
Abstract
Concern abounds about whether the health care workforce is sufficient to meet changing demands spurred by the Affordable Care Act (ACA). We project that by 2022 the health care industry needs three to four million additional workers, forty percent of which is related to demand growth under the ACA. We project faster job growth in the ambulatory care sector, especially in home health care. Given the current profile, we expect that the future health care workforce will be increasingly female, young, racially/ethnically diverse, not US-born, at or below the poverty level and at a low level of educational attainment.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The health care workforce has recently gained attention due to concerns that it might not have the capacity to meet increasing health care demand. Prior to the Affordable Care Act (ACA) of 2010, policymakers and workforce planners were already concerned about whether the workforce will be sufficient to meet the growing needs of an aging population that is living longer and with multiple chronic conditions (AAMC 2010; Rother and Lavizzo-Mourey 2009; Stone and Harahan 2010). The ACA potentially adds to this demand by extending health insurance to about 25 million Americans (CBO 2013). To meet the increase in demand, researchers anticipate the need to increase the supply of health care workers (Ricketts and Fraher 2013). This trend may present new job opportunities in health care occupations for many Americans, ranging from entry-level positions to highly trained professions (Bodenheimer and Smith 2013). This study examines in which sectors job opportunities may become available, and paints a picture of what the face of our future health care workforce may look like.
Prior to the ACA, the health care industry was already an engine of job growth. The health care industry has seen constant job growth over the last two decades, even during the most recent recession when health care added 428,000 jobs while the rest of the economy lost 7.5 million jobs (Wood 2011). Currently, health care is one of the largest employment sectors, accounting for about 12 % of the total workforce (BLS 2013a). Most analysts expect health care employment to continue to rise, in large part due to the growing elderly population that typically requires more health care services, as well as the implementation of ACA provisions (Cuckler et al. 2013). Recent projections from the Health Resources and Services Administration (HRSA) expect that 81 % of the increase in primary care demand will be due to demographics and the remaining share will be due to changes in demand under the ACA (National Center for Health Workforce Analysis 2013). In this paper, we will take a wider lens on the health care delivery system to project the growth of the health care workforce and the impact of the ACA on this growth.
We begin this paper by describing the current demographic and socioeconomic profile of those employed in the health care industry and by specific sectors (e.g., physician offices, hospitals, and long-term care). Using the current workforce as a baseline, we then use two models to project growth in health care workforce demand in the post-ACA era. The projections not only estimate growth in absolute numbers but also enable us to identify the sectors in which more job growth may occur and to what extent the ACA will drive that job growth. We close with a discussion of how the demographic and socioeconomic profile of the current health care workforce may shift with the projected job growth, and discuss the challenges that may come with these changes.
Methodology
American Community Survey
We used the 2012 American Community Survey (ACS), conducted by the U.S. Census Bureau, to look at the demographic and socioeconomic profile of those who work in different sectors of the health care industry (Ruggles et al. 2010). This household survey has been administered annually since 2000 and replaced the long form of the Decennial Census. We restricted our sample to the non-institutionalized, civilian population sixteen years or older, and used pre-defined stratified sample probability weights to make the sample nationally representative. We focused on respondents who were in the labor force, where labor force participation is defined as working or seeking work (excluding, for example, those in school, retired, or living in institutions).
The ACS uses the 2007 North American Industry Classification System (NAICS) to classify the industry in which an individual works (or if unemployed, the industry in which the individual last worked). The health care industry includes three major sectors: ambulatory health care services (NAICS 621), hospitals (NAICS 622), and nursing and residential care facilities (NAICS 623). We disaggregate ambulatory health care services to the extent that ACS allows and according to NAICS-defined groups which includes: offices of physicians, dentists, chiropractors, optometrists, and all other health care practitioners; outpatient care centers; other ambulatory health care services (including medical and diagnostic labs); and home health care services. Similarly, we disaggregate nursing and residential care facilities (which we also refer to as “long-term care”) into nursing care facilities and residential care facilities (without skilled nursing). Hospitals are not further disaggregated in ACS. We present the profile of workers within each NAICS-defined health care sector, and for comparison the profile of the entire U.S. labor force in the Results section.
National Employment Matrix
To project growth in health care jobs, we used two approaches, each of which has advantages and disadvantages. The first approach is to extract ten-year (2013 to 2022) job projections by industry and occupation from the National Employment Matrix (NEM), which are produced by the Bureau of Labor Statistics (BLS 2013b). (Note: NEM projects job growth based on 2012 employment data derived from the U.S. Current Population Survey, which we report as the baseline health care employment level.) We extracted job projections for each NAICS sector available in the ACS, and calculated the percent change in jobs over the ten-year period.
The methodology to create the NEM projections is discussed in detail elsewhere (BLS 2014). In brief, underlying the NEM model are six interrelated projection models, run iteratively, that take into account macroeconomic and sector-specific supply and demand trends. The macroeconomic projections come from a propriety model that assumes a life-cycle model for consumption, neoclassical model for investment, and full-employment in the long-run (BLS 2014). Labor force participation trends by age, gender, and race/ethnicity serve as constraints to the NEM model. The key driver of the NEM model is the projection of individual demand based on several factors, for example, personal consumption expenditures (PCE), behavioral models, and assumptions provided by industry experts. In health care, the PCE assumptions align with the projection assumptions of the National Health Expenditure Accounts produced by the Office of the Actuary in the Centers for Medicare and Medicaid Services (CMS 2014).
The NEM model is evaluated regularly by BLS staff for accuracy between projected and actual employment. In the last evaluation of their 1996 to 2006 projections, NEM projections of service industries (which encompasses health care industries) had among the lowest mean absolute percent error values compared to other industries (Wyatt 2010). By specific health care industries, NEM overestimated job growth in the long-term care and offices of physicians by one to two percentage points and almost three percentage points for all other ambulatory services, while underestimating hospital job growth about half a percentage point (Wyatt 2010). While a specific explanation for the health industries was not provided for the differences, the overall accuracy of NEM was impacted by difficulties in predicting the impact of large macroeconomic fluctuations from two wars, a housing bubble and oil prices on labor force participation.
ARCOLA model
Our second approach to projecting job growth involved using a microsimulation model called the Adjusted Risk Choice & Outcomes Legislative Assessment (ARCOLA). The ARCOLA assumptions have been described previously and are health care specific (Parente and Feldman 2013; Parente et al. 2011). The ARCOLA model was first used for the Office of the Assistant Secretary for Planning and Evaluation (ASPE) of the U.S. Department of Health and Human Services (DHHS) to simulate the effect of the Medicare Modernization Act of 2003 (MMA) on take-up of high-deductible health plans in the individual health insurance market (OACT 2013; Feldman et al. 2005). Subsequent modifications of the model added information about the utilization of health services by health insurance plan, based on a national multi-payer claims database. As of Fall 2014, the projections from ARCOLA were on par with the actual health insurance enrollment numbers. Specifically, the ARCOLA projections presented in Parente and Feldman (2013) predicted of 7.4 million new individuals to the private insurance market in 2014, and subsequently DHHS reported 7.5 million new individuals to the private insurance market.
For the purposes of this study, we translate the insurance projection take-up rates under ARCOLA into service use within different health care sectors. For example, if ARCOLA projects a 10 % increase in health insurance nationally due to increased enrollment in a Silver Preferred Provider Organization (PPO), then ARCOLA is able to project how this increase in PPO enrollment plays out as service use across physician offices, hospitals and other health care settings. ARCOLA projects service use based on models of past utilization of beneficiaries in plans similar to Silver PPO plans. In this study, we use ARCOLA to obtain projections of service use increase by health care sector with and without ACA provisions in place from 2013 to 2022. Since ARCOLA is not a workforce projection model, we assume that growth in service use within a sector directly translates into demand for health care workers in that sector.
The main benefit of using ARCOLA is to see how demand differs in a world with and without ACA, which we are not able to do with NEM. This difference allows us to gauge how much the ACA is impacting workforce demand. In order to compare the projected changes in ARCOLA versus NEM, we developed a crosswalk to map claims codes for procedure, place of service, and Bergenson-Eggers Type of Services (BETOS) in ARCOLA to specific health care sector NAICS codes in NEM (see Technical Appendix Exhibit 5).
Limitations
There are two limitations worth noting before reporting our results. First, we are not able to directly account for how job roles may be changing over time and how new models of care (e.g., Accountable Care Organizations, Patient-Centered Medical Homes) and payment systems (e.g., bundled payment) may change the delivery of care. As team-based care increases, we may find that the same amount of care may be delivered with fewer people or a different mix of occupations. People in lower-skilled occupations may be able to take on tasks (via task shifting) that were previously held by more highly-skilled workers, thereby allowing the highly-skilled workers to practice at the highest level allowed by their licenses and deliver more and better care than before.
A second limitation is that we are restricted in making major changes to the assumption of NEM’s production analysis or ARCOLA’s health insurance demand model. NEM relies on a proprietary model that we are not able to access directly and modify the inputs. Likewise, ARCOLA has a variety of specific insurance demand intercepts used to account for changes in the uninsured population that we could not alter for this analysis. We trust that the methods used for both NEM and ARCOLA are sufficiently valid due to their scrutiny in prior peer-reviewed publications.
Results
Characteristics of employees in the health care industry
Exhibits 1–3 provide a contemporary snapshot of the attributes of the employees of the health care industry. These Exhibits serve as a starting point to compare the predicted changes in the health workforce as a result of ACA by 2023 in Exhibit 4. Exhibit 1 shows that in 2012 over fifteen million people worked in the health care industry (author calculation). The demographic and socioeconomic profile of these workers varied across health care sectors, and differed from the rest of the labor force in many ways. The health care industry heavily employed women such that more than 75 % of the workforce was female versus less than 50 % in other industries. In home health care, nursing care facilities, and dental offices, women held more than 80 % of the jobs. Workers in the health care industry were also slightly older than those in other industries. Specifically, there is a higher representation of individuals 55 years and older in offices of health care practitioners which includes offices of mental health practitioners (except physicians) and offices of physical therapists, occupational therapist, speech therapists, and audiologists.

Source: Authors calculation from data and sample weights extracted from Ruggles J, Alexander T, Genadek K, Goeken R, Schroeder MB, Sobek M. Integrated public use microdata series: Version 5.0 [Machine-readable database]. Minneapolis, MN: Minnesota Population Center, University of Minnesota; 2010 [cited 2014 Jul 25]. Available from: https://usa.ipums.org/usa/

Source: Authors calculation from data and sample weights extracted from Ruggles J, Alexander T, Genadek K, Goeken R, Schroeder MB, Sobek M. Integrated public use microdata series: Version 5.0 [Machine-readable database]. Minneapolis, MN: Minnesota Population Center, University of Minnesota; 2010 [cited 2014 Jul 25]. Available from: https://usa.ipums.org/usa/
In Exhibit 2, we see a skew towards an older age distribution consistent with the fact that those employed in this sector generally have two or more years of graduate-level training before starting to practice. The offices of dentists, chiropractors, and optometrists, as well as both long-term care sectors had a large share of young workers, with over a third being below 35 years of age. With the exception of chiropractors, this pattern correlates with the high percentage (60–80 %) of workers in these sectors having some college or less education.
A high proportion of workers in the long-term care and home health care sectors were at or below the 100 % poverty threshold (Exhibit 1). One in five home health care services workers was at or below the poverty threshold, and one in eight workers in nursing care facilities and residential care facilities were at or below the poverty threshold. These statistics are largely masked by the relatively low poverty levels in the other health care sectors. Workers in other health care sectors may be more affluent than those in the long-term care sector due to their higher educational level.
In 2012, the racial and ethnic profile of the health care industry was similar to other industries except for a higher representation of African Americans and lower representation of Hispanics (Exhibit 3). The racial and ethnic profile varied considerably across sectors: minorities held over half of the home health care service jobs, and almost half of jobs in nursing care facilities and residential care facilities. The proportion of health care employees who were not born as citizens was slightly lower in the health care industry compared to other industries, but varied across sectors, ranging from a low of 8.6 % in optometrist offices to a high of 23.3 % in home health care services. Of those working in health care and who were not born in the U.S., about one third were of Asian/Pacific Islander descent, 24.5 % were Hispanic, 20 % were African American, and 20 % were white, non-Hispanic (data not shown).

Source: ARCOLA and Bureau of Labor Statistics. Table 1.9 2012-22 Industry-occupation matrix data, by industry [Internet]. Washington, DC: Bureau of Labor Statistics. [cited 2014 Jul 25; updated 2013 Dec 19]. Available from: http://www.bls.gov/emp/ep_table_109.htm
Job projections
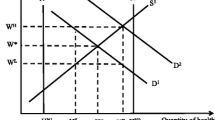
By 2022, the health care industry will need three to four million additional workers (a 20 to 26 percent increase in jobs), assuming the ACA will move forward as planned (calculated from Exhibit 4). The ambulatory care sector is projected to see the largest absolute growth as well as average percent growth in jobs under both models (Exhibit 4). Within ambulatory care, about one-third of the additional jobs in the next decade are projected to be in the home health care sector.
Based on the ARCOLA model, 1.2 million of these jobs (or forty percent of the new jobs) are related to the demand growth from the ACA (author’s calculation; data not shown). Although overall job growth in the health care sector favors ambulatory care, the ACA’s impact is projected to be greatest for hospital services, which accounts for 44 % of the ACA-related increase in health care job demand versus 36 % due to ambulatory care and 20 % due to long-term care.
NEM projected higher job growth numbers relative to ARCOLA. While the accuracy of the 2012-22 NEM projections cannot yet be evaluated, based on prior evaluations of the NEM projections for the health care sector, the difference of 900,000 jobs (most of which are in the ambulatory care sector) between NEM and ARCOLA job growth numbers are reasonably within NEM’s margin of error discussed earlier. Also, the differences should be taken in context with what we know about NEM’s past performance relative to the current demographic profile of the health care workforce. NEM overestimated job growth in health care, which may be highly correlated with NEM’s overestimation of labor force participation by White women across industries (Wyatt 2010). Although, NEM underestimated the labor force participation by about 1.5 percentage points of African-American women, who are highly represented in the home health and long-term care sectors, these underestimations may be offset by the approximately 2.5 percentage point overestimations in labor force participation by White women (Wyatt 2010). NEM also considerably underestimated labor force participation by Hispanic women by almost fifteen percentage points over a ten year period, which suggests that projections of home health and outpatient care jobs maybe on the low end (Wyatt 2010). Taken together, the NEM health care job growth estimates may be an upper bound assuming no major adjustments to labor force participation rates have been made to subsequent projections.
Another possible explanation for the differences in job projections is how ARCOLA and NEM account for health care delivery changes. While both ARCOLA and NEM take into account an aging demographic, ARCOLA focuses on how health care delivery changes via enrollment in different types of health care plans. NEM, which uses health care consumption projection models developed by CMS (2014), focuses on how health care delivery changes via changes in health spending. The NEM model also makes assumptions about the expected pressures through insurance programs (e.g., Medicare and private health insurance companies) to shift service delivery from costly inpatient to less costly outpatient settings (CMS 2014; Henderson 2013). The NEM model also projects substantially greater demand growth (228,000 more jobs) in the home health care sector compared to the ARCOLA model. Again, NEM assumes that health insurance programs will incentivize individuals to use of lower cost home health care. Also, given that ARCOLA is an insurance-based microsimulation model and the ACA had few insurance provisions related to long-term care, ARCOLA predicts little if any changes in long-term care demand. Taken together, we assume that ARCOLA’s approach is likely to be a more conservative one whereby the projected demand for health care workers may be a lower bound.
Conclusion
Our study finds that three to four million new health care jobs—a 20–26 % increase over current levels—will be created over the next decade. We project that forty percent of these new jobs are related to an increase in health care demand from the ACA. The ambulatory care sector will see the largest gain in jobs primarily due to growth in home health. Given our job projections and assuming that the current demographic and socioeconomic profile of the health care industry persists over the next decade, we expect to see an increasingly female, younger, racially and ethnically diverse, non-US born, low income, and low-education health care workforce.
A challenge for any workforce planner using projection models is to what extent they should put store on the projected values and what actions to take as a result. In this study, we report the results from the most comprehensive and reliable model available for projecting growth in health care job, the National Employment Matrix. We further validate NEM by comparing their projected values with ARCOLA, which is health care specific and a validated health care demand model in the literature. ARCOLA, however, was not designed specifically to be a workforce projection model, but rather was designed to assess how ACA impacts health care demand. Our study, however, finds that the job growth projections from NEM and ARCOLA are similar across health care sectors. Any differences may be explained by margins of error as well as by differences in assumptions about the impact of payment policies and insurance take up. The latter two points are particularly tough for any expert to predict given that these decisions are often subject to the political environment.
To some extent, actions are already taking place to get a health care workforce ready to meet the increasing demand in health care jobs. Title V of the ACA has more than forty workforce provisions ranging from student loans, training grants, and employee retention programs to expansion of health centers and innovative programs for education and new care delivery models (Spetz 2012). Many of these provisions, however, have not yet been funded. More will need to be done to ensure that the future health care workforce has the skills needed to meet future health care needs and the opportunity to advance their careers into higher-paying health care job.
The most recent action that may impact the pipeline of new health care workers is the recent proposal by President Obama in his 2015 State of the Union address to make community college free. Most health care workers across sectors have some college education or less. This trend is likely to continue as jobs are expected to grow fastest among the sectors with the lowest levels of education. The trend is consistent with other recent reports that show entry-level positions requiring relatively little prior training were prominent across the all health care sectors; home health aides, clerks, personal care aides, and technicians were among the most common jobs (Frogner and Spetz 2013). Another study found that the fastest growing health occupations require no more than a high school diploma, such as medical assistants and pharmacy technicians, and that the ACA will drive at least 40 % of the jobs growth for medical assistants, medical secretaries, pharmacy technicians, and pharmacy aides (Spetz et al. 2014). If the health care industry relies on community colleges to provide training to future health care workers, however, community colleges require further resources such as educators and labs to keep up with the demand for education in health care (Rubenfire 2015). If community colleges are not provided sufficient resources, for-profit vocational schools are more than ready to offer training for these entry-level health care occupations. This trend has raised concerns about the quality of training, high tuition costs, and student debt (Williams 2014). Greater regulation of these educational programs, and perhaps more public education programs, should be considered.
While these trends may provide new opportunities for those at the entry-level of employment, there will be a challenge in ensuring that the comparatively disadvantaged population that fills these jobs has opportunities for upward job mobility. In this study, we show that a high rate of poverty exists in the areas of the health care sector with anticipated growth; for example, one in five workers in home health services is at or below the poverty level. In a recent report of long-term care workers including home health care, Frogner and Spetz (2015) found that turnover rate appears to be high. Most of the long-term care job leavers become unemployed or exit the labor force altogether despite availability of jobs; and when they leave, these workers are at a higher state of poverty and have higher rates of work disability. Overall, health care wages have been keeping pace with wages in other industries (Frogner 2010), but the distribution of wages across largely varies where the wages of those with higher levels of education may be masking the wages of those at the other end of the distribution. The challenge is that health care delivery organizations are reimbursed on a fee-for-service basis, and the services and competencies required by lower-skill supportive occupations are generally not considered reimbursable expenses. Until new payment models, such as bundled payments and performance-based payment, become more widespread, our baseline estimates of job growth are likely to prevail. Further work is needed to monitor how payment innovations will impact the future demand for the health care workforce.
References
Association of American Medical Colleges. (2010). The impact of health care reform on the future supply and demand for physicians updated projections through 2025 [Internet]. Washington, DC: Association of American Medical Colleges. [cited 2014 Jul 18]. 2 pp. Available from: https://www.aamc.org/download/158076/data/updated_projections_through_2025.pdf.
Bodenheimer, T. S., & Smith, M. D. (2013). Primary care: Proposed solutions to the physician shortage without training more physicians. Health Affairs (Millwood), 32(11), 1881–1886.
Bureau of Labor Statistics. (2013a). Projections methodology [Internet]. Washington, DC: Bureau of Labor Statistics. [cited 2014 Jul 25; updated 2014 Jan 2]. Available from: www.bls.gov/emp/ep_projections_methods.htm.
Bureau of Labor Statistics. (2013b). Table 2.1. Employment by major industry sector [Internet]. Washington, DC: Bureau of Labor Statistics. [updated 2013 Dec 19, cited 2014 Jul 18]. Available from: http://www.bls.gov/emp/ep_table_201.htm.
Bureau of Labor Statistics. (2014). Table 1.9 2012–22 Industry-occupation matrix data, by industry [Internet]. Washington, DC: Bureau of Labor Statistics. [cited 2014 Jul 25; updated 2013 Dec 19]. Available from: http://www.bls.gov/emp/ep_table_109.htm.
Centers for Medicare and Medicaid Services. (2014). Projections of national health expenditures: Methodology and model specification [Internet]. Baltimore, MD: Centers for Medicare and Medicaid Services. [cited 2015 Jan 29; updated 2014 Sep 3]. Available from: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/ProjectionsMethodology.pdf.
Congressional Budget Office. (2013). Table 1. CBO’s May 2013 estimate of the effects of the Affordable Care Act on health insurance coverage [Internet]. Washington, DC: Congressional Budget Office. [cited 2014 Jul 18]. 3 pp. Available from: http://www.cbo.gov/sites/default/files/cbofiles/attachments/43900-2013-05-ACA.pdf.
Cuckler, G. A., Sisko, A. M., Keehan, S. P., Smith, S. D., Poisal, J. A., Wolfe, C. J., et al. (2013). National health expenditure projections, 2012–22: Slow growth until coverage expands and economy improves. Health Affairs (Millwood), 32(1), 1820–1831.
Feldman, R., Parente, S. T., Abraham, J., Christianson, J. B., & Taylor, R. (2005). Health savings accounts: Early estimates of national take-up. Health Affairs (Millwood), 24(6), 1582–1591.
Final Report (April, 2013). Contract No. OA-393-2012-0001 from the Office of the Actuary (OACT), United States Department of Health and Human Services.
Frogner, B. (2010). The missing technology: An international comparison of human capital investment in health care. Applied Health Economics and Health Policy, 8(6), 361–371.
Frogner, B., & Spetz J. (2015). Exit and entry of workers in long-term care. San Francisco. CA: UCSF Health Workforce Research Center on Long-Term Care.
Frogner, B., & Spetz, J. (2013). Affordable Care Act of 2010: Creating job opportunities for racially and ethnically diverse populations [Internet]. Washington, DC: Joint Center for Political and Economic Studies. [cited 2014 Jul 25]. Available from: http://jointcenter.org/content/affordable-care-act-2010-creating-job-opportunities-racially-and-ethnically-diverse.
Henderson, R. (2013). Industry employment and output projections to 2022. Monthly Labor Review. December: 1–34.
National Center for Health Workforce Analysis, Health Resources and Services Administration. (2013). Projecting the Supply and Demand for Primary Care Practitioners Through 2020 [Internet]. Rockville, MD: US Department of Health and Human Services. [cited 2014 Aug 30]. 37 pp. Available from: http://bhpr.hrsa.gov/healthworkforce/supplydemand/usworkforce/primarycare/projectingprimarycare.pdf.
Parente, S., Feldman, R., Abraham, J. M., & Xu, W. (2011). Consumer response to a national marketplace for individual insurance. Journal of Risk and Insurance, 78(2), 389–411.
Parente, S. T., & Feldman, R. (2013). Micro-simulation of private health insurance and Medicaid take-up following the U.S. Supreme Court decision upholding the Affordable Care Act. Health Services Research, 48(2 Pt 2), 826–849.
Ricketts, T. C., & Fraher, E. P. (2013). Reconfiguring health workforce policy so that education, training, and actual delivery of care are closely connected. Health Affairs (Millwood), 32(110), 1874–1880.
Rother, J., & Lavizzo-Mourey, R. (2009). Addressing the nursing workforce: A critical element for health reform. Health Affairs (Millwood), 28(4), w620–w624. doi:10.1377/hlthaff.28.4.w620.
Rubenfire, A. (2015). Healthcare could gain from Obama’s free community college bid. Modern Healthcare. [cited 2015 Jan 29; updated 2015 Jan 9]. Available from: http://www.modernhealthcare.com/article/20150109/NEWS/301099948.
Ruggles, J., Alexander, T., Genadek, K., Goeken, R., Schroeder, M. B., & Sobek, M. (2010). Integrated public use microdata series: Version 5.0 [Machine-readable database]. Minneapolis, MN: Minnesota Population Center, University of Minnesota. [cited 2014 Jul 25]. Available from: https://usa.ipums.org/usa/.
Spetz, J., Frogner, B., Lucia, L., & Jacobs, K. (2014). The impact of the affordable care act on new jobs. Berkeley, CA: Center for Labor Research and Education. [cited 2014 Jul 25]. Available from: http://www.bigideasforjobs.org/wp-content/uploads/2012/03/Spetz_Lee_Final.pdf.
Spetz, J. (2012). Health reform and the health care workforce [Internet]. Houston, TX: James A. Baker III Institute for Public Policy. [cited 2014 Jul 25]. Available from: http://bakerinstitute.org/files/1399/.
Stone, R., & Harahan, M. F. (2010). Improving the long-term care workforce serving older adults. Health Affairs (Millwood), 29(1), 109–115.
Williams, T. (2014). Seeking new start, finding steep cost; workforce investment act leaves many jobless and in debt. New York Times (New York Edition). Aug 17; Sect A:1.
Wood, C.A. (2011). Employment in health care: A crutch for the ailing economy during the 2007–09 recession. Monthly Labor Review, April:13–19.
Wyatt, I. D. (2010). Evaluating the 1996–2006 employment projections. Monthly Labor Review, September: 33–69.
Acknowledgments
This work was conducted with the support of the Joint Center for Political and Economic Studies. We acknowledge the support of the Health Systems Innovation Network, LLC for the use and adaptation of the ARCOLA model for this research.
Author information
Authors and Affiliations
Corresponding author
Technical Appendix
Technical Appendix
Modified assumptions of the ARCOLA model
Following is a brief discussion the model, and the updated assumptions and modifications we made for the purposes of this study. We assumed that the ACA will unfold as legislated and made the following adjustments to the ARCOLA model. First, we updated the model from the original plan characteristics defining the low, medium and high preferred provider organizations (PPOs) to reflect the likely “metallic” choices that are part of the ACA. Combining our knowledge of health insurance with the likely changes to the benefit design of the metallic plan choices, we made the following assumptions: (1) platinum plans would be equivalent to a high PPO option; (2) gold plans would map to a medium PPO option; (3) silver plans would map to a low PPO option; and (4) bronze plans would map to high-deductible health plans (HDHP). We also assumed premiums would increase by 4–8 % depending on the plan choice.
Second, we incorporated Medicaid expansion for states opting in for the expansion as of November, 2013. We used data from the Kaiser Family Foundation on benefit coverage and cost of acute-care Medicaid programs by state to simulate the expansion of the Medicaid population. Third, we factored in the health status of an individual (specifically for those with chronic conditions) assuming a person’s health status may predict which plan he or she chooses. To do this, we created a dummy variable to denote the presence of chronic illness. Since a sick person will likely drive premiums up, incorporating this variable into the model allowed for a more accurate adjustment to overall premiums and cost sharing.
After all adjustments were made, we then used claims data as well data from ehealthinsurance.com to estimate premiums offered and resulting take-up of insurance in the private health insurance market including the Medicare Advantage market, as well as estimate take-up of insurance under the Medicare Fee-for-Service sector. We then used a multi-payer insurance claims database to measure utilization of health services by type of insurance in order to develop demand projections within each health care sector.
Rights and permissions
About this article

Cite this article
Frogner, B.K., Spetz, J., Parente, S.T. et al. The demand for health care workers post-ACA. Int J Health Econ Manag. 15, 139–151 (2015). https://doi.org/10.1007/s10754-015-9168-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10754-015-9168-y