
Abstract
Little is known about outcomes for individuals with autism spectrum disorders (ASD) into adulthood. Several characteristics of individuals with ASD predict long-term outcomes, and the family environment may also play a role. The present study uses a prospective, longitudinal design to describe and predict trajectories of autism symptoms and maladaptive behaviors over 8.5 years in a large, community-based sample of adolescents and adults with ASD. Overall, autism symptoms and maladaptive behaviors were observed to improve over the study period. Above and beyond the adult’s gender, age, and level of intellectual disability, greater improvements were associated with higher levels of maternal praise (based on maternal speech samples) and higher quality mother–child relationships. Implications for future research and intervention are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) results in lifelong disability with pervasive impacts across multiple domains of development (American Psychiatric Association 2013). Once considered rare, ASD is now recognized as a commonly occurring condition whose prevalence was underestimated in the past (Fombonne 2001). ASD is now second only to intellectual disability (ID) as the most common serious developmental disability in the United States (Newschaffer et al. 2007), occurring in approximately one in 68 children nationwide (Centers for Disease Control 2014).
The growing rate of diagnosis of ASD (Charman 2002; Fombonne 2005) combined with an increasing life expectancy in the United States (Arias 2012), suggests that adults with ASD will constitute a population with growing significance. Little attention has been given either in research or policy to the prevalence, impact and needs associated with ASD in adulthood (Totsika et al. 2010). Most of the lifetime costs of ASD occur in adulthood (Ganz 2007), yet relatively little is known about optimizing outcomes during this period of development. Historically, outcomes for adults with ASD were poor (Levy and Perry 2011). Recent improvements in services, interventions, and community living supports for this population suggest the potential for better outcomes for adults with ASD living today. Health, social, residential and vocational outcomes for adults with ASD vary, but there is evidence that positive outcomes are attainable (Perkins and Berkman 2012).
Much of the research on adults with ASD has been limited to small samples, clinically-referred samples or specific subgroups of individuals with ASD (e.g., Asperger’s syndrome, high IQ). Moreover, there has been a reliance to date on cross-sectional comparisons and retrospective reports. Cross-sectional comparisons of individuals with ASD at different life stages may reflect differences in diagnostic practices, rather than true developmental processes (Seltzer et al. 2003). Comparisons of current symptoms and behaviors to those present in childhood based on retrospective reports also can be problematic (Henry et al. 1994), although reports of early childhood functioning are needed to make an autism diagnosis at any age. To address these limitations in past research, the present study uses a prospective, longitudinal design to describe and predict developmental trajectories of autism symptoms and maladaptive behaviors in a large, community-based sample of adolescents and adults with ASD.
Autism Symptoms in Adolescents and Adults with ASD
The first goal of the present study was to extend our understanding of frequency and change in the core symptoms diagnostic of autism, including impairments in social interaction, impairments in communication, and restricted, repetitive and stereotyped patterns of behavior, interests, and activities. Seltzer et al. (2004) reviewed the existing literature on change in core symptoms among individuals with Autistic Disorder over the life course. Studies reported age-related differences or changes in the severity of autism symptoms, with a general pattern of improvement with age. More recent studies have supported this general trend. McGovern and Sigman (2005) found reports of autism symptoms in young adulthood to be less severe than reports in early and middle childhood among 48 adults with autism. Esbensen and colleagues found restricted repetitive behaviors to be less frequent and less severe among older than younger individuals with ASD (Esbensen et al. 2009). Similarly, current ratings of restricted and repetitive behaviors and interests among 34 high IQ adults with ASD were significantly lower than retrospective lifetime ratings (Chowdhury et al. 2010).
Improvement in symptoms is often “splintered” across domains (Seltzer et al. 2004). For instance, greater improvements were reported for social and communication impairments than for repetitive behaviors and stereotyped interests based on retrospective reports from parents of children and adolescents with ASD (Fecteau et al. 2003). Moreover, improvement is not universal across individuals within studies. While many improve, some individuals with ASD show persistent or worsening autism symptoms into adulthood (Chowdhury et al. 2010; Fecteau et al. 2003; Piven et al. 1996). Despite a general trend of improvement with age, the majority of individuals diagnosed in childhood continue to meet criteria for ASD in adulthood (Billstedt et al. 2007; Howlin et al. 2004).
Certain characteristics of the individual with ASD may relate to symptom severity. Individuals with ASD and comorbid ID are generally reported to have worse outcomes in adulthood than their peers with ASD without ID (Lord and Bailey 2002; Seltzer et al. 2004; Shea and Mesibov 2005). Individuals with ASD and ID were found to display fewer lifetime reductions in social impairments, verbal communication, and repetitive behaviors and stereotyped interests in late adolescence and early adulthood than individuals without comorbid ID (McGovern and Sigman 2005). Among adults with ASD, lower IQ has shown a strong association with worse quality of social interaction, reciprocal communication and patterns of self-chosen activities (Billstedt et al. 2007) and worse linguistic outcomes (Mawhood et al. 2000). Lower language skills have been associated with worse functioning and a reduced likelihood of improvement over time (Howlin et al. 2004; Shea and Mesibov 2005). Gender may also play a role in symptom severity, although the findings are mixed (Howlin et al. 2004). Women with ASD have been reported to have more significant social impairment in adolescence (Tonge and Einfeld 2003), poorer quality social interactions in adulthood (Billstedt et al. 2007), and a pattern of downward vocational mobility in adulthood (Taylor and Seltzer 2012).
Maladaptive Behaviors in Adolescents and Adults with ASD
The second goal of the present study was to extend our understanding of frequency and change in maladaptive behaviors. Maladaptive behaviors are behaviors that interfere with everyday activities, including self-injurious behavior, withdrawal, uncooperative behavior, aggression, and destruction of property. The presence of ASD has been reported to be a significant risk factor for behavior problems among youth with ID (Brereton et al. 2006; Totsika et al. 2011). Into adulthood, the severity of ASD symptoms is related to the level of disruptive and self-injurious behaviors among adults with ID (Matson and Rivet 2008). A meta-analysis of 86 studies on challenging behavior in children and adults with ID found significantly higher levels of maladaptive behaviors among individuals with an ASD diagnosis, specifically self-injury, aggression, and disruption to the environment (McClintock et al. 2003).
There is a general pattern of improvement in maladaptive behaviors with age among individuals with ASD (Howlin 2005; Matson and Horovitz 2010; Shea and Mesibov 2005). Among adults with ASD, the prevalence of challenging and abnormal behaviors has been reported to reduce over time (Einfeld et al. 2006; Murphy et al. 2005; Totsika et al. 2010). Like autism symptoms, improvement was not universal across individuals. Gray et al. (2012) reported a general pattern of improvement in disruptive and self-absorbed behaviors in a sample of individuals with autism across 18 years, however some showed no change (23 %) or an increase in maladaptive behaviors (16 %) during this period.
For individuals with developmental disabilities, the presence of ID is associated with higher levels of behavior problems (Beadle-Brown et al. 2006; De Ruiter et al. 2008). Across studies of children and adults with ID, individuals with more severe ID had higher levels of maladaptive behaviors than individuals with moderate ID (McClintock et al. 2003). Among adults with ASD, those with moderate ID had higher levels of self-absorbed behaviors than those with mild ID (Gray et al. 2012). Greater maladaptive behaviors have been associated with lower language skills (Howlin et al. 2004; Shea and Mesibov 2005). Some researchers also suggest that maladaptive behaviors may be worse for females than males with ASD (Gillberg and Steffenburg 1987; Von Knorring and Hägglöf 1993), while others have found no gender differences (Kobayashi et al. 1992; Gray et al. 2012).
Positive Family Processes
Beyond the gender and ID status of the individual with ASD, aspects of the family environment may explain variability in adult outcomes. In the general literature, maternal positive affect and the quality of parent–child interactions have been predictive of child adaptation and functioning (Borkowski et al. 2001; Bornstein 2006; Landry et al. 2006). The quality of the parent–child relationship is an important factor for adjustment into young adulthood among families with typically developing children (Overbeek et al. 2007). There is growing empirical support that family processes are also predictive of outcomes for individuals with intellectual and developmental disabilities across the life course (Esbensen et al. 2013; McCarthy and Boyd 2001; Smith et al. 2008).
Less attention has been given to the importance of positive family processes within families of individuals with ASD. Findings from longitudinal studies suggest that parent behaviors can influence aspects of functioning among individuals with ASD, from early toddlerhood through adulthood (Baker et al. 2010, 2011; Greenberg et al. 2006). Positive family processes, such as parent warmth and close parent–child relationships have been associated with improved outcomes for individuals with diverse developmental risks (Caspi et al. 2004; López et al. 2004; Smith et al. 2008; Tully et al. 2004). There is a need to examine the impact of positive family processes and relationships on change in symptoms and behaviors among adults with ASD.
The Adolescents and Adults with Autism Study
In a previous study based on our ongoing research, we examined changes in autism symptoms and maladaptive behaviors in 241 adolescents and adults with ASD during a 4.5 year period (Shattuck et al. 2007). Autism symptoms and maladaptive behaviors improved significantly across domains, with the exception of repetitive behaviors and stereotyped interests. Cross-sectional and lagged regressions were used to predict initial levels and change in symptoms and behaviors. With respect to autism symptoms, older adults had higher levels of impairment in non-verbal communication but lower levels of repetitive behaviors and stereotyped interests at the start of the study. Adults with comorbid ID had significantly higher levels of autism symptoms across domains at the start of the study and less improvement over the course of the study. Concerning maladaptive behaviors, older adults had significantly fewer externalized, asocial and total maladaptive behaviors at the start of the study and greater declines across domains over the course of the study. Conversely, adults with ID had more externalized, asocial and total maladaptive behaviors at the start of the study and fewer improvements across domains. In this study, there was evidence of both improvement and stability in core symptoms of ASD and associated problem behaviors, with only a small sub-sample showing evidence of worsening of the behavioral phenotype. Notably, this study did not examine social environmental factors as potential predictors and the period of time was only 4.5 years.
In a separate study, we examined the role of mother–child relationship quality, warmth and praise as predictors of autism symptoms and behavior problems among 149 adolescents and adults with ASD co-residing with their mothers (Smith et al. 2008). Using a cross-lagged panel design over an 18-month period, a higher quality mother–child relationship predicted lower levels of subsequent externalized and internalized behaviors as well as fewer impairments in reciprocal social interactions and repetitive behaviors and stereotyped interests. Higher levels of maternal warmth and praise also predicted fewer subsequent repetitive behaviors and stereotyped interests. This study highlights how positive aspects of the family environment are linked with change in autism symptoms and maladaptive behaviors within families of adolescents and adults with ASD. It was limited to an 18-month period, however, and did not include families where the adult was no longer living in the family home.
The Present Study
The present study aims to extend previous work and address critical gaps in the literature on adults with ASD. The sample was expanded from both studies that previously addressed this topic (Shattuck et al. 2007; Smith et al. 2008) to include 313 adolescents and adults with ASD. Although aspects of the family emotional climate may be more salient to individuals who co-reside with their families, we expanded the sample to include adolescents and adults who lived in community settings since family relationships continue to exert influence on the social and psychological well-being of individuals with ID living outside of the home (Seltzer et al. 2001; Woodman et al., in press). A prospective, longitudinal design was used to examine prevalence of and change in autism symptoms and maladaptive behaviors over the course of 8.5 years, extending the study period from previous work (Shattuck et al. 2007; Smith et al. 2008). Moreover, longitudinal methods were used to predict both between-person differences and within-person change in symptoms and behaviors. Most notably, changes in both maternal praise (based on independently- and blindly-rated maternal speech samples) and mother–child relationship quality (based on mother report) were used to predict changes in autism symptoms and maladaptive behaviors. We elected to focus on positive dimensions of expressed emotion in this study. Findings regarding criticism and emotional over-involvement are reported elsewhere (Greenberg et al. 2006).
We developed several hypotheses about autism symptoms and maladaptive behaviors based on our previous findings and the current literature. We expect the level of autism symptoms and maladaptive behaviors to decline over the study period. While we expect the dominant pattern to be one of improvement, we also anticipate some variability in change. We expect individuals with ID to have more autism symptoms and maladaptive behaviors and slower rates of improvement over the course of the study. Compared to younger adults, we expect older adults will have higher non-verbal communication impairments but lower symptoms and problem behaviors in other domains. We also anticipate that rates of improvement in maladaptive behavior will be faster for older adults. Gender is not expected to relate to autism symptoms or maladaptive behaviors, based on mixed results from previous studies. Since we are extending the study period from previous work on family processes using this sample (Smith et al. 2008), we expect that maternal praise and mother–child relationship quality will have broader impacts on autism symptoms and maladaptive behaviors than previously observed. Specifically, higher levels of maternal praise and higher quality mother–child relationships will predict lower levels of autism symptoms and maladaptive behaviors across domains. Moreover, increases in maternal praise and mother–child relationship quality over time will be linked with reductions in autism symptoms and maladaptive behaviors across domains.
Method
Participants
Participants were drawn from an ongoing, longitudinal study of 406 individuals with ASD and their families, the Adolescents and Adults with Autism (AAA) study (Seltzer et al. 2003). Analyses in the present study used data from 5 waves of data collection: Wave 2 (2000–2001), Wave 3 (2002–2003), Wave 4 (2004–2005), Wave 7 (2007–2008), and Wave 8 (2009–2010). Wave 2 was the first time point in which all variables of interest to this study were measured. These time points will be referred to as Times 1 through 5 for the purposes of the present paper. Across participants, the average length of the study period was 8.5 years. Families were recruited in Massachusetts (N = 204) and Wisconsin (N = 202) through agencies, schools, diagnostic clinics and media announcements. Identical recruitment procedures were used in both states.
Families met three criteria at the start of the study: (1) the family included a child with an ASD diagnosis given by an independent medical, psychological, or educational professional, (2) the child with ASD was 10 years of age or older, and (3) the child’s scores on the research-administered Autism Diagnostic Interview-Revised (ADI-R; Lord et al. 1994) were consistent with an ASD diagnosis. Of the 406 participants, 384 (94.6 %) met criteria for Autistic Disorder on the ADI-R: qualitative impairments in communication and language, qualitative impairments in reciprocal social interaction, repetitive, restrictive, and stereotyped behaviors with an onset of symptoms prior to 36 months. The remaining 22 participants (5.4 %) demonstrated a pattern of impairment on the ADI-R that was consistent with a diagnosis of Asperger’s Disorder or Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS).
The present sample consisted of 313 families for which at least two waves of data on the outcome variables were available. The majority of the participants with ASD were male (75 %). Sixty nine percent had a comorbid diagnosis of ID, consistent with the estimated prevalence of ID among individuals with ASD more broadly (Fombonne 2003; Gillberg and Coleman 2000). Participants ranged from 10 to 49 years of age (M = 21.72, SD = 9.45) at Time 1. More than half of participants (66 %) lived in the family home at the start of the study. Most parents were married (78 %) at that time. With respect to maternal education, 22 % had a high school degree or less, 21 % had some college, 22 % had an associate’s or bachelor’s degree and the remainder had advanced degrees. On average, mothers completed approximately 16 years of education (M = 16.06, SD = 3.16). Maternal age ranged from 32 to 81 years (M = 50.56, SD = 10.36) at Time 1. More than half of mothers (67 %) were employed. The median household income was $50,000–59,999.
Compared to other families in the AAA project at Wave 1, families in the present sample had higher levels of maternal education, χ2 (3, N = 432) = 28.90, p < .01, and higher rates of maternal employment, χ2 (1, N = 432) = 7.68, p = .02, when they enrolled in the AAA project. Only 22 % of mothers in the present sample had a high school degree or less, compared to 47 % of mothers in the larger project. With respect to employment, 67 % of mothers in the present sample were employed at least part time compared to 55 % of mothers in the larger project. Since family income and maternal education were significantly correlated (r = .39, p < .001), maternal education was selected as a covariate in the models. Samples did not differ with respect to maternal age, adult age, state of origin, ID status, gender, maladaptive behaviors or autism symptoms.
More than half of families (55 %) participated in all five time points used in the present analyses. An additional 15 % participated in four time points, followed by 14 % with three time points and 16 % with two time points. Individuals with ASD who dropped out of the study (N = 140) did not differ from those who remained in the study (N = 173) on maternal education, χ2 (3, N = 313) = 6.01, p = .11, autism symptoms, t(311) = 1.10, p = .27, or maladaptive behaviors, t(311) = .31, p = .76. It therefore does not appear that individuals with greater impairments and problematic behavior were more likely to drop out of the study and thus data were missing at random.
Measures
The present study used measures across five time points. Autism symptoms, maladaptive behaviors, mother–child relationship quality, maternal praise and residential status were measured at each time point. ID, gender and age as well as maternal education were based on measures collected at Time 1.
Outcome Variables
Autism Symptoms
The Autism Diagnostic Interview-Revised (ADI-R; Lord et al. 1994) was used to measure autism symptoms. The ADI-R was conducted as a standardized investigator-driven interview with the mother. Items on this measure are based on criteria for an autism diagnosis outlined by the Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition (DSM-IV-TR; American Psychiatric Association 2000) and the International Classification of Diseases (World Health Organization 1987). Items were coded as 0 = no abnormality present, 1 = possible abnormality, and 2 = definite abnormality across four primary symptom domains: repetitive behaviors and stereotyped interests, impairments in social reciprocity, impairments in non-verbal communication, and (for 254 verbal participants only) impairments in verbal communication. Some items also contained a possible score of 3 = extreme abnormality. We recoded each item to reflect either no impairment (0) or some degree of impairment (1). This coding strategy has been used previously (Fecteau et al. 2003; Seltzer et al. 2003; Shattuck et al. 2007). Scales were computed by summing the number of items on which an individual was symptomatic within each domain and also across the four domains, yielding five scales. The interviewers who administered the ADI-R participated in an approved training program. Interrater reliability was high for individual items between two interviewers and two supervising Ph.D. clinical psychologists experienced in the diagnosis of autism and the use of the ADI-R. The ADI-R has demonstrated good test–retest reliability, diagnostic validity, convergent validity and specificity and sensitivity in past research (Hill et al. 2001; Lord et al. 1997).
Maladaptive Behaviors
Maladaptive behaviors were based on the Problem Behavior subscale of the Scales of Independent Behavior-Revised (Bruininks et al. 1996). Mothers indicated the presence of maladaptive behaviors across three domains: internalized (hurtful to self, unusual or repetitive habits, withdrawn or inattentive behavior), externalized (hurtful to others, destructive to property, disruptive behavior) and asocial (socially offensive and uncooperative behavior). Each type of behavior problem was coded as manifested during the past 6 months (1) or not manifested (0). Scales were computed by summing the number of types of maladaptive behaviors manifested within each domain and across the three domains, yielding four scales. Reliability and validity have been established by Bruininks et al. (1996).
Predictor Variables
Demographic Characteristics
The number of years of maternal education was recorded at Time 1. The age (in years) and gender (0 = female and 1 = male) of the adolescents and adults with ASD were recorded at Time 1.
Intellectual Disability
Individuals with standard scores of 70 or below on the Wide Range Intelligence Test (Glutting et al. 2000) and the Vineland Screener (Sparrow et al. 1993) were classified as having ID, consistent with diagnostic guidelines (Luckasson et al. 2002). For individuals with scores between 71 and 75, clinical consensus among three independent raters (one master’s level and two Ph.D. level clinical psychologists) was reached based on available records (e.g., standardized assessments, clinical and school records).
Mother–Child Relationship Quality
Mother–child relationship quality was assessed using the Positive Affect Index (Bengtson and Schrader 1982). Five self-report items that reflected the mother’s feelings toward her son or daughter (e.g., “How much affection do you have toward your son/daughter?”) were used from this scale. Items rated understanding, trust, fairness, respect and affection in the relationship on a six-point scale, from 1 = not at all to 6 = extremely. Previous research has established the construct and discriminant validity of the Positive Affect Index (Bengtson and Allen 1993; Bengtson and Schrader 1982; Greenberg et al. 2004). This index has been found to be a reliable measure of maternal positive affect toward adolescent and adult children with autism (Orsmond et al. 2006).
Maternal Praise
The Five Minute Speech Sample (FMSS) was used to code maternal praise based on the coding manual developed by Magaña et al. (1986). Mothers were asked to speak about their child with ASD for 5 min uninterrupted. The speech sample was tape-recorded, transcribed, and coded for various components of expressed emotion, including criticism, over involvement, positive remarks and warmth. The present study focuses on maternal praise (as indicated by the number of positive remarks). As part of the protocol for coding the Five Minute Speech Sample, raters recorded the number of times a mother praised her son or daughter. Because few mothers made more than five positive remarks, scores of five or greater were recoded to five. Ratings were performed by a coder blind to the study’s hypotheses with more than 20 years of experience in coding all aspects of expressed emotion. An independent second rater also coded 15 transcripts with a correlation coefficient of .83 in their coding of the number of positive remarks.
Analytic Plan
The distributions of the outcome variables were checked for normality. Scores on impairment in social reciprocity appeared slightly negatively skewed while scores on externalized behavior appeared slightly positively skewed upon visual inspection. The skewness statistic did not exceed two for either impairment in social reciprocity (−.91) or externalized behavior (.50), which suggests the skewness is unlikely to bias estimates (West et al. 1995). Results did not differ for raw and transformed values on these variables, therefore results using the raw values were reported to facilitate interpretation. Missing data were imputed using the Markov Chain Monte Carlo procedure in SPSS version 19. Overall, 15 % of values were missing, largely due to attrition since little data was missing on predictor variables (1.4 %). Over half of families participated in all six times points (55 %) and most (84 %) participated in at least four time points. Results present estimates pooled across 10 imputed data sets. Pooling results across multiple imputed data sets is recommended since excluding cases with missing data biases estimates and reduces statistical power (Widaman 2006).
Several analytic approaches were used to describe change in autism symptoms and maladaptive behaviors over the 10 year study period. First, differences in Time 1 and Time 5 subscale scores were tested using paired samples t tests. Second, differences in the prevalence of individual symptoms and behaviors at Time 1 and Time 5 were tested using the nonparametric McNemar test, the test recommended for dichotomous outcome variables (Agresti 1996). Since each symptom or behavior was coded as absent (0) or present (1), change at the item level is interpretable as change in the proportion of study participants who have a given symptom or behavior. Third, participants were classified into three categories based on the magnitude of individual change on subscale scores relative to the Time 1 standard deviation. Participants whose Time 5 scores were within half the Time 1 standard deviation of each respective scale were classified as “no change”. Participants who declined or increased more than a half of a standard deviation were classified as “improved” or “worsened”, respectively. The half standard deviation increment has been used to represent a medium effect size in behavioral research (Cohen 1988; Kline 2004) and also an increment of change that is clinically visible on a variety of behavioral measures (Norman et al. 2003).
Lastly, change in autism symptoms and maladaptive behaviors was examined through multilevel modeling using HLM software version 6 (Raudenbush et al. 2008). Unconditional growth models were conducted as a function of time (in years), separately for each domain and total score. Time was centered at Time 5 so the intercept would represent final levels of autism symptoms and behavior problems. Once the shape of the unconditional growth models was determined, a parallel set of predictors was entered at level 2 to predict the intercept (level at Time 5) and slope (change from Time 1 to Time 5) in each model: ID status, gender, and maternal education were entered uncentered and age was entered grand-mean centered. To address between-person differences, each family process variable (mother–child relationship quality, maternal praise) was averaged across Times 1 through 5 and entered as a level 2 predictor of the intercept and slope (grand-mean centered). To assess within-person differences, each family process variable was also entered at level 1 as a time-varying predictor (group-mean centered). Residential placement status was entered at level 1 as a time-varying predictor.
Results
Prevalence of and Change in Autism Symptoms
We first examined differences in Time 1 and Time 5 domain and total scores (Table 1). The levels of all ADI-R domain and total scores decreased significantly from the start to the end of the study, indicating reduction in severity of repetitive behaviors and stereotyped interests, non-verbal communication impairments, impairments in social reciprocity and verbal communication impairments. Next, we compared the prevalence of individual items at Time 1 and Time 5. At Time 1, impairment in friendships was the most prevalent symptom, with 89 % of participants not having mutually reciprocal relationships with peers. The least prevalent item at the start of the study was impairment in the use of neologisms (20 %). At Time 5, impairment in conventional and instrumental gestures was the most prevalent item, with 82 % of participants failing to use gestures as a form of non-verbal communication. Impairment in the use of neologisms remained the least prevalent item at Time 5, used by only 14 % of participants.
The majority of impairments decreased in prevalence from Time 1 to Time 5 (Table 1). All but two items related to repetitive behaviors and stereotyped interests significantly declined. As exceptions, impairments in unusual preoccupations and other complex mannerisms and body movements did not significantly decline. Two of the four items within the domain of non-verbal communication declined significantly, but impairments in pointing to express interest and conventional and instrumental gestures did not significantly change over the course of the study. The majority of impairments in social reciprocity did not significantly change in prevalence. As exceptions, impairments in direct gaze, range of facial expression to communicate, response to the approaches of others, friendships, inappropriate facial expression and appropriateness of social responses significantly declined. All but two items related to verbal communication impairments significantly decreased in prevalence, specifically impairments in pronominal reversals and verbal rituals.
Participants were classified as “worsened”, “no change” or “improved” based on change in domain and total scores relative to their respective Time 1 standard deviations (Table 2). Improvement was the dominant pattern of change for verbal communication impairments and repetitive behaviors and stereotyped interests. Over half the sample showed improvement in each of these core symptoms. The dominant pattern for non-verbal communication impairments, impairments in social reciprocity, and total autism symptoms was stability, with nearly half the sample demonstrating no change in each of these domains. Fewer than 25 % of the sample worsened in each of the domains.
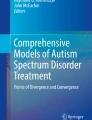
Lastly, unconditional growth models were examined to describe patterns of change in autism symptoms. Repetitive behaviors and stereotyped interests were observed to decline, b = −.10, SE = .08, p < .01, ending with an average of nearly three impairments at Time 5 out of the seven impairments that comprise this subscale, b = 2.61, SE = .01, p < .01. There was significant variability in the intercept (final level), χ2 = 755.92, df = 312, p < .01, and slope (rate of change), χ2 = 453.85, df = 312, p < .01. Impairments in non-verbal communication were found to remain stable over the course of the study, with approximately three impairments at the end of the study out of the four impairments that comprise this subscale, b = 2.94, SE = .05, p < .01. There was significant variability in the intercept, χ2 = 1,789.21, df = 312, p < .01. Impairments in social reciprocity declined over the study period, b = −.13, SE = .02, p < .01, ending with nine of 14 possible impairments on average, b = 9.19, SE = .18, p < .01. There was significant variability in the intercept, χ2 = 1,507.89, df = 312, p < .01, and slope, χ2 = 629.77, df = 312, p < .01. For verbal participants, impairments in verbal communication were also observed to decline over time, b = −.11, SE = .01, p < .01, with three of seven possible impairments on average at the final time point, b = 3.07, SE = .09, p < .01. There was significant variability in the intercept, χ2 = 849.09, df = 266, p < .01, and slope, χ2 = 484.72, df = 266, p < .01. Total autism symptoms also decreased over time, b = −.24, SE = .03, p < .01, resulting in over 14 impairments on average at Time 5, b = 14.67, SE = .26, p < .01. In other words, the number of impairments was estimated to drop from nearly 17 to just over 14 over the course of the study. There was significant variability in the intercept, χ2 = 1,599.64, df = 312, p < .01, and slope, χ2 = 631.43, df = 312, p < .01. Figure 1 displays the predicted trajectories of total autism symptoms for the entire sample (black line) and a random subset of 40 participants (gray lines).

Predicted trajectories of ADI-R autism symptoms. Black line predicted trajectory for entire sample. Shaded line predicted trajectories for a random subset of 40 participants
Predictors of Autism Symptoms
Adult ID, gender, and age as well as maternal education, praise, and perceptions of mother–child relationship quality were added to predict the intercept (level at Time 5) and slope (change from Time 1 to Time 5) of impairments in autism symptoms (Table 3). Comorbid ID predicted slower declines in impairments in social reciprocity and total autism symptoms from Time 1 to Time 5 as well as higher levels of autism symptoms across all domains at Time 5. Gender and maternal education did not predict change or final levels of impairments in autism symptoms. Older adults had significantly higher levels of impairment in non-verbal communication at the end of the study. Changes in residential status did not predict changes in autism symptoms across domains.
Between families, higher levels of maternal praise over the course of the study predicted fewer impairments in non-verbal communication and social reciprocity as well as total autism symptoms. However, within families, changes in maternal praise were not associated with changes in autism symptoms across domains. Between families, higher quality mother–child relationships overall did not predict change or final levels of impairments in autism symptoms. Within families, however, improvements in mother–child relationship quality were associated with decreases in impairments in social reciprocity and total autism symptoms.
Prevalence of and Change in Maladaptive Behaviors
Prevalence of and change in maladaptive behaviors was examined using the same analytic approaches as autism symptoms. The level of SIB-R domain and total scores decreased significantly from the start to the end of the study, indicating improvement in internalized, externalized, asocial and total maladaptive behaviors (Table 4). At Time 1, an unusual or repetitive habit was the most prevalent behavior, present in 81 % of participants. The least prevalent behavior at the start of the study was being hurtful to others (36 %). At Time 5, an unusual or repetitive habit remained the most prevalent behavior (60 %). Similarly, being hurtful to others remained the least prevalent behavior at the end of the study (23 %). All maladaptive behaviors significantly decreased in prevalence from Time 1 to Time 5.
Improvement and stability were the dominant patterns for maladaptive behaviors (Table 5). Nearly half the sample (43 %) showed improvement in externalized behaviors, with 37 % showing stability. Change in internalized behaviors was more ambiguous, with nearly as many participants remaining stable (42 %) as improving (43 %). The dominant pattern for asocial and total maladaptive behaviors was stability. Almost half of participants remained stable in asocial behaviors (44 %) and total maladaptive behaviors (47 %). Fewer than 20 % worsened on each of these domains and only 11 % worsened in total maladaptive behaviors.
Unconditional growth models were examined to describe patterns of change in maladaptive behaviors. Internalized behaviors were observed to decline, b = −.06, SE = .01, p < .01, with an average of one out of three internalized behaviors at Time 5, b = 1.41, SE = .05, p < .01. There was significant variability in the intercept, χ2 = 1,021.12, df = 312, p < .01, and slope, χ2 = 504.27, df = 312, p < .01. Externalized behaviors were also observed to decrease, b = −.06, SE = .01, p < .01, ending with less than one out of three externalized behaviors on average at Time 5, b = 0.81, SE = .05, p < .01. There was significant variability in the intercept, χ2 = 1,037.95, df = 312, p < .01, and slope, χ2 = 577.96, df = 312, p < .01. Asocial behaviors declined over the study period, b = −.04, SE = .01, p < .01, ending with less than 1 out of 2 asocial behaviors on average, b = 0.80, SE = .04, p < .01. There was significant variability in the intercept, χ2 = 869.58, df = 312, p < .01, and slope, χ2 = 513.28, df = 312, p < .01. Finally, total maladaptive behaviors was observed to decline over time, b = −.16, SE = .01, p < .01, with 3 out of 8 maladaptive behaviors on average at the final time point, b = 3.04, SE = .12, p < .01. In other words, the number of maladaptive behaviors decreased from approximately four and a half to three over the course of the study. There was significant variability in the intercept, χ2 = 1,399.42, df = 312, p < .01, and slope, χ2 = 661.53, df = 312, p < .01. Figure 2 displays the predicted trajectories of total maladaptive behaviors for the sample (black line) and a random subset of participants (gray lines).

Predicted trajectories of SIB-R maladaptive behaviors. Black line predicted trajectory for entire sample. Shaded line predicted trajectories for a random subset of 40 participants
Predictors of Maladaptive Behaviors
Adult and mother variables were added to predict change and final levels of maladaptive behaviors (Table 6). Comorbid ID predicted slower declines in internalized behaviors, externalized behaviors, and total maladaptive behaviors from Time 1 to Time 5 as well as higher levels of maladaptive behaviors across domains at Time 5. Gender and maternal education did not predict change or final levels of maladaptive behaviors. Older adults had slower declines in externalized behavior as well as lower levels of externalized, asocial and total maladaptive behaviors at Time 5. Residential status did not predict maladaptive behaviors across domains.
Between families, higher quality mother–child relationships predicted lower levels of externalized, asocial and total maladaptive behaviors at the end of the study. Within families, improvements in mother–child relationship quality were associated with decreases in impairments in asocial behaviors and total maladaptive behaviors. Higher maternal praise over the course of the study predicted fewer asocial and total maladaptive behaviors between families at Time 5. Within families, increases in maternal praise were associated with decreases in externalized and total maladaptive behaviors.
Discussion
The present study extends our understanding of change in the autism phenotype into adulthood. A prospective, longitudinal design was used to describe and predict developmental trajectories in a large, community-based sample of adolescents and adults with ASD, addressing some of the methodological weaknesses of previous work in this area. Findings suggested an overall pattern of improvement into adulthood. We used a conservative approach to measuring change (i.e., complete loss of a symptom), which may actually underrepresent true levels of improvement in adults with ASD. Nevertheless, the findings suggest a trend toward improvement during adolescence and adulthood for most individuals. Several characteristics of the adult with ASD predicted long-term outcomes in this study, but the family environment also played an important role. The results have important implications for life course impacts of ASD and potential points of intervention with families raising children with ASD.
Autism symptoms were generally found to become less severe over the course of the study. This finding is consistent with previous reports of age-related differences or changes in the severity of core symptoms among individuals with Autistic Disorder (Chowdhury et al. 2010; Esbensen et al. 2009; McGovern and Sigman 2005; Seltzer et al. 2004). Change was not universal across participants. While most had declining or persistent autism symptoms, a minority had worsening symptoms over the course of the study. Improvement was also splintered across domains, as has been observed in previous work (Seltzer et al. 2004). Improvement was most evident in repetitive behaviors and stereotyped interests and verbal communication impairments, although impairments in social reciprocity also significantly declined over time. Based on retrospective reports, Fecteau et al. (2003) found a different profile of improvement. They found the greatest improvement in social impairments in a sample of 28 verbal children and adolescents with ASD, followed by communication impairments and repetitive behaviors. Several methodological differences may explain these discrepant findings (e.g., sample, age, study period); nevertheless, both studies underscore the fragmented nature of symptom improvement in this population. In line with our results, several recent studies have documented significant age-related declines in repetitive behaviors (Chowdhury et al. 2010; Esbensen et al. 2009).
Maladaptive behaviors likewise become less severe over the course of the study. The prevalence of each problematic behavior declined from the start to the end of the study. Maladaptive behaviors worsened for only a minority of adults over the 8-year period. Among adults with ASD, the prevalence of challenging and abnormal behaviors has been reported to reduce over time (Murphy et al. 2005; Totsika et al. 2010). Our findings support this general trend. Significant declines were observed for internalized, externalized and asocial behaviors, suggesting a more uniform pattern of improvement across domains, in contrast to the splintered pattern observed in autism symptoms.
By extending the study period from Shattuck et al. (2007), additional insights about change in autism symptoms and maladaptive behaviors were gleaned. The frequency of most impairments and maladaptive behaviors was lower in the present study than in Shattuck et al.’s study. Likewise, the mean number of autism symptoms and maladaptive behaviors was lower after 8.5 years than after 4.5 years. For instance, only 35 % of individuals in Shattuck et al.’s (2007) study were observed to improve in maladaptive behaviors by at least one half standard deviation, whereas 42 % of individuals in the present study were observed to improve in that domain. This pattern of findings suggest continued improvement in functioning for adolescents and adults with ASD.
Above and beyond characteristics of the adult with ASD, aspects of the family emotional climate were related to long-term outcomes. Adults whose mothers expressed more praise of their child during Five Minute Speech Samples had fewer impairments in non-verbal communication and social reciprocity as well as fewer asocial behaviors at the end of the study. Moreover, increases in maternal praise throughout the study were associated with improvements in externalized behaviors. A similar protective role was observed for mother–child relationship quality. Mothers who reported higher quality relationships with their sons and daughters with ASD had children with fewer externalized and asocial behaviors at the end of the study. Improvements in the mother–child relationship were associated with reductions in impairments in social reciprocity as well as asocial behaviors. Taken together, these findings support the importance of family processes to individuals with ASD.
Similar to typically developing individuals (Borkowski et al. 2001) and individuals with diverse developmental risks (Caspi et al. 2004; López et al. 2004), positive family relationships and interactions were associated with positive outcomes for adults with ASD in this sample. These effects were maintained regardless of whether or not the adult with ASD was living in the family home, further emphasizing the enduring importance of the mother–child relationship. Moreover, the residential placement of the adult with ASD was not a significant predictor of autism symptoms or maladaptive behaviors. Impairment in social relationships is a hallmark of ASD (APA 2000) and few adults in this sample (20 %) were reported to have friendships at the end of the study. The family may provide the social support necessary to propel improvements in behavioral functioning for these adults. In a sample of adolescents with diverse developmental disabilities and limited reciprocated friendships, adolescent perceptions of family relationships—but not perceptions of peer friendship quality—predicted self-reported depressive symptoms and global self-worth (Tillinger 2013). Taken together, these studies suggest that family relationships play a central role in the well-being of individuals with developmental disabilities.
We hypothesized that improvements in maternal praise and mother–child relationship quality would be linked with subsequent improvements in autism symptoms and maladaptive behaviors based on previous explorations of bi-directional effects between expressed emotion and adult outcomes in this sample (Greenberg et al. 2006; Smith et al. 2008). Smith et al. (2008), for instance, found that maternal warmth, praise, and mother–child relationship quality impacted autism symptoms and maladaptive behaviors 18 months later, but there was little evidence of the reverse direction of effects. The present study extended Smith et al.’s findings by examining changes in family processes as predictors of changes in functioning over a greater period of time using multilevel modeling. Future research should probe the nature of these time-varying associations to determine the direction of causation. This study also included individuals with ASD who lived outside of the family home, suggesting that the findings regarding the importance of positive family processes generalizable to a wider range of individuals with ASD and their families.
There was variation in the rate of change across individuals in our sample. Some experienced better long-term outcomes than others. As adults, those with comorbid ID had higher levels of both autism symptoms and maladaptive behaviors at the end of the study compared to their peers without ID. This finding was consistent across domains. Individuals with ASD and ID are generally reported to have worse outcomes in adulthood than their peers with ASD without ID (Lord and Bailey 2002; Seltzer et al. 2004; Shea and Mesibov 2005). Adults with ASD and ID were also found to have slower rates of improvement over the course of the study in their social reciprocity and levels of both internalized and externalized behaviors. Similarly, McGovern and Sigman (2005) found fewer lifetime reductions in impairments in social reciprocity for adults with ASD and ID compared to adults with ASD without ID. The presence of ID has long been noted as a risk factor for behaviors problems among individuals with developmental disabilities (Beadle-Brown et al. 2006; De Ruiter et al. 2008). Our findings further support ID as a risk factor for elevated levels as well as reduced rates of improvement in maladaptive behaviors among adults with ASD. Gender did not predict differential adult outcomes or patterns of change. Others have found more problematic developmental trajectories for girls with ASD (Billstedt et al. 2007; Gillberg and Steffenburg 1987; Taylor and Seltzer 2012; Tonge and Einfeld 2003; Von Knorring and Hägglöf 1993).
This study is not without its limitations. First, the sample is primarily of Caucasian descent, thereby limiting the generalizability to other racial or ethnic groups. Second, the mothers included in present analyses had higher levels of education and higher rates of employment than mothers in the original sample. Family processes may differ across families of varying socioeconomic backgrounds. Within the analytic sample, higher maternal education was related to lower quality mother–child relationships (r = −.13, p = .02), but was unrelated to maternal praise during the five minute speech samples (r = −.08, p = .19). Although we controlled for differences in maternal education in analyses, results should be extended to other socioeconomic groups with caution. An additional limitation is the reliance on mother report for measures of adult functioning as well as measures of mother–child relationship quality. Future research should include observational measures of family processes and behavioral change.
Despite its limitations, this study addressed critical gaps in the literature on adult outcomes for individuals with ASD. The overall pattern of change was one of improvement through adulthood. There were, however, a subset of individuals who worsened in maladaptive behaviors and autism symptoms. Future research should examine these cases more closely. A strength of this study is its emphasis on the importance of positive family interactions, in contrast to previous work with individuals with intellectual and developmental disabilities guided by a deficit perspective. Family factors were found to be mechanisms of positive change for individuals with ASD. It is limited to mother–child relationships, however, and future research should consider the influence of father–child relationship quality and paternal praise on the behavioral phenotype of ASD.
Following the results of this study, interventions for individuals with ASD should target positive family processes. Interventions that aim to improve the mother–child relationship and encourage expressions of praise may improve the long-term outcomes for individuals with ASD. Existing programs and services that have improved aspects of the family emotional climate have resulted in better behavioral outcomes for children and adolescents (Webster-Stratton et al. 2004). There are several similar interventions in place for families raising children with developmental disabilities (Pelchat et al. 1999; Hudson et al. 2003). One such program, Transitioning Together, uses a multifamily group psychoeducation model to guide parents of adolescents with ASD through their teen’s transition into adulthood (Smith et al. 2012, 2014). Initial results showed improvements in parent–child relationship quality and maternal warmth following the brief 8-week intervention. ASD is a lifelong disability, but there is growing evidence that aspects of the family emotional climate can lead to abatement in autism symptoms and maladaptive behaviors. Future research should employ experimental designs to evaluate interventions aimed to improve parent–child relationships and increase positivity, as such studies may provide confirmation of the direction of effects examined in this paper.
References
Agresti, A. (1996). An introduction to categorical data analysis. New York: Wiley.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th-TR edn.). Washington, DC: American Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Arias, E. (2012). United States life tables, 2008. National Vital Statistics Reports, 61(3), 1–63.
Baker, B. L., Neece, C. L., Fenning, R. M., Crnic, K. A., & Blacher, J. (2010). Mental disorders in five-year-old children with or without developmental delay: Focus on ADHD. Journal of Clinical Child & Adolescent Psychology, 39(4), 492–505. doi:10.1080/15374416.2010.486321.
Baker, J. K., Seltzer, M. M., & Greenberg, J. S. (2011). Longitudinal effects of adaptability on behavior problems and maternal depression in families of adolescents with autism. Journal of Family Psychology, 25(4), 601–609. doi:10.1037/a0024409.
Beadle-Brown, J., Murphy, G., & Wing, L. (2006). The Camberwell cohort 25 years on: Characteristics and changes in skills over time. Journal of Applied Research in Intellectual Disabilities, 19, 317–329. doi:10.1111/j.1468-3148.2005.00289.x.
Bengtson, V. L., & Allen, K. R. (1993). The life course perspective applied to families over time. In P. G. Boss, W. J. Doherty, R. LaRossa, W. R. Schumm, & S. K. Steinmetz (Eds.), Sourcebook of family theories and methods: A contextual approach (pp. 469–504). New York: Plenum Press.
Bengtson, V. L., & Schrader, S. S. (1982). Parent–child relationship. In D. J. Mangon & W. A. Peterson (Eds.), Research instruments in social gerontology (Vol. 2, pp. 115–185). Minneapolis: University of Minnesota Press.
Billstedt, E., Gillberg, I. C., & Gillberg, C. (2007). Autism in adults: Symptom patterns and early childhood predictors. Use of the DISCO in a community sample followed from childhood. Journal of Child Psychology and Psychiatry, 48(11), 1102–1110. doi:10.1111/j.1469-7610.2007.01774.x.
Borkowski, J. G., Ramey, S. L., & Bristol-Power, M. (2001). Parenting and the child’s world: Influences on academic, intellectual, and social-emotional development. Mahwah, NJ: Lawrence Erlbaum Associates Inc.
Bornstein, M. H. (2006). Parenting science and practice. In W. Damon & R. M. Lerner (Series Eds.) & I. E. Sigel & K. A. Renninger (Vol. Eds.), Handbook of child psychology, vol. 4: Children and parenting (2nd ed., pp. 3–43). Mahwah, NJ: Erlbaum.
Brereton, A. V., Tonge, B. J., & Einfeld, S. L. (2006). Psychopathology in children and adolescents with autism compared to young people with intellectual disability. Journal of Autism and Developmental Disorders, 36(7), 863–870. doi:10.1007/s10803-006-0125-y.
Bruininks, R. H., Woodcock, R. W., Weatherman, R. F., & Hill, B. K. (1996). Scales of independent behaviour-revised. Itasca, IL: Riverside.
Caspi, A., Moffitt, T. E., Morgan, J., Rutter, M., Taylor, A., Arseneault, L., et al. (2004). Maternal expressed emotion predicts children’s antisocial behavior problems: Using monozygotic-twin differences to identify environmental effects on behavioral development. Developmental Psychology, 40(2), 149–161. doi:10.1037/0012-1649.40.2.149.
Centers for Disease Control. (2014). Prevalence of autism spectrum disorders among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2010. Morbidity and Mortality Weekly Report, 63(2), 1–21.
Charman, T. (2002). The prevalence of autism spectrum disorders. Recent evidence and future challenges. European Child and Adolescent Psychiatry, 11(6), 249–256. doi:10.1007/s00787-002-0297-8.
Chowdhury, M., Benson, B. A., & Hillier, A. (2010). Changes in restricted repetitive behaviors with age: A study of high-functioning adults with Autism Spectrum Disorders. Research in Autism Spectrum Disorders, 4(2), 210–216. doi:10.1016/j.rasd.2009.09.006.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Lawrence Erlbaum Associates Inc.
De Ruiter, K. P., Dekker, M. C., Douma, J. C., Verhulst, F. C., & Koot, H. M. (2008). Development of parent- and teacher-reported emotional and behavioural problems in young people with intellectual disabilities: Does level of intellectual disability matter? Journal of Applied Research in Intellectual Disabilities, 21(1), 70–80.
Einfeld, S. L., Piccinin, A. M., Mackinnon, A., Hofer, S. M., Taffe, J., Gray, K., et al. (2006). Psychopathology in young people with intellectual disability. JAMA, 296(16), 1981–1989. doi:10.1001/jama.296.16.1981.
Esbensen, A. J., Mailick, M. R., & Silverman, W. (2013). Long-term impact of parental well-being on adult outcomes and dementia status in individuals with Down syndrome. American Journal on Intellectual and Developmental Disabilities, 118(4), 294–309. doi:10.1352/1944-7558-118.4.294.
Esbensen, A. J., Seltzer, M. M., Lam, K. S. L., & Bodfish, J. W. (2009). Age-related differences in restricted repetitive behaviors in autism spectrum disorders. Journal of Autism and Developmental Disorders, 39(1), 57–66. doi:10.1007/s10803-008-0599-x.
Fecteau, S., Mottron, L., Berthiaume, C., & Burack, J. A. (2003). Developmental changes of autistic symptoms. Autism, 7(3), 255–268. doi:10.1177/1362361303007003003.
Fombonne, E. (2001). Is there an epidemic of autism? Pediatrics, 107(2), 411–412.
Fombonne, E. (2003). The prevalence of autism. JAMA, 289(1), 87–89. doi:10.1001/jama.289.1.87.
Fombonne, E. (2005). Epidemiological studies of pervasive developmental disorders. In F. R. Volkmar, R. Paul, A. Klin & D. Cohen (Eds.), Handbook of autism and pervasive developmental disorders, Vol. 1: Diagnosis, development, neurobiology, and behavior (3rd ed., pp. 42–69). Hoboken, NJ: Wiley.
Ganz, M. L. (2007). The lifetime distribution of the incremental societal costs of autism. Archives of Pediatrics and Adolescent Medicine, 161(4), 343. doi:10.1001/archpedi.161.4.343.
Gillberg, C., & Coleman, M. (2000). The biology of the autistic syndromes. London: Mac Keith Press.
Gillberg, C., & Steffenburg, S. (1987). Outcome and prognostic factors in infantile autism and similar conditions: A population-based study of 46 cases followed through puberty. Journal of Autism and Developmental Disorders, 17(2), 273–287. doi:10.1007/BF01495061.
Glutting, J., Adams, W., & Sheslow, D. (2000). Wide range intelligence test. Wilmington, DE: Wide Range Inc.
Gray, K., Keating, C., Taffe, J., Brereton, A., Einfeld, S., & Tonge, B. (2012). Trajectory of behavior and emotional problems in autism. American Journal on Intellectual and Developmental Disabilities, 117(2), 121–133. doi:10.1352/1944-7588-117-2.121.
Greenberg, J. S., Seltzer, M. M., Hong, J., Orsmond, G. I., & MacLean, J. (2006). Bidirectional effects of expressed emotion and behavior problems and symptoms in adolescents and adults with autism. American Journal on Mental Retardation, 111(4), 229–249.
Greenberg, J. S., Seltzer, M. M., Krauss, M. W., Chou, R. J.-A., & Hong, J. (2004). The effect of quality of the relationship between mothers and adult children with schizophrenia, autism, or Down syndrome on maternal well-being: The mediating role of optimism. American Journal of Orthopsychiatry, 74(1), 14–25. doi:10.1037/0002-9432.74.1.14.
Henry, B., Moffitt, T. E., Caspi, A., Langley, J., & Silva, P. A. (1994). On the “remembrance of things past”: A longitudinal evaluation of the retrospective method. Psychological Assessment, 6(2), 92–101. doi:10.1037/1040-3590.6.2.92.
Hill, A., Bölte, S., Petrova, G., Beltcheva, D., Tacheva, S., & Poustka, F. (2001). Stability and interpersonal agreement of the interview-based diagnosis of autism. Psychopathology, 34(4), 187–191. doi:10.1159/000049305.
Howlin, P. (2005). Outcomes in autism spectrum disorders. In F. R. Volkmar, R. Paul, A. Klin & D. Cohen (Eds.), Handbook of autism and pervasive developmental disorders, Vol. 1: Diagnosis, development, neurobiology, and behavior (3rd ed., pp. 201–220). Hoboken, NJ: Wiley.
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry, 45(2), 212–229. doi:10.1111/j.1469-7610.2004.00215.x.
Hudson, A. M., Matthews, J. M., Gavidia-Payne, S. T., Cameron, C. A., Mildon, R. L., Radler, G. A., et al. (2003). Evaluation of an intervention system for parents of children with intellectual disability and challenging behaviour. Journal of Intellectual Disability Research, 47(4–5), 238–249. doi:10.1046/j.1365-2788.2003.00486.x.
Kline, R. B. (2004). Beyond significance testing: Reforming data analysis methods in behavioral research. Washington, DC: American Psychological Association.
Kobayashi, R., Murata, T., & Yoshinaga, K. (1992). A follow-up study of 201 children with autism in Kyushu and Yamaguchi areas, Japan. Journal of Autism and Developmental Disorders, 22(3), 395–411. doi:10.1007/BF01048242.
Landry, S. H., Smith, K. E., & Swank, P. R. (2006). Responsive parenting: Establishing early foundations for social, communication, and independent problem-solving skills. Developmental Psychology, 42, 627–642.
Levy, A., & Perry, A. (2011). Outcomes in adolescents and adults with autism: A review of the literature. Research in Autism Spectrum Disorders, 5(4), 1271–1282. doi:10.1016/j.rasd.2011.01.023.
López, S. R., Nelson Hipke, K., Polo, A. J., Jenkins, J. H., Karno, M., Vaughn, C., et al. (2004). Ethnicity, expressed emotion, attributions, and course of schizophrenia: Family warmth matters. Journal of Abnormal Psychology, 113(3), 428–439. doi:10.1037/0021-843X.113.3.428.
Lord, C., & Bailey, A. (2002). Autism spectrum disorders. In M. Rutter & E. Taylor (Eds.), Child and adolescent psychiatry (pp. 664–681). Oxford: Blackwell.
Lord, C., Pickles, A., McLennan, J., Rutter, M., Bregman, J., & Folstein, S. (1997). Diagnosing autism: Analyses of data from the Autism Diagnostic Interview. Journal of Autism and Developmental Disorders, 27(5), 501–517. doi:10.1023/A:1025873925661.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24, 659–685. doi:10.1007/BF02172145.
Luckasson, R., Borthwick-Duffy, S., Buntinx, E. H., Coulter, D. L., Craig, E. M., et al. (2002). Mental retardation: Definition, classification, and systems of supports (10th ed., Vol. xiii). Washington, DC: American Association on Mental Retardation.
Magaña, A. B., Goldstein, M. J., Karno, M., Miklowitz, D. J., Jenkins, J., & Falloon, I. R. (1986). A brief method for assessing expressed emotion in relatives of psychiatric patients. Psychiatry Research, 17(3), 203–212.
Matson, J. L., & Horovitz, M. (2010). Stability of autism spectrum disorders symptoms over time. Journal of Developmental and Physical Disabilities, 22(4), 331–342. doi:10.1007/s10882-010-9188-y.
Matson, J. L., & Rivet, T. T. (2008). The effects of severity of autism and PDD-NOS symptoms on challenging behaviors in adults with intellectual disabilities. Journal of Developmental and Physical Disabilities, 20(1), 41–51. doi:10.1007/s10882-007-9078-0.
Mawhood, L., Howlin, P., & Rutter, M. (2000). Autism and developmental receptive language disorder—a comparative follow-up in early adult life. I: Cognitive and language outcomes. Journal of Child Psychology and Psychiatry, 41(5), 547–559. doi:10.1111/1469-7610.00642.
McCarthy, J., & Boyd, J. (2001). Psychopathology and young people with Down’s syndrome: Childhood predictors and adult outcome of disorder. Journal of Intellectual Disability Research, 45(2), 99–105.
McClintock, K., Hall, S., & Oliver, C. (2003). Risk markers associated with challenging behaviours in people with intellectual disabilities: A meta-analytic study. Journal of Intellectual Disability Research, 47(6), 405–416. doi:10.1046/j.1365-2788.2003.00517.x.
McGovern, C. W., & Sigman, M. (2005). Continuity and change from early childhood to adolescence in autism. Journal of Child Psychology and Psychiatry, 46(4), 401–408. doi:10.1111/j.1469-7610.2004.00361.x.
Murphy, G. H., Beadle-Brown, J., Wing, L., Gould, J., Shah, A., & Holmes, N. (2005). Chronicity of challenging behaviours in people with severe intellectual disabilities and/or autism: A total population sample. Journal of Autism and Developmental Disorders, 35(4), 405–418. doi:10.1007/s10803-005-5030-2.
Newschaffer, C. J., Croen, L. A., Daniels, J., Giarelli, E., Grether, J. K., Levy, S. E., et al. (2007). The epidemiology of autism spectrum disorders. Annual Review of Public Health, 28(1), 235–258. doi:10.1146/annurev.publhealth.28.021406.144007.
Norman, G. R., Sloan, J. A., & Wyrwich, K. W. (2003). Interpretation of changes in health-related quality of life: The remarkable universality of half a standard deviation. Medical Care, 41(5), 582–592. doi:10.1097/00005650-200305000-00004.
Orsmond, G. I., Seltzer, M. M., Greenberg, J. S., & Krauss, M. W. (2006). Mother–child relationship quality among adolescents and adults with autism. American Journal on Mental Retardation, 111(2), 121–137.
Overbeek, G., Stattin, H., Vermulst, A., Ha, T., & Rutger, C. M. E. (2007). Parent–child relationships, partner relationships, and emotional adjustment: A birth-to-maturity prospective study. Developmental Psychology, 43(2), 429–437. doi:10.1037/0012-1649.43.2.429.
Pelchat, D., Bisson, J., Ricard, N., Perreault, M., & Bouchard, J.-M. (1999). Longitudinal effects of an early family intervention programme on the adaptation of parents of children with a disability. International Journal of Nursing Studies, 36(6), 465–477. doi:10.1016/S0020-7489(99)00047-4.
Perkins, E. A., & Berkman, K. A. (2012). Into the unknown: Aging with autism spectrum disorders. American Journal on Intellectual and Developmental Disabilities, 117(6), 478–496. doi:10.1352/1944-7558-117.6.478.
Piven, J., Harper, J., Palmer, P., & Arndt, S. (1996). Course of behavioral change in autism: A retrospective study of high-IQ adolescents and adults. Journal of the American Academy of Child and Adolescent Psychiatry, 35(4), 523–529. doi:10.1097/00004583-199604000-00019.
Raudenbush, S., Bryk, A., & Congdon, R. (2008). HLM (version 6). Lincolnwood, IL: Scientific Software International.
Seltzer, M. M., Krauss, M. W., Hong, J., & Orsmond, G. I. (2001). Continuity or discontinuity of family involvement following residential transitions of adults who have mental retardation. Mental Retardation, 39(3), 181–194. doi:10.1352/0047-6765.
Seltzer, M. M., Krauss, M. W., Shattuck, P. T., Orsmond, G., Swe, A., & Lord, C. (2003). The symptoms of autism spectrum disorders in adolescence and adulthood. Journal of Autism and Developmental Disorders, 33(6), 565–581. doi:10.1023/B:JADD.0000005995.02453.0b.
Seltzer, M. M., Shattuck, P., Abbeduto, L., & Greenberg, J. S. (2004). Trajectory of development in adolescents and adults with autism. Mental Retardation and Developmental Disabilities Research Reviews, 10(4), 234–247. doi:10.1002/mrdd.20038.
Shattuck, P. T., Seltzer, M. M., Greenberg, J. S., Orsmond, G. I., Bolt, D., & Kring, S. (2007). Change in autism symptoms and maladaptive behaviors in adolescents and adults with an autism spectrum disorder. Journal of Autism and Developmental Disorders, 37(9), 1735–1747. doi:10.1007/s10803-006-0307-7.
Shea, V., & Mesibov, G. B. (2005). Adolescents and adults with autism. In F. R. Volkmar, R. Paul, A. Klin, & D. Cohen (Eds.), Handbook of autism and pervasive developmental disorders (pp. 288–311). Hoboken: Wiley.
Smith, L. E., Greenberg, J. S., & Mailick, M. R. (2012). Adults with autism: Outcomes, family effects, and the multi-family group psychoeducation model. Current Psychiatry Reports, 14(6), 732–738. doi:10.1007/s11920-012-0328-1.
Smith, L. E., Greenberg, J. S., & Mailick, M. R. (2014). The family context of autism spectrum disorders: Influence on the behavioral phenotype and quality of life. Child and Adolescent Psychiatric Clinics of North America, 23(1), 143–155.
Smith, L. E., Greenberg, J. S., Seltzer, M. M., & Hong, J. (2008). Symptoms and behavior problems of adolescents and adults with autism: Effects of mother–child relationship quality, warmth, and praise. American Journal on Mental Retardation, 113(5), 387–402. doi:10.1352/2008.113:387-402.
Sparrow, S. S., Carter, A. S., & Cicchetti, D. V. (1993). Vineland screener: Overview, reliability, validity, administration, and scoring. New Haven, CT: Yale University Child Study Center.
Taylor, J. L., & Seltzer, M. M. (2012). Developing a vocational index for adults with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(12), 2669–2679. doi:10.1007/s10803-012-1524-x.
Tillinger, M. (2013). The influence of friends and family on well-being for children and adolescents with developmental disabilities. (Doctoral dissertation). Retrieved from ProQuest Dissertations and Theses (UMI: 3560546).
Tonge, B. J., & Einfeld, S. L. (2003). Psychopathology and intellectual disability: The Australian child to adult longitudinal study. International Review of Research in Mental Retardation, 26, 61–91.
Totsika, V., Felce, D., Kerr, M., & Hastings, R. P. (2010). Behavior problems, psychiatric symptoms, and quality of life for older adults with intellectual disability with and without autism. Journal of Autism and Developmental Disorders, 40(10), 1171–1178. doi:10.1007/s10803-010-0975-1.
Totsika, V., Hastings, R. P., Emerson, E., Lancaster, G. A., & Berridge, D. M. (2011). A population-based investigation of behavioural and emotional problems and maternal mental health: Associations with autism spectrum disorder and intellectual disability. Journal of Child Psychology and Psychiatry, 52(1), 91–99. doi:10.1111/j.1469-7610.2010.02295.x.
Tully, L. A., Arseneault, L., Caspi, A., Moffitt, T. E., & Morgan, J. (2004). Does maternal warmth moderate the effects of birth weight on twins’ attention-deficit/hyperactivity disorder (ADHD) symptoms and low IQ? Journal of Consulting and Clinical Psychology, 72(2), 218–226. doi:10.1037/0022-006X.72.2.218.
Von Knorring, A.-L., & Hägglöf, B. (1993). Autism in northern Sweden. A population based follow-up study: Psychopathology. European Child and Adolescent Psychiatry, 2(2), 91–97. doi:10.1007/BF02098864.
Webster-Stratton, C., Reid, M. J., & Hammond, M. (2004). Treating children with early-onset conduct problems: Intervention outcomes for parent, child, and teacher training. Journal of Clinical Child & Adolescent Psychology, 33(1), 105–124. doi:10.1207/S15374424JCCP3301_11.
West, S. G., Finch, J. F., & Curran, P. J. (1995). Structural equation models with non-normal variables: Problems and remedies. In R. Hoyle (Ed.), Structural equation modeling: Concepts, issues and applications (pp. 56–75). Newbury Park, CA: Sage.
Widaman, K. F. (2006). Best practices in quantitative methods for developmentalists: III. Missing data: What to do with or without them. Monographs of the Society for Research in Child Development, 71(3), 42–64.
Woodman, A. C., Mailick, M. R., Anderson, K. A., & Esbensen, A. J. (in press). Residential transitions among adults with intellectual disability across 20 years. American Journal on Intellectual and Developmental Disabilities.
World Health Organization (1987). ICD-10 1986 draft of chapter 5 categories F00-F99. Mental, behavioural and developmental disorders. Geneva: Author.
Acknowledgments
This manuscript was prepared with support from the National Institute on Aging (Grant R01 AG08768, M. R. Mailick, principal investigator) and the National Institute on Child Health & Human Development (P30 HD03352, M. R. Mailick, principal investigator). We also thank the families who participated in this research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Woodman, A.C., Smith, L.E., Greenberg, J.S. et al. Change in Autism Symptoms and Maladaptive Behaviors in Adolescence and Adulthood: The Role of Positive Family Processes. J Autism Dev Disord 45, 111–126 (2015). https://doi.org/10.1007/s10803-014-2199-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-014-2199-2