
Abstract
Particulate matter air pollution is estimated to cause in the order of 350,000 excess deaths in the European Union calling for policy development and evaluation tools. In the current work, a model for PM10 exposures of children is developed using microenvironment time activities and infiltration of ambient pollution indoors, both evaluated against observations earlier and integrated with city-wide air quality models in the current work. The model is demonstrated using data from two cities in Italy. High-end short-term exposures are characterized by an episode-day situation in Turin, and annual mean exposures in downtown Bologna. The air quality model was unable to capture the highest levels during the episode, and therefore, the exposure model was adjusted using observed–modeled ratio from a monitoring station. Air quality model performance for the annual levels was significantly better. Annual exposure variability within the target population was 1.5-fold in the downtown area Bologna and tenfold during the episode day in Turin.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Ambient urban air pollution causes significant excess mortality and morbidity at the levels currently observed in American and European urban areas (e.g. [30, 31]). In the European Union, particulate matter exposure is estimated to cause annually 348,000 additional deaths (central estimate in [10]). Air pollution is a risk factor that increases the probability of death and other adverse health effects caused primarily by cardiovascular and respiratory diseases, including development of asthma in children [11]. Moreover, population exposures in many European cities have been shown to exceed many existing air quality guideline levels, including those set for particulate matter, highlighting the need to develop efficient policies to decrease the exposures [12].
The increased risks have been observed in population level epidemiological studies using ambient concentrations as measures for population exposures. The health effects caused by air pollution, however, are caused by the actual exposures of the affected population members. Exposure studies have shown that ambient levels at monitoring stations, currently used in air quality management, correlate poorly with actual personal exposures (i.e., concentrations measured with portable monitors that the subjects carry with them for a given study period; e.g., [20–22, 28]). This is caused by (1) the mobility of the population members in the variable concentration fields, (2) filtration of pollutants by the building envelopes, and (3) indoor sources of air pollution.
Further advantage of modeling is that air quality monitoring is subject to the limitations set by the small numbers of monitoring stations and the substantial variability of concentrations in urban environments [38]. Models also benefit from the recent advances in urban micrometeorological modeling [2]. The current work combines these advancements with population exposure modeling, including simple methods to account for population mobility and time spent in traffic and indoors, and uses population data from Turin and Bologna, Italy, to demonstrate the modeling system.
The two cities of this study are located in the river Po Valley in Northern Italy. Turin is one of the largest industrialized centers in Northern Italy, with a population of about 900,000 people and influenced by intense road and railway traffic. The city is located at the western edge of the Po Valley, and it lays mainly on flat topography, being surrounded by the Western Alps that rise to heights of 1,500 m, only 20 km from downtown, and with a range of hills reaching 700 m just east of Turin. Local circulation is influenced both by mesoscale (e.g., valley stagnation, mountain/valley breezes, and foehn) and urban-originated flows. As a result, despite its position at the mountain feet, the city of Turin is frequently affected by very low winds during both winter and summer, which, added to the anthropogenic emissions, give rise to severe air pollution episodes, often exceeding EU air quality standards.
Bologna is situated 300 km east-south-east from Turin in the Po Valley plateau, 50 km south of the river. The PoValley plateau is a heavily industrialized and densely populated area, where air stagnation often occurs. Annual average wind speed in Bologna is low, leading both to short-term air pollution episodes as well as frequent exceedances of both short-term and annual European air quality standards.
Public health protection is one of the main motivation for air quality monitoring and management. Therefore, air quality management needs to consider options to reduce population exposures, in particular, those of sensitive population groups. Children were selected as a target group because one of the regional priority goals of the Children’s Environment and Health Action Plan for Europe [6] is to reduce acute and chronic respiratory disorders, including asthmatic attacks in children and adolescents due to outdoor pollution. The listed means to achieve this goal vary from improvements in engine technology to pollution-free school zones and alert systems [6].
Population exposure models are needed for policy development and evaluation (e.g., [16, 34]). The objective of the current work is to present a microenvironment and time–activity-based approach for exposure model to provide quantitative health-based tools for air quality-related policy refinement and evaluation.
2 Atmospheric and Exposure Modeling Methods
Exposure models for children were developed for two Italian cities and for two different settings (Table 1) to investigate the properties of the exposure distributions and their relationships to ambient air monitoring data. The air quality and exposure models were run for NO2 and PM10. In the paper, the results for PM10 are used to demonstrate the modeling system and discuss consequences for development of policy options targeting at reduction of adverse health effects of air pollution. The modeling methods and input data are summarized below. More detailed presentation and data can be found in the technical reports available from the FUMAPEX web siteFootnote 1.
The microenvironment-based exposure model used estimate exposures (E) as the time-weighted average concentration (C) over the microenvironments visited (indexed by i) [9, 13, 23, 25, 32]. According to Eq. 1, time-weighting is done using personal time activities as fractions of time (f i) spent in each microenvironment, implicitly defining the averaging time (t; f i = t i/t):
For the purposes of the current work, four microenvironments were defined: (1) residential indoors, (2) school indoors, (3) in traffic, and (4) residential outdoors. In Turin, where the target group included both school children and children below school age, no separation was done between residence and school indoor environments. Other indoor environments, like shops or visits to a friend’s home, were not modeled.
Time spent in each microenvironment was estimated by using information derived from school administration, from a survey on a children sample in Ferrara, Italy, [18, 19], a town next to Bologna, and using typical daily timetables of school children in Italy. Details of the time–activity models are explained further on in the city-specific sections (summary in Table 2).
Building envelopes and filtration units in ventilation systems (when applicable) remove some of the outdoor pollution. Indoor concentrations have been modeled using either a mass-balance model [4, 26, 27] or infiltration model [14, 15]. Both approaches are based on the same overall mass-balance equation and have been successfully used in estimation of indoor concentrations. Residential indoor concentrations in four European cities were apportioned to fractions of PM2.5 of ambient and indoor origin [14]. Mean infiltration efficiency of PM2.5 particles ranged from 0.59 in Helsinki to 0.70 in Athens, with Basle and Prague in between. Values from the Mediterranean climate of Athens were used in the current work for PM10 (Table 2).
The indoor microenvironment concentrations (C i) were modeled from the ambient concentration according to Eq. 2:
where F inf is the infiltration factor and C a the outdoor PM10 concentration used to estimate the indoor concentration of ambient origin (F inf × C a). The additional concentrations (C Sj) caused by various sources (indexed by j) within the microenvironment were not considered in the current work. Infiltration factors analyzed for PM2.5 in four European cities [14] were used as proxies for PM10, as no European PM10 specific data was available. This estimate is conservative in terms of overestimating exposures to ambient PM10, as the coarse fraction of PM10 has a lower infiltration fraction than fine (PM2.5) fraction.
Air quality models typically under-predict the short-term variability of actual concentrations, and for many pollutants, these levels may be significantly higher than those observed in stationary microenvironments. Therefore, the concentrations experienced while in traffic were estimated using the fixed site monitoring station concentrations multiplied by coefficients (Table 2) observed in a number of studies reviewed by the World Health Organization (WHO) [36]. Similar relationships were observed in the Expolis study in Helsinki in 1996–1997, where PM2.5 concentrations were measured in 37 vehicles [15]. The average concentration experienced while in traffic was estimated to be 17.2 ± 13.9 μg m−3. In comparison to the average ambient PM2.5 concentration of approximately 10 μg m−3, this level is 1.7-fold, comparing well with the WHO report estimates.
When using an air quality model as source of concentrations, the model errors need to be estimated to get “best estimates of the true exposures.” Policy development must be based on best understanding of the true exposures, and if the models have known deficiencies, these must be accounted for. In Bologna, the PM10 level at the fixed monitoring site, San Felice, is slightly underestimated by the air quality model (33 vs 40 μg m−3, ratio 0.83). The modeled ambient concentrations used as inputs in the exposure model were adjusted using this ratio as the scaling factor. In Turin, the difference between modeled and monitored air quality at Consolata monitoring station was larger (46 vs 111 μg m−3, ratio 0.414), mainly due to the extreme episode conditions that are difficult to capture by models but also related to the coarser spatial resolution (1 km vs 50 m) of the air quality model.
2.1 Model Specifics in Bologna
Children living in and going to two primary schools within a 2 × 2 km area next to the downtown Bologna were selected as the target population. Residential coordinates of the 333 children and the two schools were used to obtain annual mean outdoor air concentrations from the high-resolution air quality model outputs (conducted by ARPA Hydro-Meteorological Service) for the period 1 June 2004–31 May 2005.
A multiscale urban air quality information and forecasting system for Bologna and the Emilia Romagna region has been designed and implemented by ARPA. It consists of the Northern Italy Network to Forecast Aerosol (NINFA) pollution, based on the regional version of the Chimere chemical transport model [3], driven by the meteorological model LAMI, the Italian implementation of the non-hydrostatic-limited area model Lokal Modell [33]. Horizontal resolutions of NINFA and LAMI are 50 and 7 km, respectively. NINFA is run daily and provides concentration forecasts for PM10, ozone, and NO2 for the following 72 h over the Northern part of Italy (regional scale) The domain covers the Turin area, but the two modeling chain are independent. During FUMAPEX, short-term simulations were done by ARPA for the Turin domain to compare the performances of the two modeling chains. Boundary conditions for the meteorological model are provided by the Prev’air model [17]; emission inventories are provided by the national inventory Corinair.
An urban AQ management and planning tool, based on the Atmospheric Dispersion Modelling System-Urban AQ model [7], is used to downscale the NINFA background concentrations to “roadside” level. Detailed urban pollution data from ADMS-Urban provide the outdoor concentration data for population exposure assessment. The simulation domain covers a district (2 × 2 km) of the Bologna urban area. Output surface fields are calculated with a 50-m horizontal resolution. ADMS-Urban does not include resuspension particles. The model does not take into account also chemical reactions that produce/transform particles. Long-range transport and secondary particulate are taken into account with the insertion of a background concentration time series (equal in all simulation domains—that is very small in Bologna’s simulations). Secondary and long-range transported particles account for more than 50% of the total PM10 concentrations.
Outdoor air concentrations corresponding to the times spent in each stationary microenvironment were calculated using the hourly monitoring station data and scaling factor estimated from the annual mean values for each location (Fig. 1).

Home, schools, and monitoring station locations and annual mean PM10 concentrations in Bologna. Size of the model area is 2 × 2 km
Time spent in traffic was calculated using the home–school distance for each child and an estimated commuting speed of 20 km h−1. Times spent in school were based on typical Italian primary school timetable (Fig. 2). Exposure of each child (E i) is then calculated for each day over the year according to Eq. 3, where f is the fraction of time spent in residences (R), outdoors (O), in school (S), and traffic (T), and corresponding concentrations (C M denotes concentration at the monitoring station):

Daily timetable of the children during different types of days experienced during the school year in Bologna
2.2 Model Specifics in Turin
The exposure model in Turin included the whole metropolitan area (120 km2) with 101,563 children aged 14 or less and targeted exposures occurring during an extreme episode condition on 13–14 January 2003. The episode lasted 4 days, but only Tuesday, the worst day, is included in the results presented in this paper.
Spatial distribution of ambient air quality was estimated using the urban air quality information and forecasting system applied in Turin, developed in the framework of the FUMAPEX project at ARPA Piemonte in collaboration with Arianet Consulting. The system was built to provide hourly forecasts on pollutants defined in the current Italian legislation (PM10, NO2, O3, CO, SO2, and benzene) on a regional and local scale with different spatial resolution. The system’s main constituents are the prognostic non-hydrostatic meteorological model RAMS [8, 29], which downscales the European Centre for Medium-Range Weather Forecasts weather forecasts, and the three-dimensional Eulerian model FARM [5] that accounts for the transport, chemical conversion, and deposition of atmospheric pollutants.
Emissions were estimated using results from the European EMEP inventory, the national Italian inventory Corinair, and the high-resolution inventory for Piemonte region, and integrated to set up the database needed to perform the chemical and dispersion simulations. Boundary conditions for the air quality model have been obtained by EMEP simulation fields, while initial concentration fields have been built by objective analysis of EMEP background fields and local observations over the Piemonte region. The modeling system applies to three nested domains, covering, respectively, Northern Italy, the Piemonte region and the Turin metropolitan area, with increasing horizontal resolution of 16, 4, and 1 km. Resuspension was estimated as a source category in the emission inventory. Long-range transport and secondary particulate matter are taken into account with initial and boundary conditions.
The modeling system was tested on a critical episode, both for meteorological and air quality conditions, with fair weather conditions and ground-based inversion—which is not unusual during winter time in the area—causing exceedances in PM10 and NO2 concentrations recorded at air quality monitoring stations. Target population in Turin urban area was originally referred to 21 districts and divided by gender and age; in the absence of information about time activities, the exposure model was applied to children less than 14 years as considered to be less mobile in their daily activities than elder people. Therefore, the outdoor air quality in their residential areas results to be more relevant for their exposures. Children of age 0–14 years were assumed to be evenly distributed between the ages when combining time activities of school children and children below school age (0–6 years).
Concentrations were calculated for 1-km2 grid, and exposures of children living in each grid cell were estimated using the grid concentration data, time activity, infiltration, and traffic concentration factors. All time spent outside home was assumed to occur during daytime (7–22). Effectively, the average exposure value for each grid cell (E) is calculated according to Eq. 4, where f is the fraction of time during the daytime hours (7–22) spent in indoors (f i), outdoors (f o), and in traffic (f t), and C is the concentration for daytime (C d) and night time (C n):
3 Results
Exceedances of EU limit values and WHO guidelines occur regularly at fixed monitoring sites in both Turin and Bologna (Table 3). Exceedances are substantially more common for PM10 than for NO2, indicating PM10 as the main concern for public health, air quality management, and policy development and, therefore, in the focus for the exposure models.
At the residential locations of the school children, the annual PM10 levels estimated by the air quality model in Bologna vary from 20 to 30 μg m−3 (Fig. 1). Highest levels occur in the vicinity of busy roads. Small variability of the annual average levels is reduced by the compact size of the target area; all the buildings are situated on a continuously built downtown area with similar building heights and surrounded by busy traffic including major routes for public buses. The annual average PM10 concentration observed during the model year at the San Felice monitoring station was 41 μg m−3, indicating the influence of the busy traffic at the crossroads where the monitoring station is located.
The average PM10 exposures (16.6 and 104 μg m−3) were 42% and 93% of the levels observed at the fixed monitoring sites in Bologna (annual) and Turin (episode day), respectively (Table 4). The lower percentage in Bologna reflects the traffic-oriented location of the monitoring site. In Turin, the Consolata monitoring site is located in the center of the city but approximately 250 m from a major road and reflects much better the overall exposures of children and probably also other population groups that do not spend substantial time in traffic. In relationship to the corresponding WHO PM10 guidelines [37], the exposures were 83% of the annual and 208% of the daily guidelines, respectively, while the ambient levels at the monitoring sites reached (Bologna) or exceeded (Turin, by 223%) the EU PM10 limit values (Table 4).
Comparison of mean exposures of children with limit values set for ambient air is not fully able to capture exposures that may have significant health consequences. Cumulative distributions of modeled exposures for both cities start from levels slightly above 10 μg m−3 (Fig. 3), but the variability of exposure levels during the Turin episode day is huge in comparison to the modest variability of annual exposures in Bologna. In Turin, approximately 90% of the children living in the metropolitan area were exposed to levels above the WHO 24-h PM10 guideline and corresponding EU PM10 limit value defined for the ambient air. In both cities, the exposure levels of children were lower than the levels observed at the fixed monitoring site (San Felice site in Bologna just reached the EU limit value of 40 μg m−3, while 24-h average at the Consolata site in Turin exceeded 110 μg m−3 for the episode peak day). The observed high variability in Turin indicates that the episode is largely of local origin that could be affected by local air quality management; long-range transported levels would show much less variability over the urban area.

Modeled PM10 exposure distributions and corresponding reference values used to evaluate ambient air quality. In the case of the episode, a substantial fraction of personal exposures exceed the guidelines
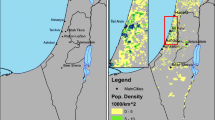
The comparison between geographical distributions of exposures modeled in Turin and the emission inventory data indicate that the higher modeled PM10 concentration levels occur in industrial and traffic areas, as confirmed in the highest levels observed in the Northern border of the area (Fig. 4). Nevertheless, the highest exposure levels occur in the south-western downtown area as a result of both the high population density in combination with the presence of industrial sources and traffic in the vicinity. Emissions from such sources are promising targets for exposure reduction.

Spatial distributions of 24-h PM10 exposures during the episode day (13 January 2003, 2200 hours, to 14 January 2003, 2159 hours): exposure concentration (top) and cumulative population exposure (bottom)
While longer averaging times typically improve air quality model performance as seen in the comparison of model results at the monitoring sites (Table 4), the PM10 levels were slightly underestimated in comparison to the monitoring data in Bologna. In the case of the episode, the relative difference was substantially larger. Therefore, also exposures calculated from uncorrected dispersion model concentrations can be expected to underestimate true exposures and to give best estimates for the true exposures; a model calibration procedure was applied to the exposure model results using the observed/modeled concentration ratio (Table 4, Figs. 3 and 5). In Bologna, the exposures were highest in the winter season (Fig. 5), partly due to the higher ambient levels, but also because of the larger fraction of time that is spent in traffic environments during the school year in comparison to the summer season and weekend days during the winter (Fig. 2).

Average PM10 personal exposures by season in comparison to annual average concentration at the San Felice monitoring station in Bologna
4 Discussion
Exposure reduction policy options may alter either the local emissions or population activity. Examples of the former include traffic limitations (implemented via environmental zones, parking fees, tolls, vehicle category based traffic bans, etc.), road network maintenance (removal and/or binding of road dust, street washing, street surface material optimization for durability), actions targeting small-scale combustion sources (like domestic cooking and heating), and restriction of emissions from industries of various size. The latter population activity means are mainly available via information and may concern avoiding time spent in traffic or outdoors, keeping windows closed and minimizing ventilation during air pollution episodes.
The current results on the exposures of school children are in line with the general understanding that exposures of various population groups are different from ambient air quality. Air quality monitoring, modeling, management, and corresponding legislation have traditionally been based on ambient concentrations. Ambient concentrations are variable, and the actual effects on health are modified by the behavior of population members, affected by locations of homes, workplaces, and public services, and the transportation systems available for the citizens. Optimal use of the resources invested in the air quality management for public health protection requires consideration of these aspects and therefore modeling of exposures.
Depending on the model type, exposure models can be utilized in different ways, including at least (1) quantification (estimation) of health effects in a given population, (2) comparison of control options and environmental policies, and (3) utilization of exposure models in urban planning. Each of these is discussed below.
The current work estimated short-term spatial (Turin) and annual interpersonal (Bologna) distributions of exposures among school children. Health risks caused by the exposure peak when a high exposure is combined with a high individual sensitivity. Thus, there is specific interest in looking at (1) higher exposure levels and (2) sensitive population groups separately. Quantification of health effects caused by air pollution gives a reference point for reasonable investments in public health protection. Most reliable dose–response or exposure–response relationships of air pollutants are based on epidemiological studies that compare health outcomes in different populations as function of proxies for their average exposures. Differences in the personal sensitivities are high, and only a small number of individuals are actually harmed. Therefore, the exposure parameters required for health impact assessment are the mean exposure levels for defined population groups.
In extreme cases, the health effects of a given individual can be associated with very short-term peak exposure levels, lasting only minutes or hours (e.g., for carbon monoxide). The majority of health effects, however, are associated with longer-term exposures. For PM2.5, statistical associations have been shown for daily (i.e., 24-h) exposures, but the corresponding risk ratio for annual exposures is estimated to be up to ten times higher, indicating that, to look for health relevance, long-term exposures should be estimated.
Evaluation of control options from the health perspective may include decisions to regulate traffic. Using the dispersion and exposure models, it is possible to estimate which fraction of the total exposures could be reduced by setting restrictions for, e.g., private car traffic or local industrial activities. The comparison of the alternative, locally relevant options and estimation of the health risk reductions for each option allows the decision-makers to protect the public health in the most efficient way.
Moreover, exposure can be utilized in long-term urban planning. Population exposures can be estimated for, e.g., alternative traffic system scenarios, as is done in Helsinki as part of the metropolitan area transportation system planning (HEAT, [35]). The modeling tools can be used to estimate exposure fractions from various sources, including the long-range transported pollution, and thus, the models can be utilized also in setting priorities for local, regional, and international emission reduction activities.
Main focus of the current work was in the analysis of the use of exposure models in environmental policy development and air quality management. Nevertheless, the current results allow also for assessment of some development areas in exposure modeling as discussed below.
Population time activity is rather similar across adult urban populations in Europe (e.g., [16]). More differences are found between urban and rural populations and populations of different ages. Time spent in traffic and in high-concentration public areas remain poorly estimated in the current approach. More observed and modeled data on levels in these microenvironments is needed and will improve reliability of the exposure model. Especially the concentrations experienced in these environments remain uncertain and should be looked at more carefully in future work.
Buildings, ventilation systems and practices, and climates are different in different parts of Europe, affecting the indoor–outdoor relationships of pollutants [14]. Concentrations experienced in traffic environments are potentially extremely variable and difficult to model. These variables require more research, and care must be taken in evaluating the usability of international data to local situations. Non-residential infiltrations will be a very interesting and relevant study subject. Significant microenvironments include schools (school children), different workplaces (working age population), hospitals (patients), and public services (active population groups).
Evaluation of models against observations is important to ensure reliability of the model and identification of the model deficiencies and limitations. The current time activity-/microenvironment-/infiltration-based exposure model was evaluated against personal exposure measurements for PM2.5 exposures of working age subjects in Helsinki [15]. Children, however, are a more difficult target group for conducted intrusive exposure measurements. Only the mere size and weight of the sampling equipment is preventive for the smallest children. A different type of difficulties concern measurement of episode exposures (c.f., the Turin model); typically in exposure monitoring studies, a relatively small number of equipment are used to measure few subjects at a time over a longer period. Such an approach is not possible for episodes, and even if the number of equipment available were sufficient, the unpredictability of episodes presents serious obstacles. Therefore, in the current work, an exposure model validated elsewhere against personal exposure measurements was used together with modeled and corrected ambient air quality data to estimate exposures of a challenging target group.
For many reasons, air quality models are not always capable of capturing the true concentrations. Examples of difficult modeling situations include episode situations in general and modeling of near-fields of emission sources, including traffic. Time spent in traffic is less than 10% on the average, but certain population groups spend significantly more time there, and their exposures are affected by the traffic PM concentrations that may be an order of magnitude higher than the urban background levels.
It has been suggested that particles with different chemical composition and physical properties (like size) may exhibit different toxicities [24]. Air quality models are potentially very valuable tools in estimating exposures for epidemiological studies as by definition; deterministic models can output exposures to particles from different source categories separately.
The current work used PM10 levels as an indicator for particulate matter pollution. Epidemiology has shown, however, that particles smaller than that, fine particles (PM2.5), are even more harmful to human health [31]. Tailpipe particulate matter emissions from motor vehicles consist almost entirely of fine particles, while the fraction of larger particles in PM10 originates from road wear and resuspension. The emissions of coarse particles depend substantially, e.g., from the wetness of the road surface and wind velocity and cannot be fully captured by the air quality models. When air quality models are run using emission estimates for tailpipe emissions only, the results calculated for PM10 represent mostly fine particles, and when evaluating the harmfulness of the levels, this fact needs to be considered. A study on chemical composition of PM10 and on dimensional analysis (ten stages: <0.5, 0.5–1, 1–1.5, 1.5–3, 3–7, and 7–10 μm) has been conducted in Bologna during 2004 [1]. The study showed that the PM2.5 fraction accounts for about 75% of the PM10 total mass and the PM1 fraction for about 65%. This indicates that, even though PM2.5 monitoring data is not available, such data would yield even more stringent results in the comparison with guideline values, as e.g., the WHO guidelines [37] assume a default value of 0.5 (i.e., 50%) for the PM2.5/PM10 ratio.
The complexity and data requirements of the two presented cases are different. The Bologna model included individual locations of the residences and schools of all the target subjects, and uses hourly time activity over the modeling year. The Turin model combines all children living in a square-kilometer grid cell together, using same outdoor concentration for all their time activity. Both models account separately for times spent in indoors, outdoors, and in traffic. The Turin approach does not allow for more detailed analysis of, e.g., demographic factors associated with exposure distributions, but on the other hand, it allows for presentations of spatial variability of exposures over the whole metropolitan area. The limited mobility of children makes this approach more plausible for this target population group than for working-age subjects. However, more work need to be carried out to refine the modeling exposure application to take into account real time activity, more detailed demographic information and improved air quality modeling (e.g., higher spatial resolution and enhanced description of traffic modulation).
5 Conclusions
A model was developed to estimate exposures of children in long-term and peak exposure scenarios to study the implications for health-based environmental policy refinement. The demonstration results were in-line with numerous studies earlier, showing that exposures are clearly different from fixed site or outdoor levels, and this relationship varies between different types of monitoring sites. Annual exposure level in Bologna was less than half of the contemporary concentration of traffic-oriented San Felice fixed monitoring site. In Turin, the monitoring station Consolata, located in the downtown but not close to the major traffic arteries, represented the average exposures of the children quite well, but the variability of exposure levels span almost over an order of magnitude.
Urban air quality information systems have been originally developed to assess compliance to air quality standards but can be utilized significantly more efficiently to promote public health in combination with exposure models. Networking of end users (metropolitan area and regional authorities), scientists (atmospheric chemists, physicists, meteorologists, modelers, environmental scientists, epidemiologists, etc.), and policy makers is needed for development and application of exposure modeling techniques to support health-based air quality management.
In both cases studied, the air quality models were able to capture the variability of levels only partly; this was especially highlighted in the case of the peak episode but was evident in the annual results, too. Therefore, it is important to evaluate models against observations and to consider a model calibration procedure, when the necessary data is available.
Majority of the children were exposed to levels of health concerns in the case of an episode. Air quality management in episode situation requires reliable forecasting to allow for the actions, like traffic restrictions, industrial shutdowns, etc., to be prepared and implemented. However, based on the epidemiological data, health effects of long-term exposures outnumber those of high but short-term peak exposures. Therefore, additional focus in environmental policy development must be in reduction of long-term exposures. In practice, this means optimization of air quality management decisions according to the quantitative estimates of exposures in alternative policy scenarios. Compliance to air quality standards is a weak optimizing target for air quality management, and it does not guarantee optimal environmental safety. This is emphasized by the facts that almost all recent epidemiology points to linear zero threshold exposure–response relationship. A long-term goal must be set to develop air quality legislation instruments toward better support to health-based decision-making.
The key uncertainties remaining in the integrated model outputs are related to the spatio-temporal variability of pollutant levels that is not fully captured by the air quality models due to uncertainties in emission estimates and critical meteorological conditions. Especially highest exposures experienced while in traffic may significantly affect the highest percentiles of children spending substantial periods of time in or close to traffic environments. Measurements of indoor and outdoor levels for estimation of infiltration factors in the local building stock are needed for refinement of model parameters and personal exposures for model evaluation.
Notes
http://fumapex.dmi.dk (accessed December 2007) section “Reports.” Deliverables D7.3 and D7.4 present the exposure modeling details, and D8.2 summarizes the air-quality modeling systems based on technical reports D1–D6 from previous work packages.
References
ARPA Emilia-Romagna and University of Bologna (2005). Caratterizzazione chimico-fisica del particolato atmosferico nelle classi dimensionali tra 10 e 0.4 μm [Chemical and physical characterization of atmospheric particulate in the dimensional classes between 10 and 0.4 μm, Internal Report in Italian]. Retrieved 14 June 2007 from http://www.arpa.emr.it/reggioemilia/download/PolveRe.pdf (in Italian).
Baklanov, A., Hänninen, O., Slørdal, L. H., Kukkonen, J., Bjergene, N., Fay, B., et al. (2005). Integrated systems for forecasting urban meteorology, air pollution and population exposure. Atmospheric Chemistry and Physics Discussions, 6, 1867–1913.
Bessagnet, B., Hodzic, A., Vautard, R., Beekmann, M., Cheinet, S., Honoré, C., et al. (2004). Aerosol modelling with Chimere: preliminary evaluation at the continental scale. Atmospheric Environment, 38, 2803–2817.
Burke, J. M., Zufall, M. J., & Özkaynak, H. (2001). A population exposure model for particulate matter: Case study results for PM2.5 in Philadelphia, PA. Journal of Exposure Analysis and Environmental Epidemiology, 11(6), 470–489.
Calori, G., & Silibello, C. (2005). FARM (Flexible Air quality Regional Model)—Model formulation and user manual, version 2.4. Arianet R2005.07. European Topic Centre on Air and Climate Change–Topic Centre of European Environment Agency. Retrieved 14 June 2007 from http://pandora.meng.auth.gr/mds/showlong.php?id=130.
CEHAPE (2004). Children’s Environment and Health Action Plan for Europe, EUR/04/5046267/7. Fourth Ministerial Conference on Environment and Health Budapest, Hungary, 23–25 June 2004. Retrieved 14 June 2007 from http://www.euro.who.int/document/e83338.pdf.
CERC (2003). ADMS-Urban user guide (version 2.0). Cambridge. European Topic Centre on Air and Climate Change–Topic Centre of European Environment Agency. Retrieved 14 June 2007 from http://pandora.meng.auth.gr/mds/showlong.php?id=18&MTG_Session=2b494cdf39facee0690d21cf7baf24cf.
Cotton, W. R., Pielke, R. A., Walko, R. L., Liston, G. E., Tremback, C. J., Jiang, H., et al. (2003). RAMS 2001: Current status and future directions. Meteorology and Atmospheric Physics, 82, 5–29.
Duan, N. (1982). Models for human exposure to air pollution. Environment International, 8, 305–309.
EC (2005). Proposal for a directive of the European parliament and of the council on ambient air quality and cleaner air for Europe. Brussels, 21.9.2005, COM (2005) 447 final, 2005/0183 (COD). Retrieved 14 June 2007 from http://ec.europa.eu/environment/air/cafe/pdf/com_2005_447_en.pdf.
Gordian, M. E., Haneuse, S., & Wakefield, J. (2006). An investigation of the association between traffic exposure and the diagnosis of asthma in children. Journal of Exposure Analysis and Environmental Epidemiology, 16(1), 49–55.
Hänninen, O. O., Alm, S., Katsouyanni, K., Künzli, N., Maroni, M., Nieuwenhuijsen, M. J., et al. (2004a). The Expolis Study: Implications for exposure research and environmental policy in Europe. Journal of Exposure Analysis and Environmental Epidemiology, 14, 440–456.
Hänninen, O. O., Kruize, H., Lebret, E., & Jantunen, M. (2003). Expolis simulation model: PM2.5 application and comparison with measurements in Helsinki. Journal of Exposure Analysis and Environmental Epidemiology, 13, 74–85.
Hänninen, O. O., Lebret, E., Ilacqua, V., Katsouyanni, K., Künzli, N., Srám, R. J., et al. (2004b). Infiltration of ambient PM2.5 and levels of indoor generated non-ETS PM2.5 in residences of four European cities. Atmospheric Environment, 38(37), 6411–6423.
Hänninen, O. O., Lebret, E., Tuomisto, J. T., & Jantunen, M. J. (2005a). Characterization of model error in the simulation of PM2.5 exposure distributions of the working age population in Helsinki, Finland. Journal of Air & Waste Managegement Association, 55, 446–457.
Hänninen, O. O., Palonen, J., Tuomisto, J., Yli-Tuomi, T., Seppänen, O., & Jantunen, M. J. (2005b). Reduction potential of urban PM2.5 mortality risk using modern ventilation systems in buildings. Indoor Air, 15(4), 246–256.
Hauglustaine, D. A., Brasseur, G. P., Walters, S., Rasch, P. J., Muller, J. F., Emmons, L. K., et al. (1998). MOZART: A global chemical transport model for ozone and related chemical tracers, 2. Model results and evaluation. Journal of Geophysical Research, 103, 28291–28336.
Istituto Superiore di Sanità (2005a). Studio di valutazione dell’esposizione inalatoria a contaminazione atmosferica nella città di Ferrara. Prima fase [Assessment study on inhalation exposure to atmospheric pollution in Ferrara] ISTISAN Report 03/19. Retrieved 14 June 2007 from http://www.iss.it/binary/publ/publi/0319.1109150761.pdf#search=%22rapporto%20istisan%2003%2F19%22 (in Italian).
Istituto Superiore di Sanità (2005b). Studio di valutazione dell’esposizione inalatoria a contaminazione atmosferica nella città di Ferrara. Seconda fase [Assessment study on inhalation exposure to atmospheric pollution in Ferrara]. ISTISAN report 05/9. Retrieved 14 June 2007 from http://www.iss.it/binary/publ/publi/05–9.1120812015.pdf#search=%22rapporto%20istisan%2005%2F9%22 (in Italian).
Kim, D., Sass-Kortsak, A., Purdham, J. T., Dales, R. E., & Brook, J. R. (2006). Associations between personal exposure and fixed-site ambient measurements of fine particulate matter, nitrogen dioxide, and carbon monoxide in Toronto, Canada. Journal of Exposure Analysis and Environmental Epidemiology, 16(2), 172–183.
Koistinen, K. J., Hänninen, O. O., Rotko, T., Edwards, R. D., Moschandreas, D., & Jantunen, M. J. (2001). Behavioral and environmental determinants of personal exposures to PM2.5 in Expolis–Helsinki, Finland. Atmospheric Environment, 35(14), 2473–2481.
Kousa, A., Oglesby, L., Koistinen, K., Kunzli, N., & Jantunen, M. (2002). Exposure chain of urban air PM2.5—Associations between ambient fixed site, residential outdoor, indoor, workplace and personal exposures in four European cities in the Expolis study. Atmospheric Environment, 36, 3031–3039.
Kruize, H., Hänninen, O. O., Breugelmans, O., Lebret, E., & Jantunen, M. (2003). Description and demonstration of the EXPOLIS simulation model: Two examples of modeling population exposure to particulate matter. Journal of Exposure Analysis and Environmental Epidemiology, 13(2), 87–99.
Laden, F., Neas, L. M., Dockery, D. W., & Schwartz, J. (2000). Association of fine particulate matter from different sources with daily mortality in six U.S. cities. Environmental Health Perspectives, 108(10), 941–947.
Letz, R., Ryan, P. B., & Spengler, J. D. (1984). Estimated distributions of personal exposure to respirable particles. Environmental Monitoring & Assessment, 4, 351–359.
Meng, Q. Y., Turpin, B. J., Korn, L., Weisel, C. P., Morandi, M., Colome, S., et al. (2005). Influence of ambient (outdoor) sources on residential indoor and personal PM2.5 concentrations: Analyses of RIOPA data. Journal of Exposure Analysis and Environmental Epidemiology, 15, 17–28.
Özkaynak, H., Xue, J., Spengler, J., Wallace, L., Pellizzari, E., & Jenkins, P. (1996). Personal exposure to airborne particles and metals: Results from the particle team study in Riverside, California. Journal of Exposure Analysis and Environmental Epidemiology, 6, 57–78.
Pellizzari, E. D., Clayton, C. A., Rodes, C. E., Mason, R. E., Piper, L. L., Fort, B., et al. (1999). Particulate matter and manganese exposures in Toronto, Canada. Atmospheric Environment, 33, 721–734.
Pielke, R. A., Cotton, W. R., Walko, R. L., Tremback, C. J., Lyons, W. A., Grasso, L. D., et al. (1992). A comprehensive meteorological modelling system—RAMS. Meteorology and Atmospheric Physics, 49, 69–91.
Pope, C. A., Burnett, R. T., Thun, M. J., Calle, E. E., Krewski, D., Ito, K., et al. (2002). Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. Journal of Americal Medical Association, 287(9), 1132–1141.
Pope, A., & Dockery, D. (2006). Health effects of fine particulate air pollution: Lines that connect. Journal of Air & Waste Management Association, 56, 709–742.
Ryan, P. B., Spengler, J. D., & Letz, R. (1986). Estimating personal exposures to NO2. Environment International, 12, 395–400.
Steppeler, J., Doms, G., Schättler, U., Bitzer, H. W., Gassmann, A., Damrath, U., et al. (2003). Meso-gamma scale forecasts using the nonhydrostatic model LM. Meteorology and Atmospheric Physics, 82, 75–96.
Tainio, T., Tuomisto, J. T., Aarnio, P., Pekkanen, J., Hänninen, O., Koistinen, K., et al. (2005). Health effects caused by primary fine particulate matter (PM2.5) emitted from busses in Helsinki Metropolitan Area, Finland. Risk Analysis, 25(1), 151–160.
Wallenius, L., Kukkonen, J., Karppinen, A., Pohjola, M., Härkönen, J., Jantunen, M., et al. (2002). Health Effects caused by urban air pollution for the transport system plan scenarios in Helsinki area-heat. In N. Moussiopoulos & K. Karatzas (Eds.) Proceedings of a SATURN-EURASAP Workshop Rhodes, Greece, 4 April 2002. Retrieved 14 June 2007 from http://aix.meng.auth.gr/saturn/aqmanagment/karpinnen.pdf.
WHO (2005). Health effects of transport-related air pollution. World Health Organisation Regional Office for Europe, Copenhagen. Retrieved 14 June 2007 from http://www.euro.who.int/document/e86650.pdf.
WHO (2006). World Health Organisation Air Quality Guidelines, Global Update 2005, Copenhagen. 484 pp. Retrieved 14 June 2007 from http://www.euro.who.int/Document/E90038.pdf.
Zauli-Sajani, S., Scotto, F., Lauriola, P., Galassi, F., & Montanari, A. (2004). Urban air pollution monitoring and correlation properties between fixed-site stations. Journal of Air & Waste Management Assocication, 54, 1236–1241.
Acknowledgment
The authors want to express their gratitude to the colleagues that have contributed to the development of the air quality information systems and models run that the current work is based on, especially Cinzia Cascone, ARPA Piemonte, Sandro Finardi, Alessio Dallura, Arianet Consulting, Marco Deserti, Linda Passoni, Vanes Polluzzi, ARPA Emilia-Romagna, and Hydro Meteorological Service (ARPA-SIM), Bologna. This work has been supported by the European Commission under the FP5 EESD program Key Action City of Tomorrow (FUMAPEX; contract no. EVK4-CT-2002-00097) and intramural funding by the participating institutions.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hänninen, O., Zauli-Sajani, S., De Maria, R. et al. Integrated Ambient and Microenvironment Model for Estimation of PM10 Exposures of Children in Annual and Episode Settings. Environ Model Assess 14, 419–429 (2009). https://doi.org/10.1007/s10666-008-9141-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10666-008-9141-y