictor of face processing ability in the first regression model, but it did emerge as a significant predictor of face processing ability in the second regression model, controlling for the effects of metacognition. In this second model, ASD diagnosis is actually predictive of better face processing skills, a result that is contrary to much of the face processing literature which suggests that ASD diagnosis is associated with worse face processing skills (e.g., Baron-Cohen et al. 2001; Celani et al. 1999; Wallace et al. 2008). This surprising result may further indicate that metacognition is a stronger predictor of poor face processing performance than ASD diagnosis, such that ASD diagnosis may not be predictive of poor face processing performance above and beyond the effects of metacognition. However, as diagnosis did not have a significant effect on face processing accuracy in the HLM analysis, which accounted for the nested structure of the data and controlled for multiple participant- and stimulus-level variables, this unexpected result should be interpreted with caution.
Limitations and Future Directions
In this study, faces were revealed in a piecemeal fashion, which constrained individuals with and without ASD to have similar face processing styles. However, this method of stimulus presentation also made it more difficult to process the face stimuli holistically. Individuals with typical development may use holistic face processing strategies to a greater extent than individuals with ASD (e.g., Dawson et al. 2005), thus this method of stimulus presentation may have conferred a face processing advantage on participants with ASD and a face processing disadvantage on participants with typical development. Additionally, this method of face presentation may have obscured diagnostic group differences in face processing that would have otherwise been observed. Given the piecemeal presentation of the face stimuli, participants were instructed to navigate the computer mouse to a ‘pause’ button on the computer screen, pause the stimulus presentation, and tell their affect selection and confidence rating to the experimenter. Methodologically, this process may have introduced minor delays between when the participant cognitively decided to pause the stimulus presentation and actually paused the stimulus presentation. In the future, it would be best to streamline this process, such that the touch of a button (without navigating to a specific point on screen) pauses the stimulus presentation.
The results of this study suggest that participants with ASD are impaired in metacognitive awareness and are overconfident in their responses on a face processing task. However, there may be alternative explanations for the results observed in this study. Participants with ASD may have had difficulty comprehending the requirements of the face processing task. However, given that there were no significant differences in IQ or face processing accuracy between participants with and without ASD, such an explanation seems unlikely. Participants with ASD may also have had difficulty differentiating between their response and their confidence in their response; participants may have provided their best guess for each affect and therefore placed full confidence in their response. In other words, since participants provided their best guess regarding affect, it may have seemed contradictory or confusing for them to then indicate that they were not confident in their affect selection. Such an explanation may still be consistent with an impairment in metacognition in ASD, albeit at a more basic level than has heretofore been discussed. However, this explanation again seems unlikely, as participants with ASD were able to monitor their awareness of the affect of the face and decide when they had gathered enough information to make an affective decision.
The face stimuli employed in the current study were static and displayed simple emotions; the metacognitive and face processing results of this study may have been different if dynamic face stimuli or face stimuli depicting more complex emotions had been used. Future research should examine the relation between metacognition and task difficulty (e.g., utilizing dynamic face stimuli or complex emotions) in participants with ASD. Metacognitive impairments may increase with task difficulty, such that participants with ASD may have experienced greater metacognitive impairments on a more complex face processing task.
Longitudinal studies are needed to more clearly ascertain the causal relation between metacognition and task performance, as well as the effects of development on metacognition. While this study proposes that metacognition is predictive of task performance, task performance may also be predictive of metacognition. It may be easier to monitor performance on high-performing tasks compared to low-performing tasks. Additionally, while age did not emerge as a significant predictor of metacognition in the current study, the research literature suggests that there may be developmental effects on metacognition. Wilkinson et al. (2010) observed greater metacognitive impairments for facial memory in children and adolescents with ASD compared to adults with ASD. Also, this study examined metacognition of facial affect in children and adolescents with ASD and showed greater metacognitive impairments than the Sawyer et al. (2014) study, which examined metacognition of facial affect in adults with ASD. As such, a longitudinal study would help to clarify the influence of development on metacognition.
Only two previous studies have examined metacognition in response to social stimuli in individuals with ASD (Sawyer et al. 2014; Wilkinson et al. 2010), and both of these studies, as well as the current study, specifically examined metacognition in response to faces. More research is needed to ascertain metacognitive awareness of general social skills in ASD, and it would be useful to examine metacognition across multiple social domains, such as social cognitive tasks (e.g., Strange Stories; White et al. 2009) and social interactions with peers. While Sawyer et al. (2014) began an initial investigation of whether metacognition was differentially impaired in social versus nonsocial contexts, future research on more analogous social and nonsocial processing tasks is needed to further flesh out this comparison. Additionally, more research is needed to examine metacognition of non-social, cognitive skill sets, such as reading comprehension and math performance.
Although this study suggests that improvements in metacognition may be associated with positive outcomes (e.g., improved face processing performance), improvements in metacognition may also be associated with negative outcomes. Individuals with ASD often experience elevated symptoms of anxiety and/or depression (e.g., Hammond and Hoffman 2014; Hurtig et al. 2009; Simonoff et al. 2008), and awareness of one’s deficits, particularly in the social skills domain, may lead to increased internalizing problems (Kuusikko et al. 2008; Vickerstaff et al. 2007). Ignorance may indeed be bliss. For example, a child with ASD may be unpopular and have few friends at school. If this child perceives that he actually has many friends and is unaware of his low social status, it is unlikely that he will experience anxiety or depression due to his social status. However, if this same child perceives that he has no friends and is aware of his low social status, it is much more likely that he will experience anxiety or depression. Although the child’s social status and rate of peer rejection remain the same across both examples, the child’s awareness of his social status is different and may therefore affect the likelihood that he will experience internalizing problems. Future research should more fully assess whether improvements in metacognitive awareness of social skills and social status are associated with internalizing problems in children with ASD. Even if such associations do exist, improvements in metacognitive awareness may ultimately be instrumental and necessary for improving one’s social skills and social status.
This study suggests that metacognition may be a useful skill set to teach within the context of a social skill intervention, although such a skill set may need to be taught under the guidance of an experienced clinician or teacher in order to minimize the development of comorbid internalizing problems. It is important to note that teaching a social skill in an intervention setting is not akin to teaching metacognitive awareness of that social skill; as such, it may be necessary to explicitly teach both the social skill and metacognitive awareness of that social skill within the intervention context. Metacognitive awareness may be an important and pivotal skill set for participants with ASD to master, such that greater awareness of social skills may lead to better social performance. In addition, metacognition may be critical for improving generalization of social skills; the ability to monitor and evaluate one’s social performance in a new setting may be key for ultimately improving one’s social performance in that setting. Overall, metacognition appears to be a promising area for social skill intervention research, and future research should evaluate metacognition as a potential pivotal skill for increasing social and/or cognitive performance.
Notes
When deemed appropriate by the experimenter (e.g., participant had substantial attention difficulties), the experimenter controlled the computer mouse and paused the face stimulus presentation when requested by the participant.
Although number of face segments revealed did not have a significant or marginally significant effect in Model 1, it was retained in the model due to its prior marginal significance in the model-building process.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., & Plumb, I. (2001). The “reading the mind in the eyes” test revised version: A study with normal adults, and adults with asperger syndrome or high-functioning autism. Journal of Child Psychology and Psychiatry, 42(2), 241–251. doi:10.1111/1469-7610.00715.
Baron-Cohen, S., Wheelwright, S., & Jolliffe, T. (1997). Is there a “language of the eyes”? Evidence from normal adults, and adults with autism or asperger syndrome. Visual Cognition, 4(3), 311–331. doi:10.1080/713756761.
Batty, M., Meaux, E., Wittemeyer, K., Rogé, B., & Taylor, M. J. (2011). Early processing of emotional faces in children with autism: An event-related potential study. Journal of Experimental Child Psychology, 109(4), 430–444. doi:10.1016/j.jecp.2011.02.001.
Berument, S. K., Rutter, M., Lord, C., Pickles, A., & Bailey, A. (1999). Autism screening questionnaire: Diagnostic validity. British Journal of Psychiatry, 175, 444–451. doi:10.1192/bjp.175.5.444.
Blais, C., Roy, C., Fiset, D., Arguin, M., & Gosselin, F. (2012). The eyes are not the window to basic emotions. Neuropsychologia, 50(12), 2830–2838. doi:10.1016/j.neuropsychologia.2012.08.010.
Castelli, F. (2005). Understanding emotions from standardized facial expressions in autism and normal development. Autism, 9(4), 428–449. doi:10.1177/1362361305056082.
Celani, G., Battacchi, M. W., & Arcidiacono, L. (1999). The understanding of the emotional meaning of facial expressions in people with autism. Journal of Autism and Developmental Disorders, 29(1), 57–66. doi:10.1023/A:1025970600181.
Dawson, G., Webb, S. J., & McPartland, J. (2005). Understanding the nature of face processing impairment in autism: Insights from behavioral and electrophysiological studies. Developmental Neuropsychology, 27(3), 403–424. doi:10.1207/s15326942dn2703_6.
Dunlosky, J., & Rawson, K. A. (2012). Overconfidence produces underachievement: Inaccurate self evaluations undermine students’ learning and retention. Learning and Instruction, 22(4), 271–280. doi:10.1016/j.learninstruc.2011.08.003.
Eaves, L. C., Wingert, H. D., Ho, H. H., & Mickelson, E. R. (2006). Screening for Autism Spectrum Disorders with the Social Communication Questionnaire. Journal of Developmental and Behavioral Pediatrics, 27(Suppl2), S95–S103. doi:10.1097/00004703-200604002-00007.
Ehlers, S., Gillberg, C., & Wing, L. (1999). A screening questionnaire for asperger syndrome and other high-functioning autism spectrum disorders in school age children. Journal of Autism and Developmental Disorders, 29(2), 129–141. doi:10.1023/A:1023040610384.
Enders, C. K., & Tofighi, D. (2007). Centering predictor variables in cross-sectional multilevel models: A new look at an old issue. Psychological Methods, 12(2), 121–138. doi:10.1037/1082-989X.12.2.121.
Falck-Ytter, T. (2008). Face inversion effects in autism: A combined looking time and pupillometric study. Autism Research, 1(5), 297–306. doi:10.1002/aur.45.
Farrant, A., Blades, M., & Boucher, J. (1999a). Recall readiness in children with autism. Journal of Autism and Developmental Disorders, 29(5), 359–366. doi:10.1023/A:1023074726548.
Farrant, A., Boucher, J., & Blades, M. (1999b). Metamemory in children with autism. Child Development, 70(1), 107–131. doi:10.1111/1467-8624.00009.
Golan, O., & Baron-Cohen, S. (2006). Systemizing empathy: Teaching adults with Asperger Syndrome or high-functioning autism to recognize complex emotions using interactive multimedia. Development and Psychopathology, 18(2), 591–617. doi:10.1017/S0954579406060305.
Grainger, C., Williams, D. M., & Lind, S. E. (2014). Metacognition, metamemory, and mindreading in high-functioning adults with autism spectrum disorder. Journal of Abnormal Psychology, 123(3), 650–659. doi:10.1037/a0036531.
Hallin, C. A., Øgaard, T., & Marnburg, E. (2009). Exploring qualitative differences in knowledge sources: A study of hierarchical effects of judgmental confidence and accuracy performance. International Journal of Knowledge Management, 5(4), 1–25. doi:10.4018/jkm.2009062901.
Hammond, R. K., & Hoffman, J. M. (2014). Adolescents with high-functioning autism: An investigation of comorbid anxiety and depression. Journal of Mental Health Research in Intellectual Disabilities, 7(3), 246–263. doi:10.1080/19315864.2013.843223.
Harms, M. B., Martin, A., & Wallace, G. L. (2010). Facial emotion recognition in autism spectrum disorders: A review of behavioral and neuroimaging studies. Neuropsychology Review, 20(3), 290–322. doi:10.1007/s11065-010-9138-6.
Hileman, C. M., Henderson, H., Mundy, P., Newell, L., & Jaime, M. (2011). Developmental and individual differences on the P1 and N170 ERP components in children with and without autism. Developmental Neuropsychology, 36(2), 214–236. doi:10.1080/87565641.2010.549870.
Hobson, R. P., Ouston, J., & Lee, A. (1988). What’s in a face? The case of autism. British Journal of Psychology, 79(4), 441–453. doi:10.1111/j.2044-8295.1988.tb02745.x.
Hurtig, T., Kuusikko, S., Mattila, M., Haapsamo, H., Ebeling, H., Jussila, K., et al. (2009). Multi-informant reports of psychiatric symptoms among high-functioning adolescents with Asperger syndrome or autism. Autism, 13(6), 583–598. doi:10.1177/1362361309335719.
Jacobs, J. E., & Paris, S. G. (1987). Children’s metacognition about reading: Issues in definition, measurement, and instruction. Educational Psychologist, 22(3–4), 255–278. doi:10.1080/00461520.1987.9653052.
Jones, C. R. G., Pickles, A., Falcaro, M., Marsden, A. J. S., Happé, F., Scott, S. K., et al. (2011). A multimodal approach to emotion recognition ability in autism spectrum disorders. Journal of Child Psychology and Psychiatry, 52(3), 275–285. doi:10.1111/j.1469-7610.2010.02328.x.
Kelly, K. J., & Metcalfe, J. (2011). Metacognition of emotional face recognition. Emotion, 11(4), 896–906. doi:10.1037/a0023746.
Klin, A., Jones, W., Schultz, R., Volkmar, F., & Cohen, D. (2002). Visual fixation patterns during viewing of naturalistic social situations as predictors of social competence in individuals with autism. Archives of General Psychiatry, 59(9), 809–816. doi:10.1001/archpsyc.59.9.809.
Kuusikko, S., Pollock-Wurman, R., Jussila, K., Carter, A. S., Mattila, M., Ebeling, H., et al. (2008). Social anxiety in high-functioning children and adolescents with autism and asperger syndrome. Journal of Autism and Developmental Disorders, 38(9), 1697–1709. doi:10.1007/s10803-008-0555-9.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., DiLavore, P. C., et al. (2000). The autism diagnostic observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223. doi:10.1023/A:1005592401947.
Lord, C., Rutter, M., DiLavore, P., & Risi, S. (2002). Manual: Autism Diagnostic Observation Schedule. Los Angeles, CA: Western Psychological Services.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic Interview—Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24(5), 659–685. doi:10.1007/BF02172145.
McGraw, A. P., Mellers, B. A., & Ritov, I. (2004). The affective costs of overconfidence. Journal of Behavioral Decision Making, 17(4), 281–295. doi:10.1002/bdm.472.
Meaux, E., Hernandez, N., Carteau-Martin, I., Martineau, J., Barthélémy, C., Bonnet-Brilhault, F., et al. (2014). Event-related potential and eye tracking evidence of the developmental dynamics of face processing. European Journal of Neuroscience, 39(8), 1349–1362. doi:10.1111/ejn.12496.
Nelson, T. O., Narens, L., & Dunlosky, J. (2004). A revised methodology for research on metamemory: Pre-judgment recall and monitoring (PRAM). Psychological Methods, 9(1), 53–69. doi:10.1037/1082-989X.9.1.53.
Neumann, D., Spezio, M. L., Piven, J., & Adolphs, R. (2006). Looking you in the mouth: Abnormal gaze in autism resulting from impaired top-down modulation of visual attention. Social Cognitive and Affective Neuroscience, 1(3), 194–202. doi:10.1093/scan/nsl030.
O’Connor, K., Hamm, J. P., & Kirk, I. J. (2005). The neurophysiological correlates of face processing in adults and children with Asperger’s syndrome. Brain and Cognition, 59(1), 82–95. doi:10.1016/j.bandc.2005.05.004.
O’Connor, K., Hamm, J. P., & Kirk, I. J. (2007). Neurophysiological responses to face, facial regions and objects in adults with Asperger’s syndrome: An ERP investigation. International Journal of Psychophysiology, 63(3), 283–293. doi:10.1016/j.ijpsycho.2006.12.001.
Osborne, J. W. (2010). Data cleaning basics: Best practices in dealing with extreme scores. Newborn & Infant Nursing Reviews, 10(1), 37–43. doi:10.1053/j.nainr.2009.12.009.
Osborne, J. W., & Overbay, A. (2004). The power of outliers (and why researchers should always check for them). Practical Assessment, Research, and Evaluation, 9(6). Retrieved March 18, 2015 from http://PAREonline.net/getvn.asp?v=9&n=6
Pallett, P. M., Cohen, S. J., & Dobkins, K. R. (2014). Face and object discrimination in autism, and relationship to IQ and age. Journal of Autism and Developmental Disorders, 44(5), 1039–1054. doi:10.1007/s10803-013-1955-z.
Papanikolaou, K., Paliokosta, E., Houliaras, G., Vgenopoulou, S., Giouroukou, E., Pehlivanidis, A., et al. (2009). Using the autism diagnostic interview-revised and the autism diagnostic observation schedule-generic for the diagnosis of autism spectrum disorders in a Greek sample with a wide range of intellectual abilities. Journal of Autism and Developmental Disorders, 39(3), 414–420. doi:10.1007/s10803-008-0639-6.
Paulus, M., Tsalas, N., Proust, J., & Sodian, B. (2014). Metacognitive monitoring of oneself and others: Developmental changes during childhood and adolescence. Journal of Experimental Child Psychology,. doi:10.1016/j.jecp.2013.12.011.
Pelphrey, K. A., Sasson, N. J., Reznick, J. S., Paul, G., Goldman, B. D., & Piven, J. (2002). Visual scanning of faces in autism. Journal of Autism and Developmental Disorders, 32(4), 249–261. doi:10.1023/A:1016374617369.
Pishghadam, R., & Khajavy, G. H. (2013). Intelligence and metacognition as predictors of foreign language achievement: A structural equation modeling approach. Learning and Individual Differences, 24, 176–181. doi:10.1016/j.lindif.2012.12.004.
Raudenbush, S., & Bryk, A. (2002). Hierarchical linear models: Applications and data analysis methods (2nd ed.). Thousand Oaks: Sage Publications Inc.
Remington, A., Campbell, R., & Swettenham, J. (2012). Attentional status of faces for people with autism spectrum disorder. Autism, 16(1), 59–73. doi:10.1177/1362361311409257.
Rutter, M., Bailey, A., & Lord, C. (2003). Social Communication Questionnaire. Los Angeles, CA: Western Psychological Services.
Sawyer, A. P., Williamson, P., & Young, R. (2014). Metacognitive processes in emotion recognition: Are they different in adults with Asperger’s disorder? Journal of Autism and Developmental Disorders, 44(6), 1373–1382. doi:10.1007/s10803-013-1999-0.
Schanding, G. J., Nowell, K. P., & Goin-Kochel, R. P. (2012). Utility of the Social Communication Questionnaire-Current and Social Responsiveness Scale as teacher-report screening tools for autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(8), 1705–1716. doi:10.1007/s10803-011-1412-9.
Schraw, G. (1998). Promoting general metacognitive awareness. Instructional Science, 26(1–2), 113–125. doi:10.1023/A:1003044231033.
Schraw, G., & Dennison, R. S. (1994). Assessing metacognitive awareness. Contemporary Educational Psychology, 19(4), 460–475. doi:10.1006/ceps.1994.1033.
Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 921–929. doi:10.1097/CHI.0b013e318179964f.
Spezio, M. L., Adolphs, R., Hurley, R. S. E., & Piven, J. (2007). Abnormal use of facial information in high-functioning autism. Journal of Autism and Developmental Disorders, 37(5), 929–939. doi:10.1007/s10803-006-0232-9.
Stone, D. N. (1994). Overconfidence in initial self-efficacy judgments: Effects on decision processes and performance. Organizational Behavior and Human Decision Processes, 59(3), 452–474. doi:10.1006/obhd.1994.1069.
Tanaka, J. W., Wolf, J. M., Klaiman, C., Koenig, K., Cockburn, J., Herlihy, L., et al. (2010). Using computerized games to teach face recognition skills to children with autism spectrum disorder: The let’s face it! program. Journal of Child Psychology and Psychiatry, 51(8), 944–952. doi:10.1111/j.1469-7610.2010.02258.x.
Tottenham, N., Tanaka, J. W., Leon, A. C., McCarry, T., Nurse, M., Hare, T. A., et al. (2009). The NimStim set of facial expressions: Judgments from untrained research participants. Psychiatry Research, 168(3), 242–249. doi:10.1016/j.psychres.2008.05.006.
Tracy, J. L., Robins, R. W., Schriber, R. A., & Solomon, M. (2011). Is emotion recognition impaired in individuals with autism spectrum disorders? Journal of Autism and Developmental Disorders, 41(1), 102–109. doi:10.1007/s10803-010-1030-y.
van der Stel, M., & Veenman, M. V. J. (2008). Relation between intellectual ability and metacognitive skillfulness as predictors of learning performance of young students performing tasks in different domains. Learning and Individual Differences, 18(1), 128–134. doi:10.1016/j.lindif.2007.08.003.
van der Stel, M., & Veenman, M. V. J. (2010). Development of metacognitive skillfulness: A longitudinal study. Learning and Individual Differences, 20(3), 220–224. doi:10.1016/j.lindif.2009.11.005.
Veenman, M. V. J., Kok, R., & Blöte, A. W. (2005). The relation between intellectual and metacognitive skills in early adolescence. Instructional Science, 33(3), 193–211. doi:10.1007/s11251-004-2274-8.
Veenman, M. V. J., & Spaans, M. A. (2005). Relation between intellectual and metacognitive skills: Age and task differences. Learning and Individual Differences, 15(2), 159–176. doi:10.1016/j.lindif.2004.12.001.
Verhoeven, E. W. M., Marijnissen, N., Berger, H. J. C., Oudshoorn, J., van der Sijde, A., & Teunisse, J. P. (2012). Brief report: Relationship between self-awareness of real-world behavior and treatment outcome in autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(5), 889–894. doi:10.1007/s10803-011-1311-0.
Vickerstaff, S., Heriot, S., Wong, M., Lopes, A., & Dossetor, D. (2007). Intellectual ability, self-perceived social competence, and depressive symptomatology in children with high-functioning autistic spectrum disorders. Journal of Autism and Developmental Disorders, 37(9), 1647–1664. doi:10.1007/s10803-006-0292-x.
von der Linden, N., & Roebers, C. (2006). Developmental changes in uncertainty monitoring during an event recall task. Metacognition and Learning, 1(3), 213–228. doi:10.1007/s11409-006-9001-6.
Wallace, S., Coleman, M., & Bailey, A. (2008). An investigation of basic facial expression recognition in autism spectrum disorders. Cognition and Emotion, 22(7), 1353–1380. doi:10.1080/02699930701782153.
Wang, A. T., Dapretto, M., Hariri, A. R., Sigman, M., & Bookheimer, S. Y. (2004). Neural correlates of facial affect processing in children and adolescents with autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 43(4), 481–490. doi:10.1097/00004583-200404000-00015.
Watier, N. N., & Collin, C. A. (2011). Metamemory for faces, names, and common nouns. Acta Psychologica, 138(1), 143–154. doi:10.1016/j.actpsy.2011.05.017.
Watier, N., & Collin, C. (2012). The effects of distinctiveness on memory and metamemory for face–name associations. Memory, 20(1), 73–88. doi:10.1080/09658211.2011.637935.
Wechsler, D. (2003). Wechsler Intelligence Scale for Children (4th ed.). San Antonio, TX: Pearson.
Weil, L. G., Fleming, S. M., Dumontheil, I., Kilford, E. J., Weil, R. S., Rees, G., et al. (2013). The development of metacognitive ability in adolescence. Consciousness and Cognition: An International Journal, 22(1), 264–271. doi:10.1016/j.concog.2013.01.004.
Weng, S., Carrasco, M., Swartz, J. R., Wiggins, J. L., Kurapati, N., Liberzon, I., et al. (2011). Neural activation to emotional faces in adolescents with autism spectrum disorders. Journal of Child Psychology and Psychiatry, 52(3), 296–305. doi:10.1111/j.1469-7610.2010.02317.x.
White, S., Hill, E., Happé, F., & Frith, U. (2009). Revisiting the strange stories: Revealing mentalizing impairments in autism. Child Development, 80(4), 1097–1117. doi:10.1111/j.1467-8624.2009.01319.x.
Wilkinson, D. A., Best, C. A., Minshew, N. J., & Strauss, M. S. (2010). Memory awareness for faces in individuals with autism. Journal of Autism and Developmental Disorders, 40(11), 1371–1377. doi:10.1007/s10803-010-0995-x.
Williams, P., Weiss, L., & Rolfhus, E. (2003). Wechsler Intelligence Scale for Children–IV, technical report 2, psychometric properties. San Antonio, TX: The Psychological Corporation.
Wilson, R., Pascalis, O., & Blades, M. (2007). Familiar face recognition in children with autism: The differential use of inner and outer face parts. Journal of Autism and Developmental Disorders, 37(2), 314–320. doi:10.1007/s10803-006-0169-z.
Wojcik, D. Z., Allen, R. J., Brown, C., & Souchay, C. (2011). Memory for actions in autism spectrum disorder. Memory, 19(6), 549–558. doi:10.1080/09658211.2011.590506.
Wojcik, D. Z., Moulin, C. J. A., & Souchay, C. (2013). Metamemory in children with autism: Exploring “feeling-of-knowing” in episodic and semantic memory. Neuropsychology, 27(1), 19–27. doi:10.1037/a0030526.
Wojcik, D. Z., Waterman, A. H., Lestié, C., Moulin, C. A., & Souchay, C. (2014). Metacognitive judgments-of-learning in adolescents with autism spectrum disorder. Autism, 18(4), 393–408. doi:10.1177/1362361313479453.
Wright, B., Clarke, N., Jordan, J., Young, A. W., Clarke, P., Miles, J., et al. (2008). Emotion recognition in faces and the use of visual context in young people with high-functioning autism spectrum disorders. Autism, 12(6), 607–626. doi:10.1177/1362361308097118.
Acknowledgments
This research was supported by the National Institute of Mental Health (NIMH), through Grant R01MH071273, and the Institute of Education Sciences, U.S. Department of Education, through Grant DED-R305C050052. The authors thank Bridget Gamber, Annie Inge, Nicole Kojkowski, Leena Mohapatra, Crystal Noller, Agu Rossetti, Caley Schwartz, and Nicole Zahka for their contributions.
Authors Contributions
CM conceived of the study, led the execution of the study, performed the statistical analyses, and drafted the manuscript; HH participated in the interpretation of the data, helped to draft the manuscript, and was co-PI of the NIMH grant that supported this study; LN participated in the design and coordination of the study and helped to draft the manuscript; MJ participated in the coordination of the study and helped to draft the manuscript; PM participated in the design of the study, helped to draft the manuscript, and was co-PI of the NIMH grant that supported this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest in the current study.
Ethical Standards
This study was part of a larger study on self-monitoring in children and adolescents with ASD which was approved by the appropriate Institutional Review Board. Participants assented and parents consented to participation in the current study.
Additional information
The opinions expressed are those of the authors and do not represent views of NIH or the U.S. Department of Education.
Rights and permissions
About this article

Cite this article
McMahon, C.M., Henderson, H.A., Newell, L. et al. Metacognitive Awareness of Facial Affect in Higher-Functioning Children and Adolescents with Autism Spectrum Disorder. J Autism Dev Disord 46, 882–898 (2016). https://doi.org/10.1007/s10803-015-2630-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-015-2630-3