
Abstract
A recent study of Wilms’ tumors discovered a new X chromosome gene, Wilms’ tumor gene on the X chromosome (WTX), which was found to harbor small deletions and point mutations. WTX protein negatively regulates Wnt/ β-catenin signaling, and is considered a tumor-suppressor gene. One of the questions about the WTX gene is whether the genetic alterations of the WTX gene are specific to only Wilms’ tumors. To see whether somatic point mutations of WTX occur in other malignancies, we analyzed the WTX gene for the detection of mutations in 141 cancer tissues by a single-strand conformation polymorphism assay. The cancer tissues consisted of 47 gastric adenocarcinomas, 47 colorectal adenocarcinomas, and 47 hepatocellular carcinomas. Overall, we detected one WTX mutation in the colorectal carcinomas (1/47; 2.1%), but there was no WTX mutation in other cancers analyzed. The detected mutation was a missense mutation (c. 1117G > A (p.Ala373Thr)). Although the WTX mutation is common in Wilms’ tumors, our data indicate that it is rare in colorectal, gastric, and hepatocellular carcinomas. The data also suggest that deregulation of Wnt/ β-catenin signaling by WTX gene mutation may be a rare event in the pathogenesis of colorectal, gastric, and hepatocellular carcinomas.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Recently Rivera et al. [1] searched for genetic abnormalities in sporadic Wilms’ tumors by array comparative genomic hybridization and found an X chromosome gene, Wilms’ tumor gene on the X chromosome (WTX) gene. They found small deletions and point mutations of the WTX gene in 13.4% and 8.5% of Wilms’ tumors, respectively [1]. The point mutations and deletions of the WTX occur at comparable frequencies in male and female Wilms’ tumors, and heterozygous deletions of WTX target the active chromosome in female Wilms’ tumors, suggesting a ‘one-hit inactivation’ of WTX [1]. Functionally, transfection of WTX cDNA in cultured cells led to suppression of colony formation and apoptosis [1]. Interestingly, WTX forms a complex with β-catenin, AXIN1, β-TrCP2 and APC, and promotes β-catenin degradation [2]. Together, these data suggest that WTX is a tumor-suppressor gene, and that both deletions and point mutations of the WTX may lead to loss of the tumor suppressor activity of WTX in Wilms’ tumor.
Rivera et al. [1] found seven point mutations of the WTX gene in 82 Wilms’ tumors, and one (c. 1072C > T) of the mutations was observed in two independent cases. The six types of the point mutations consisted of two nonsense (c. 1072C > T and c. 1000C > T), three frameshift (c. 438_439insT, c. 1649delC and c. 1070delA) and one missense (c. 876G > C) mutation (s).
Aberrant WNT/ β-catenin signaling is important not only in Wilms’ tumor [3, 4], but also in other cancers such as colorectal, gastric, and hepatocellular carcinomas [5–7]. Thus, it is important to identify whether WTX, a tumor-suppressor and regulator of WNT/ β-catenin signaling, is mutated in these cancers as well. However, to date, the data on point mutations of WTX in human cancers besides Wilms’ tumor are lacking. In this study, we analyzed 141 cases of human colorectal, gastric, and hepatocellular carcinomas tissues for the detection of point mutations in the WTX gene.
Materials and Methods
Tissue Samples
Methacarn-fixed tissues of 47 gastric carcinomas, 47 colorectal carcinomas, and 47 hepatocellular carcinomas were randomly selected for this study. The colorectal carcinomas originated from cecum (N = 1), ascending colon (N = 9), transverse colon (N = 1), descending colon (N = 2), sigmoid colon (N = 13), and rectum (N = 21). The gastric carcinomas consisted of 20 diffuse-type, 16 intestinal-type, and 11 mixed-type gastric adenocarcinomas by Lauren classification, and ten early and 37 advanced gastric carcinomas according to the depth of invasion. The hepatocellular carcinomas consisted of Edmondson grade I (N = 5), grade II (N = 19) and grade III (N = 23) according to Edmondson and Steiner’s criteria. The background histology of the hepatocellular carcinomas showed cirrhosis in 36 cases, chronic active hepatitis in eight cases, chronic persistent hepatitis in two cases, and non-specific changes in one case. Hepatitis B virus (HBV) and Hepatitis B virus (HCV) were detected in 43 and three cases, respectively.
All of the patients were Asian (Korean). Approval was obtained from the Catholic University of Korea, College of Medicine’s institutional review board for this study. We analyzed the primary tumors, but not the metastatic lesions. We did not include the cancer cell lines in this study. Tumor cells and normal cells from the same patients were selectively procured from hematoxylin and eosin-stained slides using a 30G1/2 hypodermic needle (Becton Dickinson, Franklin Lakes, NJ) affixed to a micromanipulator by the microdissection, as described previously [8, 9]. Genomic DNA extraction was performed by a modified single-step DNA extraction method by proteinase K treatment [8, 9].
Polymerase Chain Reaction (PCR) and Single-Strand Conformation Polymorphism (SSCP)
The WTX gene consists of two exons and the second exon encompasses the entire coding region [1]. We performed the mutational analysis of the WTX gene in the exon 2 sequences. Genomic DNA each from tumor cells and normal cells were amplified with 20 primer pairs. Radioisotope ([32P]dCTP) was incorporated into the PCR products for detection by autoradiogram. The PCR reaction mixture was denatured for 1 min at 94°C and incubated for 30 cycles (denaturing for 30 s at 94°C, annealing for 30 s at 50–57°C, and extending for 30 s at 72°C). Other procedures of PCR and SSCP analysis were performed as described previously [8, 9]. After SSCP, DNAs showing mobility shifts were cut out from the dried gel, and re-amplified for 30 cycles using the same primer sets. Sequencing of the PCR products was carried out using a capillary automatic sequencer (ABI Prism Genetic Analyzer, Applied Biosystems, Foster City, CA, USA) according to the manufacturer’s recommendation. We repeated the experiments three times, including PCR, SSCP and sequencing analysis to ensure the specificity of the results.
Results and Discussion
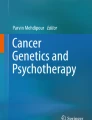
Genomic DNAs isolated from normal and cancer tissues of the 141 patients were analyzed for the detection of mutations in the entire coding region of WTX gene by the PCR–SSCP analysis. On the SSCP autoradiograms, all of the PCR products were clearly seen (Fig. 1). The PCR–SSCP analysis identified aberrant bands in one (2.1%) of the 47 colorectal carcinomas (Fig. 1), but not in other cancer types analyzed. DNA from normal tissue from the same patient with the aberrant bands on the SSCP showed no evidence of mutation on SSCP, indicating the aberrant bands had risen somatically (Fig. 1). DNA sequence analysis of the aberrantly migrating bands led to identification of a WTX missense mutation in the exon 2. The mutation was c. 1117G > A, which would result in a substitution of an amino acid (p.Ala373Thr). The colorectal carcinoma with the mutation was a rectal adenocarcinoma with TNM stage II, and was a microsatellite-stable (MSS) type carcinoma according to the NCI criteria [10]. We repeated the experiments twice, including tissue microdissection, PCR and SSCP analyses to ensure the specificity of the results, and found that the data were consistent.

Representative SSCP and DNA sequencing of WTX gene mutation. SSCP (a) and DNA sequencing analysis (b) of WTX DNA from tumors (Lane T) and normal tissues (Lane N). a: The SSCP of the PCR products with a primer pair (WTX Exon 2–5) using four colorectal cancers and their corresponding normal tissues. A colorectal carcinoma (case #51T) shows aberrant bands (arrows) compared to the SSCP from normal tissue (N) from the same patient. b: DNA sequencing analysis from the aberrant bands (case #51T) shows DNA sequence change. There is a nucleotide change (G > A) in tumor tissue (T) as compared to normal tissue (N)
One of the central aims of cancer research has been to identify mutated genes that are causally implicated in tumorigenesis [11]. Some of the causal cancer mutations, including p53, RAS and β-catenin mutations, occur widely in human cancers [5, 6, 12, 13]. By contrast, other mutations, including EGFR and JAK2 mutations, occur in specific cancer types [14, 15]. Thus, when a gene is reported to harbor somatic mutation in a cancer type, one of the following studies is to identify whether the mutation is mutated in other cancers as well [16, 17]. Because WTX mutation has been identified only in Wilms’ tumors, we tried to find out whether it is mutated in other malignancies. However, in this study, we detected only one WTX mutation in colorectal carcinomas, but none in gastric carcinomas nor hepatocellular carcinomas. These data demonstrate that somatic point mutation in the N-terminal area of the WTX is rare in common cancers in digestive system. Also, we identified that other common cancers, including breast and lung cancers, did not harbor WTX gene mutation (unpublished data). Together, these data suggest that point mutations of the WTX gene may be restricted mainly in Wilms’ tumors.
Among the WTX point mutations detected in Wilms’ tumors, all except one mutation (6/7) were nonsense or frameshift mutations that would result in premature stops of WTX protein synthesis in the N-terminal area. Because C-terminal half of WTX protein is crucial to binding of WTX with β-catenin [2], the mutational alterations of WTX likely abolish association of the mutants with β-catenin and may lead to activation of WNT/ β-catenin signaling [2]. In the present study, we found one missense mutation of WTX that would not result in any production of truncated WTX protein. Moreover, this mutation is not overlapped with the WTX mutations reported in the previous study [1]. It appears that the missense mutations of WTX detected in the earlier [1] and our studies might represent passenger mutations. The functional implication of the missense mutations of WTX remains identified in the future studies.
Although point mutation of the WTX gene is a feature of Wilms’ tumors, deletion of the WTX was more commonly found than the point mutations [1]. It is also possible that deletion of WTX gene is a way of WTX inactivation in colorectal or gastric or hepatocellular carcinoma. Therefore, deletion of WTX gene together with expression status of WTX protein in these cancers should be performed in the future studies.
References
Rivera MN, Kim WJ, Wells J, et al. An X chromosome gene, WTX, is commonly inactivated in Wilms’ tumor. Science. 2007;315:642–645. doi:10.1126/science.1137509.
Major MB, Camp ND, Berndt JD, et al. Wilms’ tumor suppressor WTX negatively regulates WNT/beta-catenin signaling. Science. 2007;316:1043–1046. doi:10.1126/science/1141515.
Koesters R, Ridder R, Kopp-Schneider A, et al. Mutational activation of the beta-catenin proto-oncogene is a common event in the development of Wilms’ tumors. Cancer Res. 1999;59:3880–3882.
Koesters R, Niggli F, von Knebel Doeberitz M, Stallmach T. Nuclear accumulation of beta-catenin protein in Wilms’ tumours. J Pathol. 2003;199:68–76. doi:10.1002/path.1248.
Clevers H. Wnt/beta-catenin signaling in development and disease. Cell. 2006;127:469–480. doi:10.1016/j.cell.2006.10.018.
Van der Flier LG, Sabates-Bellver J, Oving I, et al. The intestinal Wnt/TCF signature. Gastroenterology. 2007;132:628–632. doi:10.1053/j.gastro.2006.08.039.
de La Coste A, Romagnolo B, Billuart P, et al. Somatic mutations of the beta-catenin gene are frequent in mouse and human hepatocellular carcinomas. Proc Natl Acad Sci USA. 1998;95:8847–8851. doi:10.1073/pnas.95.15.8847.
Lee SH, Shin MS, Park WS, et al. Alterations of Fas (Apo-1/CD95) gene in non-small cell lung cancer. Oncogene. 1999;18:3754–3760. doi:10.1038/sj.onc.1202769.
Kim HS, Lee JW, Soung YH, et al. Inactivating mutations of caspase-8 gene in colorectal carcinomas. Gastroenterology. 2003;125:708–715. doi:10.1016/S0016-5085(03)01059-X.
Boland CR, Thibodeau SN, Hamilton SR, et al. A National Cancer Institute Workshop on Microsatellite Instability for cancer detection and familial predisposition: development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res. 1998;58:5248–5257.
Hanahan D, Weinberg RA. The hallmarks of cancer. Cell. 2000;100:57–70. doi:10.1016/S0092-8674(00)81683-9.
Downward J. Targeting RAS signalling pathways in cancer therapy. Nat Rev Cancer. 2003;3:11–22. doi:10.1038/nrc969.
Levine AJ. p53, the cellular gatekeeper for growth and division. Cell. 1997;88:323–331. doi:10.1016/S0092-8674(00)81871-1.
Paez JG, Jänne PA, Lee JC, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304:1497–1500. doi:10.1126/science.1099314.
Kralovics R, Passamonti F, Buser AS, et al. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N Engl J Med. 2005;352:1779–1790. doi:10.1056/NEJMoa051113.
Lee JW, Soung YH, Kim SY, et al. Mutational analysis of MYC in common epithelial cancers and acute leukemias. APMIS. 2006;114:436–439. doi:10.1111/j.1600-0463.2006.apm_383.x.
Jeong EG, Lee SH, Yoo NJ, Lee SH. Absence of nucleophosmin 1 (NPM1) gene mutations in common solid cancers. APMIS. 2007;115:341–346. doi:10.1111/j.1600-0463.2007.apm_592.x.
Acknowledgments
This work was supported by a grant from the Korea Healthcare Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A080083).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yoo, N.J., Kim, S. & Lee, S.H. Mutational Analysis of WTX Gene in Wnt/ β-Catenin Pathway in Gastric, Colorectal, and Hepatocellular Carcinomas. Dig Dis Sci 54, 1011–1014 (2009). https://doi.org/10.1007/s10620-008-0458-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-008-0458-9