
Summary
Purpose AT9283 is a potent inhibitor of the mitotic regulators, Aurora-kinases A and B, and has shown anti-tumor activity in patients with solid and haematological malignancies. This phase I study assessed safety, tolerability, pharmacokinetic and pharmacodynamic properties of AT9283. Patients and methods Patients with advanced, incurable solid tumors or non-Hodgkin’s lymphoma received AT9283 as a continuous 24-hour infusion on days 1, 8 of a 21-day cycle. A 3 + 3 dose escalation design was used with a starting dose of 1.5 mg/m2/day. Pharmacokinetic samples were collected from all patients on cycle one, and pharmacodynamic samples were collected from 4 patients at the recommended phase II dose (RP2D). Results 35 patients were evaluable for toxicity and 32 were evaluable for response. AT9283 was well tolerated, with main toxicities being reversible dose-related fatigue, gastrointestinal disturbance, anemia, lymphocytopenia and neutropenia. The dose limiting toxicities were febrile neutropenia (two patients) and neutropenia with grade 3 infection (1 patient) at 47 mg/m2/day (established as the maximum tolerated dose). The RP2D was 40 mg/m2/day. Pharmacokinetic analyses showed AT9283 appeared to follow linear kinetics, with a mean elimination half-life of 8.2 h. Pharmacodynamic analyses showed no consistent or significant changes, but trends suggested evidence of AT9283 inhibition and anti-proliferative activity. One patient had partial response and four patients experienced RECIST stable disease (median 2.6 months). Conclusion In this study, AT9283 was well tolerated. The RP2D is 40 mg/m2/day on days 1, 8 of a 21-day cycle. Ongoing AT9283 trials will assess efficacy and safety in solid and haematological cancers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Members of the Aurora-kinase family have recently emerged as key mitotic regulators required for genome stability [1–5]. The Auroras (A, B and C) are involved in regulating multiple steps of mitosis including centrosome duplication, formation of a bipolar mitotic spindle, chromosome alignment on the mitotic spindle and perhaps more importantly, the fidelity-monitoring spindle checkpoint itself. Amplification of these serine/threonine kinases has been linked to oncogenesis, tumour progression, and decreased survival [4, 6, 7]. Aurora-kinase A is commonly amplified in solid human tumours and has been established as an oncogene. Aurora B overexpression leads to defects in mitosis and increased tumour invasiveness [5, 8, 9]. To date, studies have identified many tumour types in which Aurora A was amplified or otherwise overexpressed (including breast, pancreatic, ovarian and gastric tumours), suggesting the potential of Aurora-kinase inhibitors for use in a broad spectrum of cancers [5, 10–15].
AT9283 (Astex Pharmaceuticals, Cambridge, UK) is a potent inhibitor of Aurora A and B kinases. It has potent pro-apoptotic action against tumour cell lines and is less cytotoxic against normal epithelial cells than tumour cells [16–18]. AT9283 induces characteristic phenotypic effects in proliferating tumour cells by causing endoreduplication following inhibition of Histone H3 phosphorylation (pHH3) [5, 16, 17]. Potent antitumour effects have been demonstrated in a number of xenograft models [5, 16–18]. Two phase I trials have been conducted with AT9283 delivered as a 72 h intravenous infusion every 3 weeks (Online Resource 1) [19–22]. Treatment was generally well tolerated: main toxicities reported were reversible dose-related myelosuppression, gastrointestinal disturbance, fatigue and alopecia. Febrile neutropenia (FN) was the dose limiting toxicity (DLT) in patients with solid tumours while tumour lysis syndrome was the DLT in patients with hematological malignancies.
We report a phase I trial of AT9283 given as a 24 h continuous infusion on days 1 and 8 every 21 days. The primary endpoint was to determine the recommended phase II dose (RP2D) of AT9283 given in this schedule. Secondary objectives were to determine safety and tolerability, pharmacokinetic (PK) and pharmacodynamic (PD) profiles, and anti-tumour activity [measured by the Response Evaluation Criteria in Solid Tumours (RECIST) [23] of AT9283. An assessment of AT9283 on pharmacodynamic endpoints was planned for patients enrolled at the RP2D.
Materials and methods
Eligibility criteria
Patients with advanced, incurable solid tumours or non-Hodgkin’s lymphoma (NHL) who had received up to two lines of systemic therapy for metastatic disease (no limitations for NHL), Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2, with adequate bone marrow reserve, liver and renal function were eligible for this study. There were no limitations on prior hormonal, immunological, biologic or signal transduction inhibitor therapy. At least 21 days must have elapsed from prior palliative radiotherapy or systemic therapy.
Patients with uncontrolled hypertension, cardiovascular conditions, symptomatic cardiac disease, untreated brain metastases, active or uncontrolled infections, or those receiving concurrent treatment with other experimental drugs or anti-cancer therapy were excluded.
This study was approved by the research ethics board of each participating center. All patients provided written informed consent, and the study was conducted in accordance with good clinical practice guidelines.
Patient evaluation
Pre-treatment evaluation included a history and physical, hematology, biochemistry, coagulation parameters, urinalysis, pregnancy test (for premenopausal women), ECG, CXR and other imaging to document disease. During treatment, hematology evaluations were performed twice weekly for cycles 1 and 2, and weekly for each subsequent cycle. Biochemistry was measured weekly for cycles 1 and 2 and then on day 1 of each subsequent cycle. Patient history and physical assessment were performed on day 1 of each cycle. Disease status was assessed every 6 weeks using RECIST [23]. Toxicity was graded using the Common Toxicity Criteria for Adverse Events Version 3.0 (National Cancer Institute, Bethesda, Maryland).
Therapy
AT9283 was administered as a 24-hour infusion on days 1 and 8 every 21 days. The starting dose was 1.5 mg/m2/24 h, representing 1/3 of the starting dose intensity of previous 72 h infusion trials. A minimum of three evaluable patients were entered at each dose level until the maximum tolerated dose (MTD) was reached. Dose escalation to the next dose level occurred when none of the first three patients exhibited DLT during the first cycle of treatment. If 1/3 patients experienced a DLT at a given dose level, then at least three additional patients were treated at the same dose level for a total of six patients. If no additional DLT occurred, accrual began at the next higher dose level. If at least 2/3 or 2/6 patients experienced a DLT, dose escalation was stopped and that dose level was declared the MTD. The next lower dose was the RP2D and was to be expanded to enrol up to eight additional patients.
Dose escalation was based on the worst drug related toxicity recorded in cycle 1 at the previous dose level; if grade 1, doses could be escalated 50–100 %, and if grade 2, 30–49 %. DLT was defined as the following AT9283-related toxicities in cycle 1: ≥ grade 3 non-hematologic toxicity (excluding alopecia, inadequately premedicated nausea and vomiting); grade 4 neutropenia ≥ 5 days duration; grade 4 thrombocytopenia; FN or thrombocytopenic bleeding; and/or a delay of administration of cycle 2 by 14 days or longer.
AT9283 was discontinued for grade 4 toxicity. If grade 3 toxicity (excluding alopecia and unpremedicated nausea and vomiting) was documented, AT9283 was held but could be resumed after resolution of toxicity to grade 1 or 2 at one dose level lower than the previous dose. Patients were discontinued from protocol treatment if the treatment delay (for toxicity) was greater than 14 days.
Pharmacokinetics
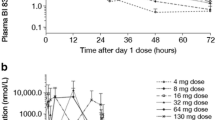
Blood samples for pharmacokinetic assessment were collected on day 1 (prior to infusion and 0.5, 3, 6, 8 and 10–12 h post start); day 2 (prior to end of infusion and 5, 15, 30, 60, 120 and 360 min post end infusion) and day 3 (24 h post end of infusion) from all patients for cycle 1 only. Samples were centrifuged immediately and plasma stored at −20 °C until analysis. Plasma AT9283 concentrations were measured using a validated high pressure liquid chromatograph-tandem mass spectrometry method. The pharmacokinetic parameters for AT9283 were calculated using non-compartmental techniques with WinNonLin Professional (Version 5.3, Pharsight Corp., St. Louis, USA).
Pharmacodynamics
All patients enrolled at the expanded RP2D level underwent sampling for pharmacodynamic endpoints including: pHH3, Ki67 p53, and PCNA. Skin biopsies (suggested site upper outer quadrant of gluteal skin) were obtained before the first infusion of AT9283, at the end of the first infusion (day 2) and 24 h after the end of the first infusion (day 3). Tumour biopsies were obtained before the first infusion of AT9283 and 24 h after the end of the first infusion (day 3). Skin biopsies were analysed by counting the number of positively stained cells in a defined epidermal area. Tumour biopsies were analysed by Astex Pharmaceuticals.
The NCIC Clinical Trials Group (NCIC CTG) sponsored the trial and performed all data management and analyses. Astex Pharmaceuticals Inc. supplied study drug and contributed financial resources to support the conduct of this trial.
Results
Patients
Characteristics of the 35 enrolled patients are summarized in Table 1. All patients were eligible and evaluable for toxicity and 32 patients were evaluable for response. Colorectal cancer (17/35) was the most common tumour type and the majority of patients (28/35) had multiple sites of disease involvement and had received multiple prior chemotherapy regimens.
Dose escalation and dose limiting toxicity
Minimal toxicity was observed in the first 4 dose levels therefore doses of AT9283 were escalated by 100 % for dose levels 1–5. Grade 2 toxicity (lymphopenia) was observed in one patient at dose level 5 and thus further dose escalation was performed as per protocol (30 % dose escalation). DLT (FN) was documented in one patient treated at dose level 8 (MTD - 47 mg/m2/day) (Table 2). Three more patients were enrolled at this dose level. Another DLT (grade 3 infection with grade 3 or 4 neutropenia) was documented in one patient. Three patients were then accrued to an intermediate dose level (40 mg/m2/day - dose level 9) with no DLT documented, although one patient had an episode of FN in cycle 2. Thus, the RP2D was defined as 40 mg/m2/day. Four more patients were enrolled at the RP2D level and had serial skin and tumour biopsies performed and blood collected.
Adverse events
The majority of treatment-related toxicities were grade 1–2 and included reversible fatigue, nausea, vomiting, anorexia, diarrhea and dose related myelosuppression (Table 3). At dose level 4 (9 mg/m2/day), there was one case of grade 3 dyspnea and two cases of grade 3 lymphocytopenia. At 36 mg/m2/day (dose level 7), grade 3 nausea, diarrhea, vomiting, and lymphocytopenia were documented (one patient each). At the MTD, two patients experienced DLT (FN and grade 3 infection), while at the RP2D, one patient had unrelated grade 3 dyspnea, two patients had unrelated grade 4 fatigue and one patient experienced treatment related FN.
No patients discontinued treatment due to drug related adverse events. Of the 14 reported serious adverse events: five patients experienced progressive disease (PD) (unrelated to study) resulting in two deaths. Other adverse events, unrelated to study treatment, included: hydronephrosis (2 pts); bowel obstruction (1 pt); pulmonary embolism (1 pt); and dehydration (2 pts). Serious adverse events related to study protocol included: neutropenia and sepsis (1 pt at RP2D) and FN (2 pts at MTD).
Drug delivery and delays
Dose intensity at dose levels 1–5 was 100 % (Online Resource 2). One patient treated at 24 mg/m2/day (dose level 6) did not get full day 1 dose due to problems with the peripherally inserted central catheter. One patient treated at 36 mg/m2/day (dose level 7) missed doses and had treatment delayed on several occasions for reasons unrelated to protocol therapy. At the highest dose level (47 mg/m2/day), granulocytopenia led to missed (2 pts), delayed (2 pts) and reduced doses (1 pt). Overall, at the MTD, only 50 % of patients received ≥ 90 % of planned dose intensity. At the RP2D (40 mg/m2/day), dose intensity was 71.4 %, with one patient requiring dose reduction and delay due to thrombocytopenia. Additionally, treatment was delayed in one patient due to fatigue and in three other patients for reasons unrelated to protocol therapy.
Antitumour activity
Thirty-two patients were evaluable for response. One patient with squamous cell carcinoma of the anal canal treated at 36 mg/m2/day had a confirmed partial response (PR) and went off protocol with symptomatic progression after receiving a total of 17 cycles of treatment. Four patients (treated at dose levels 2, 3, 6 and 9) had a best response of stable disease (SD) (median duration 2.6 months; range 2.1–3.5). One of these patients (treated at dose level 9) had skin biopsies at the RP2D (see Table 4, patient 3). A total of 27 patients had a best response of PD. Twenty seven patients had measurable lesions and subsequent response evaluation (seven were not reassessed, one had no measurable lesions) with changes in measurable lesion size shown in Online Resource 3.
Pharmacokinetics
Thirty-four patients were evaluable for pharmacokinetic evaluation. One patient treated at 24 mg/m2/day (dose level 6) did not get full day 1 dose due to difficulties accessing the central line. AT9283 pharmacokinetic parameters are summarized in Online Resource 4 and Figs. 1 and 2. There was a dose-proportional increase in AUCt, AUCinf and Cmax. The mean elimination half-life was 8.2 h (range: 5.0–18.0 h). The degree of granulocytopenia correlated significantly with AUCs and Cmax.

Pharmacokinetic evaluation of AUCinf versus dose level. vs versus, SD standard deviation

Pharmacokinetic evaluation of CMax versus dose level. vs versus, SD standard deviation
Pharmacodynamics
Pharmacodynamic evaluations were performed on four patients treated at the RP2D level (40 mg/m2/day) (see Table 4). In this small sample of skin biopsies a decrease in pHH3 levels (no positive cells) was observed in three patients post infusion, indicating Aurora inhibition. One patient showed a slight increase of pHH3 levels 24 h after infusion reflecting possible resistance. There was stabilization of p53 levels in all patients following infusion of AT9283. The majority of patients (3/4) in this subset demonstrated a decrease in PCNA and Ki67 levels. In one of four patients with a best response of SD (Table 4; patient 3), there was a decrease in pHH3, stabilization of p53, and decrease in PCNA and Ki67 levels consistent with Aurora-kinase inhibition. In contrast, one patient demonstrated an increase in Ki67 and PCNA levels. Of the two patients who underwent tumour biopsies pre and post AT9283 infusion, there were no consistent findings, although one patient showed more apoptosis post-infusion and the other patient had a larger necrotic area post-infusion.
Discussion
Members of Aurora-kinase family are key mitotic regulators required for genome stability [1–3] and have been identified, based on preclinical data as potential promising anti-cancer agents.
In this phase I dose escalation study, we demonstrated that AT9283, given as a 24 h infusion on days 1 and 8 every 21 days had a tolerable toxicity profile. The RP2D of AT9283 in this schedule was established as 40 mg/m2/day and the DLT was FN. Clinically, one patient with squamous cell carcinoma of the anal canal demonstrated a PR, and four patients had SD. The pharmacokinetics of AT9283 appear to follow linear kinetics, with dose proportional increases in AUCs and Cmax (Figs. 1 and 2).
Biological evidence of Aurora inhibition has been correlated with a reduction in pHH3 (Online Resource 1) [19–22]. Plummer et al. [19] also noted that reduction in pHH3 was accompanied by stabilization of p53 which was more marked in patient samples exhibiting complete inhibition. In our subset of patients analyzed for pharmacodynamics, changes in pHH3, Ki67, p53 or PCNA were demonstrated in a surrogate tissue (skin) in most patients. The trend towards a decrease in pHH3 is consistent with the literature and is reflective of biological evidence of Aurora inhibition [19–22, 24]. In keeping with previous studies, p53 levels appeared to stabilize after AT9283 infusion, which is typically seen in patients exhibiting complete Aurora inhibition [19]. The decrease in PCNA and Ki67 levels demonstrated in this study is encouraging given that high levels of these markers are seen in aggressive tumours with a high risk of relapse [25, 26]. In contrast to these trends, one patient showed an increase in pHH3, Ki67 and PCNA, suggestive of biological resistance to AT9283. In the two patients who underwent tumour biopsies pre and post AT9283 infusion, there were no consistent results. Given the small number of patient samples available for pharmacodynamic analysis, these results should be considered exploratory.
Our findings are in keeping with other phase I studies that have been conducted with AT9283 in patients with solid and hematological malignancies (Online Resource 1). The MTD (47 mg/m2/day) in this phase I trial is higher than demonstrated in the other solid tumour study, in which AT9283 was delivered as a 72 h continuous infusion every 3 weeks (MTD 9 mg/m2/day). In contrast, patients with refractory AML, ALL and high risk MDS have tolerated much higher doses of AT9283 (MTD of 108 mg/m2/day) [20] administered as a 72 h continuous infusion. These results have led to the exploration of prolonged infusions (up to 6 days) in this patient population.
The toxicities reported with AT9283 in the literature were mostly reversible and included gastrointestinal disturbance, fatigue, and myelosupression [19–22]. FN was the most commonly reported DLT in patients with solid malignancies, while tumour lysis syndrome and elevated enzymes were seen in the Foran et al. [20] leukemia trial. This is similar to the toxicity profile and DLTs observed in this phase I study with predominantly reversible gastrointestinal disturbance, fatigue and hematological toxicities.
A number of phase I/II studies have been conducted with other Aurora-kinase inhibitors (Online Resource 1). Dosing schedules have varied: 250–400 mg/m2/day given over 1 day every 3 or 4 weeks; 40–80 mg/m2/day given daily over a 5–14 day period, every 21–28 days; and 300–600 mg/m2/day on day 1, every 7–14 days. No differences in clinical benefit have been observed based on treatment schedule; however, smaller doses over a longer time period have been better tolerated. Similar to AT9283, the majority of toxicities experienced with other Aurora-kinase inhibitors have been mild and include reversible myelosuppression, fatigue and gastrointestinal events. The most common DLT has been neutropenia. In contrast, MLN8054 has primarily neurotoxic effects such as neurocognitive disturbance and somnolence [27, 28].
The clinical activity of single agent AT9283 reported in phase I trials has been modest with SD reported in 7–14 % of patients. We observed encouraging clinical activity in this study, with a PR observed in one patient and SD in 12.5 %. When used in leukemias, Aurora-kinase inhibitors have shown higher success rates with 14–43 % of patients experiencing clinical benefit.
The activity and tolerance of AT9283 demonstrated in this phase I study suggests that it may have potential in the treatment of a number of different tumour types. Santo et al. [18] reported growth inhibitory effects of AT9283 on multiple myeloma cell lines and patient derived cells, suggesting that Aurora-kinase inhibitors are potential therapeutic targets in myeloma [29]. The NCIC CTG launched a phase II study of AT9283 (IND.191) in patients with relapsed or refractory multiple myeloma based on the RP2D schedule of our phase I study. One case of FN was observed early in the trial resulting in a dose reduction of AT9283 to 30 mg/m2/day. The trial was closed in July 2012 due to poor accrual (8 patients).
In conclusion, this phase I study showed that AT9283 was well tolerated with a RP2D of 40 mg/m2/day given on day 1 and 8 every 21 days, while febrile neutropenia was the dose limiting toxicity. Based on results from this phase I study, further exploration of AT9283 at the RP2D schedule given on day 1 and 8 every 21 days in the phase II setting is warranted. Several trials of AT9283 and other Aurora-kinase inhibitors are underway in both solid and hematological malignancies. These trials will help define the optimal administration schedules, preferred combination partners, and the development of adequate biomarkers in selected tumour types.
References
Adams RR, Carmena M, Earnshaw WC (2001) Chromosomal passengers and the (aurora) ABCs of mitosis. Trends Cell Biol 11:49–54
Carmena M, Earnshaw WC (2003) The cellular geography of aurora kinases. Nat Rev Mol Cell Biol 4:842–854
Nigg EA (2001) Mitotic kinases as regulators of cell division and its checkpoints. Nat Rev Mol Cell Biol 2:21–32
Moore AS, Blagg J, Linardopoulos S, Pearson AD (2010) Aurora kinase inhibitors: novel small molecules with promising activity in acute myeloid and Philadelphia-positive leukemias. Leukemia 24:671–678
Qi W, Liu X, Cooke LS, Persky DO, Miller TP, Squires M et al (2012) AT9283, a novel aurora kinase inhibitor, suppresses tumour growth in aggressive B-cell lymphomas. Int J Cancer 130(12):2997–3005
Nadler Y, Camp RL, Schwartz C, Rimm DL, Kluger HM, Kluger Y (2008) Expression of Aurora A (but not Aurora B) is predictive of survival in breast cancer. Clin Cancer Res 14(14):4455–4462
Landen CN Jr, Lin YG, Immaneni A, Deavers MT, Merritt WM, Spannuth WA et al (2007) Overexpression of the centrosomal protein Aurora-A kinase is associated with poor prognosis in epithelial ovarian cancer patients. Clin Cancer Res 13(14):4098–4104
Bischoff JR, Anderson L, Zhu Y, Mossie K, Ng L, Souza B et al (1998) A homologue of Drosophila aurora kinase is oncogenic and amplified in human colorectal cancers. EMBO J 17(11):3052–3065
Renshaw JS, Patnaik A, Gordon M, Beeram M, Fischer A, Gianella-Borradori A et al (2007) A phase I two arm trial of AS703569 (R763), an orally available aurora kinase inhibitor, in subjects with solid tumors; preliminary results. J Clin Oncol 25(suppl):622s, abstract 14130
Gritsko TM, Coppola D, Paciga JE, Yang L, Sun M, Shelley SA et al (2003) Activation and overexpression of centrosome kinase BTAK/Aurora-A in human ovarian cancer. Clin Cancer Res 9(4):1420–1426
Katayama H, Ota T, Jisaki F, Ueda Y, Tanaka T, Odashima S et al (1999) Mitotic kinase expression and colorectal cancer progression. J Natl Cancer Inst 91(13):1160–1162
Li D, Zhu J, Firozi PF, Abbruzzese JL, Evans DB, Cleary K et al (2003) Overexpression of oncogenic STK15/BTAK/Aurora A kinase in human pancreatic cancer. Clin Cancer Res 9(3):991–997
Miyoshi Y, Iwao K, Egawa C, Noguchi S (2001) Association of centrosomal kinase STK15/BTAK mRNA expression with chromosomal instability in human breast cancers. Int J Cancer 92(3):370–373
Sakakura C, Hagiwara A, Yasuoka R, Fujita Y, Nakanishi M, Masuda K et al (2001) Tumour-amplified kinase BTAK is amplified and overexpressed in gastric cancers with possible involvement in aneuploid formation. Br J Cancer 84(6):824–831
Sen S, Zhou H, Zhang RD, Yoon DS, Vakar-Lopez F, Ito S et al (2002) Amplification/overexpression of a mitotic kinase gene in human bladder cancer. J Natl Cancer Inst 94(17):1320–1329
Howard S, Berdini V, Boulstridge JA, Carr MG, Cross DM, Curry J et al (2009) Fragment-based discovery of the pyrazol-4-yl urea (AT9283), a multi-targeted kinase inhibitor with potent Aurora kinase activity. J Med Chem 52(2):379–388
Curry J, Angove H, Fazal L, Lyons J, Reule M, Thompson N et al (2009) Aurora B kinase inhibition in mitosis: strategies for optimising the use of Aurora kinase inhibitors such as AT9283. Cell Cycle 8(12):1921–1929
Santo L, Hideshima T, Nelson EA et al (2009) AT9283, a small molecule multi-targeted kinase inhibitor induces antimyeloma activity via potent aurora kinase and STAT3 inhibition [abstract]. In: American Society Haematology Annual Meeting and Exposition, December 5–8, 2009, New Orleans, USA. Abstract 3883, Poster III-769
Plummer ER, Calvert H, Arkenau H, Mallett KH, Squires M, Smith D et al (2008) A dose-escalation and pharmacodynamic study of AT9283 in patients with refractory solid tumours. J Clin Oncol 26(May 20 Suppl): 117s abstract 2520
Foran JM, Ravandi F, O’Brien SM, Borthakur G, Rios M, Boone P et al (2008) Phase I and pharmacodynamic trial of AT9283, an aurora kinase inhibitor in patients with refractory leukemia. J Clin Oncol 27(155 Suppl):15s abstract 2566
Kristeleit R, Calvert H, Arkenau H, Olmos D, Adam J, Plummer ER et al (2009) A phase I study of AT9283, an aurora kinase inhibitor, in patients with refractory solid tumours. J Clin Oncol 27(Suppl 15s): abstract 2566
Arkenau HT, Plummer R, Molife LR, Olmos D, Yap TA, Squires M et al (2012) A phase I dose escalation study of AT9283, a small molecule inhibitor of aurora kinases, in patients with advanced solid malignancies. Ann Oncol 23(5):1307–1313
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L et al (2000) New guidelines to evaluate the response to treatment in solid tumours. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 92(3):205–216
Walsby E, Walsh V, Pepper C, Burnett A, Mills K (2008) Effects of the aurora kinase inhibitors AZD1152-HQPA and ZM447439 on growth arrest and polyploidy in acute myeloid leukemia cell lines and primary blasts. Haematologica 93(5):662–669
Linden MD, Torres FX, Kubus J, Zarbo RJ (1992) Clinical application of morphological and immunocytochemical assessments of cell proliferation. Am J Clin Pathol 97(5 Suppl 1):S4–S13
Cuevas E, Jones D, Wright D (1993) Immunohistological detection of tumour growth fraction (Ki-67 antigen) in formalin-fixed and routinely processed tissues. J Pathol 169(4):477–478
Dees EC, Infante JR, Cohen RB, O’Neil BH, Jones S, von Mehren M et al (2011) Phase 1 study of MLN8054, a selective inhibitor of Aurora A kinase in patients with advanced solid tumours. Cancer Chemother Pharmacol 67(4):945–954
Macarulla T, Cervantes A, Elez E, Rodriguez-Braun E, Baselga J, Rosello S et al (2010) Phase I study of the selective Aurora A Kinase Inhibitor MLN8054 in patients with advanced solid tumours: safety, pharmacokinetics, and pharmacodynamics. Mol Cancer Ther 9(10):2844–2852
Shi Y, Reiman T, Li W, Maxwell CA, Sen S, Pilarski L et al (2007) Targeting aurora kinases as therapy in multiple myeloma. Blood 109(9):3915–3921
Grant support
The trial was supported in part by the Canadian Cancer Society Research Institute core grant to the NCIC Clinical Trials Group and a research grant from Astex Pharmaceuticals Inc.
Conflicts of interest
J. Lyons is a full time employee of Astex Pharmaceuticals. All other authors declare they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial support from the Canadian Cancer Society Research Institute and Astex Pharmaceuticals Inc.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Online Resource 1
(PDF 94 kb)
Online Resource 2
(PDF 62 kb)
Online Resource 3
(PDF 9 kb)
Online Resource 4
(PDF 22 kb)
Rights and permissions
About this article
Cite this article
Dent, S.F., Gelmon, K.A., Chi, K.N. et al. NCIC CTG IND.181: Phase I study of AT9283 given as a weekly 24 hour infusion in advanced malignancies. Invest New Drugs 31, 1522–1529 (2013). https://doi.org/10.1007/s10637-013-0018-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10637-013-0018-9