
Abstract
Azithromycin (AZI) is a macrolide antibiotic that improves lung function in lung transplant recipients (LTx). Gastroesophageal reflux (GER) has been implicated in the pathogenesis of chronic rejection after LTx. Macrolide antibiotics may affect GER by modifying esophageal and gastric motility. The purpose of this study was to evaluate the effect of AZI on GER and gastric aspiration after LTx. Acid and weakly acidic GER was measured with 24-h pH-impedance monitoring in 47 LTx patients (12 patients “on” AZI). Gastric aspiration was assessed in a separate group of 30 LTx patients before and after AZI by measurements of pepsin and bile acid in bronchoalveolar lavage fluid (BALF). Patients “on” AZI had a significant lower total number of reflux events [41 (30–61) vs. 22.5 (7–37.5)], number of acid reflux events [24 (16–41) vs. 8 (4–18)], esophageal acid exposure [2.9% (0.7–7.3) vs. 0.2% (0.1–2.0)], bolus exposure [0.73% (0.5–1.4) vs. 0.21% (0.12–0.92)], and proximal extent of reflux [14 (9–24) vs. 5 (2–7)]. AZI reduced the concentration of bile acids in BALF without affecting levels of pepsin. LTx patients “on” AZI have less GER and bile acids aspiration. This effect might be due to enhanced esophageal motility and accelerated gastric emptying.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastroesophageal reflux (GER) has been implicated in the pathophysiology of chronic respiratory diseases including chronic cough [1, 2], cystic fibrosis [3, 4], and asthma [5, 6]. Furthermore, increased GER is common after lung transplantation (LTx) and might contribute to the development of chronic rejection or bronchiolitis obliterans syndrome (BOS) [7–10]. Recent studies using impedance-pH monitoring suggest that not only acid but also weakly acidic reflux might be deleterious for these patients [4, 7].
The effect of GER treatment on the evolution of respiratory diseases is uncertain. Drugs that inhibit gastric acid secretion (PPI and H2 blockers) are commonly used, empirically, in spite of controversial results of controlled clinical trials showing poor to moderate effects. Acid suppression in children with asthma and GERD did not improve asthma symptoms or lung function [11]. However, adult asthmatic patients with GERD symptoms improved significant their lung function after antireflux therapy [12, 13]. Reflux related chronic cough improved after 8 weeks of treatment with omeprazole [14]. Antireflux surgery has been used in chronic cough [15, 16] and patients with CF [17] and more recently, antireflux surgery was proposed to prevent development of BOS after LTx [18–20]. Prokinetic drugs like cisapride, domperidone, and metoclopramide can improve esophageal motility and accelerate gastric emptying [21–24] and have been used either alone or in combination with PPI for the treatment of GER. Although esophageal and gastric hypomotility could be common in GER-related respiratory disorders [25, 26], little is known about the effect of prokinetic drugs in these patients [27–29]. Macrolide antibiotics, like erythromycin, have a significant prokinetic effect and have also been proposed for the treatment of GERD [29–31].
Lung transplant patients have been successfully treated with azithromycin (AZI), an azalide antibiotic of the macrolide family [32–34]. The main mechanism of action of AZI in these patients is thought to be an immunomodulatory effect [35]. AZI activates motilin receptors and provokes in vitro GI smooth muscle contraction (Prof Dr I. Depoortere K.U. Leuven, unpublished data). The effect of AZI on esophageal motility and gastric emptying in humans is unknown. We hypothesize that AZI might affect GI motility and reduce GER in LTx recipients.
The aim of this study is to assess the effect of AZI on gastroesophageal reflux (acid and weakly acidic) and aspiration of gastric contents in lung transplant recipients.
Methods
Subjects
Studies were performed in 77 lung transplant patients. We included patients either without BOS or with BOS 0p. According to criteria established by the International Society of Heart and Lung Transplantation [36] a potential-BOS stage (BOS 0p) is a condition with a decline in lung function defined by a 10–19% decrease in FEV1 and/or by a 25% decrease in FEF25-75 from baseline. The study was approved by the Ethics Committee of the University Hospital Gasthuisberg, K.U. Leuven.
The Effect of AZI on GER and Aspiration Was Evaluated in Two Patient Populations
In a cross-sectional study we compared the prevalence of GER between a group of LTx patients not receiving AZI (n = 35) and another group of patients receiving AZI (n = 12). In a separate cohort study (n = 30), we evaluated the prevalence of aspiration in LTx patients before and after administration of AZI. The LTx patients studied with impedance-pH monitoring (reflux monitoring) were recruited consecutively over a period of 2 years. The BAL samples used to assess bile and pepsin aspiration in the cohort study were obtained before and after AZI from consecutive stable patients over a period of 3 years. BALF samples post AZI were obtained 116 (37–233) days after the start of AZI treatment. In both studies, Azithromycin (250 mg, three times a week) was added to the current immunosuppressive drug regimen as an empiric treatment in the prevention of the development of BOS. The immunosuppressive drug regimen was comprised of cyclosporine (trough levels 200–270 ng/ml) or tacrolimus (trough levels 8–12 ng/ml), azathioprine (1–2 mg/h/day, adjusted to leukocyte count) or mycophenolate (trough levels 2–4 mg/ml) and methylprednisolone (<8 mg/day). All patients were studied “off” antireflux treatment with PPI or H2 blockers (at least 1 week).
The demographic and clinical characteristics of both patient populations are listed in Table 1.
We compared the levels of pepsin and bile acids in BALF obtained from LTx patients included in the cohort study with measurements on BALF from 14 “non-transplant” patients requiring bronchoscopy (11 lung cancer, two COPD, and one lymphoma).
24-h Impedance-pH Monitoring
Gastroesophageal reflux was assessed using ambulatory 24-h esophageal impedance-pH monitoring. Esophageal impedance-pH was recorded with a 2.1-mm-diameter catheter that comprised six electrode pairs to measure intraluminal impedance and two antimony pH sensors (Sandhill Scientific, Inc; Highlands Ranch, CO, USA). The catheter was passed transnasally and positioned to record the pH in the stomach and the pH and impedance in the esophageal body. Esophageal pH was measured at 5 cm and impedance at 3, 5, 7, 9, 15, and 17 cm proximal to the lower esophageal sphincter (LES). The impedance-pH catheter was connected to an ambulatory device containing the amplifiers (Sleuth, Sandhill Scientific, Inc; Highlands Ranch, CO, USA). The impedance amplifier delivered ultra-low current in a range of 1–2 kHz with resulting current flow variations in response to intraluminal impedance changes. The impedance and pH signals were digitized at 50 Hz and stored in the data logger. Before the start of the recording, the pH electrodes were calibrated using pH 4.0 and pH 7.0 buffer solutions. Patients were asked to remain upright during the day, and lie down only at their usual bedtime. Event markers on the data logger recorded meal times and posture changes. Between meals, patients abstained from snacks, beverages with a pH < 5, and were asked to avoid lozenges and gum chewing. Before the study, patients were instructed to keep a careful diary and trained to use a dedicated event marker in the data logger.
The impedance-pH recording was independently analyzed for GER using criteria described in a recent consensus report [37]. Several reflux indices were measured: acid exposure, number of acid and weakly acidic reflux events, volume exposure and proximal extent of reflux.
Total 24-h esophageal acid exposure was calculated as the percentage of time that the esophageal pH was below 4 and was considered increased if >4.5% of the recording time.
Individual reflux events, detected by impedance, were counted and classified according to the corresponding pH change as acid, weakly acidic or weakly alkaline. A gastroesophageal reflux event was defined as a sequential orally progressing drop in impedance to less than 50% of the baseline values starting distally (3 cm above LES) and propagating retrograde to at least the next two more proximal measuring segments. Reflux was classified as acid if pH fell below 4 for at least 4 s or, if pH was already below 4, as a decrease of at least 1 pH unit sustained for more than 4 s. Weakly acidic reflux was defined as a pH drop of at least 1 pH unit sustained for more than 4 s with the basal pH remaining above pH 4. The number of reflux events were regarded as increased if above the 95th percentile of normal data obtained in healthy subjects [38].
For each reflux episode detected by impedance, the volume exposure at 5 cm above LES was calculated as the time (s) between the 50% drop in impedance until the 50% recovery of the impedance baseline. Total volume exposure/24 h was obtained by addition of volume exposure of all individual reflux events. The volume exposure was regarded as increased if above the 95th percentile of data obtained in healthy subjects [38].
The proximal extent of reflux was evaluated from the impedance tracings and expressed as total number of reflux episodes reaching 15 cm above the LES.
Detection of Aspiration Markers
BALF samples were obtained during routine bronchoscopy. BALF was performed by wedging the bronchoscope into a subsegmental bronchus of the right middle lobe or lingula, by instilling two aliquots of 50 ml and subsequently recovering the fluid by gentle manual suction. Presence of pepsin and bile acids was determined in each BALF sample, before and after azithromycin treatment.
Pepsin was measured using an enzyme-linked immunosorbent assay (ELISA). BALF samples were first incubated with a primary polyclonal antibody to porcine pepsin (dilution 1:5000). Thereafter they were incubated with a secondary antibody (IgG from gout) labeled with horseradish peroxidase (dilution 1:10000). Tetramethylbenzidine was added and the color change was measured using a spectrophotometer. Pepsin concentration in BALF was determined based on a reference standard of serial dilutions of porcine pepsin. The specificity of this ELISA assay was verified using Western blot immunoassay. The lowest level of accurate detection was 1 ng/ml.
Bile acid determination was performed using a commercially available enzymatic assay (Bioquant, San Diego, USA). The lowest level of accurate detection allowed by this technique was 0.2 μmol/l.
Statistical Analysis
Statistical analyses were performed using the PRISM 4.0 (GraphPad) statistical software. Deviations from Gaussian distribution were tested using the Kolmogorov-Smirnov test. If the data did not have a Gaussian distribution, we performed a non-parametric test. Comparison between groups was done using an unpaired or paired t-test. All data are presented as median (25th–75th percentile) unless otherwise stated. A P-value of <0.05 was considered statistically significant.
Results
Cross-Sectional Study: Effect of AZI on Gastroesophageal Reflux
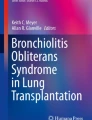
Lung transplant patients with AZI treatment had less gastroesophageal reflux compared to those patients without AZI therapy. The number of total reflux events [41(30–61) vs. 22.5(7–37.5)], acid reflux events [24(16–41) vs. 8(4–18)], nocturnal reflux events [5(2–9) vs. 0(0–5)], the ratio acid/non-acidic reflux [1.8 (1.28–2.94) vs. 0.61 (0.35–1.92)], the esophageal acid exposure [2.9% (0.7–7.3) vs. 0.2% (0.1–2.0)] and esophageal volume exposure [0.73% (0.5–1.4) vs. 0.21% (0.12–0.92)] (as measured with impedance) were significantly lower in patients “on” AZI. The proximal extent of reflux was lower in patients “on” AZI. The median number of reflux episodes reaching 15 cm above the LES was 14 (9–24) “off” AZI vs. 5 (2–7) “on” AZI; P = 0.0086. The percentage of total reflux reaching the proximal esophagus was lower “on” AZI [40% (28–53) vs. 28.6% (21–59); but this difference did not reach statistical significance [P = 0.42] (Table 2; Fig. 1).

Effect of AZI on proximal extent of GER. a Examples of reflux events detected by impedance-pH monitoring with low proximal extent (left) and high proximal extent (right). b AZI significantly reduced the number of proximal reflux events (≥15 cm)
Cohort Study: Effect of AZI on Aspiration
BALF from non-transplant controls showed no bile acids and pepsin levels with concentration of 23.83 ng/ml (0–25 ng/ml). Bile acids were positive in BAL of 15/30 patients pre AZI treatment and in 9/30 patients during AZI treatment (Fig. 2, left). After the start of AZI treatment, most of the LTx patients (28/30) included in this study had pepsin present in their BALF. Pepsin levels were higher in LTx patients compared to controls. AZI did not reduce the concentration of pepsin in BALF. Before AZI [160 ng/ml (10–379) vs. 259 ng/ml (71–594) after AZI therapy (NS). In contrast, bile acid levels in BALF were significantly reduced after AZI treatment [0.43 μM (0–2.29) vs. 0.0 μM (0–1.19)] P = 0.0106 (Fig. 2).

The concentration of bile acids in BALF was significantly reduced after azithromycin treatment [0.43 μM (0–2.29) vs. 0.0 μM (0–1.19)] P = 0.0106
Discussion
Azithromycin (AZI) is a macrolide antibiotic that improves the lung function in a subgroup of lung transplant recipients (LTx) with bronchiolitis obliterans syndrome (BOS). Gastroesophageal reflux (GER) has been implicated in the pathogenesis of BOS. Macrolide antibiotics, such as erythromycin or AZI, may affect GER by modifying esophageal and gastric motility. The aim of this study was to evaluate the effect of AZI on GER and aspiration of gastric contents in LTx recipients.
The main findings of this study were: (1) LTx patients with AZI treatment had less gastroesophageal reflux (number of reflux events, volume exposure, proximal extent, and acidity) compared to LTx recipients without AZI (2) bile acid levels in BALF, a marker of aspiration of gastric contents, was significantly reduced after AZI treatment.
AZI, a macrolide antibiotic, has a proven beneficial effect on the clinical outcome of different respiratory disorders such as diffuse panbronchiolitis [39] and cystic fibrosis [40]. Azithromycin improves lung function (FEV1) in some patients with bronchiolitis obliterans syndrome (BOS) after lung transplantation (LTx) and this improvement has been attributed to an immunomodulatory effect [32–34, 41].
Recent studies suggest that increased gastroesophageal reflux might be relevant in the evolution of patients after LTx. Several studies showed that LTx patients have a high prevalence of GER and aspiration of gastric contents (pepsin and bile acids) [7–10, 42–45]. Moreover, patients with bile acids in BALF had a higher risk of developing bronchiolitis obliterans syndrome [7].
The cause of increased gastroesophageal reflux and aspiration after LTx is uncertain. Possible factors include delayed gastric emptying, abnormal lower esophageal sphincter and/or crural diaphragm function, or impaired esophageal body motility. All these factors can promote reflux of large volume and proximal extent with the subsequent risk of aspiration. Treatment of increased GER is usually attempted with medication to reduce acid and gastric volume (PPI) and antireflux surgery has been proposed for these patients [19, 20, 46].
Prokinetic drugs have been used for treatment of GERD either alone or in combination with PPI or H2 Blockers. Macrolide antibiotics, such as erythromycin have a significant prokinetic effect on esophageal and gastric motility via activation of the motilin receptor [47]. However, the clinical effectiveness of macrolides for the treatment of chronic GERD has been hampered by the rapid loss of prokinetic activity due to desensitization of the motilin receptor [48]. AZI is a macrolide antibiotic with similar in vitro prokinetic effects compared to that observed with erythromycin (I. Depoortere, unpublished data).
We hypothesized that the clear beneficial effect of azithromycin in LTx patients is mainly due to its anti-inflammatory properties but might be further potentiated by its an anti-reflux effect due to its prokinetic properties on esophageal and gastric motility.
To test the effect of AZI on GER, we used the most sensitive technique available for reflux detection: impedance-pH monitoring. In this way, we could detect not only acid but also non-acidic reflux events [49]. However, we found a reduction in the total number of reflux events (acid and non-acid) and nocturnal reflux events induced by AZI. The mechanism by which AZI reduced the number of reflux events is unknown. Macrolides increase LES pressure but they don’t have a significant effect on the number of TLESRs. A reduction in acid reflux events was more pronounced than the reduction in non-acid reflux, resulting in a significantly reduced ratio acid/non-acid reflux as well as a significantly reduced esophageal acid exposure by AZI treatment. The higher impact of AZI on acid reflux might suggest that azithromycin is able to induce a change in gastric acid secretion and/or distribution of acid within the stomach. It is known that erythromycin can reduce gastric acid secretion [50–52]. Recent studies have shown that the acidity of refluxates is determined by the presence of an “acid pocket” in the area immediately distal to the lower esophageal sphincter [53] and Bisschops et al. [54] have shown that ERY can modify the location and the extent of the acid pocket. Based on the ERY studies, we speculate that AZI might have reduced gastric acid secretion or modify the characteristics of the “acid pocket” in our LTx patients.
We observed that patients “on” AZI had significantly lower esophageal volume exposure and proximal extent of reflux. Both parameters are indirect markers of reflux volume. It is plausible that AZI accelerated gastric emptying and thereby reduced gastric volume available for reflux. Sifrim et al. showed that AZI can increase postprandial gastric motility. Postprandial gastric contractions were found to originate higher up in the stomach in healthy volunteers after intake of AZI, suggesting a faster clearance of the proximal stomach [55].
Theoretically, a reduction in bolus exposure and proximal extent of reflux should result in a lower risk for aspiration in these patients. Previous studies showed that most LTx patients have pepsin in their BALF, indicating that aspiration after LTx is very common [7, 56]. Furthermore, other markers of aspiration have been identified in BALF of LTx patients. i.e., bile acids which were shown to be more important than pepsin in predicting the development of BOS [7, 42, 43, 57]. Aspiration of gastric contents might induce an inflammatory reaction in the lower airways resulting in chronic rejection [33].
In our study, half of the patients had bile acids present in the BALF before AZI treatment, confirming previous published data [7, 42]. AZI significantly reduced the concentration of bile acids in BALF without affecting the concentration of pepsin. We speculate that AZI on the one hand reduces gastric volume and modifies fundic acid distribution, and on the other hand it reduces duodeno-pancreatic contents in the stomach. Koek et al. [58] showed that erythromycin can improve the clearance of duodeno-gastric reflux (DGR) from the stomach in healthy volunteers and in patients with pathological DGR [59]. A reducing effect of AZI on the amount of duodenal contents might account for the selective reduction of bile acids in BALF.
Unlike the short-lasting prokinetic effect of ERY, the effect of AZI on reflux parameters was found several months after start of treatment. The explanation for this finding is not clear. One possibility to explain the long-lasting effect of AZI and absence of receptor’s desensitization is the treatment regime (low intermittent doses). However, in vitro studies are needed to further characterize the kinetic properties of AZI on GI smooth muscle.
AZI mainly reduced acid reflux and bile acids in BALF with less pronounced effect on weakly acidic reflux and pepsin. It is unknown whether such an effect can be sufficient to prevent a deleterious impact of reflux in LTx patients. It is known that patients “on” PPI, still have weakly acidic and weakly alkaline GER and aspiration of such refluxate may still induce graft dysfunction in these patients. Theoretically, antireflux surgery might be a more complete treatment option for GER in lung transplant recipients. Fundoplication has been shown to improve lung function and to prolong freedom from BOS after LTx [9, 20, 46]. However, anti-reflux surgery remains an invasive procedure and additional controlled studies on the effect of AZI on GER and prevention of BOS are warranted.
In conclusion, this study demonstrated that LTx patients “on” azithromycin have less gastroesophageal reflux and aspiration of bile acids.
References
Irwin RS, Corrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis. 1981;123(4 Pt 1):413–417.
Sifrim D, Dupont L, Blondeau K, Zhang X, Tack J, Janssens J. Weakly acidic reflux in patients with chronic unexplained cough during 24-hour pressure, pH, and impedance monitoring. Gut. 2005;54(4):449–454. doi:10.1136/gut.2004.055418.
Feigelson J, Sauvegrain J. Letter: Gastro-esophageal reflux in mucoviscidosis. Nouv Presse Med. 1975;4(38):2729–2730.
Blondeau K, Dupont L, Mertens V, Verleden G, Malfroot A, Vandenplas Y, Hauser B, Sifrim D. Gastroesophageal reflux and aspiration of gastric contents in adult patients with cystic fibrosis. Gut. 2008;57:1049–1055.
Rosztoczy A, Makk L, Izbeki F, Roka R, Somfay A, Wittmann T. Asthma and gastroesophageal reflux: clinical evaluation of esophago-bronchial reflex and proximal reflux. Digestion. 2008;77(3–4):218–224. doi:10.1159/000146083.
Harding SM. The potential role of gastroesophageal reflux in asthma. Minerva Gastroenterol Dietol. 2001;47(2):75–83.
Blondeau K, Mertens V, Vanaudenaerde BA, et al. Gastro-oesophageal reflux and gastric aspiration in lung transplant patients with or without chronic rejection. Eur Respir J. 2008;31(4):707–713. doi:10.1183/09031936.00064807.
D’Ovidio F, Keshavjee S. Gastroesophageal reflux and lung transplantation. Dis Esophagus. 2006;19(5):315–320. doi:10.1111/j.1442-2050.2006.00603.x.
Palmer SM, Miralles AP, Howell DN, Brazer SR, Tapson VF, Davis RD. Gastroesophageal reflux as a reversible cause of allograft dysfunction after lung transplantation. Chest. 2000;118(4):1214–1217. doi:10.1378/chest.118.4.1214.
Young LR, Hadjiliadis D, Davis RD, Palmer SM. Lung transplantation exacerbates gastroesophageal reflux disease. Chest. 2003;124(5):1689–1693. doi:10.1378/chest.124.5.1689.
Stordal K, Johannesdottir GB, Bentsen BS, et al. Acid suppression does not change respiratory symptoms in children with asthma and gastro-oesophageal reflux disease. Arch Dis Child. 2005;90(9):956–960. doi:10.1136/adc.2004.068890.
Jiang SP, Liang RY, Zeng ZY, Liu QL, Liang YK, Li JG. Effects of antireflux treatment on bronchial hyper-responsiveness and lung function in asthmatic patients with gastroesophageal reflux disease. World J Gastroenterol. 2003;9(5):1123–1125.
Bocskei C, Viczian M, Bocskei R, Horvath I. The influence of gastroesophageal reflux disease and its treatment on asthmatic cough. Lung. 2005;183(1):53–62. doi:10.1007/s00408-004-2526-z.
Kiljander TO, Salomaa ER, Hietanen EK, Terho EO. Chronic cough and gastro-oesophageal reflux: a double-blind placebo-controlled study with omeprazole. Eur Respir J. 2000;16(4):633–638. doi:10.1034/j.1399-3003.2000.16d11.x.
Tutuian R, Mainie I, Agrawal A, Adams D, Castell DO. Nonacid reflux in patients with chronic cough on acid-suppressive therapy. Chest. 2006;130(2):386–391. doi:10.1378/chest.130.2.386.
Mainie I, Tutuian R, Agrawal A, et al. Fundoplication eliminates chronic cough due to non-acid reflux identified by impedance pH monitoring. Thorax. 2005;60(6):521–523. doi:10.1136/thx.2005.040139.
Boesch RP, Acton JD. Outcomes of fundoplication in children with cystic fibrosis. J Pediatr Surg. 2007;42(8):1341–1344. doi:10.1016/j.jpedsurg.2007.03.030.
Cantu E III, Appel JZ III, Hartwig MG, et al. J. Maxwell Chamberlain memorial paper. Early fundoplication prevents chronic allograft dysfunction in patients with gastroesophageal reflux disease. Ann Thorac Surg. 2004;78(4):1142–1151. doi:10.1016/j.athoracsur.2004.04.044.
Hartwig MG, Appel JZ, Davis RD. Antireflux surgery in the setting of lung transplantation: strategies for treating gastroesophageal reflux disease in a high-risk population. Thorac Surg Clin. 2005;15(3):417–427. doi:10.1016/j.thorsurg.2005.03.001.
O’Halloran EK, Reynolds JD, Lau CL, et al. Laparoscopic Nissen fundoplication for treating reflux in lung transplant recipients. J Gastrointest Surg. 2004;8(1):132–137. doi:10.1016/j.gassur.2003.10.1013.
Mansi C, Borro P, Giacomini M, et al. Comparative effects of levosulpiride and cisapride on gastric emptying and symptoms in patients with functional dyspepsia and gastroparesis. Aliment Pharmacol Ther. 2000;14(5):561–569. doi:10.1046/j.1365-2036.2000.00742.x.
Fink SM, Lange RC, McCallum RW. Effect of metoclopramide on normal and delayed gastric emptying in gastroesophageal reflux patients. Dig Dis Sci. 1983;28(12):1057–1061. doi:10.1007/BF01295802.
McCallum RW, Fink SM, Lerner E, Berkowitz DM. Effects of metoclopramide and bethanechol on delayed gastric emptying present in gastroesophageal reflux patients. Gastroenterology. 1983;84(6):1573–1577.
Takeda T, Konomi H, Naritomi G, et al. Single oral dose of cisapride accelerates gastric antral emptying in healthy humans: an ultrasonographic study. J Gastroenterol. 1996;31(3):323–328. doi:10.1007/BF02355019.
Campo S, Morini S, Re MA, et al. Esophageal dysmotility and gastroesophageal reflux in intrinsic asthma. Dig Dis Sci. 1997;42(6):1184–1188. doi:10.1023/A:1018841704897.
Fouad YM, Katz PO, Hatlebakk JG, Castell DO. Ineffective esophageal motility: the most common motility abnormality in patients with GERD-associated respiratory symptoms. Am J Gastroenterol. 1999;94(6):1464–1467. doi:10.1111/j.1572-0241.1999.1127_e.x.
Malfroot A, Dab I. New insights on gastro-oesophageal reflux in cystic fibrosis by longitudinal follow up. Arch Dis Child. 1991;66(11):1339–1345. doi:10.1136/adc.66.11.1339.
Poe RH, Kallay MC. Chronic cough and gastroesophageal reflux disease: experience with specific therapy for diagnosis and treatment. Chest. 2003;123(3):679–684. doi:10.1378/chest.123.3.679.
Vandenplas Y. Clinical use of cisapride and its risk-benefit in paediatric patients. Eur J Gastroenterol Hepatol. 1998;10(10):871–881. doi:10.1097/00042737-199810000-00011.
Chen CL, Orr WC, Verlinden MH, et al. Efficacy of a motilin receptor agonist (ABT-229) for the treatment of gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2002;16(4):749–757. doi:10.1046/j.1365-2036.2002.01218.x.
Netzer P, Schmitt B, Inauen W. Effects of ABT-229, a motilin agonist, on acid reflux, oesophageal motility and gastric emptying in patients with gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2002;16(8):1481–1490. doi:10.1046/j.1365-2036.2002.01324.x.
Gerhardt SG, McDyer JF, Girgis RE, Conte JV, Yang SC, Orens JB. Maintenance azithromycin therapy for bronchiolitis obliterans syndrome: results of a pilot study. Am J Respir Crit Care Med. 2003;168(1):121–125. doi:10.1164/rccm.200212-1424BC.
Verleden GM, Dupont LJ. Azithromycin therapy for patients with bronchiolitis obliterans syndrome after lung transplantation. Transplantation. 2004;77(9):1465–1467. doi:10.1097/01.TP.0000122412.80864.43.
Yates B, Murphy DM, Forrest IA, et al. Azithromycin reverses airflow obstruction in established bronchiolitis obliterans syndrome. Am J Respir Crit Care Med. 2005;172(6):772–775. doi:10.1164/rccm.200411-1537OC.
Verleden GM, Vanaudenaerde BM, Dupont LJ, Van Raemdonck DE. Azithromycin reduces airway neutrophilia and interleukin-8 in patients with bronchiolitis obliterans syndrome. Am J Respir Crit Care Med. 2006;174(5):566–570. doi:10.1164/rccm.200601-071OC.
Estenne M, Maurer JR, Boehler A, et al. Bronchiolitis obliterans syndrome 2001: an update of the diagnostic criteria. J Heart Lung Transplant. 2002;21(3):297–310. doi:10.1016/S1053-2498(02)00398-4.
Sifrim D, Castell D, Dent J, Kahrilas PJ. Gastro-oesophageal reflux monitoring: review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut. 2004;53(7):1024–1031. doi:10.1136/gut.2003.033290.
Zerbib F, des Varannes SB, Roman S, et al. Normal values and day-to-day variability of 24-h ambulatory oesophageal impedance-pH monitoring in a Belgian-French cohort of healthy subjects. Aliment Pharmacol Ther. 2005;22(10):1011–1021. doi:10.1111/j.1365-2036.2005.02677.x.
Kudoh S, Azuma A, Yamamoto M, Izumi T, Ando M. Improvement of survival in patients with diffuse panbronchiolitis treated with low-dose erythromycin. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1829–1832.
Jaffe A, Bush A. Anti-inflammatory effects of macrolides in lung disease. Pediatr Pulmonol. 2001;31(6):464–473. doi:10.1002/ppul.1076.
Gottlieb J, Szangolies J, Koehnlein T, Golpon H, Simon A, Welte T. Long-term azithromycin for bronchiolitis obliterans syndrome after lung transplantation. Transplantation. 2008;85(1):36–41.
D’Ovidio F, Mura M, Tsang M, et al. Bile acid aspiration and the development of bronchiolitis obliterans after lung transplantation. J Thorac Cardiovasc Surg. 2005;129(5):1144–1152. doi:10.1016/j.jtcvs.2004.10.035.
D’Ovidio F, Mura M, Ridsdale R, et al. The effect of reflux and bile acid aspiration on the lung allograft and its surfactant and innate immunity molecules SP-A and SP-D. Am J Transplant. 2006;6(8):1930–1938. doi:10.1111/j.1600-6143.2006.01357.x.
Hadjiliadis D, Duane DR, Steele MP, et al. Gastroesophageal reflux disease in lung transplant recipients. Clin Transplant. 2003;17(4):363–368. doi:10.1034/j.1399-0012.2003.00060.x.
Palmer SM. Reflux of bile acids: an innate problem of lung transplantation. Am J Transplant. 2006;6(8):1757–1758. doi:10.1111/j.1600-6143.2006.01425.x.
Davis RD Jr, Lau CL, Eubanks S, et al. Improved lung allograft function after fundoplication in patients with gastroesophageal reflux disease undergoing lung transplantation. J Thorac Cardiovasc Surg. 2003;125(3):533–542. doi:10.1067/mtc.2003.166.
Peeters TL. Erythromycin and other macrolides as prokinetic agents. Gastroenterology. 1993;105(6):1886–1899.
Thielemans L, Depoortere I, Perret J, et al. Desensitization of the human motilin receptor by motilides. J Pharmacol Exp Ther. 2005;313(3):1397–1405. doi:10.1124/jpet.104.081497.
Sifrim D, Blondeau K. Technology insight: the role of impedance testing for esophageal disorders. Nat Clin Pract Gastroenterol Hepatol. 2006;3(4):210–219. doi:10.1038/ncpgasthep0446.
Bala I, Prasad K, Bhukal I, Nakra D, Pratap M. Effect of preoperative oral erythromycin, erythromycin-ranitidine, and ranitidine-metoclopramide on gastric fluid pH and volume. J Clin Anesth. 2008;20(1):30–34. doi:10.1016/j.jclinane.2007.08.002.
Asai T, Murao K, Shingu K. Pre-operative oral erythromycin reduces residual gastric volume and acidity. Br J Anaesth. 2000;85(6):861–864. doi:10.1093/bja/85.6.861.
Memis D, Turan A, Karamanlioglu B, et al. Effect of preoperative oral use of erythromycin and nizatidine on gastric pH and volume. Anaesth Intensive Care. 2002;30(4):428–432.
Clarke AT, Wirz AA, Manning JJ, Ballantyne SA, Alcorn DJ, McColl KE. Severe reflux disease is associated with an enlarged unbuffered proximal gastric acid pocket. Gut. 2008;57(3):292–297. doi:10.1136/gut.2006.109421.
Bisschops R, Sifrim D, Vos R, Janssens J, Tack J. Influence of gastric motility modifying drugs on the postprandial acid and bile pockets at the gastro-esophageal junction. Gastroenterology (in press).
Sifrim D, Matsuo H, Janssens J, Vantrappen G. Comparison of the effects of midecamycin acetate and azithromycin on gastrointestinal motility in man. Drugs Exp Clin Res. 1994;20(3):121–126.
Ward C, Forrest IA, Brownlee IA, et al. Pepsin like activity in bronchoalveolar lavage fluid is suggestive of gastric aspiration in lung allografts. Thorax. 2005;60(10):872–874. doi:10.1136/thx.2004.036426.
Mertens V, Blondeau K, Vanaudenaerde BM, et al. Pepsin or bile acids: what is the best marker of gastric aspiration in lung transplant recipients? J Heart Lung Transplant. 2008;27(2):S125–S126. doi:10.1016/j.healun.2007.11.188.
Koek GH, Vos R, Sifrim D, Cuomo R, Janssens J, Tack J. Mechanisms underlying duodeno-gastric reflux in man. Neurogastroenterol Motil. 2005;17(2):191–199. doi:10.1111/j.1365-2982.2004.00633.x.
Fountos A, Chrysos E, Tsiaoussis J, et al. Duodenogastric reflux after biliary surgery: scintigraphic quantification and improvement with erythromycin. ANZ J Surg. 2003;73(6):400–403. doi:10.1046/j.1445-2197.2003.t01-1-02654.x.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mertens, V., Blondeau, K., Pauwels, A. et al. Azithromycin Reduces Gastroesophageal Reflux and Aspiration in Lung Transplant Recipients. Dig Dis Sci 54, 972–979 (2009). https://doi.org/10.1007/s10620-009-0725-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-009-0725-4