
Abstract
Background
Endoscopic retrograde cholangiopancreatography (ERCP) in patients with Roux-en-Y anastomosis is a complex challenge. Long length of afferent limb after an acute angle at the jejunojejunostomy and altered location of the biliary orifice make biliary cannulation difficult. Single balloon enteroscopy assisted ERCP (SBE-ERCP) is a promising alternative to conventional approaches.
Aim
The purpose of this study was to assess the efficacy and safety of SBE-ERCP in patients with Roux-en-Y reconstruction at a high volume tertiary referral center.
Methods
This is a retrospective cohort study. All procedures were performed by a single, experienced pancreatobiliary endoscopist. Patient demographics and related clinical data were obtained. The rate of procedure successes and complications were determined.
Results
Fourteen patients (nine women) with a median age of 63 years (range 35–83 years) underwent 22 SBE-ERCP procedures from March 2009 to May 2011. Surgically altered anatomy consisted of Whipple procedure (n = 4), hepaticojejunostomy (n = 9) and partial gastrectomy (n = 1). Indications for SBE-ERCP were obstructive jaundice (n = 10), cholangitis (n = 7), post-PTC internalization (n = 3) and biliary stent extraction/exchange (n = 2). The hepaticojejunostomy site (HJS) was reached in 15 (68 %) procedures. Successful interventions were performed in 11 (73 %) of 15 cases, including balloon dilation of biliary strictures (n = 3), insertion of biliary stents (n = 7), retrieval of biliopancreatic stents (n = 4) and biliary stone extraction (n = 4). The mean procedural time for successful interventions was 97.6 min (range 73–147 min). No procedural complications occurred during the median follow-up of 501 days (range 22–1,242 days).
Conclusion
SBE-ERCP is safe and carries an acceptable success rate in experienced hands.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is a well recognized intervention for the management of pancreatobiliary disorders. The overall success rate of selective bile duct cannulation was reported around 90 % from a prospective study [1]. However, biliary cannulation failure can occur in patients with surgically altered anatomy, particularly in patients with Roux-en-Y entero-enteric anastomosis. These patients have complicated gastrointestinal anatomy, particularly a long afferent limb length after an acute angle at the jejunojejunostomy. The difficulty of traversing this region and the altered location of the hepaticojejunostomy site (HJS) make selective bile duct cannulation difficult.
Since successful application of double balloon enteroscopy (DBE) for the diagnosis and treatment of small bowel diseases was well recognized, the emerging role of DBE assisted ERCP for patients with postsurgical anatomy has been reported [2–8]. However, DBE requires specialized expertise that is not widely available. Single-balloon enteroscopy (SBE) is a unique technique that uses a single-balloon splinting overtube to sequentially reduce and pleat small bowel, which enables negotiation of the acute angulations sometimes found at gastroenteric or enteroenteric anastomoses [9]. Since an initial case series reported the feasibility of SBE assisted ERCP (SBE-ERCP) [10], SBE-ERCP has been introduced as an alternative method for replacing conventional approaches such as a side viewing enteroscope, forward viewing push-enteroscope, (pediatric) colonoscope or percutaneous transhepatic cholangiography (PTC). The aim of this study was to assess the efficacy and safety of SBE-ERCP in patients with Roux-en-Y anastomosis at a high volume tertiary referral center.
Method
Patients
After the study was approved by our institutional review board, we retrospectively reviewed consecutive patients with surgically altered anatomy who had undergone SBE-ERCP in a single tertiary care center between March 2009 and May 2011. Data were extracted from the electrical medical record and gastrointestinal endoscopy database. The data included patient demographics, indications for procedure, diagnostic imaging studies, endoscopic findings and therapies, and procedural complications. All the patients included in this study were initially attempted using a pediatric colonoscope. Since all the patients had Roux-en-Y anastomosis, a side-viewing scope was not attempted. Patients with surgically altered anatomy who had previously had successful ERCP with a colonoscope were excluded. All the patients provided a written informed consent prior to the procedures.
SBE-ERCP Techniques
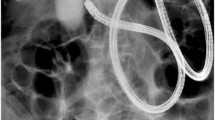
All procedures were performed by a well-experienced pancreatobiliary endoscopist (G.A.) under monitored anesthesia care. ERCP was performed with a 200-cm length SBE system (SIF Q180; Olympus America, Inc., Center Valley, PA, USA) along with an overtube with a balloon at its distal end designed specifically to facilitate deep endoscope insertion [11]. The enteroscope was advanced using a push and pull technique, with sequential inflation and deflation of a balloon (Fig. 1). The endoscopy system was inserted as far as possible in a deflated position, the balloon was inflated, and the entire system was withdrawn to promote backloading of the small bowel onto the outer surface of the overtube. The enteroscope was then advanced while the balloon was inflated, holding the proximal small bowel in the retracted position. Fluoroscopy was used in all cases to guide passage of an enteroscope to HJS and to perform ERCP. Selective common bile duct (CBD) cannulation was performed using a commercially available catheter (Cunningham-Cotton Sleeve; Cook Medical, Inc. Bloomington, IN, USA) to allow variable angulation for the biliary cannulation, bow to enter a biliary orifice [12]. Endoscopic accessories for SBE-ERCP were all commercially available. For the purpose of internalization of percutaneous biliary access, the tip of wire was grabbed using a snare and the wire was pulled via a working channel of the endoscope. In order to dilate a focal stricture or correct choledocholithiasis, a 9–12 mm diameter balloon catheter (Quantum TTC Biliary Balloon Dilators; Cook Medical, Inc. Bloomington, IN, USA) was inserted over the guide-wire. We then inserted biliary stents with 5–10 Fr fluorinated-ethylene-propylene endoprostheses (Cook Medical, Inc. Bloomington, IN, USA) or 8–12 mm non-covered or fully-covered metallic stents (Boston Scientific Corp., Natick, MA, USA). Prophylactic antibiotics were administered prior to the procedures in all cases. No patients received NSAIDs, anti-platelet agents or antithrombotic medications.

a Jejuno-jejuno anastomosis was encountered. b Afferent limb cannulation and the enteroscope advanced to the hepaticojejunostomy site. c Cholangiogram showed filling defects. d Stone and sludge were successfully extracted
Complications
Bleeding, infection and perforation were assessed as procedure-related complications. All patients were assessed immediately following their procedures and after discharge from the hospital. The first telephone contact was made a month after the SBE-ERCP in all cases. Bleeding was considered a complication when it required therapeutic intervention at the time of procedure or when it was discovered later based on a drop in hemoglobin >2 gm/dl that required blood transfusion or hospitalization. Cholangitis or pancreatitis was defined as an increase in liver function tests or pancreatic enzymes with associated clinical signs. Unless immediately recognized at the time of procedure, any suspicion for perforation required confirmation by the presence of free air on imaging studies. Endoscopic complications were scored as previously defined [13].
Definition of Endoscopic Treatment Outcome
Success rates of reaching the HJS, cannulating the biliary tract, and completing the therapeutic procedure were our outcome measures. Total procedure time was defined as the time from the beginning of insertion of a scope in patient’s mouth to the complete withdrawal of a scope from patient’s mouth. Follow-up data was collected from out-patient clinic charts, hospital records, and telephone contact with patients.
Results
A total of 22 SBE-ERCP procedures were performed in 14 patients (nine women) with a median age of 63 years (range 35–83 years; Table 1). Twelve patients (86 %) had previous diagnosis of gastrointestinal neoplasm (cholangiocarcinoma [n = 5], pancreas [n = 4], gastrointestinal stromal tumor [n = 1], gastric carcinoid tumor [n = 1] and duodenal leiomyosarcoma [n = 1]). The other two patients underwent resection of an extrahepatic bile duct for benign biliary obstruction. All patients underwent prior surgical interventions with Roux-en-Y reconstruction. Surgically altered anatomy consisted of Whipple procedure (n = 4) and hepaticojejunostomy (n = 9). One patient had undergone a partial gastrectomy which was reconstructed by gastrojejunostomy and Roux-en-Y jejunojejunostomy. The indications for SBE-ERCP procedures were obstructive jaundice (n = 10), cholangitis (n = 7), post-PTC internalization (n = 3) and biliary stent extraction/exchange (n = 2). HJS was reached in 15 (68 %) of 22 procedures. The reasons for failure of HJS detection were excessive looping of endoscope (n = 2), marked sharp intra-luminal angulation (n = 2), inability to identify despite excessive effort (n = 2) and complete malignant luminal obstruction (n = 1). Four procedures had a previous sphincterotomy. Native major papilla was found in two patients and no successful cannulation was performed in the native papilla. Therapeutic SBE-ERCP was attempted in all cases in which the HJS was reached. Out of 15 cases in which HJS was detected, successful therapeutic interventions were completed in 11 (73 %) cases. These interventions included balloon dilation of biliary strictures (n = 3), insertion of biliary stents (n = 7), retrieval of biliopancreatic stents (n = 4) and biliary stone extraction (n = 4). The mean procedural time for all attempted and successful procedures were 85.3 min (range 42–147 min) and 97.6 min (range 73–147 min), respectively. In one of four failed intervention cases, a tight stricture led to successful deep biliary cannulation but failed passage of a device for intervention. In another case, cannulation was impossible because of tumor ingrowth in the biliary tract. In the other two cases, deep cannulation was unsuccessful because of altered anatomy. All of the failed SBE-ERCP cases were successfully managed by PTC with biliary drainage (n = 7), conservative medical management (n = 3) and surgical exploration with choledochoduodenostomy, choledochoscopy and biliary stone removal (n = 1). No major acute or late procedural complications occurred during median follow-up of 501 days (range 22–1,242 days).
Discussion
Based on our relatively low success rate of biliary cannulation in patients with altered anatomy using a standard enteroscope or colonoscope, SBE-ERCP was the initial modality used in this study cohort. In the cohort of patients in whom therapeutic ERCP was indicated, we achieved 73 % successful completion in cases in which the HJS was reached. ERCP was ultimately successful in half of total attempted procedures. The major limitation in unsuccessful cases was inability to pass an endoscope or device due to altered anatomy or malignant luminal obstruction/stricture. There were no major complications related to the procedure despite prolonged procedure times.
In the current era, with a growing prevalence of Roux-en-Y gastrointestinal reconstruction for gastric bypass surgery, pancreaticobiliary surgery (pancreaticoduodenectomy, hepaticojejunostomy or choledochojejunostomy), or liver transplantation, ERCP in patients with Roux-en-Y anastomosis is more frequently required. The anatomy following a Roux-en-Y procedure (long limb that must be traversed and acute angle at the jejunojejunostomy to enter the afferent limb) presents a particular challenge when attempting to access HJS by means of standard duodenoscope. Alternative approaches have been reported using a colonoscope or a balloon assisted enteroscope.
Since the first report of ERCP in Roux-en-Y limb using colonoscope [14], this method has been commonly attempted as an alternative to the conventional duodenoscope [15, 16]. Difficulty advancing the colonoscope in a long afferent limb could be overcome by similar techniques used for colonoscopy, including alternating advancement and withdrawal of the endoscope with straightening of loops, turning the patient to the left-lateral or supine position, and manual palpation and compression of the abdomen. The study by Wright et al. [16] reported a total of 25 ERCP procedures in 15 patients with Roux-en-Y anastomosis and intact papilla using the colonoscope to explore biliary orifice and place a guidewire in the afferent limb over which duodenoscope was then passed to complete biliary interventions. They reported success in reaching the native papilla in 10 of 15 patients (67 %) and 19 of 25 procedures (76 %) with average procedure time of 137 min (range 50–225 min). It is noted that because of oblique view of native papilla, it was very difficult to cannulate or perform advanced techniques with colonoscope. In these cases, cannulation was possible by means of forward-viewing endoscopes in only two cases.
Balloon assisted enteroscopy has been implemented to perform ERCP in patients with Roux-en-Y reconstructive surgery. The balloon-loaded overtube is of value in assisting the enteroscope to proceed further into the surgically altered long limb by straightening the enteroscope into a short position. DBE became commercially available earlier than SBE and more experiences with DBE-ERCP have been reported [2, 3, 6–8]. When using DBE-ERCP for Roux-en-Y anatomy, successful rates of reaching the biliary orifice or cannulating the biliary tracts have been reported between 74 and 93 % or 85–100 %, respectively, with mean duration time of 40–111 min. Following two small case series showing feasibility of SBE-ERCP in patients with Roux-en-Y anastomosis [17, 18], three studies have demonstrated the utility of this modality for patients with surgically altered anatomy [19–21]. Saleem et al. [21] presented the largest experience and illustrated technical feasibility of SBE-ERCP in patients with Roux-en-Y anastomosis. Out of 56 procedures in 50 patients (15 gastric bypass surgery with Roux-en-Y), successful rates of reaching or cannulation of bile duct have been reported 75 % (42/56) or 70 % (39/56, 93 % of the cases in which biliary orifice was reached), respectively, with a mean procedure time of 78 min.
Because of the variability of patient demographics, it is difficult to compare the present study to the previous three studies, even to the study by Saleem et al., in which only Roux-en-Y reconstructions were included. The first two studies by Itoi et al. [19] and Wang et al. [20] included patients with Billroth II reconstruction and the latest study by Saleem et al. [21] included patients who underwent gastric bypass surgery with Roux-en-Y anastomosis. The length of afferent limb in Billroth II gastrectomy performed decades ago for peptic ulcer disease or other gastric pathology is likely shorter than that of gastric bypass surgery with Roux-en-Y anastomosis. Saleem et al. [21] reported that diagnostic success in patients with Roux-en-Y hepaticojejunostomy or choledochojejunostomy was 78 % and they did not report the rate of therapeutic success in those patients. It remains uncertain in this study whether those procedures were performed by a single person or more than one endoscopist.
Our study is unique in that we looked at a specific cohort of patients who had undergone Roux-en-Y reconstructive surgery and procedures were performed by a single operator. Our experience suggested a positive learning curve. Between the first and the last half of procedures, the success rate of reaching biliary orifice and cannulating the biliary tract were 55 % (6/11 in the first half) compared to 73 % (8/11 in the last half), and 36 % (4/11 in the first half) compared to 73 % (8/11 in the last half), respectively. Procedure times (min) were 90.9 and 79.6, respectively. In the last half of procedures, there was only one case in which reaching HJS was successful but biliary cannulation failed, and the reason for failure was tumor infiltration. No prior reports on SBE-ERCP mentioned learning curve. Our study may imply that there is a possible positive learning curve when performing the SBE-ERCP for patients with surgically altered anatomy.
To date, no conclusive data has been published to compare the usefulness between SBE-ERCP and DBE-ERCP for pancreatobiliary diseases. Disadvantages of DBE-ERCP are that it requires preparation of an additional balloon at the tip of scope and management of a two-balloon system. As mentioned in the study by Itoi et al. [19], it is possible to misjudge which balloon be inflated or deflated during procedures, which could potentially lead to procedural delay. On the other hand, in cases of sharp luminal angulation, a balloon on the tip of DBE is advantageous in traversing such angulations over the hook shape of SBE scope [22]. A case series by Moreels et al. [23] has reported four patients with Roux-en-Y anastomosis who underwent both DBE-ERCP and SBE-ERCP for biliary interventions. They mentioned that an additional balloon at the tip of the enteroscope was not a prerequisite for procedures and showed an equal efficacy of DBE and SBE in therapeutic ERCP. The study, however, concluded that the number of patients was too small to clearly recommend one balloon-assisted ERCP over the other. As another alternative, spiral overtube-assisted ERCP has recently been reported to be feasible and safe [24, 25]. However the device has not been commercially available and comparative studies have yet to be published. More recently, laparoscopic assisted ERCP (LA-ERCP) in bariatric post Roux-en-Y gastric bypass have shown its usefulness [26, 27]. The study by Schreiner et al. [27] reported that LA-ERCP resulted in superior outcomes in patients with a Roux limb length of 150 cm or longer. Overall, procedural results were favorable in comparison to LA-ERCP in terms of biliary orifice identification, cannulation rate, and therapeutic success. The disadvantage of LA-ERCP is its cost. The procedure required general anesthesia, laparoscopic surgeons, and an operating room, which all contributed to a greater cost for the procedure. A potentially longer postprocedural hospital stay following LA-ERCP also may influence the overall cost. In our study, general anesthesia was not required for all procedures. To determine the optimal endoscopic method for the management of postoperative pancreatobliary pathology, more comparative studies are warranted.
Our study has limitations. First, we had no cases of gastric bypass surgery with Roux-en-Y reconstruction. The afferent limb in Roux-en-Y gastric bypass surgery is usually longer than that in pancreaticobiliary surgery, which could favorably affect the success rate of reaching HJS. Second, given the high prevalence of underlying gastrointestinal neoplasms in our cohort, one patient’s HJS could not be reached due to complete malignant luminal obstruction. In the other two patients, biliary intervention was unsuccessful after reaching the HJS secondary to tight post-surgical biliary stricture or complete malignant occlusion of HJS due to tumor invasion. Third, we included patients who required endoscopic internalizations (Rendezvous procedure) (n = 3) after PTC drainage and patients who underwent SBE-ERCP for biliary stent extraction/exchange (n = 2). Those patients had a landmark for delineating the HJS or bile duct. Lastly, we had only one patient who still had a native papilla. Despite these limitations, our experience supported the previous studies that SBE-ERCP may be performed with great success by experienced hands.
In conclusion, we have yet to discover the gold-standard endoscopic modality for therapeutic pancreatobiliary interventions in patients with surgical altered anatomy. Though SBE-ERCP is complex and time-consuming, it is useful, safe and carries an acceptable success rate in an experienced hand.
References
Suissa A, Yassin K, Lavy A, et al. Outcome and early complications of ERCP: a prospective single center study. Hepatogastroenterology. 2005;52:352–355.
Emmett DS, Mallat DB. Double-balloon ERCP in patients who have undergone Roux-en-Y surgery: a case series. Gastrointest Endosc. 2007;66:1038–1041.
Aabakken L, Bretthauer M, Line PD. Double-balloon enteroscopy for endoscopic retrograde cholangiography in patients with a Roux-en-Y anastomosis. Endoscopy. 2007;39:1068–1071.
Mönkemüller K, Bellutti M, Neumann H, et al. Therapeutic ERCP with the double-balloon enteroscope in patients with Roux-en-Y anastomosis. Gastrointest Endosc. 2008;67:992–996.
Koornstra JJ. Double balloon enteroscopy for endoscopic retrograde cholangiopancreaticography after Roux-en-Y reconstruction: case series and review of the literature. Neth J Med. 2008;66:275–279.
Moreels TG, Hubens GJ, Ysebaert DK, et al. Diagnostic and therapeutic double-balloon enteroscopy after small bowel Roux-en-Y reconstructive surgery. Digestion. 2009;80:141–147.
Parlak E, Ciçek B, Dişibeyaz S, et al. Endoscopic retrograde cholangiography by double balloon enteroscopy in patients with Roux-en-Y hepaticojejunostomy. Surg Endosc. 2010;24:466–470.
Raithel M, Dormann H, Naegel A, et al. Double-balloon-enteroscopy-based endoscopic retrograde cholangiopancreatography in post-surgical patients. World J Gastroenterol. 2011;17:2302–2314.
Koornstra JJ, Fry L, Mönkemüller K. ERCP with the balloon-assisted enteroscopy technique: a systematic review. Dig Dis. 2008;26:324–329.
Neumann H, Fry LC, Meyer F, et al. Endoscopic retrograde cholangiopancreatography using the single balloon enteroscope technique in patients with Roux-en-Y anastomosis. Digestion. 2009;80:52–57.
ASGE Technology Committee. Overtube use in gastrointestinal endoscopy. Gastrointest Endosc. 2009;70:828–834.
Rossos PG, Kortan P, Haber G. Selective common bile duct cannulation can be simplified by the use of a standard papillotome. Gastrointest Endosc. 1993;39:67–69.
Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:383–393.
Gostout CJ, Bender CE. Cholangiopancreatography, sphincterotomy, and common duct stone removal via Roux-en-Y limb enteroscopy. Gastroenterology. 1988;95:156–163.
Elton E, Hanson BL, Qaseem T, et al. Diagnostic and therapeutic ERCP using an enteroscope and a pediatric colonoscope in long-limb surgical bypass patients. Gastrointest Endosc. 1998;47:62–67.
Wright BE, Cass OW, Freeman ML. ERCP in patients with long-limb Roux-en-Y gastrojejunostomy and intact papilla. Gastrointest Endosc. 2002;56:225–232.
Mönkemüller K, Fry LC, Bellutti M, et al. ERCP using single-balloon instead of double-balloon enteroscopy in patients with Roux-en-Y anastomosis. Endoscopy. 2008;40:E19–E20.
Dellon ES, Kohn GP, Morgan DR, et al. Endoscopic retrograde cholangiopancreatography with single-balloon enteroscopy is feasible in patients with a prior Roux-en-Y anastomosis. Dig Dis Sci. 2009;54:1798–1803.
Itoi T, Ishii K, Sofuni A, et al. Single-balloon enteroscopy-assisted ERCP in patients with Billroth II gastrectomy or Roux-en-Y anastomosis. Am J Gastroenterol. 2010;105:93–99.
Wang AY, Sauer BG, Behm BW, et al. Single-balloon enteroscopy effectively enables diagnostic and therapeutic retrograde cholangiography in patients with surgically altered anatomy. Gastrointest Endosc. 2010;71:641–649.
Saleem A, Baron TH, Gostout CJ, et al. Endoscopic retrograde cholangiopancreatography using a single-balloon enteroscope in patients with altered Roux-en-Y anatomy. Endoscopy. 2010;42:656–660.
Tsujikawa T, Saitoh Y, Andoh A, et al. Novel single-balloon enteroscopy for diagnosis and treatment of the small intestine: preliminary experiences. Endoscopy. 2008;40:11–15.
Moreels TG, Pelckmans PA. Comparison between double-balloon and single-balloon enteroscopy in therapeutic ERC after Roux-en-Y entero-enteric anastomosis. World J Gastrointest Endosc. 2010;2:314–317.
Lennon AM, Kapoor S, Khashab M, et al. Spiral assisted ERCP is equivalent to single balloon assisted ERCP in patients with Roux-en-Y anatomy. Dig Dis Sci. 2012;57:1391–1398.
Kogure H, Watabe H, Yamada A, et al. Spiral enteroscopy for therapeutic ERCP in patients with surgically altered anatomy: actual technique and review of the literature. J Hepatobiliary Pancreat Sci. 2011;18:375–379.
Saleem A, Levy MJ, Petersen BT, et al. Laparoscopic assisted ERCP in Roux-en-Y gastric bypass (RYGB) surgery patients. J Gastrointest Surg. 2012;16:203–208.
Schreiner MA, Chang L, Gluck M, et al. Laparoscopy-assisted versus balloon enteroscopy-assisted ERCP in bariatric post-Roux-en-Y gastric bypass patients. Gastrointest Endosc. 2012;75:748–756.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tomizawa, Y., Sullivan, C.T. & Gelrud, A. Single Balloon Enteroscopy (SBE) Assisted Therapeutic Endoscopic Retrograde Cholangiopancreatography (ERCP) in Patients with Roux-en-Y Anastomosis. Dig Dis Sci 59, 465–470 (2014). https://doi.org/10.1007/s10620-013-2916-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-013-2916-2