
Abstract
Obesity is associated with an increased risk of incident heart failure with preserved ejection fraction (HFpEF) and, among patients with existing heart failure, is associated with worse quality of life, higher symptom burden, and more HF hospitalizations. Anti-obesity medication (AOM) semaglutide has been shown to be efficacious at both causing intentional weight loss and improving HF symptom burden, with some evidence to suggest that HF clinical events may also be reduced. Additional ongoing trials of AOM in patients with cardiovascular disease, including HFpEF, will further improve insight into the potential role of managing obesity to improve HF status among patients with HFpEF and obesity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
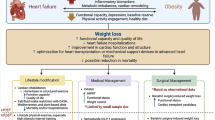
Obesity is a key risk factor for the development of heart failure, particularly heart failure with preserved ejection fraction (HFpEF) [1, 2]. Among patients with HFpEF, those with comorbid obesity report higher symptom burdens, lower quality of life, and experience higher rates of HF hospitalization when compared to patients without obesity [3,4,5]. The high burden of HF symptoms experienced by patients with comorbid obesity has been further complicated by limited pharmacologic therapies that have been available to treat either HFpEF or obesity. However, recent advances offer new opportunities to improve care for patients with HFpEF, particularly those with obesity. Sodium-glucose cotransporter 2 inhibitors dapagliflozin and empagliflozin have now been shown to improve outcomes for patients with HFpEF across a range of BMIs [5,6,7]. Among patients with obesity, emerging evidence suggests that the use of emerging anti-obesity medications (AOMs) to support intentional weight loss may improve HF status, with clearly demonstrated improvements in functional status and symptom burden and possible improvements in clinical outcomes including cardiovascular (CV) death and HF decompensations (Fig. 1). Furthermore, additional AOMs are currently under development, many of which are being explicitly tested among patients with established CV disease, including HFpEF. Here, we explore the evidence available supporting the use of AOMs to improve HF status, review new AOMs under development, and discuss areas for future research.

Heart failure with preserved ejection fraction and obesity:current knowledge and areas for future research. AOM, anti-obesity medications; BMI, body mass index; HFpEF, heart failure with preserved ejection fraction; MACE, major adverse clinical events; T2DM, type 2 diabetes
Obesity as a driver of incident heart failure with preserved ejection fraction and worse heart failure status
The relationship between elevated BMI and risk of incident heart failure has been well described: some studies have suggested that each progressive 1-point increase in body mass index (BMI) above normal is associated with a 5–7% increase in incident HF [2]. Obesity appears to be a particularly significant risk factor for the development of HFpEF [1]. As a result, up to two-thirds of patients living with HFpEF are also overweight or have obesity [8]. Among patients with HFpEF, those who also have obesity experience higher rates of HF hospitalizations and report more HF symptoms and lower quality of life [3,4,5].
Using anti-obesity medication semaglutide to improve heart failure status: available evidence
Theoretically, one possible way to mitigate the relationship between obesity and worse HF status would be to minimize obesity via intentional weight loss. Historically, clinicians and researchers have been thwarted in the pursuit of intentional weight loss due to the limited effectiveness and sustainability of available options. Even within the setting of a clinical trial with strong support and feedback, intentional weight loss among patients with obesity has been shown to be difficult to achieve and, among patients achieving intentional weight loss, difficult to maintain [9, 10]. In one trial of 60 patients with HFpEF and obesity, participants were provided with counseling and meal replacements to support intentional weight loss efforts: despite this, one-third of patients did not complete the 15-week program, and only three-quarters of the patients who did complete the program experienced weight loss. However, patients who did lose weight had significant improvements in reported quality of life as well as exercise capacity, with a degree of weight loss, correlating strongly with a degree of improvement, suggesting that though intentional weight loss via behavior changes is often not achieved, successful weight loss does lead to improvements in HF status [10].
For patients unable to achieve intentional weight loss via behavioral changes, the use of AOMs has been limited by both the modest efficacy of most therapies, as well as CV safety concerns, particularly for patients with existing CV conditions, including HF [11,12,13,14,15]. However, recent evidence suggested that GLP1-RA semaglutide may be safe and effective at inducing intentional weight loss, improving symptom burden and physical limitations, and possibly improving HF outcomes [16,17,18,19].
The Semaglutide Treatment Effect in People with Obesity and Heart Failure with Preserved Ejection Fraction (STEP-HFpEF) and STEP-HFpEF DM trials evaluated the use of semaglutide (2.4 mg once weekly subcutaneously) vs placebo among patients with HFpEF with and without type 2 diabetes (T2DM) for 52 weeks [17, 18]. At the end of each trial, patients randomized to semaglutide had lost significantly more weight (13.3% with semaglutide vs 2.6% with placebo in STEP-HFpEF and 9.8% with semaglutide vs 3.4% with placebo in STEP-HFpEF DM, both p < 0.001) and reported significantly larger improvements in their Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS), an assessment of symptom burden as well physical, emotional, and social limitation (16.6 vs 8.7 points in STEP-HFpEF and 13.7 points with semaglutide vs 6.4 points in STEP-HFpEF DM, both p < 0.001) [20]. Patients in both trials taking semaglutide also had significantly larger improvements in their 6-min walk test distance. In patients with obesity without HF, intentional weight loss is associated with increases in NT-proBNP. Somewhat paradoxically, patients in the STEP-HFpEF and STEP-HFpEF DM trials, randomized to semaglutide instead had significant decreases in NT-proBNP, supporting a reduction in cardiac stress via semaglutide, though the degree to which this was moderated by weight loss versus other mechanisms remains unclear [21, 22]. This observation was further supported by the observation that patients on loop diuretics at baseline in the trial had the largest improvements in KCCQ-CSS [23]. Furthermore, patients randomized to semaglutide were less likely to have their loop diuretic dose increased over the course of the trial and were in fact more likely to have their dose reduced. Loop diuretics are the mainstay therapy to manage volume status and cardiovascular congestion in HF, and these findings further support a direct improvement in HF status related to semaglutide use. Though relatively few HF hospitalizations occurred in either trial, they were numerically less likely to occur among patients randomized to semaglutide (1 vs 12 HF hospitalizations in STEP-HFpEF and 7 vs 18 in STEP-HFpEF DM among patients randomized to semaglutide vs placebo). Consistent with prior studies, though patients with T2DM randomized to semaglutide lost significantly more weight than those randomized to placebo, their absolute magnitude of weight loss was less than that of patients with T2DM (9.8% vs 13.3%) [16,17,18, 23, 24]. Despite experiencing a lesser degree of weight loss, patients with T2DM randomized to semaglutide experienced similar improvements in KCCQ-CSS, 6-min walk test distance, and NT-proBNP, which may suggest that some of the benefits associated with semaglutide were independent of weight loss, or alternatively that patients with T2DM experience a relatively higher burden of symptoms related to HF and obesity. Importantly, semaglutide was well-tolerated within both trials. Overall, the STEP-HFpEF and STEP-HFpEF DM trials suggest that semaglutide can be used safely among patients with HFpEF and obesity to pursue (1) intentional weight loss and (2) improvements in HF symptoms and functional status, with possible evidence of direct cardiovascular benefit.
These findings are further supported by a recent secondary analysis from the Semaglutide Effects on Cardiovascular Outcomes in People with Overweight or Obesity (SELECT) trial. Not primarily designed as a HF trial, SELECT enrolled patients with any cardiovascular disease, including HF who also had overweight or obesity (BMI ≥ 27 kg/m2), excluding patients with T2DM [25]. Of the patients enrolled, 12.9% (n = 2268) had HFpEF [26]. Patients with HFpEF enrolled in SELECT and randomized to semaglutide experienced significant reductions in a composite of CV death, non-fatal MI, and non-fatal stroke (HR 0.69, 95% CI 0.51–0.91) and had a lower risk of experiencing CV or an urgent HF visit (HR 0.75, 95% CI 0.52–1.07), though this did not meet statistical significance [19]. As in the STEP-HFpEF and STEP-HFpEF DM trials, semaglutide was well-tolerated among patients with HFpEF, with numerically more overall and specifically CV adverse events seen in patients randomized to placebo than in those randomized to semaglutide. Though these results are reassuring, there remains a need for dedicated trials powered to evaluate the impact of AOMs, including semaglutide, on long-term HF events.
Emerging anti-obesity medications and their potential application in heart failure with preserved ejection fraction
Additional AOMs beyond semaglutide are currently being evaluated for use in HFpEF and/or in patients with CV disease. These therapies are primarily incretin-based, with the action via agonism of GLP1-R, glucose-dependent insulinotropic polypeptide (GIP), and/or the glucagon receptor (GCGR). However, some emerging AOMs in early development act via non-incretin base pathways. Of these AOMs, tirzepatide is the only other AOM beyond semaglutide that is currently available clinically. Like semaglutide, tirzepatide acts as a GLP1R agonist but also acts via GIP agonism, with a modestly higher observed magnitude of weight loss when compared with semaglutide among patients with obesity (14.9% with semaglutide vs 20.9% with tirzepatide) [16, 27]. The ongoing Study of Tirzepatide in Participants with Heart Failure With Preserved Ejection Fraction and Obesity (SUMMIT) trial will test the tirzepatide in patients with HFpEF and obesity with a primary hierarchical endpoint of death, HF events, change in 6-min walk test distance, and change in KCCQ score [28]. Additional work is being done in the Study of Tirzepatide on the Reduction on Morbidity and Mortality in Adults with Obesity (SURMOUNT MMO) trial, which will evaluate a composite endpoint of death, non-fatal myocardial infarction, non-fatal stroke, coronary revascularization, and HF hospitalization/urgent visit in adults with or at high risk for CV disease with overweight or obesity [29]. Though this trial is not designed or powered to specifically evaluate HF outcomes among patients with HFpEF, patients with HFpEF will be included, and secondary analyses are expected to further understand the impact of tirzepatide on intentional weight loss within this population.
Multiple other drugs are currently being developed for intentional weight loss, many of which have planned or ongoing trials among patients with CV disease, though no HFpEF-specific trials have yet been announced. Cagrilintide/semaglutide, a combination drug that combines semaglutide with amylin analogue cagrilintide, is being tested among patients with CV disease and overweight or obesity (BMI ≥ 25 kg/m2) with a primary outcome of CV death, non-fatal-myocardial infarction, and non-fatal stroke. This trial is anticipated to include patients with HFpEF, and HF events will be a secondary endpoint [30]. Cagrilinitide/semaglutide has previously been tested among patients with overweight or obesity and T2DM, where it was associated with a 15.6% decrease in body weight [31].
Additional GLP1-RAs under development include orforglipron, pemvidutide, survodutide, and retatrutide. Orforglipron resulted in significant weight loss (14.7%) among patients with overweight or obesity in a Phase 2 trial. Orforglipron is currently being evaluated against insulin glargine in a trial of patients with T2DM, increased CV risk, and overweight or obesity with a composite outcome of CV death, non-fatal stroke, non-fatal myocardial infarction, or hospitalization for unstable angina [32, 33]. Pemvidutide, which additionally agonizes GCGR, has reported, though unpublished, efficacy in weight loss, and no CV safety or efficacy data are currently available [34]. Survodutide, which acts as a GLP1-RA and also via GCGR agonism has similarly shown efficacy in Phase 2 trials at inducing intentional weight loss. Survodutide is also being tested in a Phase 3 trial of patients with overweight or obesity with weight-related complications, and either CV or kidney disease is ongoing. This trial will evaluate a composite endpoint of CV death, HF events, non-fatal stroke, and non-fatal myocardial infarction or ischemia-related coronary revascularization [35]. Triple agonist retatrutide induces weight loss by agonizing GP1R, GCGR, and GIP with a magnitude of weight loss that may exceed currently available AOMs [36]. Retatrutide is currently being tested among patients with obesity and CV disease, albeit in a trial is designed to explore changes in body weight rather than CV endpoints [37].
Finally, some limited data are available on emerging non-GLP1-based AOMs. HU6, a controlled metabolic accelerator that increases rates of fat and sugar oxidation, has been associated with a 2.7 kg weight loss over 61 days in patients with overweight or obesity and metabolic-associated fatty liver disease. Interestingly, this weight loss was almost exclusively attributable to loss of adipose tissue, with preservation of muscle mass [38]. In most cases of intentional weight loss, both adipose tissue and skeletal muscle are lost: this has previously been a source of concern among patients with HF, who may be prone to sarcopenia as their disease progresses [15, 39, 40]. HU6 is currently being tested in a Phase 2 trial of patients with HFpEF, with a primary outcome of weight loss at 5 months (NCT05284617) [41].
Taken together, these data will help establish the role of incretin-based therapy in both (1) treating obesity and (2) preventing HF-related events among patients with HFpEF and obesity. However, important questions remain. As more trials, particularly of AOMs that induce weight loss via non-incretin-based mechanisms, are conducted, it may also be possible to start to understand the degree to which weight loss per se drives any observed benefit in HF events. It is also not known whether it may be possible to withdraw these drugs without losing any observed weight loss or CV benefit. Prior work has suggested that withdrawal of semaglutide resulted in significant weight regain as well as worsening in markers of cardiometabolic risk [42, 43]. However, it may be possible that after a longer duration of therapy, or with initiation of other weight-loss sustaining interventions or resources, benefits could be sustained with partial or complete withdrawal of an AOM, though no evidence exists at this time to support this hypothesis.
Importantly, current guidelines from major CV societies only support intentional weight loss in patients with HF and a BMI of ≥ 35 kg/m2 and are limited to only 5–10% of body weight [44,45,46]. However, many of the ongoing trials will include patients with BMIs down to 27 kg/m2 and will test AOMs that have led to > 20% weight loss in other populations. Existing evidence suggests that for patients with HFpEF, increasing BMI above a normal range (18.5–25 kg/m2) is associated with a linear increase in risk for HF hospitalization, and dedicated trials of patients with HFpEF and obesity have shown consistent evidence of improved functional status and symptom burden down to a BMI of at least 30 kg/m2, with the greatest benefits seen with a higher degree of weight loss, which substantially exceeded 10% [5, 47]. If ongoing trials continue to show a similar benefit in reduction in clinical events, it is likely that future guidelines will recommend pursuing intentional weight loss at lower BMIs, as well as higher magnitudes of weight loss in excess of 5–10%. Additional work is needed to further understand whether there is an ideal BMI target or percent weight loss goal that would maximize CV benefit.
Conclusion
Obesity represents a common and substantial cause of HFpEF. Among patients with established HFpEF, obesity is associated with lower quality of life, higher symptom burden, and increased risk for HF hospitalization. Emerging AOMs may offer an opportunity to reduce the burden of HF symptoms associated with obesity. Data have shown that AOM semaglutide is effective at inducing weight loss, improving symptom burden and exercise capacity, and possibly at reducing HF hospitalization among patients with HFpEF and obesity, and research is ongoing to understand whether these benefits are also observed with tirzepatide. Furthermore, additional AOMs are currently in development and may offer additional insight into the role of intentional weight loss in the management of HFpEF for patients with comorbid obesity. Future work is needed to fully define the impact of intentional weight loss on clinical outcomes and to understand whether it is the mechanism or magnitude of weight loss that drives any observed changes in outcomes.
References
Pandey A, LaMonte M, Klein L et al (2017) Relationship between physical activity, body mass index, and risk of heart failure. J Am Coll Cardiol 69:1129–1142
Kenchaiah S, Evans JC, Levy D et al (2002) Obesity and the risk of heart failure. N Engl J Med 347:305–313
Borlaug BA, Jensen MD, Kitzman DW, Lam CSP, Obokata M, Rider OJ (2022) Obesity and heart failure with preserved ejection fraction: new insights and pathophysiological targets. Cardiovasc Res cvac120
Obokata M, Reddy YNV, Pislaru SV, Melenovsky V, Borlaug BA (2017) Evidence supporting the existence of a distinct obese phenotype of heart failure with preserved ejection fraction. Circulation 136:6–19
Adamson C, Kondo T, Jhund P et al (2022) Dapagliflozin for heart failure according to body mass index: the DELIVER trial. Eur Heart J 43:4406–4417
Anker SD, Butler J, Filippatos G et al (2021) Empagliflozin in heart failure with a preserved ejection fraction. NEJM. 385:1451–1461
Sattar N, Butler J, Lee MM et al (2024) Body mass index and cardiorenal outcomes in the EMPEROR-Preserved trial: principal findings and meta-analysis with the DELIVER trial. Eur J Heart Fail. Published online 1 April 2024. https://doi.org/10.1002/ejhf.3221
Joyce E, Lala A, Stevens SR et al (2016) Prevalence, profile, and prognosis of severe obesity in contemporary hospitalized heart failure trial populations. JACC Heart Fail 4:923–931
The LOOK AHEAD Investigators (2013) Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med 369:145–154
El Hajj EC, El Hajj MC, Sykes B et al (2021) Pragmatic weight management program for patients with obesity and heart failure with preserved ejection fraction. J Am Heart Assoc 10:e022930
Kolata G. How Fen-Phen (1997) A diet “miracle,” rose and fell. The New York Times.
James WPT, Caterson ID, Coutinho W et al (2010) Effect of sibutramine on cardiovascular outcomes in overweight and obese subjects. N Engl J Med 363:905–917
Colman E, Golden J, Roberts M, Egan A, Weaver J, Rosebraugh C (2012) The FDA’s assessment of two drugs for chronic weight management. N Engl J Med 367:1577–1579
Blüher M, Aras M, Aronne LJ et al (2023) New insights into the treatment of obesity. Diabetes Obes Metab 25:2058–2072
Harrington J, Felker GM, Lingvay I, Pagidipati NJ, Pandey A, McGuire DK (2024) Managing obesity in heart failure: a chance to tip the scales? JACC Heart Fail 12:28–34
Wilding JPH, Batterham RL, Calanna S et al (2021) Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med 384:989–1002
Kosiborod MN, Abildstrøm SZ, Borlaug BA et al (2023) Semaglutide in patients with heart failure with preserved ejection fraction and obesity. N Engl J Med 389:1069–1084
Kosiborod MN, Petrie MC, Borlaug BA et al (2024) Semaglutide in patients with obesity-related heart failure and type 2 diabetes. N Engl J Med 390:1394–1407
Deanfield JE (2024) Semaglutide and cardiovascular outcomes in patients with overweight or obesity and heart failure: a pre-specified analysis from the select tria.l Euro Soc Cardiol Heart Fail Congress
Spertus JA, Jones PG, Sandhu AT, Arnold SV (2020) Interpreting the Kansas City Cardiomyopathy Questionnaire in clinical trials and clinical care: JACC state-of-the-art review. J Am Coll Cardiol 76:2379–2390
Madamanchi C, Alhosaini H, Sumida A, Runge MS (2014) Obesity and natriuretic peptides, BNP and NT-proBNP: mechanisms and diagnostic implications for heart failure. Int J Cardiol 176:611–617
Hollstein T, Schlicht K, Krause L et al (2021) Effect of various weight loss interventions on serum NT-proBNP concentration in severe obese subjects without clinical manifest heart failure. Sci Rep 11:10096
Shah SJ, Sharma K, Borlaug BA et al (2024) Semaglutide and diuretic use in obesity-related heart failure with preserved ejection fraction: a pooled analysis of the STEP-HFpEF and STEP-HFpEF-DM trials. Eur Heart J ehae322
Davies M, Færch L, Jeppesen OK et al (2021) Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. The Lancet 397:971–984
Lincoff AM, Brown-Frandsen K, Colhoun HM et al (2023) Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med 389:2221–2232
Lingvay I, Brown-Frandsen K, Colhoun HM et al (2023) Semaglutide for cardiovascular event reduction in people with overweight or obesity: SELECT study baseline characteristics. Obesity (Silver Spring) 31:111–122
Jastreboff AM, Aronne LJ, Ahmad NN et al (2022) Tirzepatide once weekly for the treatment of obesity. N Engl J Med 387:205–216
Eli Lilly and Company. A study of tirzepatide (LY3298176) in participants with heart failure with preserved ejection fraction and obesity. ClinicalTrials.gov. Accessed 22 July 2023. https://clinicaltrials.gov/ct2/show/NCT04847557
Eli Lilly and Company. A study of tirzepatide (LY3298176) on the reduction on morbidity and mortality in adults with obesity (SURMOUNT-MMO) Accessed 8 July 2023. https://clinicaltrials.gov/study/NCT05556512
Novo Nordisk A/S (2023) The cardiovascular safety of cagrilintide 2.4 mg s.c. in combination with semaglutide 2.4 mg s.c. (CagriSema 2.4 mg/2.4 mg s.c.) once-weekly in participants with obesity and established cardiovascular disease. clinicaltrials.gov
Frias JP, Deenadayalan S, Erichsen L et al (2023) Efficacy and safety of co-administered once-weekly cagrilintide 2·4 mg with once-weekly semaglutide 2·4 mg in type 2 diabetes: a multicentre, randomised, double-blind, active-controlled, phase 2 trial. Lancet 402:720–730
Eli Lilly and Company (2023) A phase 3, randomized, double-blind study to investigate the efficacy and safety of once-daily oral LY3502970 compared with placebo in adult participants with obesity or overweight with weight-related comorbidities (ATTAIN-1). clinicaltrials.gov.
Eli Lilly and Company (2023) A phase 3, open-label study of once daily LY3502970 compared with insulin glargine in adult participants with type 2 diabetes and obesity or overweight at increased cardiovascular risk. clinicaltrials.gov.
Anon. Altimmune obesity drug well-positioned despite safety data. BioSpace Accessed 3 Sept 2023. https://www.biospace.com/article/altimmune-shares-plunge-on-obesity-data-over-safety-concerns-/
Boehringer Ingelheim (2024) A phase 3, randomised, double-blind, parallel-group, event-driven, cardiovascular safety study with BI 456906 administered subcutaneously compared with placebo in participants with overweight or obesity with established cardiovascular disease (CVD) or chronic kidney disease, and/or at least two weight-related complications or risk factors for CVD. clinicaltrials.gov.
Jastreboff AM, Kaplan LM, Frías JP et al (2023) Triple–hormone-receptor agonist retatrutide for obesity — a phase 2 trial. N Engl J Med 389:514–526
Eli Lilly and Company (2023) A randomized, double-blind, phase 3 study to investigate the efficacy and safety of LY3437943 once weekly compared to placebo in participants with severe obesity and established cardiovascular disease. clinicaltrials.gov.
Noureddin M, Khan S, Portell F et al (2023) Safety and efficacy of once-daily HU6 versus placebo in people with non-alcoholic fatty liver disease and high BMI: a randomised, double-blind, placebo-controlled, phase 2a trial. Lancet Gastroenterol Hepatol 8:1094–1105
Horwich TB, Fonarow GC, Clark AL (2018) Obesity and the obesity paradox in heart failure. Prog Cardiovasc Dis 61:151–156
Bikou A, Dermiki-Gkana F, Penteris M, Constantinides TK, Kontogiorgis C (2024) A systematic review of the effect of semaglutide on lean mass: insights from clinical trials. Expert Opin Pharmacother 25:611–619
Rivus Pharmaceuticals, Inc. (2023) Exploratory phase 2a, double-blind, placebo-controlled, dose escalation study to determine the safety, tolerability, PD, and PK of HU6 for the treatment of subjects with obese Heart Failure with Preserved Ejection Fraction (HFpEF). clinicaltrials.gov
Rubino D, Abrahamsson N, Davies M et al (2021) Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA 325:1414–1425
Wilding JPH, Batterham RL, Davies M et al (2022) Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP 1 trial extension. Diabetes Obes Metab 24:1553–1564
Bozkurt B, Aguilar D, Deswal A et al (2016) Contributory risk and management of comorbidities of hypertension, obesity, diabetes mellitus, hyperlipidemia, and metabolic syndrome in chronic heart failure: a scientific statement from the American Heart Association. Circulation 134:e535–e578
Vest AR, Chan M, Deswal A et al (2019) Nutrition, obesity, and cachexia in patients with heart failure: a consensus statement from the Heart Failure Society of America Scientific Statements Committee. J Card Fail 25:380–400
Ponikowski P, Voors AA, Anker SD et al (2016) ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 37:2129–2200
Borlaug BA, Kitzman DW, Davies MJ et al (2023) Semaglutide in HFpEF across obesity class and by body weight reduction: a prespecified analysis of the STEP-HFpEF trial. Nat Med 29:2358–2365
Author information
Authors and Affiliations
Contributions
Manuscript drafted, written, and revised by JH.
Corresponding author
Ethics declarations
Conflict of interest
JH is an Associate Editor of the journal; she reports no other disclosures.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Harrington, J. Anti-obesity medications in the management of heart failure with preserved ejection fraction: available evidence and next STEPS. Heart Fail Rev 29, 939–944 (2024). https://doi.org/10.1007/s10741-024-10410-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10741-024-10410-0