
Abstract
The inverse relationship between physical activity and mortality may be confounded by socioeconomic factors, cardiovascular risk factors and inverse causality. We investigated long-term association between self-reported regular physical activity and mortality in a socioeconomically homogeneous, initially healthy middle-aged (mean age 47) male cohort (the Helsinki Businessmen Study). In 1974, the men were assessed with questionnaires, clinical and laboratory examinations. Cardiovascular disease (CVD) risk factors (including body mass index [BMI], age, cholesterol, glucose, systolic blood pressure and smoking) and details of physical activity of 782 men were available. Leisure time physical activity was collapsed into 3 categories: low (n = 148), moderate (n = 398) and high activity (n = 236). Physical activity was also briefly assessed in questionnaire surveys in 1985–1986 and in 2000. Total mortality up to 2007 was retrieved from the Central Population Register. Altogether 295 men (37.7%) died during the 34-year follow-up, and leisure-time physical activity was significantly related to mortality in a step-wise manner: 45.9% (n = 68), 37.7% (n = 150), and 32.6% (n = 77) died in the low, moderate, and high activity groups, respectively (P < 0.001). With high activity group as referent and adjusted for midlife CVD risk, perceived health and fitness at baseline, hazard ratio for total mortality was 1.21 (95% confidence interval: 0.90, 1.62), and 1.61 (95% confidence interval: 1.13, 2.30) in the moderate and low activity groups, respectively. Conclusion: During the 34-year follow-up, leisure-time physical activity in initially healthy middle-aged men had a graded association with reduced mortality that was independent of CVD risk, glucose and BMI.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Given that physical activity affects several cardiovascular disease (CVD) risk factors, it is possible that exercise prevents deaths simply through risk factor modification [1]. However, the known risk associations may be confounded through several pathways including lifestyle choices, social class [2] and varying adherence—or more broadly the “healthy user effect”. In other words, people who initiate and adhere to preventive habits may be systemically healthier and more health-seeking than others [3]. Furthermore, the physical activity of work and leisure time, lifestyle and other stress factors differ in both their prevalence and modifiability in various socioeconomic groups, and consequently, population-based studies may not reflect the effects of physical activity as such. In order to reduce some of these caveats, we studied the associations between leisure-time physical activity and 34-year mortality in an initially healthy and socioeconomically homogeneous cohort of middle-aged men in Helsinki, Finland.
Methods
Baseline examinations in 1974 and questionnaire surveys in 1985–1986 and 2000
The cohort and examinations have been described earlier [4]. The study procedures have been approved by the Ethics Committee of the Department of Medicine, University of Helsinki. In brief, initially healthy men of high socioeconomic status, mostly business executives born in 1919–1934, had participated in structured health check-ups during the 1960s and early 1970s at the Institute of Occupational Health in Helsinki, Finland. They were evaluated with questionnaires and clinical and laboratory examinations in 1974, whereupon 1,815 men were found to be actively working and healthy without diabetes, clinical cardiovascular disease or regular medications. Of the 1,815 men, a structured questionnaire about details of their physical activity is available for 782 men. In 1974, this detailed information was mostly (90.7%, n = 709) gathered from men who had at least one of the following risk factors: (1) serum cholesterol level 7.0 mmol/L (270 mg/dL) or higher; (2) serum triglyceride level 1.7 mmol/L (150 mg/dL) or higher; (3) systolic blood pressure 160 mm Hg or higher; (4) diastolic blood pressure 95 mm Hg or higher; (5) smoking more than ten cigarettes per day; (6) relative body weight (weight relative to mean weight for height) 120% or higher (indicating overweight); (7) 1-h glucose tolerance 9.0 mmol/L (162 mg/dL) or higher. These men were assessed to be at higher cardiovascular risk [5]. However, their age distribution as well as long-term mortality were not statistically different from those men without detailed physical activity assessment.
Although part of the men had participated in a controlled multifactorial prevention trial during the 1970s [5], our preliminary analyses showed that participation in the 1970s trial did not affect the present long-term results. Therefore, all the 782 men with detailed exercise information form the population of the present analyses.
In 1974, weight and height were measured and body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. In 1974, the men also reported their weight at 25 years of age, which was used to calculate midlife weight gain (weight in 1974 minus reported weight at 25 years of age). In 1974 the men were also asked questions on how they rated their present health and physical fitness on a 5-step scale (“very good”, “good”, “fair”, “poor”, “very poor”). To reflect composite risk of coronary artery disease, the Keys’ risk score [6] including age, BMI, smoking, cholesterol and systolic blood pressure was calculated in 1974. The Framingham risk score could not be calculated because HDL cholesterol was not available in 1974.
The men were also asked to give a global description of their leisure-time physical activity on a 4-step scale:
-
1.
Reading, watching television, going to the cinema or other sedentary activity.
-
2.
Walking, cycling, skiing, gardening, bowling, fishing or other light exercise weekly.
-
3.
Jogging, running, skiing, swimming, tennis, badminton, heavy gardening or similar exercise weekly on a regular basis.
-
4.
Regular vigorous/competitive exercise several times a week on a regular basis.
Because only 11 men reported competitive activity, groups 3 and 4 were combined in the analyses. Men answering yes to question 1 were categorized as low activity; 2 as moderate; and 3 and 4 as high activity group. Preliminary analyses showed that global description differentiated mortality risk most consistently, and therefore more detailed analyses were performed comparing these groups.
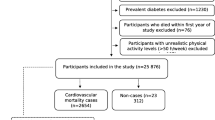
Of the 782 men, 80.7% (n = 631) and 70.6% (n = 552) could be re-assessed with questionnaires in the 11-year (1985–1986) and 26-year surveys (2000), respectively, but questions about exercise were less comprehensive than in 1974: In the 11-year survey, men were asked whether they exercised regularly and weekly, and if yes, how many hours per week; in the 26-year survey, men were asked whether they exercised regularly and weekly, and if yes, how many hours per week. However, in the 26-year survey men were also asked how many times per week they exercised with an intensity leading to sweating and breathlessness (“vigorous” activity) (Fig. 1).

Flow chart of the study. * Hypertension, dyslipidemia, overweight, gulcose intolerance or smoking
Mortality follow-up
Total mortality of the study cohort up to 31 March 2007 was retrieved from the Central Population Register, which keeps registry of all Finnish citizens. According to the Register, assessment of vital status is very reliable for people having their permanent place of residence in Finland (over 95% of the present cohort) irrespective of whether they die in Finland or abroad. Moreover, the assessment of the vital status is also quite reliable for Finnish citizens living permanently abroad. Causes of death up to 31 December 2006 were determined from the countrywide computerized Cause-of-Death Register of Statistics Finland, in which trained nosologists code the causes of death. The causes were categorized into 5 groups: cardiovascular, cancer, accidents, suicides, and other causes.
Statistical methods
NCSS statistical software (2004 version, www.ncss.com) was used for the analyses. In the analyses, global level of physical activity was categorized as described above. T-tests, nonparametric tests and analyses of covariance (ANCOVA) were used where appropriate to compare continuous variables; chi-square and trend tests were used to compare proportions. Differences in survival curves were analyzed with log rank test. Hazard ratios (HR) with their 95% confidence intervals (CI) for mortality associated with physical activity at baseline were calculated using Cox’s proportional hazards regression. Other risk factors were adjusted for in respective models. In statistical analyses 2-tailed tests were used, and P values <0.05 were taken as significant.
Results
The baseline characteristics of the study population are shown in Table 1. Of the various CVD risk factors, physical activity was inversely associated with weight gain during adulthood, BMI in midlife, and with 1-h post-load glucose concentration. Sedentary men smoked more than other groups, but serum lipid levels and blood pressure were only weakly associated with physical activity.
As a global description of physical activity, 148 (18.9%), 398 (50.9%), and 236 (30.2%) men reported low (sedentary), moderate, and high leisure-time physical activity, respectively. Most men (80.5%, n = 630) had sedentary work and commuted to work by car or public transportation. No association was observed between physical activity groups and the type of work.
Physical activity was measured three times: at baseline and in the 11- and 26-year surveys, yet the questions about physical activity were most detailed at baseline, as described above. Tracking of the baseline physical activity was good during the follow-up in the 11-year and 26-year surveys (Table 2). The reported regular weekly exercise in the 11-year and 26-year surveys was 50–70%, 69–80% and 92–85% for low, moderate and high physical activity groups, respectively (Table 2). The continuity of initially reported regular weekly exercise was significantly higher among the most physically active men in both subsequent surveys (P < 0.001 and <0.002, respectively). “Vigorous” exercise leading to sweating and breathlessness was reported by 56, 68 and 79% men in the low, moderate and high physical activity groups in the 26-year survey, while 35, 45 and 60%, respectively, performed vigorous exercise more than twice a week.
During the 34-year follow-up, 295 men died (37.8%), with the cause of death available for 282 deaths (95.6% of total). Mortality was not significantly associated with type of work (sedentary, mobile) or type of commuting to work (walking or cycling).
Global description of leisure-time physical activity significantly predicted death: mortality per 1,000 person years was 16.5, 12.9, and 10.8 (P = 0.01) in the low, moderate and high physical activity groups, respectively. Unadjusted survival curves are shown in Fig. 2, demonstrating the consistent difference between the groups. Causes of deaths are shown in Table 3, suggesting that especially CVD deaths were associated with physical activity. Multivariable analyses (Table 4) indicate that the protective effect of physical activity was independent of traditional CVD risk factors (age, BMI, cholesterol, smoking and systolic blood pressure) reflected by Keys’ risk index. The result did not change after 1-h glucose and triglycerides were added to the model.

Unadjusted survival curves according to baseline global physical activity
Discussion
The self-reported “global” leisure time physical activity was strongly associated with 34-year mortality independently of traditional CVD risk factors in a socioeconomically homogeneous cohort of men. Comparison of the causes of death showed that especially CVD mortality was associated with physical activity, supporting the findings of earlier Finnish [7–9] and other population studies in Western countries [1, 10–24].
While the difference in total work load showed the largest predictive power between the sedentary and active tertile, significant differences in mortality rates became evident after approximately 15 years of surveillance, and were interestingly shown to increase with time through the 34-year follow-up. The weekly physical activity was assessed twice during the follow-up and was shown to increase in all activity groups in both the 11-year and the 26-year survey. These findings can be accounted for by the positive effect of increasing exercise, and increasing selection through excessive mortality of sedentary participants. At the 26-year survey, vigorous exercise on a weekly basis was reported by 59 and 79% and the frequency of three times or more per week by 35 and 60% in the low and high activity groups, respectively. The exercise habit seemed to track best among the initially most active men in both surveys. An increase in both intensity and amount of exercise in all groups can be suggested to account for the dose-related decrease in mortality in relation to increased exercise.
Our results indicating that approximately 15 years of surveillance is needed before the differences between mortality rates of the low and high activity groups become evident are in accordance with a recent Swedish follow-up study [13]. It showed that an average of 10 years of increased physical activity after midlife is required to reduce excessive mortality in physically inactive men to the level of those who are physically active. Additionally, our results suggest that training has an independent dose-response effect in reducing mortality, which can even increase with time at least up to 34 years.
Both aerobic fitness and physical activity have been shown to associate with mortality. In a 16-year follow-up of Norwegian men the relative risk of death from any cause in the highest fitness quartile as compared with the lowest quartile was significantly reduced by 46% after adjustment for age, smoking status, serum lipids, blood pressure, resting heart rate, vital capacity, BMI, level of physical activity, and glucose tolerance. A high level of leisure time physical activity was strongly associated with fitness, but was not found to have an independent prognostic value. [11] In another 5.5-year prospective study with age-adjusted quartiles, a multivariate analysis including clinical characteristics, risk factors, exercise test data and activity patterns revealed that exercise capacity (HR per quartile 0.62; CI: 0.47–0.82) and energy expenditure from adulthood recreational activity (HR per quartile 0.72; CI: 0.58–0.89, P = 0.002) were the sole significant predictors of mortality [25]. It should be noted, however, that in addition to exercise training, physical fitness level is markedly influenced by hereditary factors, which can affect survival. On the other hand, regular exercise is a prerequisite for the maintenance of individual fitness level. The constancy and even increasing tendency of regular physical activity during our 34-year follow-up probably have a crucial impact on the observed mortality benefit, emphasizing the importance of a life-long sporty lifestyle.
In the present study, physical activity was inversely associated with weight gain during adulthood, BMI in midlife, and with one-hour post-load glucose concentration. Nevertheless, BMI or even one-hour glucose did not show an independent effect on mortality, in evidence against reverse causality. Our findings are in line with a follow-up study of 9.8 years in middle-aged Finnish women and men, which showed that physical inactivity has an independent effect on increased CVD risk, while obesity was concluded to increase the risk partly through the modification of other risk factors [7]. The education level included in multivariate analysis was not found to have an independent effect on CVD risk, even though it was speculated that unmeasured components of socio-economic status may strengthen the positive effect of leisure-time activity and weaken the protective effects of occupational activity [7].
It has been suggested that public health programs may be of benefit by advising each socioeconomic status group separately while considering the country’s level of development [2]. A combination of high stress levels and smoking or physical inactivity has been revealed to be especially harmful among individuals with low socioeconomic status [26]. The present study is unique in terms of a very long follow-up in a socioeconomically homogeneous cohort of men of high socioeconomic status, and it can be considered as being dated in a phase of constant and quite rapid social upswing and increasing awareness of health concerns in the Finnish society. The similarity of the results of our study with earlier Finnish population studies [7] suggests that the adoption of life-style and physical activity habits among high-economy social class of men were not markedly different from the whole population.
The distinct strength of this primary prevention study is the long follow-up time, which reduces the confounding effect of subclinical diseases at baseline. The fact that our cohort consisted of healthy men of high socioeconomic class can be considered to further reduce confounding. Most studies concerning physical activity and mortality are based on a single estimate of activity [7, 8, 14, 15, 20, 24, 27, 28], while in our study physical activity was also assessed during follow-up. Response rates to the surveys were high.
Our study also has some limitations. Physical activity was determined by self-report, which is considered to overestimate actual amounts of physical activity and thus underestimate the benefits of physical activity among older adults [10]. Despite this, our study shows a graded and independent association between physical activity and reduced long-term mortality. Another limitation is that the questionnaires sent during the follow-up were not as detailed as the questionnaire at baseline. Generally, physical activity nevertheless seems to track well during the decades in our cohort. The fact that the physical activity pattern remained largely unchanged suggests that the physical activity habits were correctly reported. A clear limitation is that our cohort consisted only of men of high socioeconomic status. However, relations between physical activity and mortality have been reported to be considerably similar between sexes [8]. Another recent study showed no significant association between leisure-time physical activity and mortality in women, but the statistical power was limited by the small number of deaths among women [23].
Conclusions
In our 34-year follow-up study, leisure-time physical activity in midlife was associated with better long-term prognosis in a stepwise manner, irrespective of CVD risk factors and BMI among men with a homogeneous socioeconomic status. Whether this longer life achieved by physical activity is also associated with better quality of life in old age is important from the compression of morbidity viewpoint and needs to be investigated further.
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- CVD:
-
Cardiovascular disease
- HR:
-
Hazard ratio
- SE:
-
Standard error
- SD:
-
Standard deviation
References
Johansson SE, Sundquist J. Change in lifestyle factors and their influence on health status and all-cause mortality. Int J Epidemiol. 1999;28(6):1073–80.
Kim S, Symons M, Popkin BM. Contrasting socioeconomic profiles related to healthier lifestyles in China and the United States. Am J Epidemiol. 2004;159(2):184–91.
Brookhart MA, Patrick AR, Dormuth C, Avorn J, Shrank W, Cadarette SM, et al. Adherence to lipid-lowering therapy and the use of preventive health services: an investigation of the healthy user effect. Am J Epidemiol. 2007;166(3):348–54.
Strandberg TE, Strandberg AY, Salomaa VV, Pitkala KH, Tilvis RS, Sirola J, et al. Explaining the obesity paradox: cardiovascular risk, weight change, and mortality during long-term follow-up in men. Eur Heart J. 2009;30(14):1720–7.
Miettinen TA, Huttunen JK, Naukkarinen V, Strandberg T, Mattila S, Kumlin T, et al. Multifactorial primary prevention of cardiovascular diseases in middle-aged men. Risk factor changes, incidence, and mortality. JAMA. 1985;254(15):2097–102.
Keys A, Aravanis C, Blackburn H, Van Buchem FS, Buzina R, Djordjevic BS, et al. Probability of middle-aged men developing coronary heart disease in five years. Circulation. 1972;45(4):815–28.
Hu G, Tuomilehto J, Silventoinen K, Barengo N, Jousilahti P. Joint effects of physical activity, body mass index, waist circumference and waist-to-hip ratio with the risk of cardiovascular disease among middle-aged Finnish men and women. Eur Heart J. 2004;25(24):2212–9.
Barengo NC, Hu G, Lakka TA, Pekkarinen H, Nissinen A, Tuomilehto J. Low physical activity as a predictor for total and cardiovascular disease mortality in middle-aged men and women in Finland. Eur Heart J. 2004;25(24):2204–11.
Pekkanen J, Marti B, Nissinen A, Tuomilehto J, Punsar S, Karvonen MJ. Reduction of premature mortality by high physical activity: a 20-year follow-up of middle-aged Finnish men. Lancet. 1987;1(8548):1473–7.
Manini TM, Everhart JE, Patel KV, Schoeller DA, Colbert LH, Visser M, et al. Daily activity energy expenditure and mortality among older adults. JAMA. 2006;296(2):171–9.
Sandvik L, Erikssen J, Thaulow E, Erikssen G, Mundal R, Rodahl K. Physical fitness as a predictor of mortality among healthy, middle-aged Norwegian men. N Engl J Med. 1993;328(8):533–7.
Slattery ML, Jacobs DR Jr, Nichaman MZ. Leisure time physical activity and coronary heart disease death. The US Railroad Study. Circulation. 1989;79(2):304–11.
Byberg L, Melhus H, Gedeborg R, Sundstrom J, Ahlbom A, Zethelius B, et al. Total mortality after changes in leisure time physical activity in 50 year old men: 35 year follow-up of population based cohort. BMJ. 2009;338:b688.
Chave SP, Morris JN, Moss S, Semmence AM. Vigorous exercise in leisure time and the death rate: a study of male civil servants. J Epidemiol Community Health. 1978;32(4):239–43.
Haveman-Nies A, de Groot LP, Burema J, Cruz JA, Osler M, van Staveren WA, et al. Dietary quality and lifestyle factors in relation to 10-year mortality in older Europeans: the SENECA study. Am J Epidemiol. 2002;156(10):962–8.
Sui X, LaMonte MJ, Blair SN. Cardiorespiratory fitness as a predictor of nonfatal cardiovascular events in asymptomatic women and men. Am J Epidemiol. 2007;165(12):1413–23.
Schnohr P, Scharling H, Jensen JS. Changes in leisure-time physical activity and risk of death: an observational study of 7, 000 men and women. Am J Epidemiol. 2003;158(7):639–44.
Paffenbarger RS Jr, Hyde RT, Wing AL, Lee IM, Jung DL, Kampert JB. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N Engl J Med. 1993;328(8):538–45.
Paffenbarger RS Jr, Hyde RT, Wing AL, Hsieh CC. Physical activity, all-cause mortality, and longevity of college alumni. N Engl J Med. 1986;314(10):605–13.
Leon AS, Connett J, Jacobs DR Jr, Rauramaa R. Leisure-time physical activity levels and risk of coronary heart disease and death. The Multiple Risk Factor Intervention Trial. JAMA. 1987;258(17):2388–95.
Chakravarty EF, Hubert HB, Lingala VB, Fries JF. Reduced disability and mortality among aging runners: a 21-year longitudinal study. Arch Int Med. 2008;168(15):1638–46.
Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024–35.
Talbot LA, Morrell CH, Fleg JL, Metter EJ. Changes in leisure time physical activity and risk of all-cause mortality in men and women: the Baltimore Longitudinal Study of Aging. Prev Med. 2007;45(2–3):169–76.
Hakim AA, Petrovitch H, Burchfiel CM, Ross GW, Rodriguez BL, White LR, et al. Effects of walking on mortality among nonsmoking retired men. N Engl J Med. 1998;338(2):94–9.
Myers J, Kaykha A, George S, Abella J, Zaheer N, Lear S, et al. Fitness versus physical activity patterns in predicting mortality in men. Am J Med. 2004;117(12):912–8.
Krueger PM, Chang VW. Being poor and coping with stress: health behaviors and the risk of death. Am J Public Health. 2008;98(5):889–96.
Lee IM, Skerrett PJ. Physical activity and all-cause mortality: what is the dose-response relation? Med Sci Sports Exerc. 2001;33(6 Suppl):S459–71. (discussion S493-4).
Yu S, Yarnell JW, Sweetnam PM, Murray L. Caerphilly study. What level of physical activity protects against premature cardiovascular death? The Caerphilly study. Heart. 2003;89(5):502–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Savela, S., Koistinen, P., Tilvis, R.S. et al. Leisure-time physical activity, cardiovascular risk factors and mortality during a 34-year follow-up in men. Eur J Epidemiol 25, 619–625 (2010). https://doi.org/10.1007/s10654-010-9483-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-010-9483-z