
Abstract
This research work aims to illustrate the geographical distribution and cluster patterns of domestic medical tourism demand in Northeast India based on the field survey from the destination Kolkata. The study was carried out in two steps, firstly, we obtained demographic and spatial information on domestic medical tourists (DMTs) traveling from 8 states of north-eastern India and visiting Kolkata, West Bengal, India to seek medical care; and then we used a Geographical Information Systems (GIS) approach to develop a spatial database, and used the ArcGIS geostatistical analysis module to explore the geographical extent, distribution pattern and spatial clustering of the source location of these medical tourists. During our study period of December 2017 to December 2018, we have received response from all the eight states of the northeast. Analysis of results exhibit that major northeastern domestic medical tourism demand regions lie over the western boundary of Tripura, south-eastern Sikkim, and central Mizoram, central Manipur, and the south-eastern region of Nagaland. We observe the district-wise spatial clusters in almost all the districts of Tripura and Mizoram, the major contributor to the domestic medical tourism segment of northeast India. Five major demand factors namely, super-specialized infrastructure, access to medical care information, cost-savings, quality of care, and treatment availability within minimum distance and time were found to be suitable in explaining the medical tourism from northeast India. This study is unique in the field of medical tourism that attempts to measure the degree of association among medical tourism generating regions at a micro-scale. Results indicate the strong spatial effect, and noted that domestic medical tourism demand is localized in nature that is highly controlled by the physician referral system, patient preferences and choices, and availability of financial and logistical support with flexible health insurance schemes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Traveling to access medical care to non-local facilities within the jurisdictional territory of the nation or country (Burns, 2015), contributes to the largest sphere of the medical tourism demand on the global scale (Hudson & Li, 2012). Regional disparity in healthcare services, urban-biased in healthcare infrastructure development, and increasing consumerism in accessing the tertiary healthcare infrastructure are cited as the most relevant factors behind the practice of domestic medical tourism (Cohen, 2010). Domestic medical tourism is cited as the viable solution in response to the healthcare disparity in third-world countries (Biswas & Rai, 2022). Cohen (2010) believes that domestic medical tourism will significantly rise in the countries like India, Malaysia, Thailand, and China. In fact, as a viable tool of healthcare reform, domestic medical tourism is widely promoted across the globe. Countries like the USA (Nwachukwu et al., 2015), Australia (Tham, 2018), Germany (Salm & Wübker, 2019), Italy (Manna et. al., 2020), and China (Chia & Liao, 2020) have successfully implemented national-level initiatives to promote the domestic medical travel.
Acknowledgement of domestic medical tourism as a double-edged tool of healthcare reforms and revenue generator for the regional economy has recently drawn the attention of academia (Tham, 2018). Few scholars have carried out empirical research to investigate the profile, motivations, and experience of domestic medical tourists to understand the nature of domestic medical tourism demand from the perspective of consumer of the services (Biswas & Rai 2022; Manna et. al., 2020; Rouland & Jarraya, 2020). However, measuring geographical and spatial effects on domestic medical tourism demand is highly ignored in the existing literature. Perhaps, it is imperative to understand the geographies of medical tourism.
Many research studies have explored the geographical and spatial clustering of tourism demand and argued that studying the spatial pattern of tourism demand yields more valuable results and can provide a scientific and empirical reference to local governments, tourism planners, and administrative units regarding resource allocation and infrastructure development (Ma et al., 2022). Deng and Athanasopoulos (2011) incorporated spatiotemporal dynamics into an Australian domestic tourism demand model study. Yang and Zhang (2019) found that spatio-temporal models have a significantly enhanced effect on the domestic tourism demand forecasting in China. Similar social psychology, tourism demand, travel patterns, and spatial preference are noted for the tourists originating from the same region (Ma et al., 2022; Massidda & Etzo, 2012). Although, the analysis of spatial patterns of domestic tourism demand has gained scholarly attention, to our knowledge no study contemplates the same in exploring the niche demand of medical tourism. To fill this knowledge gap, this research aims to explore the spatial patterns and driving factors of domestic medical tourism demand in the South Asian region. The study uses the empirical data acquired from the primary surveys on domestic medical tourists (DMTs). Spatial, demographic, and trip profile data of traveling patients are further analyzed to unwrap the medical tourism demand factors in South Asia by adopting a case study on Indian DMTs originating from northeastern region. The countries of South Asia include Pakistan, Afghanistan, Bangladesh, Bhutan, India, the Maldives, and Bangladesh. Each country in this incredibly diverse region has very distinct populations, developmental stages, and health metrics. Despite nation-specific difficulties, regional problems with the health system's operation are commonly shared (UNICEF, 2021), such as the accessibility of services in terms of geography, the availability of essential medicines and supplies, a lack of funding for the sector (Sengupta et al., 2018), the unequal distribution of health workers between the public and private sectors, out-of-pocket expenses for their services (Kumar, 2019), and need-based regional medical travel (Biswas & Rai, 2022). In fact, in South Asia, domestic medical tourism is a solution to need-based medical travel through which chronic and everyday healthcare needs are met (Ormond & Sulianti, 2017). Domestic medical tourism is also acknowledged as the undisputed driver of healthcare development. Few studies provide a unique example of enhanced service expansion and capacity building where medical tourism has changed the health landscape of city and repositioned its existence in the global healthcare market (Rai, 2019).
India not only serves as a popular medical tourism destination for its South Asian neighbours, but it also represents the particular traits of the region's medical tourism system, in which the majority of local medical travel is need-based (Khan et al., 2017). As a worldwide player in medical tourism, India's medical tourism system has piqued the interest of academics (Collins et al., 2019), yet a significant portion of domestic medical tourism demand remains unexplored (Chakrabarti & Tatavarthy, 2019). We select the northeast region of India to pursue the present study. The unique socio-economic territory of Northeast India (Dikshit & Dikshit, 2014) contributes to the major segment of domestic medical tourism in India (Chakrabarti & Tatavarthy, 2019) and represents unique domestic medical tourism generating region of South Asia, where most of the medical travel is need-based and driven by restrictive conditions (Khan et. al., 2017). DMTs are present in almost all of India's major cities (NCDIR, 2017). We chose the metropolitan city of Kolkata as the domestic medical tourists' destination for northeastern patients to conduct our case study given the importance of source–destination proximity in destination selection (Mishra & Bansal, 2017) and the city's significant contribution to luring domestic medical tourists from the region (Biswas & Rai, 2022). We include primary domestic medical tourists’ surveys of those who are visiting Kolkata.
Research objectives and hypotheses
This study attempts to analyse domestic medical tourism demand, geographical direction, distribution, clustering, and spatial heterogeneity using empirical data from northeastern domestic medical tourists (DMTs) arriving in Kolkata. The country of origin has a considerable impact on the travel motivations of medical tourists at the national level (Jaapar et al., 2017). However, how various medical travel motivations are constructed within a country's national boundaries of similar geographical and need-based context, has received little attention in academia (Biswas & Rai, 2022). This research is intended to fill this information gap. We intend to test the following hypotheses based on our existing knowledge of domestic medical tourism in South Asian context:
H1
Demand for medical travel is not randomly distributed across the northeastern states.
H2
Medical tourism demand is clustered in the northeastern states.
H3
Geographical location significantly affects the demand and travel motivations for domestic medical tourism in northeastern states.
Literature review
Geography of domestic medical tourism
Domestic medical tourism includes the act of travel to access medical care to non-local facilities within the jurisdictional territory of the nation or country (Hudson & Li, 2012). The practice of intra-bound medical tourism or domestic medical tourism is on the rise worldwide where a significant share of the medical tourism industry is occupied by domestic buyers (Tham, 2018). The prevalence of such practices is assumed to be contributed by the availability of medical specialists, decreased waiting time, advanced medical care, lower cost of complex medical procedures, and availability of individual insurance coverage (Keckley & Underwood, 2008). In the United States, more employers and insurers are encouraged through financial assistance to opt for treatment within the USA (Kwong et al., 2019). NSSO 72nd round states that in India, 90 overnight trips per 100 rural tourist households and 51 overnight trips per 100 urban tourist households were undertaken from June 2014 to Jun 2015 with the leading purpose of health and medical (Chakrabarti & Tatavarthy, 2019). In Italy, more than 80% tourists are domestic health tourists (Manna et. al., 2020). China (Chia & Liao, 2020), Australia (Tham, 2018), Germany (Salm & Wübker, 2019), Indonesia (Ormond et al., 2017), and many other countries have been promoting domestic medical travel on a national scale. Despite the enormous effects of domestic medical tourism on the medical tourism industry, academic research on the spatiality of domestic medical tourism demand is still lacking. Many academic studies have focused on the characteristics and demand of international medical tourists (Collins et al., 2019; Medhekar & Wong, 2020); nevertheless, it is necessary to examine the geographical characteristics of domestic medical tourists in order to comprehend the geography of medical tourism.
Domestic medical tourism demand
Scholars have attempted to identify the geographical and spatial clustering of domestic tourism demand. Spatio-temporal models found enhanced effect on the domestic tourism demand forecasting in China (Yang & Zhang, 2019). Ma et al. (2022) have applied spatial pattern analysis and predicted the provincial tourism demand in China. Deng and Athanasopoulos (2011) incorporated spatiotemporal dynamics into an Australian domestic tourism demand model study. However, to our knowledge, no scholarly attempts have been made in exploring the geographical and spatial clustering of domestic medical tourism demand, exclusively in context of South Asia. Perhaps, studying the spatial pattern of tourism demand yields more valuable results and can provide a scientific and empirical reference to local governments, tourism planners, and administrative units regarding resource allocation and infrastructure development (Ma et al. (2022). This study aims to fill this gap and from the perspective of micro-planning. It attempts to analyse the clustering, geographical direction, and heterogeneity of the domestic medical tourism demand in the context of third world adopting a case study of northeast India, where medical tourism is need-based geographical phenomenon (Khan et. al., 2017).
Spatiality of travel motivation
“Travel motivation is the inner state of a person, or certain needs and wants of the tourists that can be considered as one of the most important psychological influences of tourist behaviour” (Bhattacharya & Kumar, 2017, 443). Exploring factors motivating the medical tourism movement is the core focus of the available pieces of literature. Research has focused extensively on the push and pull elements of medical tourism decision-making (John & Larke, 2016). Diverse socio-demographic and health characteristics of individual visitors (John & Larke, 2016; Fetscherin & Stephano, 2016); geographic inequalities in the delivery of healthcare services (Ngaihte et al., 2019); regional variations in timely access to care (Croome et al., 2015); inter- and intra-regional level physician referral systems (Salm & Wübker, 2019); and variances in health insurance benefits (Kwong et al., 2019); the developing online market for medical care services (Turner, 2012); and presence of a geographically proximate medical tourism destination (Mishra & Bansal, 2017) are commonly cited travel motivators. Academics have frequently discussed how travel intentions or motivations differ among countries (Lunt et al., 2016; Jaapar et. al., 2017; Rai, 2019). However, there have been few scholarly endeavours done at the micro level (Balia et al., 2018; Han et al., 2018; Rouland & Jarraya, 2020). This study empirically investigates the geographic disparities in the travel motive of DMTs and decision-makings delving down at state level geographical linkages, acknowledging the significance of demarcating medical tourism demand at the micro-scale that is essential for understanding the geographies of medical tourism.
Study area
To address our research aim, we have selected the northeastern states of India (Fig. 1). Chakrabarti and Tatavarthy (2019) investigate the geography of medical travel in India and discover that residents in the northeastern region have a higher share of out-of-state destination choices for medical travels. The northeastern area of India is one of the poorest and most backward regions due to its geographical, cultural, and political sensitivity. It consists of eight states: Arunachal Pradesh, Assam, Manipur, Meghalaya, Mizoram, Nagaland, Sikkim, and Tripura, occupies 7.9% of India's total land area and is home to 8 million people (3.9% of the country's population). Rural areas are home to more than 80% of the population (NECS 2016). The northeastern region of India's health sectors frequently identifies concerns such as impassable hilly terrain, limited access to healthcare facilities, a lack of medical professionals, a high prevalence of vector-borne infectious disease, a high incidence of cancer, and other lifestyle maladies (Dev et al., 2015; Goswami, 2010; Ramashankar & Sharma, 2015;). According to the Indian Council of Medical Research, the majority of patients from northeastern states rely on medical facilities that are located outside (NCDIR (National Centre for Disease Informatics and Research), 2017). To receive treatment for their ailments, thousands of patients from the North-East states come to different Indian metropolises (Ngaihte et al., 2019). We select the metro city of Kolkata given the importance of source–destination proximity in destination selection (Mishra & Bansal, 2017) and the city's significant contribution to attracting domestic medical tourists from the region (Biswas & Rai, 2022).

Study Area
Kolkata is the capital of West Bengal and the gateway to Eastern India. At the time of the 2011 Census, Kolkata had a population of 44,96,694 people, with a density of 24,306 people per km2. It has a higher literacy rate than the overall average of India, which is 74%, at 86.31% (males: 88.34%; females: 84.06%). The city, which is the main economic hub in eastern India, has 60,000 commuters every day (KMC, 2016). The healthcare industry in Kolkata is characterized by cutting-edge, modern, and advanced technology together with a patient-friendly, multi-dimensional approach to healthcare delivery under this dominant paradigm of corporate governance. Kolkata has 62.3 hospital beds per 10,000 people, which is greater than the national average of 9.0 hospital beds per 10,000 people. Kolkata, as the largest city in eastern India, serves not just its own population but the entire state, as well as neighbouring states to the east and northeast, as well as neighbouring countries such as Bangladesh, Bhutan, Nepal, and Myanmar (Rai, 2019 pp. 56).
Materials & methodology
The study was carried out in two steps, firstly we used a structured questionnaire schedule and obtained demographic and spatial information on domestic medical tourists traveling from 8 states of northeastern India and visiting Kolkata, West Bengal India to seek medical care; and then we used a Geographical Information Systems (GIS) approach to develop a spatial database, after which we used the ArcGIS geostatistical analysis module to explore the geographical extent of the source location of these medical tourists. Nearest Neighbour Analysis, Global Moran’s I (Moran, 1950) and Local Moran’s I (Anselin, 1995) were employed to investigate spatial autocorrelation, while Getis-Ord General G (Ord & Getis, 2001) was utilized for cluster analysis. Statistical significance was defined as a P-value of less than 0.05. Descriptive statistical analysis, t-test, and ANOVA tests were executed to map the demographic and trip profile of medical tourists. Exploratory factor analysis with the eigenvalue 1 approach was used to extract major factors affecting medical tourism demand.
Development of survey instruments
We adopt a structured observation method to acquire data from the field. As the survey is conducted at the destination of Kolkata, a questionnaire was designed with a focus on destination-specific pull items. The survey item for this study is adapted from Rai (2019). Survey instruments were developed following two stages—content validity and face validity. Content validation is done through a two-round Delphi study. The responses of eight experts are measured on a 5-point Likert Scale of importance and consensus is obtained (Median ≥ 4, IQR ≤ 2, frequency [4–5] ≥ 70%). Items not matching consensus criteria were removed from the questionnaire and updated questionnaire emailed in round 2. All the responses and suggestions of expert panels on the survey items were collated and used to formulate a refined questionnaire. The face validation of the questionnaire is done through a pilot field study among domestic medical tourists visiting Kolkata. Questionnaires were designed in English.
Data acquisition
We purposely selected 20 hospitals (private = 17; public hospitals = 3) and 9 northeast houses which offer additional accommodation to visitors from the northeastern states traveling to Kolkata. No help was asked from the healthcare service providers, and the DMTs’ survey was conducted in and around hospital premises. The individual persons who manage the north-eastern houses were contacted and the background and nature of the study were explained to them. On their consent, further communication was established with the patients. A letter of intent, a sample questionnaire, and a consent form were sent to individual patients before the survey. The participants who expressed their intent to participate in the survey were further interviewed over the telephone or through face-to-face meetings. In some cases, patients authorized their companions to share their required information on behalf of themselves. No control over the sample size was kept and surveys were conducted from December 2017 to December 2018. We received 336 questionnaire responses from domestic medical tourists. Twenty-four questionnaires (n = 24) were excluded from the analysis due to their incomplete responses. In total, we had 312 (a response rate = 92.86%) usable questionnaires that were included in the study for further analysis. The responses cover the answers to queries about tourists’ demographic and trip profiles, and major factors that influenced the medical tourism decision-making.
Database creation and spatial distribution mapping of tourism demand
Based on the zip code and residence address of the domestic medical tourists, we have developed point data from their geographical information. Geocoding was used to construct a point layer based on the Zip code for each address. The centroid location, directional pattern, compactness, and orientation of domestic medical tourists were determined by standard deviation ellipse or SDE (Fig. 2). The ellipse can be used to detect whether the distribution of features is elongated and, as a result, has a certain orientation (Routh et al., 2022).

Spatial distribution of domestic medical tourism demand in north-eastern India
Spatial pattern analysis
The nearest-neighbor analysis measures the average distance between the centroid locations of each feature and those of its closest neighbours, providing evidence of clustering, random, or regular point patterns (Bishop, 2010; Mitchell, 2005). The average NNR can be computed by dividing the recorded average distance by the expected average distance.
where, \({\overline{D} }_{0}\) is the observed mean distance between each location and its nearest neighbour
where, \({d}_{i}\) equals the distance between location ‘i’ and its nearest neighbouring location,
‘n’ corresponds to the total number of locations,
\({\overline{D} }_{E}\) is the expected mean distance for the location given in a random pattern
‘A’ is the area of a minimum enclosing rectangle around all features or it’s a user-specified area value.
Clustering occurs when the index is less than 1.
The mathematical expression for Global Moran's I, a spatial autocorrelation indicator based on cross products of variables was assessed at the district level:
where n denotes the number of locations;
xi denotes the DMTs presence i; \(\overline{x }\) is the average value of DMTs; and wij denotes the variables of a spatial lag operator W (spatial weights of matrix W). The usefulness of the index is frequently evaluated in a situation with a statistical distribution (Mazzulla & Forciniti, 2012). A positive number denotes the likelihood that a point will be added to its neighbours' points, whilst a negative value denotes the opposite. The value of Global Moran's I ranges from −1 to 1, with a positive number suggesting the contrary.
Join count statistics for medical tourism demand clustering
The degree of clustering or dispersion among a group of spatially contiguous locations can be assessed using join counts statistics (JCSs). It decides whether area i and the neighbourhood exhibit some other type of localised pattern or form a cluster.
It determined by:
Using given formula, we can calculate common low clustering (where both area ‘i’ and the places surrounding it likely to be dispersed):
It may be required to distinguish between low–high associated pairings (bi = 0, bj = 1) and high-low associated pairings (bi = 1, bj = 0) when defining localised patterns. In such circumstances, the two local JCS are identical.
Wij is a binary spatial association and is determined by whether areas ‘i’ and ‘j’ are contiguous (wij = 1) or not (wij = 0). Ni indicate the area i's neighbourhood, i.e., the set of areas adjacent to area ‘i’ (those with wij = 1), and believe that this neighbourhood comprises Li areas (Li = \({J}_{i}+{J}_{0i}+{J}_{10i}+{J}_{01i}\)).
Exploratory factor analysis of driving factors
We have included the ranking of 17 motive items on a 10 – point scale (with "1" denoting the least important factor and "10" denoting the most significant one) in order to determine the key motivating factors influencing the decision of medical tourists. In line with the findings of Taherdoost (2019) and Rai and colleagues (2016), we noticed in our pilot study that respondents preferred scales with greater choices to appropriately describe their feelings; as a result, a 10-point rating scale was used to gather the replies. Exploratory factor analysis was used to evaluate motive items. To determine whether the data are suitable for factor analysis, the KMO measure of sampling adequacy and Bartlett's test of sphericity are applied. To identify important components, the eigenvalue more than one technique is used. The factors were only explained using the items with loadings above 0.40. Internal consistency among the assessed items was more than 0.70. The variability of the factors driving the demand for medical tourism based on the geographic location of medical tourists was investigated using an ANOVA test.
Results
Demographic and trip characteristics of domestic medical tourists originating from Northeast India
As evident from Table 1, our sample includes domestic medical tourists from all the eight states of the northeast during the study period. Based on our sample study we observed that a higher share is contributed from the states of Mizoram (26.28%) and Tripura (25.98%) followed by Sikkim (12.82%), Manipur (9.94%), Nagaland (9.62%), Assam (8.01%), Arunachal Pradesh (4.17%), and Meghalaya (3.21%). The shares of domestic medical tourists’ arrival are inclined towards middle and upper age groups. Male contribution (63.46%) in domestic medical tourism demand is higher than female share (36.45%), and it is visible in all age groups. The service sector or employees of various public and private organizations (49.03%) constitute the major segment of medical tourism demand. Graduation degrees or above is the common level of education attained by these domestic medical tourists.
We also note that almost half (47.44%) of the DMTs were regular consumers. We record diversified demand for medical treatment ranging from cardiology (24.68%), oncology or cancer care (21.47%), and Nephrology (9.29%) to check-ups and consultations. They are mostly referred by the doctors/hospitals of the native state (59.29%). They sometimes rely on the internet (7.73%) to find out the medical travel services out of state. However, most of them relied on the word-of-mouth referrals received from friends, family members, and colleagues (45.83%) or the physicians visited at home. They come with their companions and on average spent about 10 days to 30 days on their medical trip to Kolkata. Most of these medical trips are self-financed (65.38%), however, it is also sponsored under employee (18.91%) or insurance (15.71%) benefits schemes. Despite ‘need-based medical travel conditions’ nearly half of the medical tourists had interacted, consumed, and enjoyed conventional tourism opportunities in and around Kolkata.
Spatial distribution of medical tourism demand at micro-scale
Referring to the spatial distribution map based on the residential address of the medical tourists in Fig. 2, we note that major DMT demand locations lie over the western and northern boundary of Tripura, south-eastern Sikkim, and central Mizoram, central Manipur, and south-eastern region of Nagaland. The ellipse is oriented in a northwest-southeast direction, indicating that majority of domestic medical tourism demands are located in the western and southern parts of the northeastern states (Fig. 2). The p-value for the NNA is less than 0.005 as shown in Table 2, which demonstrates that our result of NNA is significant at the 1% level indicating that demand for medical travel is not randomly distributed across the northeastern states at a 99% significant level, hence accepts H1.
Spatial clustering of medical tourism demand at district level
The Global Moran’s I statistics were used to understand the areal distribution of medical tourism demand within an administrative boundary (Fig. 3). We observe the district-wise spatial clusters in almost all the districts of Tripura and Mizoram, the major contributor to the domestic medical tourism segment of northeast India. Districts like Aizwal, Champhai, Kolasib in Mizoram, West Tripura, Sipahijala, North Tripura, Gomati, Dhalai, and Khowai in Tripura, East Sikkim, and South Sikkim in Sikkim, Imphal East, and Imphal West in Manipur, East Khasi Hills and South West Garo Hills in Meghalaya, Dimapur and Kohima in Nagaland, Papum Pare, and Lower Dibang Valley in Arunachal Pradesh, Jorhat, Kamrup Metropolitan, and Sonitpur in Assam are observed as a major spatial cluster of medical tourism demand at district-level. Table 2 shows the Moran’s I statistic and its p-value. P-value is less than 0.005, demonstrates that there is less than a 1% likelihood that clustered pattern could be the result of random choice. Global Moran’s I test (z scores above 1.96) suggests spatial heterogeneity the null hypothesis of the Global Moran’s I statistics, which contends that the DMT is distributed randomly among the districts of north-eastern states, is rejected (p-value less than 0.05) and accepts H2.

Spatial clustering (global) of domestic medical tourism demand zones in northeast India
The Getis-Ord Gi* tool evaluates the occurrence of DMTs in each district and compares the regional situation in the neighbouring districts to the local situation. The values from Getis-Ord Gi* statistics, z-score, and p-value are displayed in Table 2. These results showed that the spatial autocorrelation was positive and the z-score values were statistically significant at 0.05. The spatial distribution of high and/or low values of DMT demand in the data set was spatially clustered more than expected if the underlying spatial processes were changed. Significant regional clustering of domestic medical tourism is observed in Mizoram and Tripura, as shown by joins count statistics (Fig. 4). High-high DMT demand clusters have been observed over Mizoram's Aizawl and Champhai districts, as well as West Tripura and Sipahijala of Tripura.

DMTs clusters (local) in northeast India
Domestic medical clustering and hotspot
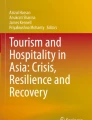
The Hot Spot Analysis tool computes the Getis-Ord Gi* statistic for each feature in a dataset. The obtained z-scores and p-values demonstrate the districts where attributes with either high or low values are clustered geographically. Each characteristic is evaluated in relation to its surroundings. To be a statistically significant hot spot, a feature must have a high value and be surrounded by other features that also have high values. A statistically significant z-score is generated when the local sum of a feature and its neighbours is proportionally compared to the overall number of features. This happens when the local sum deviates significantly from the expected local sum and the discrepancy is too large to be caused by random chance. The Gi* statistic that was provided for each feature in the dataset is known as a z-score. The concentration of high values rises with increasing z-scores for statistically significant positive z-scores (hot spot). For statistically significant negative z-scores, smaller z-scores exhibit more intense low-value clustering (cold spot). The statistically significant hotspot for DMT demand occurrences is shown in Fig. 5. During the study period, Aizawl, Champhai, Mamit, Serchip, Kolasib, and Lunglei (Mizoram); Khowai, West Tripura, and Sipahijala (Tripura); Churachandpur and Cachar (Manipur) and East and North Sikkim (Sikkim) formed significant medical tourism demand hotspots and were estimated to be extremely important districts that require strategic planning to lay the foundations of sustainable domestic medical tourism for eastern India.

DMTs Hotspot in northeast India
Driving factors affecting domestic medical tourists’ travel motivation
On a total of 17 structured questions that were created during the questionnaire design, we evaluate the domestic medical travel motivations. According to Table 3, the data are acceptable for the factor analysis according to the KMO measure of sample adequacy (0.803) and Bartlett's sphericity test (P<0.000). Using the eigenvalue 1 method, we identified five key demand factors: factor 1 (super-specialized infrastructure); factor 2 (access to medical information); factor 3 (cost savings); factor 4 (quality of care); and factor 5 (treatment availability within a minimal travel distance). Domestic medical tourism from northeast India can be explained by these factors.
At the item level, competence of doctors (mean = 9.15, SD = 1.327), advanced medical specialty and access to service quality (mean = 7.71, SD = 1.66), pre-treatment consultation (mean = 8.23, SD = 1.79), referred by doctors, friends, relatives, and family members (mean = 9.02, SD = 1.889), quality non clinical infrastructure (mean = 6.91, SD = 1.901), availability of medical insurance benefits (mean = 4.02, SD = 4.063), and quality of treatment received (mean = 9.40, SD = 1.114) have obtained higher EFA loadings of 0.808, 0.773, 0.737, 0.734, 0.729, 0.718, and 0.717 respectively.
Heterogeneity in medical tourism demand factors
We perform ANOVA and post hoc comparison to examine the differences, if present, in these five medical tourism demand factors with respect to tourists’ state of residence in Tables 4 and 5. P-value less than 0.005 indicates the significant impact of geographical location (state of residence) on medical tourism demand factors. It accepts H3, and states that geographical location significantly affects the demand and travel motivations for domestic medical tourism in north eastern states. Except, cost-savings, all factors or components showing significant mean differences in items based on the geographical locations or state of residence of the tourists.
A higher mean score was obtained among Mizo medical tourists (residents of Mizoram) for the availability of treatment within the shortest possible time and distance. Access to highly specialised infrastructure and the availability of reliable medical information are important motivators for medical tourists from Nagaland. The only category that significantly received a higher score among respondents from Arunachal Pradesh was cost-saving.
Discussion
Domestic medical tourism is the largest yet highly neglected segment of medical tourism research in the global south (Tham, 2018). This research aims to explore the geography of medical tourism demand in the global south. In the context of South Asia, this study on the northeastern region of India unwraps crucial chapters of domestic medical tourism demand at the micro-scale.
In the context of demographic characteristics, similarities with the global medical tourists are observed. Most of the domestic medical tourists are male and young adults. Salm and Wübker (2019) and Welke and colleagues (2019) also found that gender and age are the major determinants of regional patient migration. The medical trips from northeastern India are more regular that are driven by the need-based demand and inefficiency of the local healthcare system to address the same. The domestic medical tourists had been visiting the city repeatedly to avail the medical services they needed, which in most cases involved follow-up care and routine check-ups. Kolkata offers a diversified market of medical tourism products to its consumers varying from elective surgeries to health screening. This is true for most of the domestic medical tourism travel across the world (Croome et al., 2015; Manna et. al., 2020). Although most of these medical trips are self-financed (65.38%), however, it is also sponsored insurance (15.71%) benefits schemes. Interestingly, it is noted, that insurance benefits have been emerging as the major market driver of domestic medical tourism across the globe (Salm & Wübker, 2019).
Studying the spatial pattern of tourism demand yields more valuable results and can provide a scientific and empirical reference to local governments, tourism planners, and administrative units regarding resource allocation and infrastructure development (Ma et al., 2022). As stated earlier, the analysis of spatial patterns of domestic tourism demand has gained scholarly attention, to our knowledge no study contemplates the same in exploring the niche demand of medical tourism. This research fills these gaps and explores the spatial patterns and driving factors of domestic medical tourism demand in the South Asian region by adopting a case study of Northeast India. We note that major domestic medical tourism demand regions lie over the most populated western boundary of Tripura, south-eastern Sikkim, central Mizoram, central Manipur, and the south-eastern region of Nagaland. We observe the district-wise spatial clusters in almost all the districts of Tripura and Mizoram, the major contributor to the domestic medical tourism segment of northeast India. Districts like Aizawl, Champhai, Kolasib in Mizoram, West Tripura, Sipahijala, North Tripura, Gomati, Dhalai, and Khowai in Tripura, East Sikkim, and South Sikkim in Sikkim, Imphal East, and Imphal West in Manipur, East Khasi Hills and South West Garo Hills in Meghalaya, Dimapur and Kohima in Nagaland, Papum Pare, and Lower Dibang Valley in Arunachal Pradesh, Jorhat, Kamrup Metropolitan, and Sonitpur in Assam are observed as a major spatial cluster of medical tourism demand at district-level. Statistics from joins count suggest that Mizoram and Tripura have the largest regional concentrations of domestic medical tourism (Fig. 4). Aizawl and Champhai districts in Mizoram, as well as West Tripura and Sipahijala in Tripura, have shown high-high DMT demand clusters. Aizawl, Champhai, Mamit, Serchip, Kolasib, and Lunglei (Mizoram); Khowai, West Tripura, and Sipahijala (Tripura); Churachandpur and Cachar (Manipur); and East and North Sikkim (Sikkim) established significant medical tourism demand hotspots throughout the study period and were judged to be extremely important districts that require strategic planning to lay the foundations of sustainable domestic medical tourism for eastern India.
High population, poor maintenance of healthcare resources, and unavailability of specialists are the major reasons cited behind this medical travel (Ngaihte et al., 2019). Saikia and Das (2014) found that though with the number of healthcare facilities had improved in the northeastern states with the implementation of the National Rural Health Mission in 2005, most of the states’ healthcare system is in poor condition due to the unavailability of basic services like electricity, power supply, telecom, computer, etc.; shortage of health workers or health assistants, and acute shortages of specialists, radiographers, and nursing staffs. This set the stage for the out-of-state patient migration in search of better alternatives (Chakrabarti and Tatavarthy, 2019). In our assessment of the domestic medical travel motivations of 17 structured items we also obtained five major demand factors namely, access to super-specialized infrastructure, medical care information cost savings, quality of care, and treatment availability within minimal time and distance that can explain the domestic medical tourism from northeast India. At the item level, the competence of doctors, access to advanced medical specialty, pre-treatment consultation, physician referral, quality nonclinical infrastructure, medical insurance benefits, and quality medical care have emerged as major determinants. These factors show significant mean differences based on the respondents’ state of residence or geographical location. Availability of treatment within minimal time and distance significantly obtained a higher mean score among domestic medical tourists of Mizoram. For medical tourists coming from Nagaland, availability of highly specialised facilities and trustworthy medical information are key motivators. Among those from Arunachal Pradesh, cost-saving is the only element that notably received a higher score. The major factor influencing domestic medical tourism demand is definitely geography or place of residence, where the neighbourhood has widely embraced the dissemination of information about medical tourism practises. Major segments followed the recommendations and references of their doctors, friends, and relatives. Domestic medical tourists are notable among the chaos of regional disparities in healthcare resource allocation and need-based travel within restrictive medical travel conditions. DMTs are more delighted and enthusiastic to enjoy in destinations' growing range of diverse tourism activities.
Conclusion
Thousands of patients from northeastern states land in various metro cities of India to access care for their ailments that are not available at their homes. This study aims to examine the needs and aspirations of these migrating patients of northeast India who are visiting Kolkata, a major medical tourism hub of eastern India. By conceptualizing spatiality in mapping medical tourism demand, this study is unique in the field of medical tourism study, where we attempt to measure the degree of association among medical tourism generating regions at a micro-scale. Results indicate the strong spatial effect, and also note that domestic medical tourism demand is localized in nature that is highly controlled by the physician referral system, patient preferences and choices, and availability of financial and logistical support with flexible health insurance schemes. The results of this study are intended to aid medical tourism service providers and significant industry stakeholders in recognising market demand, making informed decisions, developing appropriate service packages, and sustaining their business in the long run.
Data availability
The data supporting the analysis of this article will be made available to readers on request.
References
Anselin, L. (1995). Local indicators of spatial association—LISA. Geographical Analysis, 27, 93–115.
Balia, S., Brau, R., & Marrocu, E. (2018). Interregional patient mobility in a decentralized healthcare system. Regional Studies, 52(3), 388–402. https://doi.org/10.1080/00343404.2017.1307954
Bhattacharya, S., & Kumar, R. V. (2017). Modeling Tourists’ Opinions Using RIDIT Analysis. In P. Vasant & M. Kalaivanthan (Eds.), Handbook of Research on Holistic Optimization Techniques in the Hospitality, Tourism, and Travel Industry (pp. 423–443). USA: IGI Global. https://doi.org/10.4018/978-1-5225-1054-3.ch020
Bishop, M. A. (2010). Comparative nearest neighbor analysis of mega-barchanoid dunes, Ar Rub al Khali sand sea: The application of geographical indices to the understanding of dune field self-organization, maturity and environmental change. Geomorphology, 120, 186–194. https://doi.org/10.1016/j.geomorph.2010.03.029
Biswas, T., & Rai, A. (2022). Medical Travel from North – East India: An assessment of domestic medical tourists’ travel profile and experience. Asian Geographer. https://doi.org/10.1080/10225706.2022.2098506
Burns, L. R. (2015). Medical tourism opportunities and challenges: Illustration from US-India trade. International Journal of Healthcare Management, 8(1), 15–26. https://doi.org/10.1179/2047971914Y.0000000091
Chakrabarti, S., & Tatavarthy, A. D. (2019). The geography of medical travel in India: Differences across states, and the urban-rural divide. Applied Geography, 107(April), 12–25. https://doi.org/10.1016/j.apgeog.2019.04.003
Chia, K. W., & Liao, Y. M. (2020). An Exploratory Study of Factors Influencing Chinese Outbound Medical Tourism. Journal of China Tourism Research, 00(00), 1–19. https://doi.org/10.1080/19388160.2020.1780177
Cohen, I. G. (2010). Protecting patients with passports: Medical tourism and the patient-protective argument. Iowa Law Review, 95(5), 1467–1567.
Collins, A., Medhekar, A., Wong, H. Y., & Cobanoglu, C. (2019). Factors influencing outbound medical travel from the USA. Tourism Review, 74(3), 463–479. https://doi.org/10.1108/TR-06-2018-0083
Croome, K. P., Lee, D. D., Burns, J. M., Perry, D. K., Keaveny, A. P., & Taner, C. B. (2015). Patterns and outcomes associated with patient migration for liver transplantation in the United States. PLoS ONE. https://doi.org/10.1371/journal.pone.0140295
Deng, M., & Athanasopoulos, G. (2011). Modelling Australian domestic and international inbound travel: A spatial–temporal approach. Tourism Management., 32, 1075–1084.
Dev, V., Sharma, V. P., & Barman, K. (2015). Mosquito-borne diseases in Assam, north-east India: Current status and key challenges. WHO South East Asia Journal of Public Health., 2(2), 20–29.
Dikshit, K. R., & Dikshit, J. K. (2014). North-East India: Land, people and economy. Springer.
Fetscherin, M., & Stephano, R.-M. (2016). The medical tourism index: Scale development and validation. Tourism Management, 52, 539–556. https://doi.org/10.1016/j.tourman.2015.08.010
Goswami, N. 2010. India's Northeast 2020: Four Alternative Futures. IDSA Occasional Paper No. 13, New Delhi: Institute for Defence Studies and Analyses.
Han, J. S., Lee, T. J., & Ryu, K. (2018). The promotion of health tourism products for domestic tourists. International Journal of Tourism Research, 20(2), 137–146.
Hudson, S., & Li, X. R. (2012). Domestic medical tourism : a neglected dimension of medical tourism research domestic medical tourism. Journal of Hospitality Marketing and Management, 21(3), 227–246. https://doi.org/10.1080/19368623.2011.615018
Jaapar, M., Musa, G., Moghavvemi, S., & Saub, R. (2017). Dental tourism: Examining tourist profiles, motivation and satisfaction. Tourism Management, 58, 538–552. https://doi.org/10.1016/j.tourman.2017.02.023
John, S. P., & Larke, R. (2016). An analysis of push and pull motivators investigated in medical tourism research published from 2000 to 2016. Tourism Review International, 20(2–3), 73–90. https://doi.org/10.3727/154427216X14713104855810
Keckley, P H, & Underwood. H.R. 2008. Medical Tourism: Consumers in Search of Value. Survey of Health Care Consumers, Washington: Deloitte Centre for Health Solutions
Khan, J. M., Chelliah, S., Haron, M., & Ahmed, S. (2017). Push factors, risks, and types of visit intentions of international medical travellers – A conceptual model. International Journal of Healthcare Management, 10(2), 115–121. https://doi.org/10.1080/20479700.2017.1304345
KMC (2016) Kolkata Municipal Corporation. [Online] Available at: https://www.kmcgov.in/KMCPortal/jsp/BasicStatistics.jsp. Accessed 8 Oct 2022
Kumar, R. (2019). Public–Private partnerships for universal health coverage? the future of “free health” in Sri Lanka. Globalization and Health, 15, 75. https://doi.org/10.1186/s12992-019-0522-6
Kwong, A. J., Mannalithara, A., Heimbach, J., Prentice, M. A., & Kim, W. R. (2019). Migration of patients for liver transplantation and waitlist outcomes. Clinical Gastroenterology and Hepatology, 17(11), 2347–2355.
Lunt, N., Horsfall, D., & Hanefeld, J. (2016). Medical tourism: A snapshot of evidence on treatment abroad. Maturitas, 88, 37–44. https://doi.org/10.1016/j.maturitas.2016.03.001
Ma, X., Yang, Z., & Zheng, J. (2022). Analysis of Spatial patterns and driving factors of provincial tourism demand in China. Scientific Reports, 12(1), 1–15. https://doi.org/10.1038/s41598-022-04895-8
Manna, R., Cavallone, M., Ciasullo, M. V., & Palumbo, R. (2020). Beyond the rhetoric of health tourism: Shedding light on the reality of health tourism in Italy. Current Issues in Tourism, 23(14), 1805–1819. https://doi.org/10.1080/13683500.2019.1650726
Massidda, C., & Etzo, I. (2012). The determinants of Italian domestic tourism: A panel data analysis. Tourism Management, 33, 603–610.
Mazzulla, G., & Forciniti, C. (2012). Spatial association techniques for analysing trip distribution in an urban area. European Transport Research Review, 4, 217–233.
Medhekar, A., & Wong, H. Y. (2020). Medical travellers’ perspective on factors affecting medical tourism to India. Asia Pacific Journal of Tourism Research, 25(12), 1295–1310. https://doi.org/10.1080/10941665.2020.1837893
Mishra, S. S., & Bansal, V. (2017). Role of source-destination proximity in international inbound tourist arrival: Empirical evidences from India. Asia Pacific Journal of Tourism Research, 22(5), 540–553. https://doi.org/10.1080/10941665.2017.1287107
Mitchell, A. (2005). The ESRI Guide to GIS Analysis (Vol. 2). ESRI Press.
Moran, P. A. P. (1950). Notes on Continuous stochastic phenomena. Biometrika, 371, 17–23.
NCDIR (National Centre for Disease Informatics and Research). 2017. A Report on Cancer Burden in North Eastern States of India. Panel Report, Bengaluru: Indian Council of Medical Research
NECS (North Eastern Council Secretariat). 2016. Basic Statistics of North Eastern Region 2015. Annual Report, North Eastern Council Secretariat, Shillong: Directorate of Printing and Stationary, Government of Meghalaya
Ngaihte, P., Zomawia, E., & Kaushik, I. (2019). Cancer in the NorthEast India: Where we are and what needs to be done? Indian Journal of Public Health, 63(3), 251–253. https://doi.org/10.4103/ijph.IJPH_323_18
Nwachukwu, B. U., Dy, C. J., Burket, J. C., Padgett, D. E., & Lyman, S. (2015). Risk for complication after total joint arthroplasty at a center of excellence: The impact of patient travel distance. Journal of Arthroplasty, 30(6), 1058–1061.
Ord, K., & Getis, A. (2001). Testing for local spatial autocorrelation in the presence of global spatial autocorrelation. Journal of Regional Science, 41, 411–432.
Ormond, M., & Sulianti, D. (2017). More than medical tourism: Lessons from Indonesia and Malaysia on South-South intra-regional medical travel. Current Issues in Tourism, 20(1), 94–110.
Rai, A. (2019). Medical tourism in Kolkata, Eastern India. Springer Nature Publishing.
Rai, A., Chakrabarty, P., & Sarkar, A. (2016). A quantitative appraisal of the level of satisfaction of the medical tourists in Kolkata, West Bengal. Indian Journal of Spatial Science, 7(2), 8–17.
Ramashankar, S. D., & Sharma, B. K. (2015). Traditional healing practices in North East India. Indian Journal of History of Science, 50(2), 324–332.
Rouland, B., & Jarraya, M. (2020). From medical tourism to regionalism from the bottom up: Emerging transnational spaces of care between Libya and Tunisia. Journal of Ethnic and Migration Studies, 46(20), 4248–4263. https://doi.org/10.1080/1369183X.2019.1597475
Routh, D., Rai, A., & Bhunia, G. S. (2022). Post-lockdown spatiotemporal pattern of COVID clustering in North 24 Parganas, West Bengal. India. Spat. Inf. Res. https://doi.org/10.1007/s41324-022-00483-0
Saikia, D., & Das, K. K. (2014). Status of rural health infrastructure in the North-East India. Management În Sănătate XVIII, 2, 34–38.
Salm, M., & Wübker, A. (2019). Sources of regional variation in healthcare utilization in Germany. Journal of Health Economics. https://doi.org/10.1016/j.jhealeco.2019.102271
Sengupta, A., Zaidi, S., Sundararaman, T., Onta, S., & Weerasinghe, M. C. (2018). Tackling the Primary Care Access Challenge in South Asia. BMJ, 363, k4878. https://doi.org/10.1136/bmj.k4878
Taherdoost, H. (2019). What Is the best response scale for survey and questionnaire design: Review of different lengths of rating scale/attitude scale/likert scale. International Journal of Academic Research in Management (IJARM), 8(1), 1–10.
Tham, A. (2018). Sand, surgery and stakeholders: A multi-stakeholder involvement model of domestic medical tourism for Australia’s Sunshine Coast. Tourism Management Perspectives. https://doi.org/10.1016/j.tmp.2017.11.002
Turner, L. (2012). Beyond “medical tourism”: Canadian companies marketing medical travel. Globalization and Health, 8, 16. https://doi.org/10.1186/1744-8603-8-16
UNICEF. 2021. Accelerating Progress Towards Universal Health Coverage in South Asia in the Era of COVID-19, UNICEF, September 2021, accessed on Jun 15, 2022 at https://www.unicef.org
Welke, K. F., Pasquali, S. K., Lin, P., Backer, C. L., Overman, D. M., Romano, J. C., & Jacobs, J. P. (2019). Hospital distribution and patient travel patterns for congenital cardiac surgery in the United States. The Annals of Thoracic Surgery, 107(2), 574–581. https://doi.org/10.1016/j.athoracsur.2018.07.047
Yang, Y., & Zhang, H. (2019). Spatial-temporal forecasting of tourism demand. Annals of Tourism Research, 75, 106–119.
Acknowledgement
We would like to express our gratitude to the Department of Geography, School of Basic and Applied Sciences, Adamas University for providing necessary resources to carry out this research.
Funding
No external funding sources.
Author information
Authors and Affiliations
Contributions
AR and TB initiated, designed and coordinated the study. TB conducted data collection, AR has analyzed the data, AR and TB wrote the draft manuscript. AR checked the results and critically revised, modified and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Biswas, T., Rai, A. Analysis of spatial patterns and driving factors of domestic medical tourism demand in North East India. GeoJournal 88, 3163–3181 (2023). https://doi.org/10.1007/s10708-022-10798-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10708-022-10798-y