
Abstract
This study analyses the potential impact of e-cigarettes on the death toll of cigarette smoking in the Russian Federation by working under a variety of assumptions pertaining to how much vaping might affect smoking cessation and initiation, and its adverse impacts on health in comparison to conventional smoking. Within this study, each combination of these assumptions generates a single vaping scenario (210 in total). A dynamic population simulation model, specifically for the Russian Federation, that is tailoured to tobacco control policy analysis, is built for estimation purposes. Considering the toll of smoking on cumulative life-years saved via the inclusion of vaping across a period of 80 years, the simulation analysis produces positive results in 88.1% of e-cigarette scenarios, ranging from − 3.3 million to 38.5 million life-years saved. In relative terms, the estimated life-years saved from vaping varies from − 1.6 to 18.6% of the predicted life-years lost from smoking. Most of the model scenarios involve a significant number of individuals who stopped smoking in favour of vaping. These results suggest that vaping has great potential to reduce the prevalence of smoking and the related death toll in the Russian Federation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
According to the latest international survey on tobacco consumption conducted in the Russian Federation, the Global Adult Tobacco Survey (WHO 2018) estimates that 29.9% (35.8 million) of the adult population were smokers in 2016; the prevalence of current smokers was 48.8% among men and 14.2% among women.
Moreover, our estimates, based on the Russian Longitudinal Monitoring Survey (RLMS), suggest that the level of smoking prevalence in the Russian Federation remains significant: in 2019, it was 27.4% (43.9% for men and 13.8% for women), higher than the world average.
The death toll from smoking in the Russian Federation also remains high: In 2019, around 291.4 thousand people died from smoking-related diseases, which accounts for 16.3% of all deaths in the country (Institute for Health Metrics and Evaluation 2019). These numbers place the Russian Federation within the top five countries for highest smoking-related mortality.
Reducing the levels of disease and death from smoking has been one of the main goals for public health policies. The Russian Federation ratified the World Health Organization Framework Convention on Tobacco Control in 2008. Further tobacco-control efforts were directly associated with the necessity of bringing Russian legislation in line with the requirements of international agreements and the willingness of authorities to decrease the prevalence of conventional smoking (the use of combustible cigarettes) and its negative impact on public health.
In November 2019, the Russian Federation adopted a strategy on countering tobacco consumption as well as any other nicotine-containing products by the government’s decree which targets to reduce smoking prevalence among adults to 21% by 2035. Starting in 2020, the Russian Federation has been implementing the policy of equally regulating combustible cigarettes and any other nicotine-containing products (including e-cigarettes) without considering the health risks degree associated with the use of these products (WHO FCTC 2020).
In April 2021, the Russian Federation adopted a plan for the introduction of normative acts which, in the opinion of the authors, will decrease not only cigarette consumption but the use of any nicotine-containing products (The Russian Government 2021). These acts include:
-
1.
The introduction of the ban on the classification of nicotine-containing products based on the level of toxic substances.
-
2.
Expansion of the bans functioning in Russia on production, export, and import of nasvay (smokeless tobacco for oral use, which is produced and used mostly in central Asian countries) and snus to the territory of all members of the Eurasia Union.
-
3.
Introduction of plain packaging requirements for nicotine-containing products.
It appears that the Russian Federation does not plan to assist current smokers (who are not able to quit smoking unaided) to quit by switching to safer alternatives, while an increasing number of countries recognize that enabling access to non-cigarette alternatives, such as electronic cigarettes (e-cigarettes), could be used as an effective harm reduction policy measure (Kennedy et al. 2017; Shah et al. 2021).
In general, the efficacy of vaping (the use of e-cigarettes) in reducing the toll of smoking is dependent on the following factors: (i) its effect on human health compared to smoking, (ii) its effect on smoking cessation in adults, and (iii) its effect on smoking initiation in the youth (National Academies of Sciences, Engineering, and Medicine 2018).
Recent studies suggest that vaping has substantially fewer health risks compared to smoking (Sobczak et al. 2020); namely, it reduces the adverse general and oral health effects of smoking (Cassidy et al. 2020; O’Connel et al. 2016, Polosa et al. 2020; Tatullo et al. 2016). In addition, a clinical trial conducted in Italy identified that vaping helps smokers reduce tobacco consumption and improve pulmonary health conditions (Lucchiari et al. 2020). However, opponents of e-cigarettes emphasize that the health risks of vaping are considerably higher than supporters advocate as the implications for long-term health effects are not yet well researched (National Academies of Sciences, Engineering, and Medicine 2018; Singh et al. 2020; Wang et al. 2018). Therefore, a level of uncertainty about the degree of risk reduction associated with vaping does still exist within the literature.
Notwithstanding, numerous studies suggest that vaping is not only safer than smoking but that it also increases cessation among adult smokers (Abrams et al. 2018; Caraballo et al. 2017; Cook et al. 2019; Hartmann-Boyce et al. 2021; Ramamurthi et al. 2016).A time series analysis of trends from the population in the UK reveals that e-cigarette use is associated with an improvement in the success rate of stopping smoking (Beard et al. 2020). The positive impact of vaping on the success rate of quit attempts has also been observed in Australia (Chambers 2022). A similar study conducted in the USA showed that vaping is not only positively associated with quitting success, but moreover increases the likelihood of attempting to stop smoking (Levy et al. 2018). Other studies find that vaping increases smoking cessation in the adult population and is a more effective cessation tool than nicotine replacement products (Berry et al. 2019; Chan et al. 2021; Zhu et al. 2017). In Germany, the use of e-cigarettes as a smoking cessation aid is also associated with greater success than attempting to stop unaided (Kotz et al. 2022). Furthermore, randomized clinical trials conducted in New Zealand show improvement in cessation when patches are used in combination with e-cigarettes containing nicotine (Walker et al. 2019). Contrarily, however, some studies argue that vaping does not help smokers quit (Weaver et al. 2018).By vaping in places where smoking is prohibited, smokers also dull the effects of smoke-free environmental policies, which itself could stimulate the dual use of electronic and combustible cigarettes and reduce smoking cessation rates (Glantz and Bareham 2018).
One additional concern in the promotion of e-cigarettes as a harm reduction tool is the possibility that vaping might act as a gateway that increases smoking initiation rates, especially in the youth (Baenziger et al. 2021; Centers for Disease Control and Prevention 2019).National cross-sectional studies conducted in both South Korea and the USA from 2014 provide evidence that vaping is associated with a higher prevalence of smoking among adolescents (Dutra and Glantz 2014; Lee et al. 2014;). A meta-analysis conducted in 2017 identified that vaping increases the likelihood of subsequent smoking in young vapers (aged 14–30 years) by four times (Soneji et al. 2017). Although recent studies conducted in the Netherlands and Belgium show that associations between vaping and smoking initiation are attributable to the shared risk factors of tobacco use in general (Kim and Selya 2020; Martinelli et al. 2021), these risk factors include parental education and smoking, peer smoking, sensation-seeking behaviour, impulsivity, delinquent behaviour, internalizing symptoms (depression, anxiety, etc.), alcohol and marijuana use, exposure to health warning labels on cigarette packs, and cigarette advertising receptivity (Kim and Selya 2020).
Some argue that e-cigarette use is largely concentrated among youths with similar characteristics to smokers, suggesting that vaping acts as a replacement for smoking, rather than it being an instigating factor (Sokol and Feldman 2021). Furthermore, adolescents who initially experiment with e-cigarettes are less likely to initiate smoking than their peers with a matched propensity score (Shahab et al. 2021). These findings, therefore, indicate that e-cigarette use might reduce the initiation of smoking.
Literature assessing the potential for e-cigarettes to diminish the death toll from smoking is still limited. Most studies that estimate the health impact of e-cigarettes on the population only focus on the USA and the UK (Lee et al. 2020), while to the best extent of our knowledge, such estimates do not exist for the Russian Federation. Consequently, this present study offers a unique contribution as the first attempt to estimate the potential impact of e-cigarettes on the toll of smoking within the Russian Federation.
For estimation purposes, we constructed a dynamic population simulation model that is tailoured towards tobacco control policy analysis in the Russian Federation, based on the methodology developed by Mendez et al. (1998) and extended by Jin et al. (2015). Following Mendez and Warner (2021), we simulate the proportion of smoking-related deaths in the Russian Federation that could be reduced with e-cigarette use, under a variety of assumptions—those based on how vaping might affect smoking initiation and cessation, and its adverse impacts on health in comparison to traditional cigarettes.
Methodology
Background Simulation Model
The dynamic population simulation model tracks individuals from the ages of 0 to 70 + , as differentiated by sex and smoking status (never smokers, current smokers, and former smokers), with the baseline year taken from 2019 (the last year before the COVID-19 pandemic for which data on smoking and diseases attributable death rates are available).
The first step in the construction of the model was the estimation of the population by age, sex, and smoking status during the baseline year. For each subsequent year, the population evolves: A new birth-cohort is introduced; at 18 years old, certain never smokers start and become current smokers; some current smokers quit and become former smokers; and everybody is subject to age-, sex-, and smoking status-specific death rates (for a schematic representation of the model and model specification, see Supplementary Materials B).
We obtained sex- and age-specific population statistics for 2019 from the Center for Demographic Research at the New Economic School (CDR-NES) (Table A1).
To estimate sex- and age-specific smoking prevalence in the baseline year, we used RLMS data. RLMS is a nationally representative survey which collects data on the health and economic welfare of households and individuals in the Russian Federation. Data have been collected annually from 1994 at the individual, household, and community levels. RLMS consists of two types of samples: (a) original sample addresses (drawn in 1994) and (b) follow-up addresses. Follow-up addresses are needed for panel analyses of individual changes, while original sample addresses create a representative sample for a given year. In our analysis, we use only the cross-sectional part of the sample. For a detailed description of RLMS data, see Supplementary Materials C.
Based on RLMS data from 2019, we attributed adults who presently report smoking any tobacco products (filtered, non-filtered, or fine tobacco) into the current smoker group, without considering additional information on smoking intensity. More specifically, these are individuals who provided a positive answer to the question “Do you now smoke?”. Former smokers are those who report smoking tobacco products in the past, but do not smoke at present (negatively answered the question “Do you now smoke?” and positively answered the question “Have you ever smoked?”). We attributed individuals who did not smoke now and had not smoked in the past to never smokers (Table A2).
It should be mentioned that RLMS 2019 data include former smokers aged 18—people who briefly started and gave up smoking before they turned 19. We treat these individuals as never smokers because temporary teen year smokers are not particularly important to public health policy.
By combining our estimates of sex- and age-specific smoking prevalence (current, former, and never smokers) with population statistics, we estimated the population for the baseline year by age, sex, and smoking status (Table A3).
For succeeding years, we work on the assumption that the new birth cohort is constant annually—the number of births is kept at the level of the baseline year. Moreover, following Jin et al. (2015) and Mendez and Warner (2021), we regard everyone aged 0–17 to be a never smoker: with smoking initiation only occurring at 18, and those who start thereafter regarded as current smokers. From age 19, some smokers begin to quit the habit, with those who do stop becoming former smokers—we also assume that initiation does not reoccur.
We obtained smoking cessation and initiation rates, by sex, from RLMS data from 2019. Sex-specific smoking cessation rates are estimated for three age categories: the population aged 19–34, 35–50, and > 50 as the proportion of people who stopped smoking within one year and do not currently smoke. More specifically, these rates represent the share of smokers who indicated “1 year” as an answer to the question “How many years ago did you quit smoking?” in total smokers. Smoking cessation rates are estimated by age categories as the relationship between cessation rates and age might differ across countries or over time. Some studies suggest that the smoking cessation rate declines with age (Babb et al. 2017; Messer et al. 2008), while others found the opposite (Jeon et al. 2018; Mendez et al. 1998). In the case of the Russian Federation, smoking cessation increases with age among men and decreases among women (Table 1). One possible explanation is that pregnancy might act as a powerful force that discourages smoking among young women. Indeed, data identify relatively high cessation rates among women of childbearing age, with lower rates for older women.
Sex-specific smoking initiation rates are estimated as the proportion of current smokers in the population aged 18 (Table 1). According to our estimates, the initiation rate among men (14.4%) is considerably higher in the Russian Federation than among women (5.3%). This is in line with the existing trends in smoking prevalence among men and women in the Russian Federation (Figs. 2 and 3).
In the next stage, we estimated sex- and age-specific death rates separately for never smokers, current smokers, and former smokers. We used existing estimates of the relative risk of adult mortality from smoking-related diseases (the likelihood of dying for current and former smokers relative to the risk of death for never smokers) in the USA: as defined by smoking status and age for different tobacco-related diseases (19 disease categories in total), provided by the National Center for Chronic Disease Prevention and Health Promotion Office (USA) on Smoking and Health (2014) and based on Cancer Prevention Study II (Table A4). We combined the estimated relative risks with the sex-, age-, and disease-specific mortality data from the Russian Federation, provided by the CDR-NES. A detailed description of the methodology is provided in the Supplementary Materials D. Table A5 demonstrates the sex- and age-specific death rates differentiated by smoking status. Following Mendez and Warner (2021), we assume that smoking-related deaths do not occur before the age of 35; therefore, death rates before 35 do not differ by smoking status.
Based on the collected data and estimated variables, we constructed a dynamic population simulation model for the Russian Federation. This model projects the population size by smoking status for each year and every year of age for 80 years, starting from the baseline of 2019. The model has the potential to be employed in the analyses of the impact of both preexistent and future policies on tobacco control and taxation.
Model Accuracy—Retrospective Model for Russia
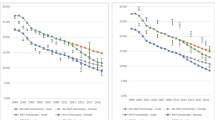
It is important to question whether the constructed model can produce accurate estimates. Therefore, to check the predictive power of the model, we used a retrospective analysis. More specifically, we constructed a retrospective model for the Russian Federation using the same methodology described above, though in this instance based on data from 2000 rather than 2019; the year was selected as it is the earliest period in which all the variables required for the model were available. All the other assumptions and estimation techniques were held constant across all years. Subsequently, we compared the simulation results of our model with estimates from the available RLMS data on smoking—among total adults, men, and women, respectively, from 2000 to 2019 (Figs. 1, 2, and 3).

Comparison of simulation results and RLMS estimates for smoking prevalence, 2000–2019. Source: Authors’ estimations based on RLMS 2000–2019, simulations

Comparison of simulation results and RLMS estimates for smoking prevalence among men, 2000–2019. Source: Authors’ estimations based on RLMS 2000–2019, simulations

Comparison of simulation results and RLMS estimates for smoking prevalence among women, 2000–2019. Source: Authors’ estimations based on RLMS 2000–2019, simulations
According to our estimates based on the RLMS, the smoking prevalence has been gradually declining since 2000, when it was 35.0%. The smoking prevalence rates simulated by the model are close to the actual indicators calculated based on the RLMS data, in both levels and trends. Our projections are, on average, 4.5 percentage points (pp) lower than RLMS estimates between 2000 and 2019. This appears to be driven predominantly by the lower accuracy of the model in predicting smoking prevalence among women—the gap between the simulated and the estimated prevalence increases over time, as our model predicts a gradual decline in smoking rates among women, whereas RLMS estimations show a stable trend. In the analysis of 2000–2019, the difference between the simulated and the RLMS estimated smoking prevalence is on average 5.9 pp for women; in contrast, the difference for men smoking prevalence is only 2.8 pp.
This distinction between the simulated and RLMS-calculated smoking prevalence in women might be explained by a possible underestimation of the initiation rate. Estimated initiation rates might be lower than true initiation rates as self-reported smoking prevalence generally tends to underestimate the actual smoking prevalence (Connor et al. 2009), particularly among women and adolescents (Hwang et al. 2018).
When constructing our model, we also fixed smoking cessation rates in women at its level for 2000 − 5.7%, while cessation rates were lower from 2002 to 2013 and 2016 to 2019 (Fig. 4). This might lead to an overestimation of cessation rates in our model.

RLMS estimates of smoking initiation and cessation rates among men and women, 2000–2019. Source: Authors’ estimations based on RLMS 2000–2019
Moreover, as the cessation rates are calculated by the proportion of smokers who quit a year ago (smokers in 1999 who quit in 2000), the estimated cessation rates both for men and women may be slightly overestimated as some of those who quit may relapse later (we assume no relapse in our model).
When we calibrate the retrospective model by reducing smoking cessation rates by 20% and using men’s initiation rate for women, the model accuracy notably improved: the difference between the simulated and the RLMS estimated smoking prevalence becomes on average 0.3 pp for women and 1.6 pp for men (Figs. 5 and 6).

Comparison of simulation results and RLMS estimates for smoking prevalence among men: Calibrated retrospective model, 2000–2019. Source: Authors’ estimations based on RLMS 2000–2019

Comparison of simulation results and RLMS estimates for smoking prevalence among women: Calibrated retrospective model, 2000–2019. Source: Authors’ estimations based on RLMS 2000–2019
Sensitivity Analysis
To assess the robustness of the results reported here, we conducted a sensitivity analysis. First, we estimated the background smoking initiation rate as the proportion of current smokers in the population aged 18–24. Our assumption used in the main model that smoking initiation only takes place at age 18 simplifies the estimations; however, in real life, initiation occurs before or after 18 years of age as well (Barrington-Trimis et al. 2020). The data support this argument: In 2019, smoking prevalence in the Russian Federation was notably higher in the population aged 19–24 compared to 18 years old (20.1% vs. 10.0%) (Table A2). Second, based on the results of the retrospective analysis, we used the estimated initiation rate among men as a background initiation rate for women. Third, as estimated background cessation rates may be overestimated due to our assumption that initiation does not reoccur among former smokers, we adjust them by 20%. Using new values for background cessation and initiation rates (Table A6), we reran all simulations.
Simulation Analysis
Within the first stage of our simulation analysis, we replicated the Russian population under two reference scenarios:
-
1.
A status quo scenario: assuming a continuation of the baseline smoking initiation and cessation rates for the following 80 years.
-
2.
A never-smoking scenario: assuming no one ever smoked, nobody smokes in the baseline year or will smoke in the future. Therefore, there are no smoking-related deaths, which indicates that all individuals are subject to the same death rates as never smokers.
The difference between these two scenarios demonstrates an estimation of the total life-years lost (LYL) due to smoking in the absence of vaping. This exercise is needed to express the life-saving potential of e-cigarettes as a share of smoking-related LYL.
We thereafter simulated population size by applying various assumptions (described below) on how vaping affects smoking behaviour and health outcomes (Table 2). Each combination of these assumptions thus creates a single e-cigarette scenario (210 scenarios in total). The annual difference in population size between each e-cigarette scenario and the status quo provides that year’s estimated life-years saved (LYS) or LYL due to vaping. Cumulative LYS or LYL for the full 80 years are calculated by adding these annual estimates. In addition, we expressed the cumulative LYS or LYL for each e-cigarette scenario as a share of the LYL due to smoking in the status quo scenario. Finally, we estimated the share of vaping-induced quitters (“e-quitters”) from the total number of quitters during the entire simulation period.
Annual background smoking cessation (1) and initiation (2) rates are held constant for all years of the simulation analysis. While assumptions on the impact of vaping on smoking behaviour and health are replicated from Mendez and Warner (2021) with some modifications, specifically:
-
3.
The impact of vaping on smoking cessation rates: We assume that vaping increases the background cessation rate from 5 to 200%. Vaping having no effect or having a negative impact on smoking cessation has not been considered. It should be emphasized that each value represents an increase in the overall population cessation rate; however, only a fraction of smokers use vaping as a cessation tool. For instance, assuming 10% of smokers use e-cigarettes in the quit attempts and if the population-wide smoking cessation increases by 5%, the cessation rate for those using e-cigarettes would increase by 50%, while the cessation rate for other smokers will be unaffected. This estimation is in line with recent a study from Australia suggesting that vaping increases the success rate of quit attempts by 68–98% (Chambers 2022).
-
4.
The impact of vaping on smoking initiation rates: Our e-cigarette scenarios incorporate a broader range of assumptions on a change in smoking initiation due to vaping than in Mendez and Warner (2021), in which half of e-cigarette scenarios assume a 10% increase in smoking initiation and the remaining half assume vaping has no impact on the instigation of smoking. We considered even greater (a 15% and 20% increase) allowances for the impact on initiation. However, as discussed earlier, the relationship between smoking and vaping might be spurious. Recent studies suggest that vaping might act as a replacement for smoking and adolescents who initially experiment with vaping are less likely to start smoking than their peers with similar characteristics (Shahab et al. 2021; Sokol and Feldman 2021). These findings together with the fact that smoking initiation among US youth and young adults declined rapidly in parallel with increased vaping suggest that e-cigarettes might reduce the initiation of smoking. Therefore, in simulation analysis, we also used a 10%, 15% and 20% decrease in annual smoking initiation due to vaping.
-
5.
The health risks of vaping for former smokers: We assume that smokers who quit smoking with using vaping might have an elevated mortality risk compared to those who quit without it. The magnitude of an increase in mortality risk depends on the duration of vaping after quitting smoking. Smokers who quit with the help of e-cigarettes and continue to use them into the future will experience much greater risks compared to those who also give up vaping shortly after quitting smoking. The values of vaping-associated risks used in our model are applied to all e-quitters and represent the average risk experienced by vaping-aided smoking cessation, which means that, for example, a 5% vaping risk used in the model represents much higher risks for long-term vapers and much lower for those who quit vaping shortly. Therefore, assumptions on 10% or even 5% of vaping health risks are conservative compared to estimates of the UK health authorities that found the vaping health risks for long-term vapers to be less than 5% (McNeill et al. 2018; Royal College of Physicians 2016).
Results
Life-Years Lost due to Smoking
According to our estimation, in the absence of vaping, the annual death toll from smoking in the Russian Federation amounted to around 245.4 thousand lives in 2019. This is a more conservative figure than projected by the Institute for Health Metrics and Evaluation (2019) according to which nearly 291.4 thousand people died from smoking-related diseases in Russia that year. However, this difference might lie within the methodologies used, as the Institute for Health Metrics and Evaluation uses its classification system, list of smoking-related diseases, and own estimates for the relative risks of smoking. They also assume that smoking-related deaths occur from age 30 onwards, while we assumed that the corresponding age is 35 onwards.
In addition, over 80 years after the baseline, we estimated the cumulative LYL from smoking in the absence of e-cigarettes (Table A7). The simulations reveal that approximately 207.3 million life-years would be lost due to smoking over this period. Due to a higher smoking prevalence, the LYL for men is considerably greater than for women. In the absence of e-cigarettes, the estimated smoking-related LYL accounts for 2.3% and 24.1% of life-years for the adult population and current smokers, respectively.
According to our dynamic population model, the smoking prevalence in the status quo scenario in the Russian Federation would decline from 27.4% in 2019 to 17.4% in 2030 (Fig. 8). By 2040, smoking prevalence would decline further to 11.4%. In the long term, as smoking cessation and initiation rates in the model are fixed at the level of 2019, smoking prevalence would reach its equilibrium at 4.3%.
Such a sharp decline in smoking in the status quo scenario is driven by decreasing smoking initiation and increasing smoking cessation rates in the Russian Federation (Fig. 4). At the same time, as discussed earlier, estimated initiation and cessation rates may differ from their true values due to assumptions applied during their estimations.
E-cigarette Scenarios
Summary Results for All 210 Scenarios
In total, 88.1% of e-cigarette scenarios (185 out of 210) produce positive LYS. Table 3 provides a summary of the simulations; detailed results of simulations for all e-cigarette scenarios are presented in Supplementary Table A10. The LYS range from − 3.3 million to 38.5 million years. In relative terms, the estimated LYS vary from − 1.6 to 18.6% of LYL due to smoking. The scenario with the lowest LYS is a combination of assumptions, namely that vaping increases smoking cessation by 5% and smoking initiation by 20%, while e-quitters have a 20% elevated mortality risk. In the scenario with the highest LYS, vaping increases smoking cessation by 200%, reduces smoking initiation by 20%, and has no adverse health impacts on former smokers who quit smoking using e-cigarettes.
Life-Years Saved by Vaping: Comparison with Results Provided by Mendez and Warner (2021)
Table 4 identifies the life-saving potential of vaping when it increases smoking cessation by 10%, 25%, 50%, and 100%. The results are provided for both assumptions—when vaping does not affect smoking initiation and when it increases initiation by 10%. Equally, these estimations identify the relative risk of vaping (5%, 10%, and 20%)—the reduction in the mortality benefits from quitting smoking without vaping compared to quitting with vaping. The results present those e-cigarette scenarios for which assumptions on smoking cessation, initiation, and health risks of vaping are replicated from Mendez and Warner (2021). We demonstrate the calculations as LYS, its share in LYL due to smoking in the absence of vaping, and number of e-quitters.
Every combination of assumptions yields positive cumulative LYS in the 80 years—ranging from 2.9 to 22.8 million life years in absolute terms, and from 1.6 to 11.0% as a share of LYS by vaping in LYL due to smoking. All the scenarios involve a significant number of e-quitters, reaching up to 17.3 million in the scenarios that increase smoking cessation by 100% and smoking initiation by 10%.
These results are comparable with the ones estimated by Mendez and Warner (2021). In absolute terms, a number of LYS and e-quitters in the Russian Federation are 60–90% lower than in the USA. This difference is primarily driven by the US population size which is more than twice the population in the Russian Federation. On other hand, smoking prevalence is higher in the Russian Federation than in the USA, which reduces the difference in the estimates of LYS and e-quitters. In relative terms (the share of LYS by vaping in LYL due to smoking), a simulation analysis for chosen scenarios shows nearly identical results to the ones estimated by Mendez and Warner (2021).
The estimates in Table 4 suggest that the greatest impact on LYS is derived from the assumption that vaping does heighten smoking cessation rates, while the results are less sensitive to changes in the assumptions on vaping risk and the effect of vaping on smoking initiation.
E-cigarette Scenarios with a Negative Impact on Life-Years
Out of 210 e-cigarette scenarios, vaping implies a negative impact on life-years in 25 scenarios. In those 25 scenarios, 15 scenarios are created by the combination of assumptions that vaping increases smoking cessation by 5% and smoking initiation by 10%, 15%, or 20%. In the other 10 scenarios, we assume that the impact of vaping on the cessation rate is 10%, while initiation increases by 15% or 20%. In all these scenarios, the elevated health risks of vaping from 0 to 20% are assumed.
We believe that these scenarios are highly unlikely. As mentioned earlier, recent studies suggest that the use of e-cigarettes is associated with higher smoking prevalence in young adults with similar characteristics to young smokers; this association is attributable to the shared risk factors of tobacco use in general (Kim and Selya 2020; Martinelli et al. 2021). Also, adolescents who first tried e-cigarettes are less likely to initiate cigarette smoking than their peers (Shahab et al. 2021). Therefore, e-cigarettes most likely decrease smoking initiation rather than increase it.
In addition, if vaping increases the success rate of smoking quit attempts by about 100% (Chambers 2022), the assumption used in our simulations that vaping increases the population-wide cessation rate by 5% (or 10%) implies that on average only 5% or 10% of smokers would use e-cigarettes in their quitting attempts in the following 80 years from the baseline. While this seems to be a realistic assumption considering the existing setup in the Russian Federation, the share of smokers who will use e-cigarettes to quit smoking in the future depends on the regulation and taxation of e-cigarettes and the attitude of policymakers towards the use of e-cigarettes as a cessation tool. If 20% or more of smokers will use e-cigarettes in their quitting attempts, assumption of 5% or 10% increase in population-wide cessation rates would be a conservative estimate.
Most Plausible E-cigarette Scenarios
Based on the discussion provided earlier on the impact of vaping on smoking cessation and initiation, we chose four e-cigarette scenarios which we believe are most plausible (Table 5). These are scenarios in which we assume an increase in smoking cessation of 25% and 50% and a decrease in smoking initiation by 10%. As we do not believe that vaping is risk-free, in these scenarios, we also assume vaping risk of 5% or 10%.
Every combination of assumptions yields positive cumulative LYS in the 80 years showing the potential of e-cigarettes to avert smoking-related deaths. In these scenarios, LYS ranges from 9.9 to 16.8 million life years in absolute terms (Fig. 7), and from 4.8 to 7.9% as a share of LYS by vaping in LYL due to smoking. The potential number of e-quitters is estimated at 5.3 million in scenarios when vaping increases smoking cessation by 25% and 9.6 million in cases when smoking cessation increases by 50%. Due to higher cessation and lower initiation rates, smoking prevalence in selected e-cigarette scenarios declines more rapidly than in status quo scenario and reaches its long-term equilibrium at 3.4% (impact of vaping on cessation: 50%) and 3.1% (impact of vaping on cessation: 25%) (Fig. 8).

The cumulative life-years saved due to e-cigarettes over the 80 years in most plausible e-cigarette scenarios. Source: Authors’ calculations

Estimated smoking prevalence in most plausible e-cigarette scenarios and status quo over the 80 years. Source: Authors’ calculations
Sensitivity Analysis
After using adjusted background smoking cessation and initiation rates, simulation analysis produces 167 scenarios with positive LYS (79.5% of all e-cigarette scenarios). Table A8 provides a summary of simulations, while detailed results of simulations for all e-cigarette scenarios are presented in Supplementary Table A11. The additional 18 scenarios with negative LYS are the combination of assumptions that vaping has a positive impact on cessation (25% or 50%), but simultaneously increases initiation (by 15% or 20%) and health risks for e-quitters (by 5%, 10%, or 20%). Also, the resulting LYS range is notably wider on both positive and negative sides and varies from − 14.8 million to 56.4 million years in absolute and from − 6.3 to 24.1% of LYL due to smoking in relative terms. The scenarios with the lowest and highest LYS are the same combination of assumptions as in the main specification of the model. In cases of the most plausible e-cigarette scenarios, the sensitivity analysis produces similar results (Table A9).
Conclusion
Our research demonstrates that vaping has the significant potential to reduce smoking prevalence and the related death toll in the country. Most vaping scenarios yield positive LYS, except for 25 scenarios in which the LYS are negative but close to 0. The scenarios with negative results are highly unlikely. According to our estimates, vaping potentially may save up to 18.6% (in the most optimistic scenario) of the LYL due to smoking in the Russian Federation.
Meanwhile, the Russian Federation’s current policies do not regard e-cigarettes as a tool for combatting smoking. Furthermore, the recent changes in the Russian regulatory framework for e-cigarettes would discourage smokers from using e-cigarettes as an alternative to combustible cigarettes, keeping the prevalence of e-cigarette use on or below 5% level. This reduces the amplitude of possible impacts of vaping on smoking cessation and smoking initiation. And the chances of achieving the level of LYS observed in the most optimistic e-cigarette scenarios (when vaping increases cessation by 100% or 200% and decreases smoking initiation) substantially decrease. Thus, the policy recently implemented in the Russian Federation will negatively affect the potential health benefits of vaping (LYS).
Based on our analysis, and given the current policies, it is possible that vaping could help to save between 4.8 and 7.9% of LYL due to cigarette smoking in the Russian Federation, which would translate to an estimated 9.9 to 16.8 million life-years saved. It is important to note, however, that these estimates are based on the scenarios we selected and that real-world outcomes may vary within the ranges mentioned above.
Limitations
The study has several limitations. First, we fixed constant smoking initiation and cessation rates at the 2019 levels. Nevertheless, the researchers suggest that initiation has been declining over recent decades, while cessation rates have been increasing (Cantrell et al. 2018; Hamzeh et al. 2020; Marcon et al. 2018).
Another limitation is that we only consider elevated vaping-related health risks for people who successfully quit smoking. The greater health risks for dual users—those who failed to stop smoking via vaping and continued both smoking and vaping—have been discounted.
Finally, the baseline year in our model is 2019. Given that people were already vaping in 2019, estimated background smoking cessation and initiation rates already reflect a fraction of vaping impacts. In 2016, 3.5% of the adult population in the Russian Federation (5.4% of men and 1.9% of women) reported currently vaping (WHO 2018). The trade data further indicate that the volume of imported e-cigarettes increased from 0.7 million sticks in 2016 to 2.7 million by 2019 (Melkadze 2021).
Data Availability
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Change history
31 July 2023
A Correction to this paper has been published: https://doi.org/10.1007/s10603-023-09549-4
References
Abrams, D. B., Glasser, A. M., Pearson, J. L., Villanti, A. C., Collins, L. K., & Niaura, R. S. (2018). Harm minimization and tobacco control: Reframing societal views of nicotine use to rapidly save lives. Annual Review of Public Health, 39(1), 193–213. https://doi.org/10.1146/annurev-publhealth-040617-013849
Babb, S., Malarcher, A., Schauer, G., Asman, K., & Jamal, A. (2017). Quitting smoking among adults — United States, 2000 – 2015. MMWR, 65, 1457–1464. https://doi.org/10.15585/mmwr.mm6552a1external
Baenziger, O. N., Ford L., Yazidjoglou, A., Joshy, G., & Banks, E. (2021). E-cigarette use and combustible tobacco cigarette smoking uptake among non-smokers, including relapse in former smokers: Umbrella review, systematic review and meta-analysis. BMJ Open, 11(3), e045603. https://doi.org/10.1136/bmjopen-2020-045603
Barrington-Trimis, J. L., Braymiller, J. L., Unger, J. B., McConnell, R., Stokes, A., Leventhal, A. M., Sargent, J. D., Samet, J. M., & Goodwin, R. D. (2020). Trends in the age of cigarette smoking initiation among young adults in the US from 2002 to 2018. JAMA Network Open, 3(10). https://doi.org/10.1001/jamanetworkopen.2020.19022
Beard, E., West, R., Michie, S., & Brown, J. (2020). Association of prevalence of electronic cigarette use with smoking cessation and cigarette consumption in England: A time–series analysis between 2006 and 2017. Addiction, 115, 961–974. https://doi.org/10.1111/add.14851
Berry, K. M., Reynolds, L. M., Collins, J. M., Siegel, M. B., Fetterman, J. L., Hamburg, N. M., Bhatnagar, A., Benjamin, E. J., & Stokes, A. (2019). E-cigarette initiation and associated changes in smoking cessation and reduction: The population assessment of tobacco and health study, 2013–2015. Tobacco Control, 28(1), 42–49. https://doi.org/10.1136/tobaccocontrol-2017-054108
Cantrell, J., Bennett, M., Mowery, P., Xiao, H., Rath, J., Hair, E., & Vallone, D. (2018). Patterns in first and daily cigarette initiation among youth and young adults from 2002 to 2015. PloS One, 13(8), e0200827. https://doi.org/10.1371/journal.pone.0200827
Caraballo, R. S., Shafer, P. R., Patel, D., Davis, K. C., & McAfee, T. A. (2017). Quit methods used by US adult cigarette smokers, 2014–2016. Preventing Chronic Diseases, 14, 160600. https://doi.org/10.5888/pcd14.160600
Cassidy, R. N., Tidey, J. W., & Colby, S. M. (2020). Exclusive e-cigarette users report lower levels of respiratory symptoms relative to dual e-cigarette and cigarette users. Nicotine & Tobacco Research, 22, 54–60. https://doi.org/10.1093/ntr/ntaa150
CDC. (2019). Quick facts on the risks of e-cigarettes for kids, teens, and young adults. Centers for Disease Control and Prevention. https://www.cdc.gov/tobacco/basic_information/ecigarettes/Quick-Facts-on-the-Risks-of-E-cigarettes-for-Kids-Teens-and-Young-Adults.html
Chambers, M. S. (2022). Effect of vaping on past-year smoking cessation success of Australians in 2019 - evidence from a national survey. Addiction, 2022, 1–10. https://doi.org/10.1111/add.15897
Chan, G. C. K., Stjepanović, D., Lim, C., Sun, T., Shanmuga, A. A., Connor, J. P., Gartner, C., Hall, W. D., & Leung, J. (2021). A systematic review of randomized controlled trials and network meta-analysis of e-cigarettes for smoking cessation. Addictive Behaviors, 119, 106912. https://doi.org/10.1016/j.addbeh.2021.106912.
Connor, G. S., Schofield-Hurwitz, S., Hardt, J., Levasseur, G., & Tremblay, M. (2009). The accuracy of self-reported smoking: A systematic review of the relationship between self-reported and cotinine-assessed smoking status. Nicotine & Tobacco Research, 11(1), 12–24. https://doi.org/10.1093/ntr/ntn010
Cook, R., Davidson, P., Martin, R., & Dissemination Centre, N. I. H. R. (2019). E-cigarettes helped more smokers quit than nicotine replacement therapy. BMJ, 365, 12036. https://doi.org/10.1136/bmj.l2036
Dutra, L. M., & Glantz, S. A. (2014). Electronic cigarettes and conventional cigarette use among U.S. adolescents: A cross-sectional study. JAMA Pediatrics, 168(7), 610–617. https://doi.org/10.1001/jamapediatrics.2013.5488
Glantz, S. A., & Bareham, D. W. (2018). E-cigarettes: Use, effects on smoking, risks, and policy implications. Annual Review of Public Health, 39, 215–235. https://doi.org/10.1146/annurev-publhealth-040617-013757
Hamzeh, B., Farnia, V., Moradinazar, M., Pasdar, Y., Shakiba, E., Najafi, F., & Alikhani, M. (2020). Pattern of cigarette smoking: Intensity, cessation, and age of beginning: Evidence from a cohort study in West of Iran. Substance Abuse Treatment, Prevention, and Policy, 15(83), 2022. https://doi.org/10.1186/s13011-020-00324-z
Hartmann-Boyce, J., Lindson, N., Butler, A. R., McRobbie, H., Bullen, C., Begh, R., Theodoulou, A., Notley, C., Rigotti, N. A., Turner, T., Fanshawe, T. R., Hajek P. (2021). Electronic cigarettes for smoking cessation. Cochrane Database Systematic Reviews, 11. https://doi.org/10.1002/14651858.CD010216.pub7
Hwang, J. H., Kim, J. Y., Lee, D. H., Jung, H. G., & Park, S. W. (2023). (2018) Underestimation of self-reported smoking prevalence in Korean adolescents: Evidence from gold standard by combined method. International Journal of Environmental Research and Public Health, 15(4), 689. https://doi.org/10.3390/ijerph15040689
IHME. (2019). 2019 Global Burden of Disease (GBD) study. Institute for Health Metrics and Evaluation, University of Washington. https://vizhub.healthdata.org/gbd-results/. Accessed 26 May 2022
Jeon, J., Holford, T. R., Levy, D. T., Feuer, E. J., Cao, P., Tam, J., Clarke, L., Clarke, J., Kong, C. Y., & Meza, R. (2018). Smoking and lung cancer mortality in the United States From 2015 to 2065: A comparative modeling approach. Annals of Internal Medicine, 169(10), 684–693. https://doi.org/10.7326/M18-1250
Jin, L., Kenkel, D., Liu, F., & Wang, H. (2015). Retrospective and prospective benefit-cost analyses of U.S. Anti-smoking policies. Journal of Benefit-Cost Analysis, 6(1), 154–186. https://doi.org/10.1017/bca.2014.1
Kennedy, R. D., Awopegba, A., De León, E., & Cohen, J. E. (2017). Global approaches to regulating electronic cigarettes. Tobacco Control, 26, 440–445. https://doi.org/10.1136/tobaccocontrol-2016-053179
Kim, S., & Selya, A. S. (2020). The relationship between electronic cigarette use and conventional cigarette smoking is largely attributable to shared risk factors. Nicotine & Tobacco Research, 22(7), 1123–1130. https://doi.org/10.1093/ntr/ntz157
Kotz, D., Jackson, S., Brown, J., & Kastaun, S. (2022). The effectiveness of e-cigarettes for smoking cessation-a comparison with nicotine replacement therapy and no use of evidence-based cessation aids in the German population. Deutsches Ärzteblatt. https://doi.org/10.3238/arztebl.m2022.0162
Lee, S., Grana, R. A., & Glantz, S. A. (2014). Electronic cigarette use among Korean adolescents: A cross-sectional study of market penetration, dual use, and relationship to quit attempts and former smoking. Journal of Adolescent Health, 54(6), 684–90. https://doi.org/10.1016/j.jadohealth.2013.11.003
Lee, P. N., Abrams, D., Bachand, A., Baker, G., Black, R., Camacho, O., Curtin, G., Djurdjevic, S., Hill, A., Mendez, D., Muhammad-Kah, R. S., Murillo, J. L., Niaura, R., Pithawalla, Y. B., Poland, B., Sulsky, S., Wei, L., & Weitkunat, R. (2020). Estimating the population health impact of recently introduced modified risk tobacco products: A comparison of different approaches. Nicotine & Tobacco Research, 23(3), 426–437. https://doi.org/10.1093/ntr/ntaa102
Levy, D., Yuan, Y., & Abrams, D. B. (2018). The relationship of e-cigarette use to cigarette quit attempts and cessation: Insights from a large, nationally representative U.S. survey. Nicotine & Tobacco Research, 20(8), 931–939. https://doi.org/10.1093/ntr/ntx166
Lucchiari, C., Masiero, M., Mazzocco, K., Veronesi, G., Maisonneuve, P., Jemos, C., Omodeo, S. E., Spina, S., Bertolotti, R., & Pravettoni, G. (2020). Benefits of e-cigarettes in smoking reduction and in pulmonary health among chronic smokers undergoing a lung cancer screening program at 6 months. Addictive Behaviors, 103(106222), 2022. https://doi.org/10.1016/j.addbeh.2019.106222
Marcon, A., Pesce, G., Calciano, L., Bellisario, V., Dharmage, S. C., Garcia-Aymerich, J., et al. (2018). Trends in smoking initiation in Europe over 40 years: A retrospective cohort study. PLoS One, 13(8), e0201881. https://doi.org/10.1371/journal.pone.0201881
Martinelli, T., Candel, M. J. J. M., de Vries, H., Talhout, R., Knapen, V., van Schayck, C. P., & Nagelhout, G. E. (2021). Exploring the gateway hypothesis of e-cigarettes and tobacco: A prospective replication study among adolescents in the Netherlands and Flanders. Tobacco Control. https://doi.org/10.1136/tobaccocontrol-2021-056528
McNeill, A. D., Brose, L. S., Calder, R., Bauld, L., & Robson, D. J. (2018). Evidence review of e-cigarettes and heated tobacco products 2018: A report commissioned by Public Health England. Public Health England. https://www.gov.uk/government/publications/e-cigarettes-and-heated-tobacco-products-evidence-review. Accessed 13 Jan 2023
Melkadze, A. (2021). Import volume of electronic cigarettes in Russia from 2016 to 2020, from 2016 to 2020 (in in 1,000s) [Chart]. Statista. https://www.statista.com/ Accessed 29 Apr 2022
Mendez, D. & Warner, K.E. (2021). A magic bullet? The potential impact of e-cigarettes on the toll of cigarette smoking. Nicotine & Tobacco Research, 23(4), 654–661. https://doi.org/10.1093/ntr/ntaa160.
Mendez, D., Warner, K.E., & Courant, P.N. (1998). Has smoking cessation ceased? Expected trends in the prevalence of smoking in the United States. American Journal of Epidemiology, 148(3), 249–58. https://doi.org/10.1093/oxfordjournals.aje.a009632.
Messer, K., Trinidad, D. R., Al-Delaimy, W. K., & Pierce, J. P. (2008). Smoking cessation rates in the United States: A comparison of young adult and older smokers. American Journal of Public Health, 98, 317–322. https://doi.org/10.2105/AJPH.2007.112060
National Academies of Sciences, Engineering, and Medicine. (2018). Public health consequences of E-cigarettes. The National Academies Press.
O’Connell, G., Graff, D. W., & D’Ruiz, C. D. (2016). Reductions in biomarkers of exposure (BoE) to harmful or potentially harmful constituents (HPHCs) following partial or complete substitution of cigarettes with electronic cigarettes in adult smokers. Toxicology Mechanisms and Methods, 26(6), 453–464. https://doi.org/10.1080/15376516.2016.1196282
Polosa, R., Morjaria, J. B., Prosperini, U., Busà, B., Pennisi, A., Malerba, M., Maglia, M., & Caponnetto, P. (2020). COPD smokers who switched to e-cigarettes: Health outcomes at 5-year follow up. Therapeutic Advances in Chronic Disease. https://doi.org/10.1177/2040622320961617
Ramamurthi, D., Gall, P. A., Ayoub, N., & Jackler, R. K. (2016). Leading-brand advertisement of quitting smoking benefits for e-cigarettes. American Journal of Public Health, 106, 2057–2063. https://doi.org/10.2105/AJPH.2016.303437
Royal College of Physicians. (2016). Nicotine without smoke: Tobacco harm reduction. Royal College of Physicians.
Shah, A., Britton, J., & Bogdanovica, I. (2021). Developing a novel e-cigarette regulatory and policy control scale: Results from the European Union. Drugs: Education, Prevention and Policy. https://doi.org/10.1080/09687637.2021.1959520
Shahab, L., Beard, E., & Brown, J. (2021). Association of initial e-cigarette and other tobacco product use with subsequent cigarette smoking in adolescents: A cross-sectional, matched control study. Tobacco Control, 30(2), 212–220. https://doi.org/10.1136/tobaccocontrol-2019-055283.
Singh, S., Windle, S. B., Filion, K. B., Thombs, B. D., O’Loughlin, J. L., Grad, R., & Eisenberg, M. J. (2020). E-cigarettes and youth: Patterns of use, potential harms, and recommendations. Preventive Medicine, 133, 106009. https://doi.org/10.1016/j.ypmed.2020.106009
Sobczak, A., Kośmider, L., Koszowski, B., & Goniewicz, M. L. (2020). E-cigarettes and their impact on health: From pharmacology to clinical implications. Polish Archives of Internal Medicine, 130, 668–675. https://doi.org/10.20452/pamw.15229
Sokol, N. A., & Feldman, J. M. (2021). High school seniors who used e-cigarettes may have otherwise been cigarette smokers: Evidence from monitoring the future (United States, 2009–2018). Nicotine & Tobacco Research, 23(11), 1958–1961. https://doi.org/10.1093/ntr/ntab102
Soneji, S., Barrington-Trimis, J. L., Wills, T. A., Leventhal, A. M., Unger, J. B., Gibson, L. A., Yang, J., Primack, B. A., Andrews, J. A., Miech, R. A., Spindle, T. R., Dick, D. M., Eissenberg, T., Hornik, R. C., Dang, R., & Sargent, & J. D. (2017). Association between initial use of e-cigarettes and subsequent cigarette smoking among adolescents and young adults: A systematic review and meta-analysis. JAMA Pediatrics, 171(8), 788–797. https://doi.org/10.1001/jamapediatrics.2017.1488
Tatullo, M., Gentile, S., Paduano, F., Santacroce, L., & Marrelli, M. (2016). Crosstalk between oral and general health status in e‑smokers. Medicine, 95(49), e5589. https://doi.org/10.1097/MD.0000000000005589
The Russian Government. (2021). Goverment decree №1151-R. http://static.government.ru/media/files/bpG6BAI2ud92bfxPEiXMe5Mbl3cAAhzf.pdf. Accessed 14 Jan 2023
U.S. Department of Health and Human Services. (2014). The health consequences of smoking: 50 years of progress. A report of the surgeon general. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
Walker, N., Parag, V., Verbiest, M., Laking, G., Laugesen, M., & Bullen, C. (2019). Nicotine patches used in combination with e-cigarettes (with and without nicotine) for smoking cessation: A pragmatic, randomised trial. Lancet Respiratory Medicine, 8(1), 54–64. https://doi.org/10.1016/S2213-2600(19)30269-3
Wang, J. B., Olgin, J. E., Nah, G., Vittinghoff, E., Cataldo, J. K., Pletcher, M. J., & Marcus, G. M. (2018). Cigarette and e-cigarette dual use and risk of cardiopulmonary symptoms in the Health eHeart Study. PLoS One, 13(7), e0198681. https://doi.org/10.1371/journal.pone.0198681
Weaver, S. R., Huang, J., Pechacek, T. F., Heath, J. W., Ashley, D. L., & Eriksen, M. P. (2018). Are electronic nicotine delivery systems helping cigarette smokers quit? Evidence from a prospective cohort study of U.S. adult smokers, 2015–2016. PLoS One, 13(7), e0198047. https://doi.org/10.1371/journal.pone.0198047
WHO FCTC. (2020). Russian Federation: New regulations on nicotine-containing products adopted. World Health Organization Framework Convention on Tobacco Control, Convention Secretariat. https://untobaccocontrol.org/impldb/russian-federation-new-regulations-on-nicotine-containing-products-adopted/ Accessed 10 Oct 2022
WHO. (2018). GATS Russian Federation, Global Adult Tobacco Survey: Country Report 2016. World Health Organization. https://www.euro.who.int/__data/assets/pdf_file/0010/392887/gats-rus-rep-eng.pdf. Accessed 19 Mar 2022
Zhu, S. H., Zhuang, Y. L., Wong, S., Cummins, S. E., & Tedeschi, G. J. (2017). E-cigarette use and associated changes in population smoking cessation: Evidence from US current population surveys. BMJ, 358, j3262. https://doi.org/10.1136/bmj.j3262
Acknowledgements
This study was funded with a grant from the Foundation for a Smoke-Free World, Inc. (“FSFW”), a US nonprofit 501(c)(3), independent global organization. The contents, selection, and presentation of facts, as well as any opinions expressed herein, are the sole responsibility of the authors and under no circumstances shall be regarded as reflecting the positions of the Foundation for a Smoke-Free World. FSFW had no role in the planning or execution of this study, data analysis, or publication of results.
Funding
Foundation for a Smoke-Free World (P-0062).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: The original version of this article unfortunately contained missing Acknowledgment and Funding information.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mzhavanadze, G., Yanin, D. The Potential Impact of E-cigarettes on the Life-Years Lost from Conventional Smoking in the Russian Federation. J Consum Policy 46, 253–274 (2023). https://doi.org/10.1007/s10603-023-09540-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10603-023-09540-z