
Abstract
This study investigates whether the level of language ability and presence of autistic symptomatology in adolescents with a history of SLI is associated with differences in the pattern of difficulties across a number of areas of later functioning. Fifty-two adolescents with a history of SLI participated. At age 14, 26 participants had a history of SLI but no autistic symptomatology and 26 had a history of SLI and autistic symptomatology. At age 16, outcomes were assessed in the areas of friendships, independence, academic achievement, emotional health and early work experience for both subgroups and for 85 typically developing peers. Autistic symptomatology was a strong predictor of outcomes in friendships, independence and early work experience whilst language was a strong predictor of academic achievement. No significant associations were found for later emotional health.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Specific language impairment (SLI) is a developmental disorder that involves deficits in language learning and performance in the absence of factors such as low nonverbal IQ, hearing impairment or neurological damage (Bishop 1997; Leonard 1998). At kindergarten age, the prevalence of SLI is approximately 7% (Tomblin et al. 1997), making it one of the most common childhood disorders. Autism spectrum disorders (ASD) also involve limitations in language and other aspects of communication, but additionally are characterized by marked difficulties in social interaction and social cognition and by repetitive/stereotyped behavioural repertoires (American Psychiatric Association, 2000; Tager-Flusberg et al. 2005; Volkmar and Klin 2005). Estimates of the prevalence of autism are controversial. However, recent data from the UK indicate around 1.16% (Baird et al. 2006) and a similar figure of 1.10% has also been reported in the USA (Kogan et al. 2009), though the prevalence of traits resembling those found in ASD is higher, continuously distributed in the general population (Constantino and Todd 2003; Skuse et al. 2009). Traditionally, SLI and ASD have been regarded as distinct disorders, but for a long time researchers have been aware of similarities between them (Paul et al. 1983; Rutter 1967) and the overlap remains very much a matter of current interest and debate (Bishop and Norbury 2002; Rice et al. 2005; Tager-Flusberg et al. 2005; Volkmar and Klin 2005; Whitehouse et al. 2008; Williams et al. 2008).
SLI and ASD: Commonalities and Overlap
Children diagnosed with either disorder are likely to manifest some level of problems associated with the other category. Thus, even high functioning individuals with ASD continue to experience difficulties with some dimensions of language into adolescence and beyond (Kelley et al. 2006; Rapin and Dunn 2003; Seltzer et al. 2003; Whitehouse et al. 2009a, b). Conversely, among individuals with SLI, social difficulties are often reported through childhood and adolescence (Brinton and Fujiki 2002; Durkin and Conti-Ramsden 2007; Snowling et al. 2006). Some investigators have suggested that there are key commonalities in the language profiles of individuals with ASD and individuals with SLI (Kjelgaard and Tager-Flusberg 2001). Furthermore, parents of children with SLI and parents of children with ASD have been found to have significantly lower communication abilities than parents of children with Down Syndrome (Ruser et al. 2007), and siblings of children with SLI have been found to have elevated risk for diagnosis of autism (Tomblin et al. 2003). These findings suggest genetic and/or environmental overlaps between SLI and ASD. In particular, it has been suggested that a notable proportion of individuals with a history of SLI develop autistic symptomatology during adolescence without exhibiting the level of severity that would lead to a formal diagnosis of ASD (Conti-Ramsden et al. 2006).
It is important to emphasize that the focus of interest here is individuals with a history of SLI who do not have a previous diagnosis of ASD. The young people with SLI with autistic symptomatology have not been identified by services as having ASD nor do they appear to have greater language difficulties than their peers with SLI who do not develop autism symptomatology. These are individuals with SLI as their primary diagnosis. What this study aims to do is focus on the potential for overlap between SLI and autistic symptomatology over the course of development.
The above approach is not novel. Longitudinal studies in the 1980s involving children with SLI observed that approximately 50% of children with persistent language difficulties evidenced features similar to autism (Paul et al. 1983; Paul and Cohen 1984). These symptoms included poor social relations, aloofness, affectless behaviour and unusual responses to stimuli. Much like the recent Conti-Ramsden et al. study (2006), Paul and colleagues found few differences in the language skills of children with SLI with and without ASD features, suggesting that autistic symptomatology is not exclusively associated with poorer language abilities. They noted also that a number of the children with SLI were performing poorly on performance IQ measures (Paul et al. 1983) and furthermore that there appeared to be a decrement in performance IQ over time (Paul and Cohen 1984). Several researchers have since documented a decline in nonverbal abilities of individuals with a history of SLI in middle childhood and adolescence (Botting 2005; Johnson et al. 1999; Tomblin et al. 1992), suggesting more complex, dynamic developmental interactions occur among cognitive systems. Thus, children with SLI who have performance IQs in the normal range in early childhood may meet criteria for intellectual disability later in development. What is of particular relevance to the present study is that later in development, performance IQ in the intellectual disability range is a feature of individuals with SLI with autistic symptomatology but also of those without (Paul and Cohen 1984).
Notwithstanding the overlaps and commonalities noted above, it is very clear that different individuals manifest different patterns of symptoms of developmental disorders. Both ASD and SLI are heterogeneous (Conti-Ramsden 2008; Leonard 1998; Norbury et al. 2008; Rutter and Schopler 1987; Tager-Flusberg 2004; Volkmar and Klin 2005). Some individuals diagnosed as having SLI appear to have profiles of difficulties that are intermediate between SLI and autism. These individuals have often been referred to as having pragmatic language impairment (PLI) (Bishop 2000; Botting and Conti-Ramsden 1999, 2003; Whitehouse et al. 2009a, b). However, not all individuals with SLI who have pragmatic difficulties also exhibit autistic symptomatology (Bishop and Norbury 2002; Loucas et al. 2008). Concerning those individuals with SLI who present autistic symptomatology in later childhood, there is debate as to whether these are cases reflecting earlier misdiagnoses or instrument insensitivity (Noterdaeme et al. 2002) versus instances of late onset development of autistic features (Conti-Ramsden et al. 2006). As well as variability in diagnostic processes and criteria, there are changes across development in the manifestation and severity of autistic symptoms (McGovern and Sigman 2005; Seltzer et al. 2003; Shea and Mesibov 2005; Volkmar and Klin 2005) and of language impairments (Bishop and Norbury 2002; Conti-Ramsden 2008; Tager-Flusberg et al. 2005).
All of these considerations point to the need for a more dimensional approach to diagnosis and a recognition that some individuals will represent different combinations of symptoms (Bishop 2000; Bishop and Norbury 2005; Constantino and Todd 2003; Volkmar and Klin 2005). As well as providing fuller information on variation within conditions, i.e., between SLI and ASD, and commonalities across these conditions, such investigations can illuminate specific relationships among developmental variables (Bishop 2000; Rice et al. 2005). They can also help to make predictions about likely outcomes and improve the knowledge base supporting therapy and services (Klin et al. 2007). Researchers have emphasized the need in particular for prospective, longitudinal investigations to disentangle some of the issues raised by current data (Barnhill 2007; Bishop 2000; Howlin 2003; Klin et al. 2007; Nordin and Gillberg 1998). In this study, we follow adolescents from age 14 to age 16 and examine the relationships between dimensions of symptomatology measured at the earlier age and later functional outcomes.
Functional Outcomes in Adolescence
Adolescence is a time of increasing challenges for most young people but particularly so for individuals with developmental disorders and their families (Durkin and Conti-Ramsden 2010; Hendricks and Wehman 2009; Seltzer et al. 2003; Shea and Mesibov 2005). In the UK, for example, age 16 marks the end of compulsory secondary education and the beginning of a more choice-driven lifestyle. Notably, the primary concern of the parents of adolescents with a history of SLI shifts from their offsprings’ language difficulties to worries about their transition to adulthood, in particular their socialization, future independence and the resources that may be available to support them (Conti-Ramsden et al. 2008). Although research on longer-term outcomes for individuals with SLI has been accumulating (Beitchman et al. 1996a, b; Conti-Ramsden and Durkin 2008; Durkin and Conti-Ramsden 2007; Howlin et al. 2000; Mawhood et al. 2000; Whitehouse et al. 2009a, b), little is known about the outcomes of young people with a history of SLI who also exhibit autistic symptomatology during adolescence.
What we know about functional outcomes comes mainly from comparative longitudinal research between groups of individuals with SLI and groups of individuals with diagnosed ASD. Perhaps the most well-known study is that of Howlin and colleagues (Howlin et al. 2000; Howlin et al. 2004; Mawhood et al. 2000). In this investigation, two groups of individuals, one with SLI and one with ASD were followed from childhood into early adulthood. The investigators found that young men with ASD had significantly more difficulties than the young men with SLI in maintaining friendships, being independent and obtaining or sustaining employment. In terms of academic achievement, however, there were no differences found between the two groups and identifying variables which predicted educational outcomes proved difficult. The authors found some associations between early language ability and outcome in the ASD group, but no particular associations were evident in the group with SLI. Poorer employment outcomes have also been reported in high-functioning adults with ASD (Billstedt et al. 2005; Renty and Roeyers 2006; Szatmari et al. 1989; Whitehouse et al. 2009a, b). Thus, friendships, independence and employment experiences appear to be key areas of functioning that differentiate between individuals with SLI and individuals with ASD, whilst academic achievement does not. In the present study, we investigate these four areas of functioning to examine whether we find a similar pattern of findings when comparing individuals with a history of SLI with autistic symptomatology to those without.
Another important area of functioning of particular salience during adolescence is emotional health. Studies have found higher levels of anxiety-related disorders, depression and other psychological difficulties in individuals with ASD (Bellini 2004; Ghaziuddin et al. 2002; Kim et al. 2000; Shea and Mesibov 2005; White and Roberson-Nay 2009; Whitehouse et al. 2009). Higher anxiety and depressive symptoms have also been found in adolescents with a history of SLI (Beitchman et al. 2001; Conti-Ramsden and Botting 2008) but, interestingly, little relationship has been observed between severity of language difficulties and emotional health symptoms. A study directly comparing 8–12 year-old children with ASD and children with SLI revealed those in the former group to be significantly more anxious than those in the latter (Gillott et al. 2001). In this investigation we include an examination of adolescents’ emotional health in order to ascertain whether individuals who have both SLI and symptoms of ASD may have a higher risk.
The Present Study
There is a dearth of longitudinal study of functional outcomes of young people with SLI and the factors that influence them, especially in relation to the presence of autistic symptomatology. This investigation aimed to compare a range of key outcomes in adolescents with a history of SLI that have been previously examined in the literature contrasting SLI and ASD and to test the extent to which these outcomes are predicted by individual differences in language ability and autistic symptomatology. Participants included a subgroup of adolescents diagnosed as having a history of SLI but not manifesting autistic symptomatology (henceforth, SLI-only), a subgroup diagnosed as having a history of SLI and also manifesting autistic symptomatology (SLI+ASD), and a comparison group of typically developing adolescents (TD group).
Because language is such an integral part of learning, of social interaction, and of the formulation and implementation of most behavioural strategies (Paul 2007; Tager-Flusberg et al. 2005), we expected that both subgroups of individuals with a history of SLI would be disadvantaged with respect to all the areas of functioning examined and hence should show deficits when compared to their TD peers. Based on previous research comparing individuals with SLI and individuals with ASD (Gillott et al. 2001; Howlin et al. 2000; Whitehouse et al. 2009a, b), we expected adolescents with a history of SLI and autistic symptomatology to have poorer outcomes than adolescents with a history of SLI without autistic symptomatology in several respects. This was anticipated to be the case for friendship quality, level of independence, experience of part-time employment, and emotional health symptoms. However, based on the work of Howlin et al. (2000), no differences in academic achievement were expected between the two SLI subgroups.
In addition, we expected that level of language ability and severity of autistic symptomatology would contribute to the explanation of variance in functional outcomes for adolescents with a history of SLI. However, given the often social, interpersonal nature of deficits associated with autistic symptomatology and the findings of Howlin et al. (2000, 2004) regarding poorer levels of independence for individuals with ASD, we expected severity of autistic symptomatology to be a stronger predictor than language of quality of friendships and level of independence. Furthermore, based on the findings of little association between severity of language difficulties and emotional health symptoms (Conti-Ramsden and Botting 2008) and the higher rates of anxiety-related disorders and depression in ASD (Kim et al. 2000), we anticipated autism symptomatology to be associated with anxiety and depression. In contrast, because language skills have been shown to be strongly predictive of academic attainment in individuals with SLI (Conti-Ramsden et al. 2009; Whitehouse et al. 2009a, b) we expected language ability to be the main predictor of educational achievement. Finally, we expected that both autistic symptomatology and language ability would be relevant to success in securing part-time employment.
Method
Participants
Background to Participants
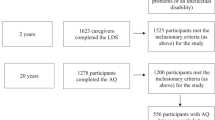
The participants were originally part of a wider longitudinal study, the Conti-Ramsden Manchester Language Study (Conti-Ramsden and Botting 1999a, b; Conti-Ramsden et al. 1997). This cohort was recruited from 118 language units attached to mainstream schools in England. Language units are classes that provide intensive language support for children with primary language difficulties (usually) in ordinary schools. They have on average ten children attending, a specialist teacher, a nursery nurse or other type of assistant, and in most cases a half-time speech and language therapist as well (Conti-Ramsden and Botting 2000). Thus, the ratio and level of expertise in language units is substantial and placements in these units are offered after a team of trained professionals has assessed referred children (usually prior to Kindergarten entry) and deemed them to have primary language difficulties, i.e., specific language impairment (SLI).
These language units provided a list of year 2 children (approximately 7 years of age) attending for at least 50 percent of the week. Children reported by teachers to have frank neurological difficulties, diagnoses of autism, known hearing impairment or general learning impairments were excluded. Across England approximately 500 children fitted this criterion. Subsequently, approximately half of the eligible children in each unit were randomly sampled. This resulted in an initial study cohort of 242 children. The age range was 7.5–8.9 years and consisted of 186 males and 56 females (females forming 23.1 percent of the cohort). These children were reassessed 1, 3, 7 and 9 years later (i.e., at approximately 8, 11, 14 and 16 years of age).
From the original cohort, fifty-two adolescents with a history of SLI participated in the present study. At the first stage of the longitudinal study (age 7 years) the two subgroups of participants (see below for sub grouping criteria) had on average normal nonverbal IQ as measured by the Raven’s Coloured Progressive Matrices (Raven, 1986; SLI-only M = 103.7, SD = 15.9; SLI+ASD M = 100.6, SD = 17.6). Both subgroups demonstrated difficulties with language. Expressive language as measured by the Bus Story (Renfrew, 1991) was on average approximately 1 SD below the mean (SLI-only M = 85.1, SD = 13.6; SLI+ASD M = 84.9, SD = 11.0) as was receptive language as measured by the Test of Reception of Grammar (Bishop, 1982; SLI-only M = 86.0, SD = 12.6; SLI+ASD M = 84.2, SD = 14.4). As discussed in the Introduction, nonverbal IQ can decline in SLI in middle childhood and adolescence (Botting 2005; Johnson et al. 1999; Tomblin et al. 1992). Thus, children with SLI who have nonverbal skills in the normal range in early childhood may meet criteria for intellectual disability later in development. The adolescents in this study are no exception. The nonverbal IQ scores at age 14 years for the subgroups (see Table 1 and section below) show a decline when compared to their scores at age 7 years. Thus, approximately a third of the participants in this study functioned within the intellectual disability range during adolescence (SLI-only = 27%; SLI+ASD = 31% with performance IQ < 70). This is in contrast to only one child in each subgroup having a performance IQ score of 69 at age 7 years.
Subgrouping of Participants
It has been previously found that there is a subgroup of children with SLI that display autistic symptomatology (Conti-Ramsden et al. 2006). At 14 years of age, the 52 participants were assigned to two subgroups based on whether or not they had additional autistic symptomatology (+ASD). Thus, in the present investigation, there were twenty-six adolescents with SLI+ASD (18 M, 8 F, mean age 14.6) who were matched for age and socio-economic status to a subgroup of 26 adolescents with SLI but no autistic symptomatology (21 M, 5 F, mean age 14.3).
The presence of autistic symptomatology was evaluated using two criterion-referenced assessments: the Autism Diagnostic Interview—Revised (ADI-R; Lord et al. 1994) and the Autism Diagnostic Observation Schedule—Generic (ADOS-G; Lord et al. 2000). These instruments are considered gold-standard measures. The data were gathered by two postdoctoral research assistants who had been trained and certified for the use of the instruments. The ADI-R is an interview with the main carer and places substantial emphasis on reported behavior in the 4–5 year old period. The ADI-R generates an algorithm score based on behaviors in three domains: verbal and non-verbal communication, social interaction and repetitive and stereotyped behaviors. The algorithm codes are based on behavioral descriptions of the child at 4–5 years of age for some items and of “ever” for other items. There is an established cut-off for childhood autism (Lord et al. 1994). There is also a less strict cut-off for ASD suggested by Risi et al. (2006) described below. The ADOS-G is a structured observation concerned solely with contemporaneous behavior. The ADOS-G consists of 4 modules, each appropriate to different levels of speech and language competence. It is designed to elicit particular behaviors with a number of “presses”, and scores social communication and social interaction. The ADOS-G algorithm score has established cut-offs both for childhood autism and ASD. Following St Clair et al. (2010), the subgroup with a history of language impairment (SLI-only) had a diagnosis of no autism on both the ADI-R and ADOS-G. The subgroup with autistic symptomatology (SLI+ASD) showed some evidence of broad phenotype autistic behaviors, i.e. autistic symptomatology without full diagnosis. These children either met criteria for ASD on the ADOS-G or achieved impairment level in the social domain of the ADI-R in addition to impairment level on at least one of the remaining two domains (communication or repetitive/stereotyped behaviors), or qualified on both criteria (Risi et al. 2006). The focus of our investigation was not on individuals considered by both instruments to present with all the characteristics necessary for a diagnosis of autism. Five young people were diagnosed with autism by both of the instruments and thus met criteria for full autism (Conti-Ramsden et al. 2006). It is a matter of debate whether these individuals represent previously misdiagnosed cases of autism or true cases of late-onset autism in SLI (i.e., in which autistic symptoms develop outside the typical age range for autism diagnosis). These five individuals were not included in this study. Our aim was to examine the outcomes of individuals who had a primary diagnosis of SLI in childhood, and examine how overlaps with ASD symptomatology over the course of development may affect such outcomes.
A total of 9 individuals qualified for ASD status by the results of the ADOS-G alone, indicating only current, but not historic symptoms, while 9 individuals qualified only on the ADI-R criteria (mainly historic symptoms with some “ever” items). The remaining 8 individuals qualified for ASD status through both the ADI-R and the ADOS-G criteria, but their symptoms were not sufficient to meet criteria for full autism diagnosis. We are aware that the issues relating to classification and diagnosis of these individuals are complex. Nonetheless, for the purposes of this investigation, we refer to the aforementioned 26 individuals as having SLI+ASD, whereas those who did not meet criteria for ASD on either instrument are referred to as SLI-only.
The categorical approach used in participant recruitment described above was supplemented by a dimensional approach in our analyses whereby ASD symptomatology was also examined as a continuous variable. A continuous measure of ASD was derived through summing the scores for the algorithm items on the ADI-R and ADOS-G instruments. This yielded a score that combined historic/ever and current symptomatology, with a potential minimum of 0 and a maximum of 93. For the present sample, the range of scores observed was 3–72 (SLI-only subgroup 3–26, SLI+ASD subgroup 12–72). As expected, there was a difference in the ASD continuous score between subgroups, with a large effect size (SLI-only M = 13.5, SD = 7.3; SLI+ASD M = 38.3, SD = 14.5), F(1,50) = 60.35, p < .001, partial η2 = .55).
It needs to be noted that the ADI-R instrument contains one algorithm diagnostic item on friendships (1 out of 15 items in the social domain section of the ADI-R). As one of the outcome variables is quality of friendships this could be a potential difficulty if participants have been selected on an instrument which taps the same domain. With this in mind, we re-ran all the analyses reported in this study excluding the algorithm item on friendships. All findings were unchanged and the values were virtually identical.
Characteristics of the Subgroups
At Time 1, when assessment of autistic symptomatology was carried out (14 years of age), the mean psycholinguistic standard scores for both subgroups were comparable. Performance IQ was assessed using the Wechsler Intelligence Scale for Children (WISC III-UK; Wechsler 1992). Total Language scores were obtained using the Clinical Evaluation of Language Fundamentals—Revised UK (CELF-R; Semel et al. 1987). The two subgroups had similar performance IQ (SLI-only M = 85.6, SD = 23.5; SLI+ASD M = 82.5, SD = 23.5, p = .61). The two subgroups also had similar total language scores (SLI-only M = 74.5, SD = 17.4; SLI+ASD M = 76.2, SD = 20.0, p = .75). Table 1 presents details of the characteristics of the two subgroups.
Although all participants had a history of SLI and were attending language units for primary language difficulties at age 7 years, by 14 years of age a number of these young people no longer met criteria for current SLI. The presence of large standard deviations reveal heterogeneity. Table 1 shows that by 14 years of age, although the majority of individuals continued to have language difficulties (SLI-only = 65%; SLI+ASD = 62%), approximately one third performed within the normal range, i.e., within one standard deviation of the mean (SLI-only = 35%; SLI+ASD = 37%). Research, nonetheless, has suggested that individuals who appear to have “resolved” their childhood language impairments may still present with difficulties in later childhood, adolescence and adulthood in a number of areas of functioning, including literacy (Simkin and Conti-Ramsden 2006; Stothard et al. 1998), verbal memory (Stothard et al. 1998), perceptual response time (Miller and Poll 2009), and social skills (Conti-Ramsden and Botting 2004). Thus, individuals with a history of SLI who no longer meet criteria for the disorder in adolescence can provide informative data in the area of functional outcomes. The key point to note here is that both subgroups of individuals were similarly heterogeneous presenting with virtually identical (albeit wide) spread of language ability and nonverbal skills. Language ability and nonverbal skills were highly correlated in each of the subgroups (SLI-only = .76; SLI+ASD = .67).
The participants were re-assessed on outcome measures at Time 2 when they were 16 years of age and they were attending the final year of compulsory education in the UK (SLI-only mean age 15;9, SLI+ASD mean age 15.8). Outcomes at this stage of individuals’ development were thought to be particularly informative given that young people were moving towards the more open, more choice-driven world of adulthood. Funding for the project at 14 years did not permit an examination of outcomes at that phase of the investigation.
Socio-Economic Background
Maternal education levels ranged from no educational qualifications (SLI-only 27%; SLI+ASD 14%), to GCSE/O’levels/A-levels/college (SLI-only 65%; SLI+ASD 64%) to university/polytechnic/postgraduate education (SLI-only 8%; SLI+ASD 23%). No significant differences in maternal education levels were found between subgroups, χ²(2, N = 48) = 2.86, p = .24.
Household income bands ranged from <£10,400 per annum (SLI-only 15%; SLI+ASD 13%), to £10,401–£20,800 (SLI-only 27%; SLI+ASD 35%) to £20,801–£36,400 (SLI-only 27%; SLI+ASD 17%) to >£36,401 (SLI-only 31%; SLI+ASD 35%). Household income band did not differ significantly between subgroups, χ²(3, N = 49) = 0.85, p = .84.
Typically Developing Comparison Group
An age-matched comparison group of 85 typically developing (TD) adolescents (53 M/32 F, mean age 15.11) was used to provide data on typical functioning at 16 years of age. These participants had normal PIQ (M = 104.9, SD = 12.2) and language skills (Expressive Language, M = 102.3, SD = 12.3; Receptive Language M = 104.0, SD = 10.8). They had no history of special educational needs or of speech and language therapy provision. All were attending their final year of compulsory secondary education.
Materials
Functional Outcomes in Adolescence (16 years)
Quality of Friendships
The quality of the adolescents’ friendships was measured using the Friendships and Social Relationships section of the Social-Emotional Functioning Interview (SEF-I; Howlin et al. 2000). The participant version was administered to the adolescents and the informant version was administered to their parents. Following previous research with individuals with SLI (Durkin and Conti-Ramsden 2007), the responses by both informants on the three SEF-I items (Perception of acquaintances, Description of current friendships, and Conception of friendships/Quality of friendships) were combined to yield a friendship score with a minimum score of 0 and a maximum score of 16. A score of 0 represented good quality of friendship. Conversely, a score of 16 represented severely restricted quality of friendship. A cut-off point of greater than or equal to 3 represents poor quality of friendships. Durkin and Conti-Ramsden (2007) found that self-report and parent-reports were highly correlated, r = .73. The quality of friendship score has also been found to have adequate reliability (Cronbach’s alpha of .89).
Independent Functioning
The independence score was taken from the work of Conti-Ramsden and Durkin (2008) with individuals with SLI. These authors developed a parental report scale which included items on self-help skills (e.g., looking after oneself), the ability to carry out tasks necessary for everyday living (e.g., using the telephone) and the ability to carry out activities outside the home (e.g., travelling independently, going out on their own or with friends). A composite independence score was created by summing the individual items. This created a variable with a minimum of 0 (no independent functioning) to a maximum of 11 (high independent functioning). The independence score has been found to have adequate reliability (Cronbach’s alpha of .77). One key independence variable, namely their parents’ opinion of whether or not adolescents could look after themselves without help, was used to establish a category of ‘impaired independent functioning’.
Educational Achievement
Educational achievement was measured using KS4 examination results, the national measure for 16 year-olds in the UK. These are usually General Certificates of Secondary Education (GCSE) examinations but also vocational qualifications such as General National Vocational Qualifications (GNVQ). These national examinations have been used previously to assess academic achievement in individuals with SLI (Conti-Ramsden et al. 2009; Snowling et al. 2001). To calculate a score which represented both the quantity and quality of KS4 attainment, grades were converted into numeric scores using the point scoring system used nationally to assess results. In the UK, GCSE grades range from a top score of A* (A star) to A, B, C, D, E, F and G. Numerical conversions are as follows: GCSE A* = 58, A = 52, B = 46, C = 40, D = 34, E = 28, F = 22, G = 16, Unclassified or absent = 0. For GNVQ, the conversion is as follows: Full Intermediate (Distinction = 220, Merit = 184, Pass = 160), Full Foundation (Distinction = 136, Merit = 112, Pass = 76), Part One Intermediate (Distinction = 110, Merit = 92, Pass = 80) Part One Foundation (Distinction = 68, Merit = 56, Pass = 38). Those who were not entered for KS4 examinations were assigned a point score of 0. Higher scores indicate higher levels of academic achievement. A category of ‘poor educational outcome’ was defined as those not achieving the expected grade levels for their age (Level 2 for 16 year olds) in their examinations (e.g., GCSE grade A*-C).
Emotional Health
To measure depression, the Short Form Moods and Feelings Questionnaire (MFQ; Costello and Angold 1988) was used. This is a questionnaire for depressed mood, designed for young people aged 8–18. Respondents are required to say whether each of 13 statements about their feelings were ‘definitely true’ ‘somewhat true’ or ‘not true’ over the previous 3 months. To reduce comprehension difficulties, items from the scale were read out loud and the response options were also represented visually. Higher scores indicate higher levels of depressed mood. As suggested by the MFQ, a cut-off of greater than or equal to 8 was used to establish a category of clinical depression. The MFQ has been found to have adequate reliability (Cronbach’s alpha of .90).
To measure anxiety, the Child Manifest Anxiety Scale (CMAS-R; Reynolds and Richman 1978) was used. This is a questionnaire for anxiety symptoms, designed for young people aged 6–19. Respondents are required to say whether 28 statements are ‘true’ or ‘not true’ for the previous 3 months. To reduce comprehension difficulties, items from the scale were read out loud and the response options were also represented visually. Higher scores indicate higher levels of anxiety. As suggested by the CMAS-R, a cut-off of greater than or equal to 19 was used to establish a category of clinical anxiety. The CMAS-R has been found to have adequate reliability (Cronbach’s alpha of .85).
Part-Time Employment
Participants were asked whether they had ever secured part-time employment. This required a ‘yes/no’ response. In the UK, there is a tradition for adolescents to seek employment (e.g. babysitting, paper round) for pocket money. However, we did not directly assess motivation to seek part-time employment. Thus, the findings of the study could reflect failure to secure part-time employment by participants who were motivated to do so or an absence of motivation to seek part-time employment.
Procedure
The adolescents were assessed and interviewed either at home or school on the above measures as part of a wider battery when they were 14 and subsequently 16 years of age. Assessments took place in a quiet room with only the participant and a trained researcher present. Each testing session lasted for either a morning or afternoon with appropriate breaks. The parents of the participants were interviewed separately at home for a single period of about 2 h. Ethical approval for the study was gained from the University of Manchester.
Results
Adolescent Functional Outcomes
The functional outcome scores for each of the TD group and the two SLI subgroups at age 16 are presented in Table 2. These measures provide a broad profile of the functioning of the SLI subgroups in late adolescence against the backdrop of their TD peers.
A one-way between groups MANOVA was conducted on the five outcome measures that provided continuous variable scores. This analysis revealed a significant effect of group, F(2,120) = 12.19, p < .001, partial η2 = .34. Subsequent univariate analyses confirmed significant group differences on each measure: quality of friendships (F(2,127) = 70.30, p < .001, partial η2 = .53), independent functioning (F(2,124) = 58.43, p < .001, partial η2 = .49), educational achievement (F(2,131) = 36.75, p < .001, partial η2 = .36), depression (F(2,132) = 5.07, p < .01, partial η2 = .07), and anxiety (F(2,132) = 5.12, p < .01, partial η2 = .07).
Bonferroni corrected pairwise comparisons revealed distinctive patterns of differences as a function of each particular area of outcome. The friendship scores showed a clear hierarchy, with the SLI+ASD subgroup being poorer than the SLI-only subgroup, who were in turn poorer than their TD peers on this measure (all comparisons p < .001). The mean score for the SLI+ASD subgroup (M = 5.6) was above the cut-off point 3, suggesting clinically significant difficulties. A similar pattern was observed for independent functioning, with the SLI+ASD subgroup being less independent than the SLI-only subgroup and both subgroups being significantly less independent than their TD peers (all comparisons p < .001). However, the two SLI subgroups were comparable on educational achievement as indexed by their GCSE point score (p = .77) but both lagged significantly behind their TD peers on this measure (both comparisons p < .001). Finally, in terms of emotional health, the two language impaired subgroups did not differ from each other on depression scores (p = .88). Those in the SLI-only subgroup were not significantly different to their peers (p = .25). However, the SLI+ASD subgroup reported higher depression symptoms than did the TD adolescents (p = .01). The same pattern was observed for anxiety. The two language impaired subgroups did not differ from each other on this measure (p = .99) and those in the SLI subgroup were no different to their TD peers (p = .21). However, the SLI+ASD subgroup scored higher on anxiety than did the TD adolescents (p = .01). Nonetheless, it needs to be noted that the mean scores for both subgroups were not above the clinical cut off point suggested for impairment by the instruments used.
In order to provide a fuller picture of the clinical significance of the findings, the proportion of individuals in each subgroup with impaired functioning is shown in Fig. 1. This was calculated by applying the appropriate cut-off scores to each of the five continuous variables. It can be observed that in terms of friendships, independence and educational achievement, over half of the individuals with SLI+ASD and over a third of individuals with SLI-only have impaired functioning. Poor friendship quality was the worst outcome, observed in 81% of individuals with SLI+ASD. In contrast, the poorest outcome in terms of proportion of individuals (54%) was educational achievement for the SLI-only group. Differences in the proportions of those who did and did not report having part-time employment were examined using chi square. Individuals in the SLI-only subgroup were more likely to have part-time employment than those in the SLI+ASD subgroup (p = .02). There were no differences between the TD adolescents and the SLI-only subgroup in this respect (p = .18). However, significantly more TD adolescents (65%) had part-time employment compared to the adolescents with SLI+ASD (19%) (p < .001). The findings for emotional health suggest over one third of adolescents in both SLI subgroups are depressed.

Proportions of SLI-only, SLI+ASD and TD subgroups with impaired functioning on adolescent outcome measures at 16 years. Note: Impaired functioning for each outcome variable was classified using the cut-off points specified in the Method section
Language Ability and Autistic Symptomatology: What Predicts Later Adolescent Outcomes?
The correlational and regression analyses reported in this section involve examining language ability and autistic symptomatology as continuous variables. Thus, the data involve all 52 participants with a history of SLI. These analyses complement the analysis carried out with the categorical subgroup variables of SLI-only and SLI+ASD. In the case of autistic symptomatology, this approach allows us to examine, for example, whether the relationship between outcomes and autistic symptomatology is a negative continuous relationship: the higher the autistic symptomatology the worse the outcomes (except for the friendships difficulty score where the relationship should be positive, the higher the autistic symptomatology the higher the friendships difficulties score). In the case of language ability, the regression analysis is particularly useful given the heterogeneity of language scores within the subgroups. Regression analyses affords the examination of language ability as a continuous variable, which in the case of this study ranges from considerably impaired (a standard score of 50), to the uppermost point within the normal range (a standard score of 115). We can therefore examine, for example, whether the relationship between outcomes and language ability is a positive continuous relationship: the better the language, the better the outcomes.
Correlations between the ASD continuous score and the total language score at 14 years and the outcome measures at 16 years are presented in Table 3.
Medium correlations were observed between the ASD continuous score and friendships difficulty score and independence score. A higher ASD continuous score was related to difficulties with friendships (positive correlation) and less independence (negative correlation). A large positive correlation was observed between the CELF Total Language score and the GCSE point score representing educational achievement. The ASD continuous measure was not correlated with the CELF Total Language score (r = .04, p = .78).
A series of multiple regression analyses were conducted, with CELF Total Language score and the ASD continuous score as predictor variables in a single step. Regression models were examined for each of the outcome measures that were found to be significantly correlated with the independent variables (namely friendships difficulty score, independence score and GCSE point score). Table 4 presents the results of these analyses.
For the regression model predicting friendships outcome, 15% of the variance was accounted for, with the ASD continuous score being the only significant predictor, with a medium effect size (p = .004, f 2 = 0.23). For the independence model, 22% of variance was accounted for, with the ASD continuous score being the only significant predictor, with a large effect size (p = .001, f 2 = 0.35). For the educational achievement measure, 41% of variance was accounted for, with the CELF Total Language score being the only significant predictor, with a large effect size (p < .001, f 2 = 0.87).
Logistic regression was conducted to examine predictors of part-time employment. A forward stepwise procedure was used with significance levels for entry set at p = .05. Outcome was coded as 0 (had part-time employment) and 1 (had not obtained part-time employment). Logistic regression coefficients were used to estimate the odds ratios for each of the independent variables in the model. The ASD continuous score and CELF Total Language score were entered as predictor variables in one block. The ASD continuous score was identified as a significant predictive factor (p = .012) in the model. The individual odds ratio was 1.06 (95% CI: 1.01–1.10), suggesting that for every one unit increase in the ASD continuous score (on a scale from 0 to 93), risk of poor outcome (not having part-time employment) is increased by 6%.
It needs to be noted, however, that the individuals in this study exhibited a wide range of nonverbal skills scores. Not only were there individuals that fell in the intellectual disabilities range but there were also adolescents who fell in the above average category. Further subgrouping within subgroups or omitting certain participants from the study were not feasible as a reduction of subgroup size or loss of participants would result in loss of power. Within this context, given the importance of IQ as a general predictor of long term outcomes (Howlin et al. 2004; Nordin and Gillberg 1998; Szatmari et al. 1989) and the heterogeneity of performance IQ present in the subgroups all of the regression analyses were repeated controlling for performance IQ. The pattern of results presented above remained unchanged. This suggests that the reported results are likely to be robust in this sample. This may be due, at least partly, to the relatively high correlation between performance IQ and language ability in the subgroups of this study. Given that the original analyses had language ability as a key predictor and language ability and performance IQ were highly correlated, the inclusion of performance IQ did not alter the pattern of results observed.
Discussion
An important, though neglected, question for researchers and practitioners working with young people with disorders is what factors can predict real-world success (Klin et al. 2007; Paul et al. 1983). The present study aimed to investigate the possible implications of language ability and autistic symptomatology for the functional outcomes of young people with a history of SLI. A variety of measures were used, involving self-report, information provided by parents, and school examination results. Data from a large comparison group of TD adolescents provided a backdrop for interpreting the findings for the two impaired subgroups. The findings across the measures showed the expected pattern of differences. As anticipated, level of language ability has pervasive implications for adolescent outcomes. More revealing, however, is the pattern of findings between the two SLI subgroups. These results indicate that adolescents with a history of SLI and autistic symptomatology have poorer functioning in the areas of friendships, achieving personal independence, and obtaining early work experience than adolescents with a history of SLI without autistic symptomatology. However, the two SLI subgroups did not differ in terms of academic achievement or emotional well-being. Importantly, then, the overall results of this investigation help to differentiate the implications of varying levels of symptomatology among adolescents with a history of SLI.
Autistic Symptomatology and Adolescent Functioning in Individuals with a History of SLI
Adolescents with SLI+ASD had significantly more difficulties with friendships, independence and early work experience. These findings are strikingly similar to those found by Howlin and colleagues when they compared young adults with SLI to young adults with diagnosed ASD (Howlin et al. 2000, b) and recent reports by Whitehouse et al. (2009a, b). Klin et al. (2007) found marked deficits in communicative and social adaptive skills in a large sample of high functioning children and adolescents with ASD. Paul et al. (1983) reported that children with developmental language disorders together with autistic symptoms presented with much poorer social relations than those with language disorders but no autistic symptomatology. We found that adolescents with a history of SLI and autistic symptomatology were less able to make friends and had more limited social contact than adolescents with a history of SLI-only. Similarly, and again consistent with findings in Klin et al.’s sample of high functioning youth with ASD, adolescents with a history SLI and autistic symptomatology were less competent in the basic skills associated with self-sufficiency, such as keeping a doctor’s appointment, taking a telephone message or managing money. These individuals also lacked early work experience in the form of part-time employment whilst attending schooling. This is a noteworthy finding because, while it is well established that adolescents with disabilities are more vulnerable in the job market (Cameto 2005), our results indicate that autistic symptomatology is particularly disadvantageous. Given the absence of a comparison group with diagnosed ASD in this study, it is difficult to ascertain whether the magnitude of the part-time employment difficulties observed for adolescents with a history of SLI and autistic symptomatology is similar to the magnitude of difficulties that are likely to be experienced by young people with diagnosed ASD. Future research including a group of young people with diagnosed ASD with similar psycholinguistic abilities would clarify the nature of the suggested similarities. What is evident is that young people with a history of SLI who exhibit autistic symptomatology in adolescence have poorer functioning in the aforementioned areas than their peers with a history of SLI without autistic symptomatology, despite having similar levels of language ability.
In three areas of functioning, i.e., friendships, independence and early employment, autistic symptomatology was, as expected, a strong predictor in the regression analyses, with medium to large effect sizes. Language ability, however, did not contribute significantly to these outcomes. It appears that, for these outcomes, the influence of autistic symptomatology overrides any potential influence of language ability as measured by the CELF total language score. It may be worth noting that the autistic symptomatology of the participants with a history of SLI in this study was characterized mainly by difficulties with social interaction and social communication, with less evidence of stereotyped behaviors. These skill areas are likely to be particularly relevant to the three outcomes discussed so far. However, it needs to be noted that stereotyped behaviors are not part of the algorithm for establishing ASD using the ADOS-G, one of the instruments we used to establish autistic symptomatology in our participants.
The subgroups of adolescents with a history of SLI had similar levels of educational achievement. The presence of autistic symptomatology did not appear to influence the level of qualifications obtained at the end of compulsory education. It is important to stress that the adolescents with a history of SLI and autistic symptomatology in this study did not meet criteria for a categorical diagnosis of ASD as defined by the gold standard autism diagnosis instruments, i.e., ADI-R and the ADOS-G. As such, these individuals may be less likely to exhibit classroom behaviors, such as repetitive and idiosyncratic activity, self-injury, tantrums and aggression, which are more prevalent in children with pronounced ASD symptomatology and may be expected to interfere with achievement (Dominick et al. 2007; Eaves and Ho 1997). While autistic symptomatology was not a predictor of educational achievement, language ability was. The results of the regression analysis identified language ability as the key predictor of academic results, explaining 41% of the variance, with a large effect size. This finding is compatible with previous arguments and evidence (Nordin and Gillberg 1998; Paul et al. 1983; Whitehouse et al. 2009a, b), that language ability can be prognostic of some—particularly educational—outcomes in young people with language disorders and ASD.
The results for emotional health outcomes were less clear. Contrary to expectations, there were no significant differences between the two SLI subgroups in symptoms of either depression or anxiety. The mean scores of the SLI+ASD subgroup were significantly higher than that of the TD adolescents. No significant correlations were found between autistic symptomatology and depression, or between autistic symptomatology and anxiety. However, the significant differences observed in these areas of functioning (depression and anxiety) yielded small effect sizes. It needs to be acknowledged that our study may have not had enough power to detect consistent differences between those with SLI and TD peers, as well as between the two SLI subgroups. This is a potential limitation of the present investigation which should be addressed in future research involving larger number of participants.
For emotional health, therefore, we suggest tentatively that adolescents with a history of SLI and autistic symptomatology do not appear to be functioning like young people who meet the full criteria for ASD. Individuals with ASD have been found to have higher levels of anxiety- and depression-related disorders generally, and higher levels than their peers with SLI (Gillott et al. 2001; Kim et al. 2000). As expected, language ability was not significantly correlated with either depression or anxiety. Emotional health in adolescents with SLI is an important area of concern and it is evident that there is an increased risk of anxiety and depression for this population compared to the typical population (Conti-Ramsden and Botting 2008), but the correlates and risk factors for difficulties in this area remain unclear (Clegg et al. 2005).
A limitation of the present study was the lack of consistency in the type of informant used to assess the different areas of functioning. Thus, information on emotional health and part-time employment was gathered via the adolescents’ self-report whilst level of independence was ascertained via parental report. Friendship quality used both self-report and parental information. This may have affected our findings. Although in the area of friendship quality self-report and parental report are highly correlated, this may not be the case for other areas of functioning. Future research could usefully include the same informant for all the areas of functioning examined and ideally involve multiple informants to triangulate the findings.
The Nature of SLI
The heterogeneous nature of SLI has been stressed by clinicians and researchers alike (Conti-Ramsden 2008; Leonard 1998; Norbury et al. 2008). This heterogeneity is present both across individuals (i.e., different individuals have different types of difficulties of varying severity), as well as within individuals (i.e., there appears to be variation in the constellation and severity of difficulties an individual may experience over time; Conti-Ramsden 2008). This heterogeneity makes it difficult to predict from the individual’s language ability other associated difficulties. Long-term outcomes have been no exception (Beitchman et al. 1996a, b; Howlin et al. 2000). We acknowledge that variables influencing outcomes are likely to be complex and involve both intrinsic and extrinsic factors to the individuals concerned. This investigation focused on two sets of individual competencies, namely language ability and autistic symptomatology. We have contributed to the understanding of the heterogeneity of SLI by identifying autistic symptomatology in adolescence as an important predictor of functional outcomes, in particular quality of friendships, level of independence and early experience of employment. We have underlined the importance of language ability to educational achievement in adolescents with SLI with and without autistic symptomatology. In addition, we have drawn attention to emotional health as an important area of functioning where further research is needed to identify potential predictors.
The above contributions, however, come with an important caveat. The very large range of both verbal and nonverbal skills of our participants complicates the interpretation and generalizability of our findings. For example, in the case of the influence of language ability on educational achievement (accounting for 41% of the variance), it is difficult to know what is the contribution of the normal language ability scores versus the impaired scores. Overall, we know there is a positive relationship between the two: the better the language, the higher the educational achievement. However, we are unable to provide a more finely grained analyses of how different ability ranges interact with outcomes. Future research with larger, more homogeneous subsamples of individuals with a history of SLI is needed to examine the aforementioned potential relationships in more detail.
One important issue of relevance to the understanding of the nature of SLI is comorbidity. Could the differences observed between the SLI subgroups be due to “undetected” comorbidity of ASD in a proportion of individuals with a history of SLI? It is known that children with two disorders tend to be more severe and/or have poorer outcomes than those with single disorders (Kaplan et al. 2006). Thus, it is possible that individuals with a history of SLI have a mild form of ASD, a low level comorbidity that goes undetected for most of their development. However, this type of explanation is difficult to reconcile with the fact that over one third of individuals with SLI+ASD presented with symptomatology detected in adolescence only. Why would comorbid, mild ASD be observed in adolescence but not in childhood? What we would like to emphasize is that in addition to comorbidity, there is a need to examine in more depth and detail the role of development in developmental disorders (Sroufe 2009). SLI is at once a dynamic, complex product of development and a contributing factor to development; these bidirectional processes remain in need of elucidation. From this perspective, one of the issues that needs to be addressed by future research is the developmental course of SLI+ASD, that is, what developmental interactions are likely to cause autistic symptomatology in some individuals with a history of SLI in adolescence.
Finally, the existence of autistic symptomatology in young people with SLI and its role in adolescent functioning provide support for the view that SLI is more than a language problem. Accumulating evidence points to the changing, developmental nature of SLI (Conti-Ramsden 2008; Conti-Ramsden and Durkin 2008; Durkin and Conti-Ramsden 2007). Deficits emerge in areas of functioning which are related to language ability but deficits also emerge in areas which do not appear to be directly related to language per se. Within this context, there needs to be much greater awareness of the changing nature of SLI and the potential pervasive and long-standing difficulties that may be experienced by at least a subgroup of adolescents with the disorder, i.e., those also showing autistic symptomatology. The present findings support recent calls for additional training and support to ensure that practitioners working with individuals with a history of SLI or with autism are equipped to gauge symptoms associated with the other disorder (Bennett et al. 2008; Bishop and Norbury 2002; Skuse et al. 2009; Tomblin et al. 2003). Those working and living with individuals with a history of SLI need to ensure that the young persons’ characteristics and potentialities continue to be assessed during adolescence and that relevant individuals have access to good quality support for the range of difficulties they are likely to experience.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders—Test Revision (DSM-IV-TR) (4th ed.). Washington, DC: American Psychiatric Association.
Baird, G., Simonoff, E., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., et al. (2006). Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: The special needs and autism project (SNAP). Lancet, 368, 210–215.
Barnhill, G. P. (2007). Outcomes in adults with Asperger syndrome. Focus on Autism and Other Developmental Disabilities, 22, 116–126.
Beitchman, J. H., Wilson, B., Brownlie, E. G., Walters, H., & Lancee, W. (1996a). Long-term consistency in speech/language profiles: I. Developmental and academic outcomes. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 804–814.
Beitchman, J. H., Wilson, B., Brownlie, E. G., Walters, H., Inglis, A., & Lancee, W. (1996b). Long-term consistency in speech/language profiles: II. Behavioral, emotional and social outcomes. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 815–825.
Beitchman, J. H., Wilson, B., Johnson, C. J., Atkinson, L., Young, A., Adlaf, E., et al. (2001). Fourteen year follow-up of speech/language impaired and control children: Psychiatric outcome. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 75–82.
Bellini, S. (2004). Social skill deficits and anxiety in high-functioning adolescents with autism spectrum disorders. Focus on Autism and other Developmental Disabilities, 19, 78–86.
Bennett, T., Szatmari, P., Bryson, S., Volden, J., Zwaigenbaum, L., Vaccarella, L., et al. (2008). Differentiating autism and Asperger syndrome on the basis of language delay or impairment. Journal of Autism and Developmental Disorders, 38, 616–625.
Billstedt, E., Gillberg, I. C., & Gillberg, C. (2005). Autism after adolescence. Population based 13–22 year follow-up study of 120 individuals with autism diagnosed in childhood. Journal of Autism and Developmental Disorders, 35, 351–360.
Bishop, D. V. M. (1982). Test for reception of grammar. Manchester: University of Manchester.
Bishop, D. V. M. (1997). Uncommon understanding: Development and disorders of language comprehension in children. Hove: Psychology Press.
Bishop, D. V. M. (2000). Pragmatic language impairment: A correlate of SLI, a distinct subgroup or part of the autistic continuum? In D. V. M. Bishop & L. B. Leonard (Eds.), Speech and language impairments in children: Causes, characteristics, intervention and outcome (pp. 99–114). Hove: Psychology Press.
Bishop, D. V. M., & Norbury, C. F. (2002). Exploring the borderlands of autistic disorder and specific language impairment: A study using standardized diagnostic instruments. Journal of Child Psychology and Psychiatry, 43, 917–929.
Bishop, D. V. M., & Norbury, C. F. (2005). Executive functions in children with communication impairments in relation to autistic symptomatology. I: Generativity. Autism, 9, 7–27.
Botting, N. (2005). Non-verbal cognitive development and language impairment. Journal of Child Psychology and Psychiatry, 46, 317–326.
Botting, N., & Conti-Ramsden, G. (1999). Pragmatic language impairment without autism. Autism, 3, 371–396.
Botting, N., & Conti-Ramsden, G. (2003). Autism, primary pragmatic difficulties and specific language impairment: Can we distinguish them using psycholinguistic markers? Developmental Medicine and Child Neurology, 45, 515–524.
Brinton, B., & Fujiki, M. (2002). Social development in children with specific language impairment and profound hearing loss. In P. K. Smith & C. H. Hart (Eds.), Blackwell handbook of childhood social development (pp. 588–603). Blackwell: Malden, MA.
Cameto, R. (2005). Employment of youth with disabilities after high school. In M. Wagner, L. Newman, R. Cameto, N. Garza, & P. Levine (Eds.), After high school: A first look at the post-school experiences of youth with disabilities (Report from the National Longitudinal Transition Study—Vol. 2, pp. 5–1 to 5–21). Menlo Park, CA: SRI International. Available from http://www.nlts2.org/pdfs/afgterhighschool_chp5.pdf.
Clegg, J., Hollis, C., Mawhood, L., & Rutter, M. (2005). Developmental language disorders–a follow-up in later adult life: Cognitive, language and psychosocial outcomes. Journal of Child Psychology and Psychiatry, 46, 128–149.
Constantino, J. N., & Todd, R. D. (2003). Autistic traits in the general population: a twin study. Archives of General Psychiatry, 60, 524–530.
Conti-Ramsden, G. (2008). Heterogeneity of specific language impairment (SLI): Outcomes in adolescence. In C. Norbury, B. Tomblin, & D. V. M. Bishop (Eds.), Understanding developmental language disorders in children: From theory to practice (pp. 117–130). Hove, UK: Psychology Press.
Conti-Ramsden, G., & Botting, N. (1999a). Classification of children with specific language impairment: Longitudinal considerations. Journal of Speech, Language and Hearing Research, 42, 1195–1204.
Conti-Ramsden, G., & Botting, N. (1999b). Characteristics of children attending language units in England: A national study of 7 year-olds. International Journal of Language and Communication Disorders, 34, 359–366.
Conti-Ramsden, G., & Botting, N. (2000). Educational placements for children with specific language impairments. In D. V. M. Bishop & L. B. Leonard (Eds.), Speech and language impairments in children: Causes, characteristics, intervention and outcome (pp. 211–226). Hove: Psychology Press.
Conti-Ramsden, G., & Botting, N. (2004). Social difficulties and victimization in children with SLI at 11 years. Journal of Speech, Language and Hearing Research, 47, 145–161.
Conti-Ramsden, G., & Botting, N. (2008). Emotional health in adolescents with and without a history of specific language impairment (SLI). Journal of Child Psychology and Psychiatry, 49, 516–525.
Conti-Ramsden, G., & Durkin, K. (2008). Language and independence in adolescents with and without a history of specific language impairment (SLI). Journal of Speech, Language, and Hearing Research, 51, 70–83.
Conti-Ramsden, G., Crutchley, A., & Botting, N. (1997). The extent to which psychometric tests differentiate subgroups of children with SLI. Journal of Speech, Language and Hearing Research, 40, 765–777.
Conti-Ramsden, G., Simkin, Z., & Botting, N. (2006). The prevalence of autistic spectrum disorders in adolescents with a history of specific language impairment (SLI). Journal of Child Psychology and Psychiatry, 47, 621–628.
Conti-Ramsden, G., Botting, N., & Durkin, K. (2008). Parental perspectives during the transition to adulthood of adolescents with a history of specific language impairment (SLI). Journal of Speech, Language and Hearing Research, 51, 84–96.
Conti-Ramsden, G., Durkin, K., Simkin, Z., & Knox, E. (2009). Specific language impairment and school outcomes. I: Identifying and explaining variability at the end of compulsory education. International Journal of Language and Communication Disorders.
Costello, E. J., & Angold, A. (1988). Scales to assess adolescent depression. Journal of the American Academy of Child and Adolescent Psychiatry, 27, 726–737.
Dominick, K. C., Davis, N. O., Lainhart, J., Tager-Flusberg, H., & Folstein, S. (2007). Atypical behaviors in children with autism and children with a history of language impairment. Research in Developmental Disabilities, 28, 145–162.
Durkin, K., & Conti-Ramsden, G. (2007). Language, social behavior, and the quality of friendships in adolescents with and without a history of specific language impairment. Child Development, 78, 1441–1457.
Durkin, K., & Conti-Ramsden, G. (2010). Young people with SLI: A review of social and emotional functioning in adolescence. Child Language Teaching and Therapy, 26, 1–17.
Eaves, L. C., & Ho, H. H. (1997). School placement and academic achievement in children with autistic spectrum disorders. Journal of Developmental and Physical Disabilities, 9, 277–291.
Ghaziuddin, M., Ghaziuddin, N., & Greden, J. (2002). Depression in persons with Autism: Implications for research and clinical care. Journal of Autism and Developmental Disorders, 32, 299–306.
Gillott, A., Furniss, F., & Walter, A. (2001). Anxiety in high-functioning children with autism. Autism, 5, 277–286.
Hendricks, D. R., & Wehman, P. (2009). Transition from school to adulthood for youth with Autism spectrum disorders: Review and recommendations. Focus on Autism and Other Developmental Disabilities, 24, 77–88.
Howlin, P. (2003). Outcome in high-functioning adults with autism with and without early language delays: Implications for the differentiation between autism and Asperger syndrome. Journal of Autism and Developmental Disorders, 33, 3–13.
Howlin, P., Mawhood, L., & Rutter, M. (2000). Autism and developmental receptive language disorder—a follow-up comparison in early adult life. II: Social, behavioural, and psychiatric outcomes. Journal of Child Psychology and Psychiatry, 41, 561–578.
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry and Allied Disciplines, 45, 212–229.
Johnson, C. J., Beitchman, J. H., Young, A., Escobar, M., Atkinson, L., Wilson, B., et al. (1999). Fourteen-year follow-up of children with and without speech/language impairments: Speech/language stability and outcomes. Journal of Speech, Language, and Hearing Research, 42, 744–760.
Kaplan, B., Crawford, S., Cantell, M., Kooistra, L., & Dewey, D. (2006). Comorbidity, co-occurrence, continuum: What’s in a name? Child, care. Health and Development, 32, 723–731.
Kelley, E., Paul, J., Fein, D., & Naigles, L. R. (2006). Residual language deficits in optimal outcome children with a history of autism. Journal of Autism and Developmental Disorders, 36, 807–828.
Kim, J. A., Szatmari, P., Bryson, S. E., Streiner, D. L., & Wilson, F. J. (2000). The prevalence of anxiety and mood problems among children with autism and Asperger syndrome. Autism, 4, 117–132.
Kjelgaard, M. M., & Tager-Flusberg, H. (2001). An investigation of language impairment: Implications for genetic subgroups. Language and Cognitive Processes, 16, 287–308.
Klin, A., Saulnier, C., Sparrow, S. S., Cicchetti, D. V., Volkmar, F. R., & Lord, C. (2007). Social and communication abilities and disabilities in higher functioning individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37, 788–793.
Kogan, M. D., Blumberg, S. J., Schieve, L. A., Boyle, C. A., Perrin, J. M., Ghandour, R. M., et al. (2009). Prevalence of parent-reported diagnosis of autism spectrum disorders among children in the US, 2007. Pediatrics, 124, 1395–1403.
Leonard, L. B. (1998). Children with specific language impairment. Cambridge: MIT Press.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview-revised—a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24, 659–685.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., DiLavore, P. C., et al. (2000). The Autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30, 205–223.
Loucas, T., Charman, T., Pickles, A., Simonoff, E., Chandler, S., Meldrum, D., et al. (2008). Autistic symptomatology and language ability in autism spectrum disorder and specific language impairment. Journal of Child Psychology and Psychiatry, 49, 1184–1192.
Mawhood, L., Howlin, P., & Rutter, M. (2000). Autism and developmental receptive language disorder—a comparative follow-up in early adult life: Cognitive and language outcomes. Journal of Child Psychology and Psychiatry, 41, 547–559.
McGovern, C. W., & Sigman, M. (2005). Continuity and change from early childhood to adolescence in autism. Journal of Child Psychology and Psychiatry, 46, 401–416.
Miller, C. A., & Poll, G. H. (2009). Response time in adults with a history of language difficulties. Journal of Communication Disorders, 42, 365–379.
Norbury, C. F., Tomblin, J. B., & Bishop, D. V. M. (2008). Understanding developmental language disorders: From theory to practice. Hove: Psychology Press.
Nordin, V., & Gillberg, C. (1998). The long-term course of autistic disorders: Update on follow-up studies. Acta Psychiatrica Scandinavica, 97, 99–108.
Noterdaeme, M., Mildenberger, K., Sitter, S., & Amorosa, H. (2002). Parent information and direct observation in the diagnosis of pervasive and specific developmental disorders. Autism, 6, 159–168.
Paul, R. (2007). Language disorders from infancy through adolescence: Assessment and intervention (3rd ed.). St. Louis, MO: Mosby-Year Book.
Paul, R., & Cohen, D. (1984). Outcomes of severe disorders of language acquisition. Journal of Autism and Developmental Disorders, 14, 405–421.
Paul, R., Cohen, D., & Caparulo, B. (1983). A longitudinal study of patients with severe, specific developmental language disorders. Journal of the American Academy of Child Psychiatry, 22, 525–534.
Rapin, I., & Dunn, M. (2003). Update on the language disorders of individuals on the autistic spectrum. Brain and Development, 25, 166–172.
Raven, J. C. (1986). Coloured progressive matrices. London: H. K. Lewis & Co.
Renfrew, C. (1991). The bus story: A test of continuous speech. Oxford, UK: C. E. Renfrew.
Renty, J., & Roeyers, H. (2006). Satisfaction with formal support and education for children with autism spectrum disorder: the voices of the parents. Child: Care, Health and Development, 32, 371–385.
Reynolds, C. R., & Richman, B. O. (1978). What I think and feel: A revised measure of children’s manifest anxiety. Journal of Abnormal Child Psychology, 6, 271–280.
Rice, M. L., Warren, S. F., & Betz, S. K. (2005). Language symptoms of developmental language disorders: An overview of autism, down syndrome, fragile X, specific language impairment, and Williams syndrome. Applied Psycholinguistics, 26, 7–28.
Risi, S., Lord, C., Gotham, K., Corsello, C., Chrysler, C., Szatmari, P., et al. (2006). Combining information from multiple sources in the diagnosis of Autism spectrum disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 45, 1094–1103.
Ruser, T. F., Arin, D., Dowd, M., Putnam, S., Winklosky, B., Rosen-Sheidley, B., et al. (2007). Communicative competence in parents of children with autism and parents of children with specific language impairment. Journal of Autism and Developmental Disorders, 37, 1323–1336.
Rutter, M. (1967). A children’s behaviour questionnaire for completion by teachers: Preliminary findings. Journal of Child Psychology and Psychiatry, 8, 1–11.
Rutter, M., & Schopler, E. (1987). Autism and pervasive developmental disorders: Concepts and diagnostic issues. Journal of Autism and Developmental Disorders, 17(2), 159–186.
Seltzer, M. M., Krauss, M. W., Shattuck, P. T., Orsmond, G., Swe, A., & Lord, C. (2003). The symptoms of autism spectrum disorders in adolescence and adulthood. Journal of Autism and Developmental Disorders, 33, 565–581.
Semel, E., Wiig, E., & Secord, W. (1987). Clinical evaluation of language fundamentals—revised. San Antonio, TX: The Psychological Corporation.
Shea, V., & Mesibov, G. (2005). Adolescents and adults with autism. In F. R. Volkmar, R. Paul, A. Klin, & D. J. Cohen (Eds.), Handbook of autism and pervasive developmental disorders (pp. 288–311). New Jersey: Wiley.
Simkin, Z., & Conti-Ramsden, G. (2006). Evidence of reading difficulty in subgroups of children with specific language impairment. Child Language Teaching and Therapy, 22, 315–331.
Skuse, D. H., Mandy, W., Steer, C., Miller, L. L., Goodman, R., Lawrence, K., et al. (2009). Social communication competence and functional adaptation in a general population of children: Preliminary evidence for sex-by-verbal IQ differential risk. Journal of the American Academy of Child & Adolescent Psychiatry, 48, 128–137.
Snowling, M. J., Adams, J. W., Bishop, D. V. M., & Stothard, S. E. (2001). Educational attainments of school leavers with a preschool history of speech-language impairments. International Journal of Language and Communication Disorders, 36, 173–183.
Snowling, M. J., Bishop, D. V. M., Stothard, S. E., Chipchase, B., & Kaplan, C. (2006). Psychosocial outcomes at 15 years of children with a preschool history of speech-language impairment. Journal of Child Psychology and Psychiatry, 47, 759–765.
Sroufe, L. A. (2009). The concept of development in developmental psychopathology. Child Development Perspectives, 3, 178–184.
St Clair, M., Durkin, K., Conti-Ramsden, G., & Pickles, A. (2010). Growth of reading skills in children with a history of specific language impairment (SLI): The role of autistic symptomatology and language related abilities. British Journal of Developmental Psychology, 28, 109–131.
Stothard, S. E., Snowling, M. J., Bishop, D. V. M., Chipchase, B. B., & Kaplan, C. (1998). Language impaired preschoolers: A follow-up into adolescence. Journal of Speech and Hearing Research, 41, 407–418.
Szatmari, P., Bartolucci, G., Bremmer, R., Bond, S., & Rich, S. (1989). A follow-up study of high functioning autistic children. Journal of Autism and Developmental Disorders, 19, 213–225.
Tager-Flusberg, H. (2004). Language and communicative deficits and their effects on learning and behavior. In M. Prior (Ed.), Asperger syndrome: Behavioral and educational aspects (pp. 85–103). New York: Guilford Press.
Tager-Flusberg, H., Paul, R., & Lord, C. (2005). Language and communication in autism. In F. R. Volkmar, R. Paul, A. Klin, & D. J. Cohen (Eds.), Handbook of autism and pervasive developmental disorders (3rd ed., pp. 335–364). New York: Wiley.
Tomblin, J. B., Freese, P. R., & Records, N. L. (1992). Diagnosing specific language impairment in adults for the purpose of pedigree analysis. Journal of Speech and Hearing Research, 35, 832–843.
Tomblin, J. B., Records, N., Buckwalter, P., Zhang, X., Smith, E., & O’Brien, M. (1997). Prevalence of specific language impairment in kindergarten children. Journal of Speech, Language, and Hearing Research, 40, 1245–1260.
Tomblin, J. B., Hafeman, L. L., & O’Brien, M. (2003). Autism and autism risk in siblings of children with specific language impairment. International Journal of Language & Communication Disorders, 38, 235–250.
Volkmar, F. R., & Klin, A. (2005). Issues in the classification of autism and related conditions. In F. R. Volkmar, R. Paul, A. Klin, & D. J. Cohen (Eds.), Handbook of autism and pervasive developmental disorders (3rd ed., pp. 5–41). New York: Wiley.
Wechsler, D. (1992). Wechsler intelligence scale for children—third edition. London: The Psychological Corporation Limited.
White, S. W., & Roberson-Nay, R. (2009). Anxiety, social deficits, and loneliness in youth with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 1006–1013.
Whitehouse, A. J., Barry, J. G., & Bishop, D. V. M. (2008). Further defining the language impairment of autism: Is there a specific language impairment subtype? Journal of Communication Disorders, 41, 319–336.
Whitehouse, A. J., Durkin, K., Jaquet, E., & Ziatas, K. (2009a). Friendship, loneliness and depression in adolescents with Asperger’s syndrome. Journal of Adolescence, 32, 309–322.
Whitehouse, A. J., Line, E. A., Watt, H. J., & Bishop, D. V. M. (2009b). Qualitative aspects of developmental language impairment relate to language and literacy outcomes in adulthood. International Journal of Language and Communication Disorders, 44, 489–510.
Whitehouse, A. J., Watt, H. J., Line, E. A., & Bishop, D. V. M. (2009c). Adult psychosocial outcomes in children with specific language impairment, pragmatic language impairment and autism. International Journal of Language and Communication Disorders, 44, 511–528.
Williams, D., Botting, N., & Boucher, J. (2008). Language in autism and specific language impairment: Where are the links? Psychological Bulletin, 134, 944–963.
Acknowledgments
The authors gratefully acknowledge the Economic and Social Research Council (ESRC, fellowship to Gina Conti-Ramsden, RES-063-27-0066), the Wellcome Trust (grant 060774) and the Nuffield Foundation (grant EDU/8366) for their continued financial support. The authors would like to thank the research assistants involved in data collection as well as the young people, schools and families that helped us with the research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Durkin, K., Conti-Ramsden, G. & Simkin, Z. Functional Outcomes of Adolescents with a History of Specific Language Impairment (SLI) with and without Autistic Symptomatology. J Autism Dev Disord 42, 123–138 (2012). https://doi.org/10.1007/s10803-011-1224-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-011-1224-y