
Abstract
Background and Aims
Surgically altered gastrointestinal (GI) tract anatomy hinders deep enteroscopy. While enteroscopy-assisted endoscopic retrograde cholangiopancreatography (ERCP) in patients with altered GI anatomy has been heavily investigated, the role of non-ERCP balloon-assisted enteroscopy (BAE) has yet to be fully elucidated.Please check and confirm the author names and initials are correct. Also, kindly confirm the details in the metadata are correct.I have checked all you asked and have no correction. Thank you.
Methods
A multicenter retrospective study of non-ERCP BAEs in patients with surgically altered GI tract anatomy at two tertiary academic hospitals was performed from January 2006 to December 2020. Altered GI tract anatomy was defined by surgical reconstruction affecting the length, angle, or overall trajectory of the endoscope during the intended approach. The main outcome measurements included technical success rate, diagnostic and therapeutic yields, and complication rate.Please check the edit made in the title of the article and correct if necessary.No more correction. Thank you.
Results
A total of 68 patients with surgically altered GI tract anatomy underwent 56 antegrade and 24 retrograde non-ERCP BAE procedures. The technical success rate was 86.2% in both, including 83.9% via antegrade approach and 91.7% via retrograde approach. Antegrade approach in Roux-en-Y anatomy was associated with the lowest success rate of 77.8%, whereas retrograde approach in patients with colon resection resulted in the highest rate of 100%. The diagnostic and therapeutic yields of non-ERCP BAE were 79.4% and 82.9%, respectively. The diagnostic yields varied according to the procedural indications. The major complication was luminal perforation in one case (1.3%).
Conclusions
Non-ERCP BAE is effective and safe via both antegrade and retrograde approaches with a high technical success rate and diagnostic and therapeutic yields in patients with surgically altered GI tract anatomy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Since overtube-assisted double-balloon enteroscopy (DBE) was firstly introduced in 2001 as a new method of deep enteroscopy [1], balloon-assisted enteroscopy (BAE) heralded a new chapter in extensive endoscopic examination of the small intestine. Unlike other diagnostic modalities of the small intestine such as computed tomography or magnetic resonance enterography, or wireless capsule endoscopy, enteroscopy offers therapeutic intervention as along with diagnosis of the small bowel pathology. The advantages of BAE include relatively long insertion depth and noninvasiveness compared with push enteroscopy and intraoperative enteroscopy [2, 3].
However, surgically altered gastrointestinal (GI) tract anatomy is a major obstacle preventing successful BAE. First, areas that are easily reached via BAE in patients with native anatomy may no longer be accessible. Second, intra-abdominal adhesions due to past laparotomies create sharp angles, which are difficult to navigate with larger-diameter enteroscope and result in a long length of insertion. Third, the presence of an anastomosis increases the risk of perforation during the procedure [4].
Previous studies in surgically altered GI tract anatomy mostly focused on enteroscopy-assisted endoscopic retrograde cholangiopancreatography, ERCP [5,6,7,8]. BAE increases the success rate of ERCP in patients with anatomical alterations of GI that prevent access to the pancreaticobiliary system via conventional endoscopy. In a systematic review, the overall success rate of BAE-assisted ERCP in patients with surgically altered GI tract anatomy was 74%, with variations according to the type of surgical anatomy [8]. However, few studies have evaluated non-ERCP indications [9,10,11]. Further, these studies are weak in study design, including a single-center design, inadequate sample size, and a relatively small number of retrograde BAEs.
Therefore, the aim of our study was to evaluate the success rate, efficacy, and safety of both antegrade and retrograde non-ERCP BAE procedures in patients with surgically altered GI tract anatomy using enteroscopy databases from two academic hospitals.
Methods
Study Population
The present study was designed as a multicenter retrospective study of patients with surgically altered GI tract anatomy who underwent BAE at two tertiary academic hospitals (Seoul St. Mary’s Hospital and Soonchunhyang University Hospital, Seoul, Korea) from January 2006 to December 2020. Altered GI tract anatomy was defined by surgical reconstruction affecting the length, angle, or overall trajectory of the endoscope during the intended approach [12]. Patients with surgically altered GI tract that was irrelevant to the examination (e.g., a patient with Roux-en-Y anatomy who was undergoing a retrograde BAE) were excluded from the analysis (n = 12). BAE-assisted ERCP was not evaluated in this study.
Data were collected from the electronic medical records and enteroscopy reports from the two hospitals above. The details included patients’ sex, age, type of surgical anatomy, indication for procedure, procedural duration, estimated depth of BAE insertion, technical success, diagnostic yield, therapeutic yield, and adverse events. The depth of insertion was estimated by landmarks rather than metric distance because the destination often was anatomic. This study was approved by an independent Institutional Review Board (IRB Number: XC21RCDI0121, date of approval 2021-09-17) and conformed to the ethical guidelines of the 1975 Helsinki Declaration. Informed consent was waived for this retrospective study in accordance with the Institutional Review Board.
Endoscopic Procedure
BAE was performed by five expert endoscopists from two institutions with experience involving more than 100 BAE procedures. The decision of whether to perform the BAE via antegrade and/or retrograde approaches was dependent on the endoscopist choice based on the patient’s clinical presentation and prior endoscopy and radiology findings. All BAEs were performed after obtaining appropriate informed consent.
Enteroscopy procedures were performed using a commercially available DBE system (EN-450P5, T5 or EN-530T; Fujinon, Inc., Saitama, Japan) or a single-balloon enteroscopy (SBE) system (Olympus Optical Co., Ltd., Tokyo, Japan). The selection of the insertion route depended on the suspected lesion location which was based on pre-procedure examinations such as capsule endoscopy or cross-sectional imaging. In the BAE via antegrade approach, patients were nil by mouth for at least 8 h before the procedure. In the BAE via retrograde approach, patients were prepared for colonoscopy using at least 2 L polyethylene glycol–electrolyte lavage solution the day before the procedure, which was the accepted protocol at that time. BAE procedures were performed on patients monitored via anesthesia with a fluoroscopy unit. All BAE procedures were performed under conscious and moderate sedation with intravenous midazolam administered by endoscopists following the sedation protocol of each center. BAEs were performed in standard fashion for DBE and SBE, respectively. Most enteroscopic therapeutic interventions including hemostasis, balloon dilatation, and polypectomy were performed in the same manner as duodenoscopy or colonoscopy.
Definitions
Technical success was defined by access to the intended anatomical area based on the procedural goal regardless of diagnosis or therapy. Diagnostic yield was defined as achieving any pertinent findings associated with the procedural indications [11]. BAEs performed during follow-up examination, established diagnosis, or therapeutic interventions such as removal of bezoar were excluded from the calculation of diagnostic yield. Therapeutic yield was defined as the number of BAE procedures successfully able to perform appropriate endoscopic treatment for the pertinent indication of the procedure. Biopsy procedures for diagnosis were not included in this calculation.
Statistical Analysis
Descriptive statistics were used to characterize the demographic features of the study population. Continuous variables were expressed as mean (± standard deviation). Categorical variables were expressed as number (percentage) and compared between groups using χ2 or Fisher’s exact test as appropriate. All data analyses were performed using R software version 4.1.0.
Results
A total of 80 non-ERCP BAE procedures involving 68 patients (58.8% male) with surgically altered GI anatomy were included. Patients’ mean age was 56.7 years (range 21–84 years, Table 1). Two most common indications for non-ERCP BAE were intestinal obstruction (n = 21) and obscure GI bleeding (n = 20). The other indications were followed by therapy (n = 16), abdominal pain (n = 9), polyposis or neoplastic evaluation (n = 5), Crohn’s disease (n = 5), and others (n = 4). BAE for therapy included small bowel polypectomy (n = 5), removal of migrated stent (n = 5) or impacted bezoar (n = 4), small bowel stent placement (n = 1) and perforation closure (n = 1). Based on the type of enteroscopy, 48 (60%) procedures were performed with SBE. Based on the approach route, 56 (70%) BAEs were performed via antegrade approach, and 24 (30%) BAEs via retrograde approach.
Based on surgically altered GI tract anatomy, small bowel resection (n = 22, 39.3%) was the most frequent type of surgical anatomy in the antegrade approach of BAE, which was followed by total gastrectomy with Roux-en-Y esophagojejunostomy (n = 10, 17.9%), common bile duct (CBD) resection with Roux-en-Y hepaticojejunostomy (n = 8, 14.3%), pylorus-preserving pancreaticoduodenectomy (n = 7, 12.5%), subtotal gastrectomy with Billroth-II anastomosis, and Whipple operation (n = 2, 3.6%, Table 2). In case of BAE via retrograde approach, small bowel resections were performed in 14 (58.3%), whereas colon resection alone was done in 10 cases (41.7%).
The technical success rate, diagnostic yield, and therapeutic yield of non-ERCP BAE were 86.2% (69/80), 79.4% (54/68), and 82.9% (34/41), respectively (Table 3). Based on the approach route, the technical success rate, diagnostic yield, and therapeutic yield of BAE via antegrade approach were 83.9%, 80.4%, and 82.1%, respectively, and 91.7%, 77.3%, and 84.6%, respectively, via retrograde BAE. In case of antegrade approach, the technical success rate of BAE in patients with Roux-en-Y anatomy was lower than in those with non-Roux-en-Y anatomy, although the difference was not statistically significant (77.8% vs. 86.8%, p = 0.448). In case of retrograde approach, all BAE procedures of patients who underwent only colon resection were successful, whereas the technical success rate in patients who underwent small bowel resection was 84.6%. However, there was no statistically significant difference (p = 0.448). Dividing the diagnostic yield according to the indications for the procedure, diagnostic BAEs indicated for polyposis or neoplastic evaluation and Crohn’s disease were all successful, whereas the diagnostic yield of BAE was 55.6% when the indication was abdominal pain (Table 4). One major complication (luminal perforation) occurred during BAE via antegrade approach. It was managed by surgically primary closure.
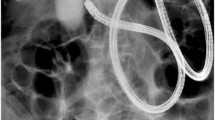
Findings with positive diagnostic yield and successful therapeutic interventions are presented in Table 5. The most common diagnosis was luminal stenosis (35.2%, 19 of 54 procedures), followed by ulcer (22.2%, 12 of 54 procedures) and angioectasia (9.3%, 5 of 54 procedures). The most common successful therapeutic intervention was clip placement (32.4%, 11 of 34 procedures), followed by balloon dilatation (29.4%, 10 of 34 procedures) and polypectomy (11.8%, 4 of 34 procedures). Figure 1 shows representative images of therapeutic interventions by BAE. We also analyzed the long-term outcomes after therapeutic interventions with a median follow-up period of 12 months (range 2–24 months). After hemostasis via clip placement or argon plasma coagulation, rebleeding occurred in 16.7% (2 of 12 procedures), of which one patient was treated with transcatheter arterial embolization. After resolution of intestinal obstruction via balloon dilatation or small bowel stent placement, relapse of obstruction or luminal narrowing occurred in 46.2% (6 of 13 procedures), of which two patients underwent small bowel segmental resection with adhesiolysis.

Representative images of therapeutic interventions by BAE. a Clip placement. b Balloon dilatation. c Polypectomy. d Removal of migrated stent. e Removal of impacted bezoar
Discussion
Although BAE has been performed widely in patients with surgically altered GI tract, such studies were mainly focused on BAE-assisted ERCP. Only a few studies focusing non-ERCP BAE were reported, and most of them analyzed only antegrade BAE [9, 11]. Our study investigated a relatively large number of non-ERCP BAEs including both antegrade and retrograde examinations in patients with surgically altered GI tract affecting the insertion route. In our study, we found a high technical success rate (86.2%) of non-ERCP BAE in such patients, which was comparable to that of BAE involving normal GI tract anatomy [13, 14]. Diagnostic and therapeutic yields were satisfactory. In addition, the efficacy of retrograde BAE was comparable to that of antegrade BAE. All procedures associated with colon resection alone were technically successful. Our results confirm the safety and effectiveness of non-ERCP BAE in patients with surgically altered GI tract anatomy in both antegrade and retrograde approaches.
Enteroscopy has been developed for endoscopic mucosal inspection and treatment of the small intestine. The BAE facilitates deeper evaluation of small intestine with a specialized overtube device [3, 15]. The grip-and-pull technique, in which the balloon on the tip of the overtube grips the intestinal wall and the examiner pulls both the endoscope and the overtube while holding the intestine, enables intestinal pleating over the overtube and shortening of the length to allow insertion of the endoscope deeper into the intestine in normal bowel anatomy [13, 16]. However, in surgically altered GI tract, the small intestine is more difficult to inspect via BAE due to tortuosity, postoperative peritoneal adhesions, or anastomotic strictures [17]. Nevertheless, BAE is frequently indicated for surgically altered anatomy due to the increased frequency of anastomotic stenosis, bleeding, or small bowel perforation in the operated intestine [10]. Also, capsule endoscopy is usually not indicated for surgically altered anatomy because of the high risk of retention and the inability to examine excluded portions of the small bowel [18].
The technical success rate of all 80 antegrade and retrograde BAEs in patients with surgically altered GI tract anatomy was as high as 86.2%, which is comparable to the rates of 83–92% reported in previous studies [9, 11, 18]. However, the previous studies only included 9 to 57 non-ERCP BAEs. Further, the retrograde BAEs were ranged between 4 and 7 examinations [9, 11]. The high technical success rate of BAE persisted even in altered GI tract anatomy that affected the insertion route based on the analysis of a number of antegrade and retrograde examinations. Antegrade BAE in Roux-en-Y anatomy was associated with a technical success rate of 77.8%. Because Y-branching of the small bowel prevented access via conventional endoscopy, various types of endoscopy have been attempted to reach the afferent limb in Roux-en-Y anatomy [19, 20]. BAE is the preferred option for this difficult anatomy and associated with high technical success, which is consistent with the results of our study [18, 21]. Retrograde BAE in colon resection anatomy showed a technical success rate of 100%, probably because the colon is larger in diameter than small intestine and colonic stenosis is rare even after colectomy.
Diagnostic and therapeutic yields were as high as 80% in our study, consistent with the results of previous studies. Most of the related studies reported that the diagnostic yield of BAE in surgically altered GI tract anatomy was comparable to the diagnostic yield of BAEs in normal anatomy [9, 11, 18]. In studies investigating BAE in normal anatomy, the diagnostic yield ranged from 50 to 80% for DBE and from 58 to 65% for SBE [22,23,24,25,26,27]. Diagnostic yield might vary according to the indication. In a study involving more than 2000 DBEs, the diagnostic yield was greater than 80% in patients with Peutz–Jeghers syndrome and less than 20% in patients with abdominal pain or diarrhea [28]. Also in our study, the diagnosis of internal obstruction and polyposis was relatively easy due to clear endoscopic findings associated with higher diagnostic yield, but low when the indication was abdominal pain.
The present study has some limitations. First, because the study populations were limited to Korean, procedures such as bariatric surgery performed in the West were not included. In case of bariatric surgery, Roux-en-Y gastric bypass was mostly performed, which may be associated with a low technical success rate and diagnostic and therapeutic yields [12, 29, 30]. Second, although our study was a multicenter study consisting of two tertiary academic hospitals, each hospital used only one type of endoscope, either DBE or SBE. Therefore, comparison based on the endoscope type could be biased. Third, due to the retrospective nature of this study, whether or not the small bowel was thoroughly observed was judged based on the electronic medical record. We defined the success of the examination when the examiner achieved any pertinent finding or performed appropriate endoscopic treatment after they succeeded to insert the scope at the area of interest.
In conclusion, non-ERCP BAE is effective and safe with a high technical success rate in patients with surgically altered GI tract anatomy, which is demonstrated in both antegrade and retrograde approaches. Despite differences depending on the indication, non-ERCP BAE is associated with a sufficiently high diagnostic yield and provides the intended therapy regardless of the type of therapeutic intervention. Further prospective studies on the effectiveness and safety of BAE according to the diverse types of surgical anastomosis are needed.Please note that the references are renumbered to ensure sequential ordering.OK. Thank you.
References
Yamamoto H, Sekine Y, Sato Y et al. Total enteroscopy with a nonsurgical steerable double-balloon method. Gastrointestinal Endoscopy. 2001;53:216–220.
May A. How to approach the small bowel with flexible enteroscopy. Gastroenterol Clin North Am. 2010;39:797–806.
Morita Y, Bamba S, Inatomi O et al. Prototype single-balloon enteroscopy with passive bending and high force transmission improves depth of insertion in the small intestine. Intest Res. 2020;18:229–237.
Gerson LB, Tokar J, Chiorean M et al. Complications associated with double balloon enteroscopy at nine US centers. Clin Gastroenterol Hepatol. 2009;7:1177–1182, 1182.e1171–1173.
Haber GB. Double balloon endoscopy for pancreatic and biliary access in altered anatomy (with videos). Gastrointest Endosc. 2007;66:S47-50.
Neumann H, Fry LC, Meyer F, Malfertheiner P, Mönkemüller K. Endoscopic Retrograde Cholangiopancreatography Using the Single Balloon Enteroscope Technique in Patients with Roux-en-Y Anastomosis. Digestion. 2009;80:52–57.
Azeem N, Tabibian JH, Baron TH et al. Use of a single-balloon enteroscope compared with variable-stiffness colonoscopes for endoscopic retrograde cholangiography in liver transplant patients with Roux-en-Y biliary anastomosis. Gastrointestinal Endoscopy. 2013;77:568–577.
Skinner M, Popa D, Neumann H, Wilcox CM, Mönkemüller K. ERCP with the overtube-assisted enteroscopy technique: a systematic review. Endoscopy. 2014;46:560–572.
Patel MK, Horsley-Silva JL, Gomez V, Stauffer JA, Stark ME, Lukens FJ. Double balloon enteroscopy procedure in patients with surgically altered bowel anatomy: analysis of a large prospectively collected database. J Laparoendosc Adv Surg Tech A. 2013;23:409–413.
Skinner M, Peter S, Wilcox CM, Mönkemüller K. Diagnostic and therapeutic utility of double-balloon enteroscopy for obscure GI bleeding in patients with surgically altered upper GI anatomy. Gastrointest Endosc. 2014;80:181–186.
Kurzynske FC, Romagnuolo J, Brock AS. Success of single-balloon enteroscopy in patients with surgically altered anatomy. Gastrointest Endosc. 2015;82:319–324.
Cai JX, Diehl DL, Kiesslich R et al. A multicenter experience of through-the-scope balloon-assisted enteroscopy in surgically altered gastrointestinal anatomy. Surg Endosc. 2017;31:2753–2762.
Committee AT, Chauhan SS, Manfredi MA et al. Enteroscopy. Gastrointest Endosc. 2015;82:975–990.
Prachayakul V, Deesomsak M, Aswakul P, Leelakusolvong S. The utility of single-balloon enteroscopy for the diagnosis and management of small bowel disorders according to their clinical manifestations: a retrospective review. BMC Gastroenterol. 2013;13:103.
Yamamoto H, Ogata H, Matsumoto T et al. Clinical Practice Guideline for Enteroscopy. Dig Endosc. 2017;29:519–546.
Lo SK, Yamamoto H. How we do deep enteroscopy. Gastrointest Endosc. 2021;94:452–456.
Shimatani M, Takaoka M, Matsushita M, Okazaki K. Endoscopic approaches for pancreatobiliary diseases in patients with altered gastrointestinal anatomy. Dig Endosc. 2014;26:70–78.
Moreels TG, Hubens GJ, Ysebaert DK, Op de Beeck B, Pelckmans PA. Diagnostic and Therapeutic Double-Balloon Enteroscopy after Small Bowel Roux-en-Y Reconstructive Surgery. Digestion. 2009;80:141–147.
Hintze RE, Adler A, Veltzke W, Abou-Rebyeh H. Endoscopic access to the papilla of Vater for endoscopic retrograde cholangiopancreatography in patients with Billroth II or Roux-en-Y gastrojejunostomy. Endoscopy. 1997;29:69–73.
Elton E, Hanson BL, Qaseem T, Howell DA. Diagnostic and therapeutic ERCP using an enteroscope and a pediatric colonoscope in long-limb surgical bypass patients. Gastrointest Endosc. 1998;47:62–67.
Chua TJ, Kaffes AJ. Balloon-assisted enteroscopy in patients with surgically altered anatomy: a liver transplant center experience (with video). Gastrointest Endosc. 2012;76:887–891.
Heine GDN, Hadithi M, Groenen MJM, Kuipers EJ, Jacobs MAJM, Mulder CJJ. Double-Balloon Enteroscopy: Indications, Diagnostic Yield, and Complications in a Series of 275 Patients with Suspected Small-Bowel Disease. Endoscopy. 2006;38:42–48.
Di Caro S, May A, Heine DGN et al. The European experience with double-balloon enteroscopy: indications, methodology, safety, and clinical impact. Gastrointestinal Endoscopy. 2005;62:545–550.
Yamamoto H, Kita H, Sunada K et al. Clinical outcomes of double-balloon endoscopy for the diagnosis and treatment of small-intestinal diseases. Clinical Gastroenterology and Hepatology. 2004;2:1010–1016.
Upchurch BR, Sanaka MR, Lopez AR, Vargo JJ. The clinical utility of single-balloon enteroscopy: a single-center experience of 172 procedures. Gastrointestinal Endoscopy. 2010;71:1218–1223.
Ramchandani M, Reddy DN, Gupta R et al. Diagnostic yield and therapeutic impact of single-balloon enteroscopy: Series of 106 cases. Journal of Gastroenterology and Hepatology. 2009;24:1631–1638.
Takano N, Yamada A, Watabe H et al. Single-balloon versus double-balloon endoscopy for achieving total enteroscopy: a randomized, controlled trial. Gastrointestinal Endoscopy. 2011;73:734–739.
Moschler O, May A, Muller MK, Ell C, German DBESG. Complications in and performance of double-balloon enteroscopy (DBE): results from a large prospective DBE database in Germany. Endoscopy. 2011;43:484–489.
Bukhari M, Kowalski T, Nieto J et al. An international, multicenter, comparative trial of EUS-guided gastrogastrostomy-assisted ERCP versus enteroscopy-assisted ERCP in patients with Roux-en-Y gastric bypass anatomy. Gastrointest Endosc. 2018;88:486–494.
Choi EK, Chiorean MV, Coté GA et al. ERCP via gastrostomy vs. double balloon enteroscopy in patients with prior bariatric Roux-en-Y gastric bypass surgery. Surg Endosc. 2013;27:2894–2899.
Funding
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science & ICT (NRF-2018M3A9E8021507) and also supported by the Soonchunhyang University Research Fund.
Author information
Authors and Affiliations
Contributions
Study concept and design: JHS, SRJ, HHL. Data acquisition: JHS, SRJ, JSK, B-IL, J-OK. Data analysis and interpretation: JHS, HHL. Drafting of the manuscript: JHS, HHL. Critical revision of the manuscript for important intellectual content: SRJ, HHL. Statistical analysis: HHL. Obtained funding: SRJ, HHL. Overall project administration and study supervision: HHL.
Corresponding author
Ethics declarations
Conflict of interest
Song JH, Kim JS, Lee BI, Kim JO have no conflicts to declare. Lee HH was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science & ICT (NRF-2018M3A9E8021507). Jeon SR was supported by grant from Soonchunhyang University Research Fund.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Song, J.H., Jeon, S.R., Kim, J.S. et al. Performance of Balloon-Assisted Enteroscopy for Non-ERCP Indications in Patients with Surgically Altered Gastrointestinal Anatomy. Dig Dis Sci 68, 2545–2552 (2023). https://doi.org/10.1007/s10620-023-07854-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-023-07854-z