
Abstract
Background
Data regarding hospitalization outcomes in patients with inflammatory bowel disease (IBD) with respect to hospital teaching status are largely unknown.
Aims
We aimed to investigate the impact of hospital teaching status on IBD hospitalization outcomes.
Methods
In this retrospective analysis, we queried the 2016 and 2017 National Inpatient Sample (NIS) databases using the International Classification of Diseases 10th revision (ICD-10) coding system. All adult patients with a principal diagnosis of IBD were included. We stratified the IBD group into ulcerative colitis (UC), Crohn’s disease (CD), and complicated IBD. Our primary outcome was mortality. Statistical analysis was performed using STATA, version 16.0.
Results
Of the 189,950 adult patients with IBD, the majority were admitted to teaching hospitals (70.9%). There was no significant difference in mortality based upon hospital teaching status (aOR 1.18, p = 0.48); however, these patients had an increased mean length of stay (adjusted coefficient: 0.82, p < 0.01), charges (adjusted coefficient: $8732, p < 0.01), and costs ($2871, p < 0.01). On subgroup analysis, patients with UC admitted to teaching hospitals had a significantly increased in-hospital mortality (aOR 2.11, p < 0.05), while those admitted with CD did not (aOR 0.80, p = 0.4). Among patients with complicated IBD, 73.17% were admitted to teaching hospitals, and no significant difference in in-hospital mortality was seen (aOR 1.06, p = 0.8).
Conclusion
While outcome differences are likely related to multiple unaccounted factors, greater efforts should be placed to cost-effectively manage patients with IBD at teaching institutions. Future studies are warranted to fully comprehend these variations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The US health care system revolves around two major hospital systems: teaching hospitals—generally large academic medical centers and non-teaching hospitals—generally smaller community hospitals [1]. Traditionally, teaching hospitals have served an instrumental role in providing quality medical education, promoting new research, leading innovations, and delivering quality care for underprivileged individuals. On the other spectrum, community hospitals fill in the void and serve a vast majority (roughly 80%) of all hospitalizations and patient care [2]. Teaching hospitals are excluded from some insurance networks as they are considered to be more expensive compared to non-teaching hospitals, with the rationale that comparable quality of care is delivered at both [3]. This presumption, however, may not be entirely accurate as a recent study showed some evidence that the overall mortality for common conditions was indeed lower in teaching hospitals compared to non-teaching hospitals [1].
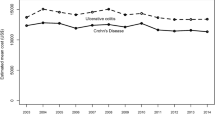
Inflammatory bowel disease (IBD) poses a significant health care burden, which from an economic perspective is particularly true for hospitalized patients with IBD. Indeed, a nationwide analysis using the National Inpatient Sample (NIS) database from 2003 to 2014 estimated a mean charge of $11,345 and $13,412 for hospitalized patients with Crohn’s disease (CD) and ulcerative colitis (UC), respectively [4]. The rising cost of hospitalization in patients with IBD is dictated by the severity, associated complications, and type of intervention used [5]. As such, the current priority to deliver health care is not only focused toward improving disease outcomes but also efficient and cost-effective care.
Data regarding the hospitalization outcomes of patients with IBD with respect to hospital teaching status (teaching versus non-teaching) are largely unknown. In this setting, we attempted to investigate the impact of hospital teaching status on IBD hospitalization outcomes. We hypothesized that while the length of stay and/or costs may be greater for patients with IBD admitted to teaching hospitals, no significant mortality or clinical outcome difference will be detected in these patients, despite the increased complexity of IBD cases seen at teaching hospitals.
Methods
Data Source
In this retrospective cohort study, we queried the 2016 and 2017 National Inpatient Sample (NIS) databases. The NIS is a database of inpatient hospital stays, excluding rehabilitation and long-term acute care hospitals, derived from billing data submitted by hospitals to statewide organizations, based off discharge abstracts. The NIS 2016 database contains data from 7.1 million hospital stays in 4575 hospitals in 47 US states, while the NIS 2017 database contains data from 7.1 million hospital stays in 4584 hospitals in 48 US states. They contain de-identified clinical and non-clinical elements at both the patient level and hospital level all using the International Classification of Diseases 10th revision, Clinical Modification (ICD-10-CM) coding system. As we used the combination of the NIS 2016 and NIS 2017 databases (the two newest databases), we obtained updated and more specific ICD-10-CM codes and were able to analyze an increased total number of cases/patients.
Study Population
Adult patients (above the age of 18) with a principal diagnosis of IBD were included in the study. We stratified the IBD group into UC, CD, and complicated IBD. Complicated IBD as defined by the ICD-10-CM diagnostic code corresponds to IBD complicated by either a fistula, bleed, obstruction, or abscess. The ICD-10-CM diagnostic and procedural codes used in this study are presented in the Supplementary Appendix (Supplementary Tables 1, 2). Inclusion and exclusion criteria are shown below in a flow diagram (Fig. 1). Institutional Review Board approval was not required for this study as it was performed using de-identified and nationally available data.

Patient inclusion and exclusion flow diagram
Study Variables
Patient demographics were age, sex, race (Caucasian, Black, Hispanic, Asian, Pacific Islander, Native American, and other), median household income (based on patient’s zip code), primary expected payer (Medicare, Medicaid, private insurance, and uninsured), hospital bed size (small, medium, and large), teaching status, hospital region (Northeast, Midwest, South, and West), and urban location. Burden of comorbidities was assessed using Charlson comorbidity index.
Study Outcomes
The primary outcome was in-hospital all-cause mortality. Secondary outcomes were: (a) mean LOS, (b) mean hospitalization charges (the amount billed by the hospital for the rendered services) and (actual) costs, (c) incidence of shock, (d) incidence of sepsis, (e) incidence of acute kidney injury (AKI), (f) incidence of Intensive Care Unit (ICU) admission, (g) likelihood of discharge to home (as opposed to an acute or sub-acute rehabilitation facility), (h) incidence of total parenteral nutrition (TPN), and (i) incidence of gastrointestinal (small and large bowel) surgery. All outcomes were defined using standard ICD-10 diagnostic and procedural codes as shown in the Supplementary Appendix (Supplementary Table 1).
Statistical Analysis
Statistical analysis was performed using STATA, version 16.0 (StataCorp., College Station, Texas, USA). This software facilitates analysis to produce nationally representative unbiased results, variance estimates, and p values. Weighting of patient-level observations was implemented. Multivariate regression analysis was used to adjust for potential confounders. Univariate analysis was initially performed to calculate unadjusted odds ratio and determine confounders significantly associated with the outcomes. Significant association was determined with a cutoff p value of 0.2. Multivariate regression model was then built by including all confounders that were found to be significant by univariate analysis, to calculate adjusted odds ratio. Logistic regression was used for binary outcomes and linear regression was used for continuous outcomes. Proportions were compared using the Fisher exact test, and continuous variables were compared using the Student t test. All p values were two-sided, with 0.05 as threshold for statistical significance. Non-teaching hospitals outcomes were taken as reference when looking at differences in outcomes.
Results
Patient and Hospital Characteristics
A total of 189,950 adult patients with a diagnosis of IBD were included in the final analysis. Mean age was 45.14 years, and majority of patients were female (53.21%). Private insurance was the primary payer of the patients (48.33%). Majority of patients were white (73.23%). They were predominantly admitted to teaching hospitals (70.9%). 94,680 (49.84%) patients had complicated IBD, and 95,270 (50.16%) patients had uncomplicated IBD. 73.17% of all patients with complicated IBD were admitted to teaching hospitals, while 68.77% of all patients with uncomplicated IBD were admitted to non-teaching hospitals. The complete patient and hospital characteristics are presented in the accompanying Tables 1 and 2.
All-Cause In-Hospital Mortality
The total all-cause in-hospital mortality was 0.28% (545 out of 189,950 admissions) in patients admitted with IBD. The mortality rate in patients admitted to teaching hospitals was 0.28%, compared to 0.29% in patients admitted to non-teaching hospitals. There was no significant difference in mortality for patients admitted to non-teaching hospitals compared to patients admitted to teaching hospitals (aOR 1.18, p = 0.48) (Fig. 2).

In-hospital outcomes in patients with inflammatory bowel disease (IBD)
Length of Stay
The overall mean length of stay (LOS) was 4.97 (4.90–5.03) days for all patients admitted with IBD. In patients admitted to teaching hospitals, the mean LOS was 5.23 days, compared to 4.34 days in patients admitted to non-teaching hospitals. After multivariate analysis, patients admitted to teaching hospitals had a significantly longer mean LOS compared to patients admitted to non-teaching hospitals (adjusted coefficient: 0.82, p < 0.05) (Table 3).
Mean Hospitalization Charges and Costs
The mean hospitalization charges and cost for patients admitted with IBD were $47,237 and $11,844, respectively. In patients admitted to teaching hospitals, the mean charges and costs were $50,667 and $12,711 compared to $38,919 and $9740 in patients admitted to non-teaching hospitals, respectively. After multivariate analysis, patients admitted to teaching hospitals had significantly higher hospitalization charges and costs compared to patients admitted to non-teaching hospitals (adjusted coefficient: $8732, p < 0.05 and $2871, p < 0.05, respectively) (Table 3).
Shock
The overall incidence of shock was 0.76% (1460 out of 189,950) in all patients admitted with IBD. Patients admitted to teaching hospitals with IBD had a 0.79% incidence of shock compared to 0.71% in patients with IBD admitted to non-teaching hospitals. There was no significant difference in the likelihood of shock in patients admitted to teaching hospitals compared to those admitted to non-teaching hospitals (aOR 1.15, p = 0.35) (Fig. 2).
Sepsis
The overall incidence of sepsis was 2.01% (3825 out of 189,950 patients) in all patients admitted with IBD. Patients admitted to teaching hospitals had a 2.06% incidence of sepsis compared to 1.87% in patients admitted to non-teaching hospitals. There was no significant difference in the likelihood of developing sepsis for patients admitted to teaching hospitals compared to those admitted to non-teaching hospitals (aOR 1.10, p = 0.35) (Fig. 2).
Acute Kidney Injury
The overall incidence of AKI in patients admitted with IBD was 7.39% (14,045 out of 189,950 patients). Patients admitted to teaching hospitals had a 7.21% incidence of AKI, compared to 7.8% in patients admitted to non-teaching hospitals. On multivariate analysis, there was no significant difference in likelihood of AKI for patients admitted to teaching hospitals compared to those admitted to non-teaching hospitals (aOR 0.98, p = 0.81) (Fig. 2).
ICU Admission
The total incidence of ICU admission in patients admitted with IBD was 0.52% (995 out of 189,950). Patients admitted to teaching hospitals with IBD had a 0.55% incidence of ICU admission compared to 0.45% in patients with IBD admitted to non-teaching hospitals. There was no significant difference in the likelihood of ICU admission in patients with IBD admitted to teaching hospitals compared to patients with IBD admitted to non-teaching hospitals (aOR 1.16, p = 0.40) (Fig. 2).
Intra-abdominal Surgery
Among all patients with IBD, the overall incidence of some form of intra-abdominal/gastrointestinal surgery during admission was 9.84% (18,710 out of 189,950). 12.11% of all patients with IBD admitted to teaching hospitals had surgery, while only 4.3% of patients admitted to non-teaching hospitals had surgery. Upon multivariate analysis, patients with IBD admitted to teaching hospitals had a significantly higher likelihood of undergoing intra-abdominal/gastrointestinal surgery than patients admitted to non-teaching hospitals. (aOR 2.97, p < 0.05) (Fig. 2).
Total Parenteral Nutrition
Among patients with IBD, the total incidence of TPN use during hospitalization was 3.32% (6320 out of 189,950 patients). 3.93% of patients admitted to teaching hospitals with IBD required TPN, while only 1.84% of patients admitted to non-teaching hospitals with IBD required TPN. Upon multivariate analysis, patients with IBD admitted to teaching hospitals had a significantly higher likelihood of requiring TPN than patients admitted to non-teaching hospitals (aOR 2.04, p < 0.05) (Fig. 2).
Home Discharge
Among patients with IBD, the total incidence of discharge to home (as opposed to a rehabilitation facility) after hospitalization was 82.77% (157,225 out of 189,950 patients). 110,735 (82.14%) of patients admitted to teaching hospitals with IBD were discharged home, while 46,490 (84.31%) of patients admitted to non-teaching hospitals with IBD were discharged home. Upon multivariate analysis, patients with IBD admitted to teaching hospitals had a significantly lower likelihood of being discharged home than patients admitted to non-teaching hospitals. (aOR 0.76, p < 0.01) (Table 3).
Subgroup Analysis (UC Alone, CD Alone, and Complicated IBD)
UC Alone
In patients with UC, there was a significantly increased in-hospital mortality for patients admitted to teaching hospitals (aOR 2.11, p < 0.05). Additionally, there was a significantly higher mean charge (adjusted coeff: $13,711, p < 0.05), mean cost (adjusted coeff: $3300, p < 0.05), and mean LOS (1.02 days, p < 0.05) for these patients. They also had an increased likelihood of surgery (aOR 5.13, p < 0.05), TPN use (aOR 1.94, p < 0.05), and ICU admission (aOR 1.81 p < 0.05), compared to those admitted to non-teaching hospitals. There was no significant difference in likelihood of shock (aOR 1.38, p = 0.12), sepsis (aOR 1.17, p = 0.24), or AKI (aOR 1.02, p = 0.73) (Table 4 and Fig. 3).

In-hospital outcomes in patients with ulcerative colitis (UC) only
CD Alone
In contrast to patients with UC, patients with CD admitted to teaching hospitals did not have a significant difference in in-hospital mortality (aOR 0.80, p = 0.4). However, patients with CD admitted to teaching hospitals had significantly higher mean charges (adjusted coeff: $11,305, p < 0.05), mean costs (adjusted coeff: $2546, p < 0.05), and mean LOS (0.89 days, p < 0.05). They also had an increased likelihood of surgery (aOR 2.18, p < 0.05) and TPN use (aOR 2.07, p < 0.05) compared to patients with IBD admitted to non-teaching hospitals. There was no significant difference in likelihood of shock (aOR 1.13, p = 0.51), sepsis (aOR 1.07, p = 0.5), AKI (aOR 1.06, p = 0.3), or ICU admission (aOR 0.98, p = 0.92) (Table 4 and Fig. 4).

In-hospital outcomes in patients with Crohn’s disease (CD) only
Complicated IBD
Patients with complicated IBD (as defined by the ICD-10 codes) admitted to teaching hospitals did not have a significant difference in in-hospital mortality during admission compared to those admitted to non-teaching hospitals (aOR 1.06, p = 0.8). However, those admitted to teaching hospitals had significantly higher mean charges (adjusted coeff: $12,126, p < 0.05), mean costs (adjusted coeff: $2928, p < 0.05), and mean LOS (0.97 days, p < 0.05). Moreover, they had an increased likelihood of surgery (aOR 2.11, p < 0.05) and TPN use (aOR 1.86, p < 0.05). There was no significant difference in likelihood of shock (aOR 0.96, p = 0.8), sepsis (aOR 1.26, p = 0.10), AKI (aOR 1.01, p = 0.87), or ICU admission (aOR 0.98, p = 0.9) (Table 3 and Fig. 5).

In-hospital outcomes in patients with complicated inflammatory bowel disease (IBD) only
Discussion
In this retrospective study examining a national database, we identified nearly 200,000 patients with IBD and compared their outcomes based upon the hospital teaching status. Patients with IBD treated at teaching hospitals were more likely to be male, have private insurance, and be treated at urban centers than patients treated at non-teaching hospitals. We identified significant differences between teaching and non-teaching hospitals, as admission to a teaching hospital was associated with an increased LOS as well as increased hospitalization charges and costs relative to non-teaching hospitals. Patients admitted to teaching hospitals were also nearly twice as likely to receive blood transfusions or TPN and approximately three-times more likely to undergo surgery. Despite these differences, in-hospital mortality was not significantly different between teaching and non-teaching hospitals for the IBD population as a whole. However, in-hospital mortality for UC patients was roughly twice as much at teaching hospitals relative to non-teaching hospitals. UC patients treated at teaching hospitals were also approximately twice as likely to be admitted to ICUs and five-times as likely to undergo surgery. In addition to this, over 70% of all patients with complicated IBD were admitted to teaching hospitals, yet this did not translate into a significant difference in in-hospital mortality between teaching and non-teaching hospitals.
It is unclear why teaching status was associated with increased mortality for UC patients but not for patients with CD or complicated IBD. Outcome differences may be related to the increased likelihood of surgery (three-times more likely) at teaching hospitals. Additionally, the increased need for surgery may be hinged on the fact that patients in need of surgery at non-teaching hospitals are referred and/or transferred to teaching hospitals specifically for this reason. A recent database study examining outcomes at teaching and non-teaching hospitals for patients with IBD also noted increased in-hospital mortality for UC patients at teaching hospitals; however, these results did not persist in multivariate analysis [6]. However, these data are contrary to results from other similar studies, many of which identified lower overall mortality for various conditions at teaching hospitals [1, 7]. Notably, in a study looking at myocardial infarction survival at teaching and non-teaching hospitals, patient transfers were found to be an unmeasured source of confounding [7]. Hence, a similar effect may be at play concerning UC patients at teaching hospitals. Moreover, as with patients requiring surgery, other significant interventions, such as TPN, may be offered more readily at teaching hospitals, thus attributing to its increased likelihood among patients with IBD at these hospitals. It has also been noted that, in the case of stroke, teaching hospitals may disproportionately treat patients with more severe disease, potentially confounding the associated stroke mortality metrics [8, 9]. Coding and/or disease severity differences may influence the apparent mortality difference concerning UC noted in this study. In addition, some residual confounding for clinical features is not well captured by variables in the database. However, if a true association between teaching status and mortality among UC patients exists, physician education programs, including targeted didactics and guest lectures, may help improve such metrics.
Perhaps our finding that patients with IBD admitted to teaching hospitals were less likely to be discharged home (as opposed to a rehabilitation facility) was because more careful and thoughtful planning was established. Indeed, multiple studies have established reduced post-discharge mortality among teaching hospitals compared to non-teaching hospitals for acute myocardial infarction, congestive heart failure, and pneumonia [1, 7, 10].
Economic differences were noted between teaching and non-teaching hospitals with teaching hospitals charging and costing approximately $9000 and $3000 more than non-teaching hospitals. These results are contrary to a similar recent analysis, which found no significant differences in price between teaching and non-teaching hospitals for IBD [6]. This same analysis noted disease severity to be a greater influencing measure on price than teaching status. However, costs and charges may be driven by the increased interventions (surgery, TPN use, etc.) provided at teaching hospitals. Indeed, in a study looking at hospitalization costs in patients with UC, increased costs were found to be due to surgery (colectomy) and biologic (infliximab) use [11]. In addition, some studies have suggested teaching hospitals tend to code less aggressively than non-teaching hospitals, thus being penalized under administrative risk-adjusted quality metrics [1]. Despite this, our study merits further evaluation for the need to place a greater emphasis on proper budgeting/improve allocation resources to potentially mitigate higher hospital costs for teaching hospitals.
This study is limited by several factors. The inability to assess patient transfers between teaching and non-teaching hospitals may have unduly influenced outcomes in ways we could not account for. In addition, institutions which had dedicated IBD centers perhaps fared better than the average teaching hospital, thus acting as a source of confounding. Furthermore, while we utilized the Charlson comorbidity index to describe certain patient demographics, we were unable to delineate among specific comorbidities, which may also disproportionately influence outcomes. To further circumvent outcomes being skewed, we utilized univariate and multivariate regression analysis to adjust for potential confounders.
Despite these limitations, our study was powered by a large sample size, the multitude of institutions included, and the numerous outcomes analyzed, hence accurately representing hospital outcomes from the nationwide patient population.
In conclusion, while we did not find significant differences concerning primary outcomes between teaching and non-teaching hospitals, we did find increased mortality among UC patients treated at teaching hospitals. Moreover, we identified increased health care utilization required by teaching hospitals for patients with both complicated and non-complicated IBD. These data are consistent with the current, albeit limited, literature on the topic. Greater delineation concerning specific patient- and institutional-level factors, particularly in the case of UC, may help to understand the underlying cause of these results. In addition, large prospective studies comparing hospitalization outcomes in teaching and non-teaching hospitals, with and without dedicated IBD centers, should be encouraged to fully comprehend the variation of hospitalization outcomes in patients with IBD.
References
Burke LG, Frakt AB, Khullar D, et al. Association between teaching status and mortality in US hospitals. JAMA. 2017; 317: 2105–2113. 05/24/2017. https://doi.org/10.1001/jama.2017.5702.
Fleishon HB, Itri JN, Boland GW, et al. Academic medical centers and community hospitals integration: trends and strategies. J Am Coll Radiol. 2017; 14: 45–51. 11/07/2016. https://doi.org/10.1016/j.jacr.2016.07.006.
Haeder SF, Weimer DL and Mukamel DB. Narrow networks and the affordable care act. JAMA. 2015; 314: 669–670. 06/26/2015. https://doi.org/10.1001/jama.2015.6807.
Xu F, Liu Y, Wheaton AG, et al. Trends and factors associated with hospitalization costs for inflammatory bowel disease in the United States. Appl Health Econ Health Policy. 2019; 17: 77–91. 09/28/2018. https://doi.org/10.1007/s40258-018-0432-4.
Park KT, Ehrlich OG, Allen JI, et al. The cost of inflammatory bowel disease: an initiative from the Crohn’s & Colitis foundation. Inflamm Bowel Dis. 2020; 26: 1–10. 05/22/2019. https://doi.org/10.1093/ibd/izz104.
Dalal RS, Vajravelu RK, Lewis JD, et al. Hospitalization outcomes for inflammatory bowel disease in teaching vs nonteaching hospitals. Inflamm Bowel Dis. 2019; 25: 1974-1982. 05/01/2019. https://doi.org/10.1093/ibd/izz089.
Navathe AS, Silber JH, Zhu J, et al. Does admission to a teaching hospital affect acute myocardial infarction survival? Acad Med. 2013; 88: 475-482. 02/22/2013. https://doi.org/10.1097/acm.0b013e3182858673.
Fonarow GC, Alberts MJ, Broderick JP, et al. Stroke outcomes measures must be appropriately risk adjusted to ensure quality care of patients: a presidential advisory from the American Heart Association/American Stroke Association. Stroke. 2014; 45: 1589–1601. 02/14/2014. https://doi.org/10.1161/str.0000000000000014.
Fonarow GC, Pan W, Saver JL, et al. Comparison of 30-day mortality models for profiling hospital performance in acute ischemic stroke with vs without adjustment for stroke severity. JAMA. 2012; 308: 257–264. 07/17/2012. https://doi.org/10.1001/jama.2012.7870.
Drye EE, Normand SL, Wang Y, et al. Comparison of hospital risk-standardized mortality rates calculated by using in-hospital and 30-day models: an observational study with implications for hospital profiling. Ann Intern Med. 2012; 156: 19–26. 01/04/2012. https://doi.org/10.7326/0003-4819-156-1-201201030-00004.
Coward S, Heitman SJ, Clement F, et al. Ulcerative colitis-associated hospitalization costs: a population-based study. Can J Gastroenterol Hepatol. 2015; 29: 357–362. 06/17/2015. https://doi.org/10.1155/2015/627370.
Author information
Authors and Affiliations
Contributions
SS, SW, TIM, and MA assisted with data acquisition, analyses, and manuscript preparation. AA, IV, AN, ZK, MA, AK, and AS drafted and critically revised the manuscript. AN and MS provided input regarding methodology. AN, MS, and AS provided direct supervision and guidance. SS is the article guarantor. All authors agree to the final version of this manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
None to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sharma, S., Weissman, S., Mehta, T.I. et al. Role of Hospital Teaching Status on Outcomes of Patients with Inflammatory Bowel Disease: A Nationwide Analysis. Dig Dis Sci 66, 2216–2226 (2021). https://doi.org/10.1007/s10620-020-06497-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-020-06497-8