
Abstract
Public stigma toward those experiencing symptoms of schizophrenia in the general population is high; yet research into such stigma within the diverse Latino communities remains under-investigated. This study employed a randomized experimental vignette methodology to assess various domains of public stigma toward individuals experiencing psychosis and/or diabetes within Latino communities. A communitybased sample of 243 Latino adults participated. Contrary to our expectations, respondents who were more sympathetic toward those with mental health problems tended to score higher on public stigma. The belief that a person was responsible for their own mental health problems was associated with higher levels of stigma. Results indicate that perceptions of dangerousness toward someone experiencing psychosis were common, and the perception that a person was responsible for their mental health problems was associated with higher levels of stigma Results emphasize the complex nature of stigma within the diverse Latino communities and the need for ongoing research.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Schizophrenia is a serious and chronic mental health condition which if left untreated can have a significant negative impact on the quality of life of those experiencing psychosis, their families and communities (Charlson et al., 2018; National Institute on Mental Health, 2020). Symptoms of schizophrenia may include delusions, hallucinations, challenges with interpersonal relationships, social isolation, and cognitive impairment (National Institute on Mental Health, 2020). It is estimated that at any given time, 1.5 million individuals in the United States meet the diagnostic criteria for a diagnosis of schizophrenia (National Alliance on Mental Illness, 2021), and that the lifetime prevalence of self-reported psychotic symptoms for individuals from Latino1 backgrounds is currently 19.9% (Cohen & Marino, 2014). In addition, members of Latino communities are significantly more likely to receive a diagnosis of schizophrenia when admitted to a psychiatric hospital relative to their White peers (Hamilton et al., 2018). Individuals with a diagnosis of schizophrenia are at increased risk of multiple other co-occurring health conditions including increased risk of death due to COVID-19, death by suicide and other forms of early mortality, heart disease and Type II diabetes (Annamalai et al., 2017; Cadenhead et al., 2019; Charlson et al., 2018; Laursen et al., 2014; Nemani et al., 2021; Olfson et al., 2015).
Mental Health Stigma
Most prior researchers conceptualize mental health stigma as a multidimensional construct (Authors in press; Corrigan & Watson, 2002; Corrigan et al., 2017; Luoma et al., 2007). The authors (in press) put forth a model of public stigma which included five distinct stigma-related domains: (1) social distance stigma, referring to stigma around how an individual feels about someone experiencing a given physical or mental health concern; (2) public stigma, referring to how the larger community perceives a person experiencing a given physical or mental health concern; (3) negative future possibility, referring to stigma around the likelihood of someone experiencing negative outcomes; (4) dangerousness stigma refers to the assessment of someone’s potential for involvement with law enforcement or harming others. Stigma is one of the most salient barriers to seeking help for mental health related conditions as stigma is often related to perceptions of dangerousness, character defects and shame impacting the self, family and community (Corrigan, et al., 2014; Parcesepe & Cabassa, 2013; Turan et al., 2019).
Latinos and Mental Health Stigma
Little is currently known about stigma within Latino communities specifically towards those experiencing symptoms of psychosis or commonly associated physical health conditions such as diabetes (Lopez et al., 2018; Magaña et al., 2007). This lack of knowledge is exacerbated by the fact that although the empirical literature talks about ‘Latinos’ as a single distinct cultural group, Latinos are actually a very heterogenous cultural group despite the fact that they may share a common language (Spanish), history of colonization and geographical region of origin (Cobas et al., 2015; Falicov, 2009; Guarnaccia et al., 2007) Accordingly, it is important to expand the scope of existing literature to better understand the various domains of health and mental health related stigma within Latino communities.
The limited existing stigma research in Latino populations has primarily focused on self-stigma (Gómez-de-Regil et al., 2014), familial stigma (Dorian et al., 2008; Magaña et al., 2007), or reports of stigma from others experienced by those living with severe mental illness (Collins et al., 2008). Prior research is mixed in terms of whether demographic factors such as age, gender, nativity, education level and religiosity influence Latinos’ stigma beliefs in relation to mental illness (Bradbury, 2020; Caplan, 2019; Choi et al., 2019; Gonzalez et al., 2005, 2011; Hirai et al., 2015). One systematic review of stigma in Latinos noted that few studies which included measures of stigma demonstrated a relationship between stigma and sociodemographic characteristics such as gender, education level, and religiosity, but also found that increased age was associated with higher levels of mental health related stigma (Eghaneyan & Murphy, 2020). Echoing the lack of a strong relationship between demographics and stigma, Gómez-de-Regil et al. (2014) reported no significant differences in stigma based on gender or level of education. However other researchers in this area have found that some demographic characteristics such as higher levels of religiosity (Caplan, 2019; Savage & Mezuk, 2014) are correlated with higher levels of stigma toward those with mental health or substance use concerns.
Prior findings are more consistent in relation to acculturation (i.e., minoritized individuals adapting to mainstream cultures) and enculturation (i.e., individuals being socialized into/adhering to their culture of origin) and stigma, both of which have consistently shown to be associated with mental health related stigma in Latino communities (Eghaneyan & Murphy, 2020; Hirai et al., 2015; Rojas-Vilches et al., 2011). Several studies have demonstrated a positive relationship between mental health stigma associated and higher enculturation into Latino-American culture and lower acculturation to mainstream Anglo- American culture (Eghaneyan & Murphy, 2020; Gearing et al., 2021a, 2021b; Hirai et al., 2015; Rojas-Vilches et al., 2011). Rojas-Vilches and et al. (2011) studied mental illness stigma in Puerto Rican and Cuban American young adults and their parents. They found that for both young adults and parents, greater acculturation into mainstream U.S. culture was associated with less negative attitudes toward mental illness and treatment. Values like hard work, fulfilling family obligations, and self-reliance in managing one’s problems are some of the cultural values that may contribute to the stigmatization of mental illness that occurs in Latino communities (Eghaneyan & Murphy, 2020; Mascayano et al., 2016; Yang et al., 2014). Prior work in this area also indicates that Latinos’ experiences of shame further perpetuate stigma toward mental illness and for seeking formal treatment for mental health concerns. (Cabassa, 2003; Eghaneyan & Murphy, 2020; Givens et al., 2007; Jimenez et al., 2013).
Another crucial aspect to understanding mental health related stigma in Latinos is grasping how stigma is impacted by the characteristics of the individual living with symptoms of mental illness. A systematic review by Parescepe and Cabassa (2013) indicated stigmatizing beliefs varied across mental disorders and by the sociodemographic characteristics of the person experiencing mental health concerns. For example, Pescosolido et al. (2010) found that schizophrenia is still a highly stigmatized condition relative to other mental health concerns such as depression or anxiety. A qualitative study of Latina women in New York living with severe mental illness by Collins et al. (2008) highlighted first-hand accounts of the women experiencing the negative impacts of stigma, specifically when it related to their sexual and romantic relationships and their ability to fulfill culturally defined gender roles.
Stigma, Schizophrenia, and Diabetes
Diabetes is another significant health condition impacting Latino communities in the United States and abroad. Approximately 2.5 million Latinos in the United States have been diagnosed with Type II diabetes and many more remain undiagnosed (Aguayo-Mazzucato et al., 2019; American Diabetes association, n.d.). Although no publicly available data exists on the incidence of diabetes within various Latino subgroups, such as Mexican Americans, Puerto Ricans, Cubans etc., compared to non-Hispanic Whites, Latinos have over a 50% increased risk of developing Type II diabetes sometimes during their lifetime and tend to develop this serious health concern at a younger age than their non-Hispanic white peers (American Diabetes Association, n.d.). Existing research has focused on internal factors rather than structural barriers (e.g., stigma from providers). The perception that people with Type II diabetes ‘brought it on themselves’ through unhealthy lifestyle choices such as poor diet, low levels of physical activity and alcohol consumption may contribute to stigma associated with a diabetes diagnosis (Browne et al., 2013; Himmelstein & Puhl, 2021; Lui et al., 2019). The co-occurrence of schizophrenia and Type II diabetes within Latino communities continues to provide challenges for those seeking to improve their physical and psychological health simultaneously. Recent work by Mangurian et al., 2020 indicates that co-occurrence of diabetes and any serious mental illness is higher in Latino communities and is less well controlled. Further complicating this issue and potentially perpetuating stigma in this area is fact that the primary medical treatment for schizophrenia, antipsychotic medication, significantly increases one’s risk of Type II diabetes (Hirsch et al., 2017; Neilson et al., 2010; Smith et al., 2008), potentially discouraging those with untreated psychotic symptoms from seeking care for these symptoms.
Latinos’ Conceptualization of Psychotic Symptoms
The majority of Latinos understand and access mental health care through their primary care providers (Valdez et al., 2011) rather than through a specialty mental health care provider. Accordingly, Casas et al., (2014) and Lopez et al. (2009) assert the need for awareness campaigns to promote ‘psychosis literacy’ in Latino communities to promote overall health and wellness within Latino communities. A study examining the effectiveness of a psychosis literacy campaign in Los Angeles targeting Spanish-speaking Latinos reported that prior to the campaign, only 2% of community residents and 11% of caregivers of individuals with schizophrenia could correctly identify psychotic symptoms experienced by a subject described in a vignette. Moreover, respondents tended to attribute the subject’s struggles to external factors like divorce and family conflict rather than to a treatable medical condition (Lopez et al., 2009). Other work by Cassas et al., (2014) and Dassori et al. (1995) indicates a general reluctance of those in Latino communities to identify psychotic symptoms as something needing medical attention, and may conceptualize these experiences as something mystical, religious or spiritual in nature (Earl et al., 2015; Lewis-Fernandez, 2009) potentially delaying early identification and linkage to beneficial interventions. When taken together these findings point to differences in the presumed etiology of psychotic symptoms by those within Latino communities. Regardless of the presumed etiology, conceptualizes these symptoms through a Western, indigenous, or other lenses, psychotic symptoms have the potential to have a significant negative impact on the interpersonal relationships and functioning of those experiencing these symptoms and those close to them.
Stigma around psychotic symptoms creates an important barrier to members of Latino communities receiving adequate care. The high prevalence of comorbid health disorders, such as diabetes in people living with psychosis exacerbates existing health disparities experienced by Latinos. Prior research in this area indicates that Latinos in the United States report a higher prevalence of psychotic symptoms compared to non-Hispanic Whites (Cohen & Marino, 2014), although the incidence of psychotic symptoms within Latino subgroups is currently unknown. This vulnerability, paired with the well-established challenges in contextualizing and diagnosing psychotic spectrum disorders in Latino populations, highlights the critical need for a better understanding of the various dimensions of stigma and how it manifests in Latino populations (Casas et al., 2014; Lewis-Fernández et al., 2009).
In response to this existing gap in the current empirical literature, this study explores various domains of stigma expressed by Latinos toward Latino individuals experiencing symptoms of schizophrenia, schizophrenia with co-occurring Type II diabetes, or diabetes alone. The aims of the current work are to: (1) to determine if sociodemographic characteristics of study respondents were associated with stigma across multiple domains; (2) to test whether stigma in each domain is different based on the vignette subject experiencing symptoms of schizophrenia alone, diabetes alone, or schizophrenia and co-occurring diabetes, and (3) to examine whether respondents’ perception about the degree to which the vignette person was responsible for his or her condition was associated with different levels of public stigma across domains.
Methods
Participants and Procedures
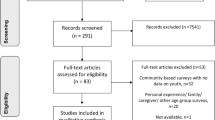
A convenience sample of 500 self-identified Latinos were recruited to participate in an experimental vignette study investigating their attitudes toward and stigma beliefs about mental health related conditions. Participants were recruited by a bilingual research team with the assistance of partner organizations serving the Latino community such as churches, Latino-focused social service agencies, and English-as-a-second-language (ESL) classes. As a group, potential participants were given information about the study, eligibility criteria, expected time of participation, and potential risks and benefits. Eligibility criteria included: 18 years of age or older, self identification as Latino, and reside full time in the U.S. and the ability to communicate in either English or Spanish. This project was approved by the Institutional Review Board (IRB) of the (University blinded for review). Due to nature of group based anonymous recruitment, the research team did not track the total number of individuals who received information about the study, nor the number of people who declined to participate and/or their reasons for non-participation.
Interested participants provided verbal consent to participate, as the research team had requested and received a waiver of documented written consent from the first author’s IRB to ensure the privacy and anonymity of participants, many of whom had the potential to be undocumented immigrants. Following verbal consent, participants received a paper and pencil survey which they could complete in either English or Spanish. Approximately90% of the surveys were administered in Spanish. Participants with vision restrictions or limited reading or writing proficiency had a member of the research team member read them the survey questions and record their responses verbatim. The survey took approximately 45 min to complete, and each participant was given a $15 Walmart gift card for their time and participation which is a common amount of renumeration for completing a survey of this length.
Measures
Whenever possible, validated Spanish language versions of the standardized instruments were used. However, if no validated Spanish language version of the instruments was available the English measures were translated and back translated by a team of professional Spanish language translation experts with input of local community members to help to capture the language nuances of the local Latino communities. A certificate of translation assurance was required by the IRB of the first author’s university prior to data collection to ensure the translation process was both rigorous and accurate.
Demographic Characteristics
Before being presented with the vignettes, participants were asked a series of demographic questions including age, gender, marital status, number of children, education, employment status, financial status, current residential status, country of origin, and generation of immigration. They were also asked if they had ever experienced a mental health problem, if they had a friend or family member who had experienced a mental health problem, or if they knew anyone with a mental health problem. These three items were used to create two binary indicators. One indicator reflects having a relationship with a distant person (i.e., other than family, friends, self or no one) who have mental health problems while the other indicator reflects knowing anyone with a mental health problem (including self, friends, or family).
Spirituality
Religiosity was measured as the mean of six items taken from the Daily Spiritual Experiences Scale (Underwood & Teresi, 2002). Items were answered on a 6-point Likert-type scale from 1 = “Never or Almost never” to 6 = “Many times a day”. Higher scores indicate higher levels of spirituality (Ellison & Fan, 2007). Prior studies indicate that this measure has an internal reliability consistency ranging from 0.89 to 0.95. (Underwood, 2011). A review of the questions included in this scale can be found in Authors (in press).
Acculturation
Acculturation was measured through the 12-item Linguistic Proficiency subscale of the Bidimensional Acculturation Scale for Hispanics (BAS; Marin & Gamba, 1996), which provides scores for two cultural domains: Hispanic (mean of items 1–6) and non-Hispanic (mean of items 7–12). Each item is rated on a Likert-type scale ranging from 1 = “Almost Never” to 4 = “Almost Always.” The internal reliability of this measure ranges between 0.80-0.90 (Cabassa, 2003).
Vignette Experimental Conditions
Participants were presented with two separate vignettes of someone experiencing a mental health condition (depression, schizophrenia, alcohol misuse, or suicidal ideation). Depending on the mental health condition, characteristics of the vignette were modified based on whether the vignette subject was experiencing symptoms of co-occurring Type II diabetes. This paper focuses on a subset of participants (n = 243) who were randomly assigned a vignette featuring a male or female subject experiencing symptoms of psychosis, symptoms of diabetes, or both, resulting in six versions of the vignette. The schizophrenia vignette was originally developed by Link and et al. (1999). The diabetes vignette was constructed drawing on the currently available empirical health literature and then refined through consultation with bilingual experts in the local Latino communities along with medical and mental health professionals.
Vignette Stem
Until 1 year ago, life was very good for [NAME]. But after the year, things started to change. (S/He) thought the people around (her/him) were making comments of disapproval and talking behind (her/his) back. [NAME] was convinced that people were spying on (her/him) and could hear what (she/he) was thinking. [NAME] lost (her/his) motivation to participate in (her/his) daily activities and familiar habits and went to (her/his) house, spending a majority of (her/his) day in (her/his) bedroom. [NAME] was hearing voices even though there was no one else around. These voices told (her/him) what to do and what to think. (S/He) has been living like this for six months. (Schizophrenia with no diabetes).
Mental Health Related Stigma
Following each vignette, participants were asked if they thought the subject of the vignette had a ‘problem’ that needed addressing and were also asked to indicate what they would call that problem. They then completed a 12-item public stigma scale (Brewer et al., 2022) assessing the level and types of stigma the participant held toward the individual in the vignette. This scale, presented in Table 1, has shown strong internal consistency reliability in prior studies (Cheung et al., 2022) focusing on mental health stigma in historically underrepresented ethnic minority communities. The 12 items represented public stigma across four dimensions: social distance (4 items; how the participant perceived the subject of the vignette); public stigma (3 items; how the participant thought the community would perceive the subject of the vignette); dangerousness (2 items; how likely it is that the vignette subject is violent or will end up in legal trouble); negative future (3 items; how likely it is that the vignette subject will be successful and respected in the community). Each item was measured on a 7-point Likert type scale with 1 = “Very unlikely” to 7 = “Very likely”. Nine items were reverse coded so that higher scores represent higher levels of stigma across all items.
Participant Conceptualization of Vignette Diagnosis
One important aspect of vignette-based studies is whether participants adequately comprehend the presented vignette scenario (Auspurg & Hinz, 2015) as participants’ expressed stigma may differ depending on their understanding of the problem. Two dummy indicators were created from their verbatim responses to of “what would you call this problem” for subsequent regression models. Two authors with extensive mental health treatment experience reviewed the qualitative responses and then grouped them into categories of “mental health problem”, “physical health problem” or “other problem” and then further categorized responses to be “correct” if they identified the problem as psychosis, diabetes or both. Disagreement on how to categorize these data was resolved by consensus after consulting with an additional author.
Responsibility
Using a seven-point Likert scale, a single item “Is a person like (vignette subject) responsible for what happened to him/her in life, or is it a result of things beyond his/her control?” was used to measure if the respondent believed the vignette person was responsible for his or her condition. Higher scores indicated greater responsibility.
Statistical Analysis
Factor analysis was performed, and reliability was estimated to assure adequate psychometric performance of the dependent variables, including the stigma scale. Robust maximum likelihood estimation was used since the factor indicators were not normally distributed. Ordinary least squares (OLS) regression was used to estimate the effects of the independent variable and covariates. Mplus 8 was used for factor analysis and Stata 17 was used for all other analyses. Missingness was generally less than five percent, excepting financial circumstances (7%) and responsibility (13%). For factor analysis, missingness was handled using maximum likelihood. For the regression models, missingness was handled using multiple imputation. Fifty datasets were generated using fully conditional specification, which is appropriate for mixtures of variables with different types of distributions (Enders, 2010). Auxiliary variables were used to increase the tenability of the missing at random assumption necessary for multiple imputation. Graphical methods were used to assess imputation model convergence and reasonableness of imputed values.
The mvreg command in Stata was used to accommodate several dependent variables. With this approach, results are identical to estimating separate, OLS regression models for each dependent variable, except that it is possible to perform hypothesis tests across models. This provides a method of controlling Type I error rates. For example, it is possible to examine the joint significance of all equations (i.e., the joint significance of R2 values for all dependent variables) or individual terms across all equations. This approach to controlling Type I error rate is philosophically similar to the premise of finding a significant omnibus test of a regression model prior to interpreting p-values for individual predictors (Cohen & Cohen, 1983), using multivariate analysis of variance prior to interpreting several univariate analyses of variance (Bray & Maxwell, 1985), or to performing an omnibus test prior to interpreting several dummy variable coefficients that combine to form a single predictor with multiple categories (Hardy, 1993). Finally, a variety of diagnostic tests and plots involving leverage, residual behavior, heteroscedasticity, variance inflation, omitted variables, and link violation were checked to ensure the usual assumptions of ordinary least squares regression were tenable. A check was also made to ensure homogeneity of regression slopes for each of the covariates.
Results
Sociodemographic Characteristics of Participants
Sociodemographic characteristics of study participants are included in Table 2. The participants were mostly female (n = 160, 66.12%), partnered (n = 151, 62.40%), and had a high school education or less (n = 148, 61.41%). The mean age of participants was 41.99 years (SD = 15.42), median of 40, ranging from 18 to 86 years of age. Median number of children was two, ranging from zero to 11. Approximately one third reported full-time paid employment (n = 79, 32.51%) and the majority of respondents reported living in an urban area (n = 160, 74.77%). Most were first generation Americans (n = 160, 78.43%) and the most frequently cited country of origin was Mexico (n = 133, 56.36%). Respondents scored relatively high on Hispanic cultural orientation (M = 3.53, SD = 0.59) compared with non-Hispanic cultural orientation (M = 2.31, SD = 0.90) on a scale of one to four. The mean score on spirituality was 4.63 (SD = 0.97) on a scale from one to six. Just over 40 percent (n = 99, 41.60%) indicated that they did not know anyone with a mental health and 10.50% (n = 25) indicated that they had experienced a mental health problem themselves. Respondents were nearly evenly distributed among the experimental groups (n ≈ 80). Approximately 84% of the sample indicated they thought the subject of the vignette had a problem. However, only 36 participants (16.8%) identified the subject of the vignette’s problem (schizophrenia, diabetes, or both) correctly. Eighty-nine participants were partially correct in their assessment (41.6%), meaning they indicated that the vignette subject had some kind of diagnosis related to mental or physical health concerns, or that they correctly identified one out of two diagnoses (but not both) for co-occurring diabetes and psychosis. The mean score for responsibility, on a seven-point scale with higher scores indicating the vignette person had greater responsibility for his or her condition, was 3.10 (SD = 2.01).
Dependent Variable Measurement Model
Since the theorized measurement model for the dependent variables was known, an attempt was made to fit a confirmatory factor model. However, an inadmissible solution was generated. This is likely due to empirical under-identification, which can occur when there are fewer than three indicators per latent variable (Brown, 2015), as is the case with both the ability to change and dangerousness subscales. In addition, two other subscales (public stigma and negative future) only have three indicators each. In sum, there are likely too few items to estimate five latent variables.
Given the unavailability of confirmatory factor analysis to check the measurement model, exploratory factor analysis was used to at least ensure items loaded onto the expected subscales. An oblique rotation criterion (goemin) was used to account for correlation among the subscales.
Items comprising the unable to change subscale were dropped due to cross-loadings. The final model thus included four of the original five subscales. Fit of the final model was marginal: \({\chi }_{Yuan-Bentler}^{2}\) (24) = 71.06, p < 0.001; RMSEA = 0.09, 90% CI [0.07, 0.11]; CFI = 0.95; TLI = 0.86; SRMR = 0.02. Local fit indices revealed the source of the misfit is primarily the social distance subscale, wherein some subsets of variables are more highly correlated with each other. Nevertheless, all items loaded onto the expected factors, with standardized loadings ranging from 0.56 to 0.97.
Correlations between the retained subscales and their reliabilities are reported in Table 3. Reliability was adequate, ranging from 0.75 to 0.93. Respondents who scored higher on public stigma (e.g., vignette persons would have difficulty making friends) tended to score lower (r = −0.34) on social distance (e.g., would be friends with vignette person) and lower (r = −0.34) on negative future (e.g., vignette person will not develop into a successful person). It follows that social distance was strongly, positively correlated (r = 0.51) with negative future. Higher scores on public stigma were modestly, positively correlated (r = 0.24) with dangerousness (e.g., vignette person getting into trouble with the law). Dangerousness was not significantly correlated with social distance or negative future.
Structural Model
Model building proceeded in several steps. Potential covariates were selected based on theoretical considerations. Those that were not significantly correlated with any dependent variable were not included in the model; this includes gender, financial circumstances, Bidimensional Acculturation Scale (Hispanic domain), and spirituality. Preliminary models indicated vignette person gender was not significant for any of the dependent variables either as a main effect or moderator, so it was excluded from later models. The first model included all selected covariates along with interaction effects involving the crossing of experimental group with two dummy variables representing attribution of the vignette person’s problem as physical or mental, respectively. An omnibus test of both interaction effects across all four equations did not achieve significance, thus they were deleted: F (16, 225) = 1.01, p = 0.45. Another set of explanatory variables was also jointly non-significant across all equations, including age, education, parental status, Bidimensional Acculturation Scale (non-Hispanic domain), and the dummy indicator for vignette person’s problem is a mental health issue: F (20, 228.9) = 1.55, p = 0.07.
Results for the final model are shown in Table 4. Each individual equation was significant (i.e., the p-values for R2), and all four equations were also jointly significant: F (24, 233.8) = 4.46, p < 0.001. Proportion of variance explained in the dependent variable ranged from 0.05 to 0.10. An omnibus test of effects for experimental condition failed to achieve significance: F (8, 234) = 1.35, p = 0.22. As can be seen in Table 5, means for all four dependent variables are relatively homogenous across experimental groups. One exception is the dangerousness subscale, wherein the means are somewhat higher for the two schizophrenia groups. As shown in Table 4, these differences are significant when considering only the model for the dangerousness subscale. Nevertheless, due to the non-significant omnibus test for experimental group, this finding is tentative.Footnote 1
The omnibus test for the dummy variable indicating respondents attributed a physical health problem to the vignette person achieved significance: F (4, 234) = 7.79, p < 0.001. At the equation level, this effect achieved significance for all subscales except negative future. Attributing a physical health problem was associated with lower social distance and dangerousness scores but higher public stigma scores. The omnibus test for marital status achieved significance—F (4, 234) = 4.30, p = 0.002—but was individually significant only for the negative future subscale, with married respondents indicating lower scores. The omnibus test for responsibility achieved significance F (4, 228.3) = 3.12, p = 0.02. At the equation level, this effect was significant for only public stigma and negative future. Respondents who believed vignette persons were responsible for their problems tended to score lower on public stigma but higher on negative future.
The omnibus test for mental health problem exposure (i.e., knowing anyone with a mental health problem) achieved significance—F (4, 233.6) = 3.55, p = 0.008—but individually achieved significance only for the negative future subscale. Respondents who knew someone with mental health problems generally expressed higher scores for negative future. A different parameterization was also checked, wherein the dummy indicator represented knowing only a friend or family member with a mental health problem, versus knowing anyone at all. All model results were very similar using this alternate parameterization with the exception of the public stigma subscale. Once again, the omnibus test was significant: F (4, 231) = 4.71, p = 0.001. However, unlike the former parameterization, knowing a friend or family member with a mental health problem was positively predictive of public stigma: b = 0.39, 95% CI (0.02, 0.76), t = 2.06, p = 0.04.
Discussion
This study examined schizophrenia-related stigma among Latino individuals. Only 17% identified the vignette problem as symptoms of psychosis, and approximately 42% were partially correct in their assessment. Although Latinos are more likely to report frequently experiencing symptoms of psychotic disorders compared to other cultural groups, Latinos may perceive or interpret auditory or visual hallucinations differently than as symptoms of a psychotic disorder (Moreira-Almeida et al., 2011). This awareness gap indicates a continued need for increased health literacy in the Latino community to facilitate early identification an linkage to care, as has been echoed in other studies (Casas et al., 2014; Lopez et al., 2009). Future research in this area may wish to qualitatively explore Latinos’ understanding of what it means to have psychotic symptoms and the relationship between this ‘meaning’ and the various domains of stigma. Future research in this area may also wish to better understand the within group differences related to different ethnic groups who are often considered part of the larger “Latino” community in order to determine if certain groups of Latinos may understand the meaning of psychotic symptoms in different ways.
Among participant characteristics, marital status and knowing someone with a mental health problem were significant predictors of negative future scores. Generally, considering the diversity of participant characteristics included within the study (i.e., education, age, gender, financial circumstances, parental status, acculturation, and spirituality), it is somewhat surprising that only two characteristics were found to be associated with two of the subscales. Interestingly, acculturation and spirituality, which have been shown to be associated with mental health-related stigma in Latino communities in previous work (Eghaneyan & Murphy, 2020; Hirai et al., 2015; Rojas-Vilches et al., 2011), was not significant in the current study. However, our findings do align with existing research into mental health stigma within Latino communities, which has failed to show a relationship between stigma and demographic factors (Eghaneyan & Murphy, 2020; Gómez-de-Regil et al., 2014).
Respondents who were married generally expressed lower scores for negative future. This study appears to be the first to observe marital status among Latinos as being related to a subscale of stigma. Other studies have observed how family and social structures within Latino communities can influence such characteristics as attitudes towards mental health therapy (Rojas-Vilches et al., 2011), and so this relationship between marital status and mental health stigma could be an area for further examination.
Respondents who knew someone with mental health problems generally expressed higher scores for negative future. When a different parameterization was checked that was limited to whether respondents knew a friend or family member with a mental health problem as opposed to anyone (acquaintance, etc.) a positive association was also observed with the public stigma subscale. Less utilization of mental healthcare services can lead to poorer health outcomes, and so if the person with a mental health issue known to respondents was untreated—which is not unlikely in the broader context of barriers to care for this population—than they could continue to experience a range of difficulties. Moreover, respondents who know a friend or family member with a mental health problem may be directly involved in their care, as informal caregiving is not uncommon in certain Latino communities and therefore may have encountered barriers to accessing formal support for their loved ones (Rojas-Vilches et al., 2011). These respondents may have witnessed or experienced first-hand public stigma while supports for a friend or family member with a mental health issue. Additionally, knowing someone with mental health issues was associated with two of the study’s subscales, and differences were observed depending on the category of relationship (e.g., friend and family versus acquaintance). Future research might consider how different social network characteristics within different Latino communities may impact these relationships and constructions of different kinds of stigma, a recommendation that has been put forth by other scholars (Pescosolido et al., 2010).
Findings from the regression model indicate, there was no difference in stigma based on symptoms experienced by the vignette subject (psychosis, Type II diabetes or both). Stigma levels were relatively homogenous across diagnostic groups. Endorsement of dangerousness was higher for both schizophrenia groups (schizophrenia, and schizophrenia and diabetes health problem). Given the low level of accuracy of identifying psychotic symptoms in this study, a finding that has been seen in other studies (Lopez et al., 2009), it is difficult to interpret what aspects of the schizophrenia symptoms may be eliciting higher perceptions of dangerousness. Also, given that Latino communities have been shown to describe and attribute psychotic symptoms to domains outside of the biomedical model (Cassas et al., 2014; Dassori et al., 1995), it is not clear as what interpretations of these symptoms (religious, social, etc.) may be related to perceptions of dangerousness.
Conceptualization of the problem as being related to one’s physical health emerged as an important factor. Both perceptions of dangerousness and desire for social distance decreased when participants conceptualized the vignette problem as being related to physical, rather than mental health.
The extent to which a person was viewed as being responsible for their situation influenced both public stigma and expectations about the person’s future, albeit in opposite directions. Public stigma was lower with greater attribution of responsibility. However, greater attribution of responsibility predicted higher perceptions of negative future. The construct of responsibility relates to previously identified cultural values of self-reliance in managing one’s problems as well as fulfilling familial and work obligations that are possible contributors to the stigmatization of mental illness that occurs in Latino communities (Eghaneyan & Murphy, 2020; Mascayano et al., 2016; Yang et al., 2014). One way to consider this finding is that respondents may be operating from different causal models for mental illness. For example, a study by Dillon and et al. (2011) on how Latina women infer causation for different types of addictive disorders identified spiritual, moral character, and disease attribution models. For the current study, one possibility is that respondents are operating from a moral character attribution model wherein mental health problems are the result of poor individual choices. In this model, the vignette person’s issues are not exacerbated by societal forces such as stigma but rather by their decisions.
Limitations
Estimating regression parameters using latent variables or at least estimated latent variable factor scores is preferable to using naïve mean scores because measurement error is controlled (McNeish & Wolf, 2020). This was not possible in the present study due to an inadmissible solution when attempting to fit a CFA model to the dependent variables, likely due to an insufficient number of indicators per subscale (Brown, 2015). Further scale development efforts should be undertaken to increase the number of items per subscale for this measure.
These results were based on a convenience sample of Latino participants in a large urban area in the Southcentral United States. Thus, our findings may not generalize to rural Latino communities or Latino communities in other areas of the U.S. Moreover, it is important to not conceptualize all Latinos as a monolithic cultural group, although demographic characteristics such as region of origin were not significantly related to any of the domains of stigma in this study, it is still important to conceptualize Latinos as having a significant degree of within group heterogeneity. All measures were self-reported, and the main study outcome was stigma; as such, social desirability bias may have influenced these findings.
Conclusion
This study contributes to the literature in several understudied and important areas by focusing on the relation between different domains of public stigma within a sample of people from Latino communities (location blinded for review). Our findings have relevance to mental health literacy campaigns that seek to increase symptom identification, and to mental health service utilization efforts that seek to ensure early detection and treatment. Regardless of whether one conceptualizes schizophrenia as a mental health condition, a sign of spirituality or something else, if untreated schizophrenia can have significant negative impacts on one’s quality of life and the quality of life of others close to them. Efforts to help people in the community accurately identify symptoms of psychosis as a significant, but treatable, health condition, may help to further decrease stigma toward schizophrenia and increase the number of people in Latino communities receiving treatment for health-related concerns. Efforts to support increased understanding of mental and physical health conditions is critical, since there is ample evidence indicating Latinos wait until late in the progression of illness to seek formal help (Cassas et al., 2014; Aguayo-Mazzucato et al., 2019; Oh et al., 2014) and that delaying help often results in a poorer long term treatment prognosis. Traumatic interactions with providers, such as involuntary hospitalizations and the involvement of law enforcement, may decrease the likelihood that individuals will want to seek help (Aguayo-Mazzucato et al., 2019). To better facilitate care for those in Latino communities, recommendations include building trust and respect for one’s lived experiences and cultural values, while ensuring that patients’ basic needs are addressed, and assessing for within group differences related to beliefs regarding help seeking within Latino communities. Interventions which include family members from the beginning and those aimed at directly helping individuals to access and engage early in mental health care are recommended. Research indicates that family members can support access to formal care and assist with barriers to treatment (Gearing, 2008; Rojas-Vilches et al., 2011). This study adds to a growing body of research seeking to build a more inclusive and culturally nuanced understanding of mental health stigma that reaches beyond predominantly White non-Hispanic samples. Such work continues to be essential to understanding mechanisms that keep those experiencing serious mental illness, particularly those from historically marginalized communities from accessing and receiving help.
Notes
One other consideration is that all covariates were verified to be unrelated to experimental group except for the dummy indicator for assessing the vignette person’s problem as being related to physical health. This indicator had a significant, non-trivial association with experimental group: χ2 (2) = 65.33, p < .001, V = .52. In fact, when re-estimating the model without this indicator the omnibus test for experimental group effect is significant: F (8, 235) = 3.80, p < .001. Nevertheless, as before, individually the effects only achieve significance for the dangerousness subscale, albeit with slightly higher effect sizes (1.21 vs. 0.84 for the schizophrenia group and 0.89 vs. 0.67 for the schizophrenia and diabetes group).
References
Aguayo-Mazzucato, C., Diaque, P., Hernandez, S., Rosas, S., Kostic, A., & Caballero, A. E. (2019). Understanding the growing epidemic of type 2 diabetes in the Hispanic population living in the United States. Diabetes/metabolism Research and Reviews, 35(2), e3097. https://doi.org/10.1002/dmrr.3097
American Diabetes Association (n.d.) Diabetes Overview: Complications. https://www.diabetes.org/diabetes/complications
Annamalai, A., Kosir, U., & Tek, C. (2017). Prevalence of obesity and diabetes in patients with schizophrenia. World Journal of Diabetes, 8(8), 390–396. https://doi.org/10.4239/wjd.v8.i8.390
Auspurg, K., & Hinz, T. (2015). Factorial survey experiments. SAGE Publications Inc.
Cheung, M., Leung, P., Chen, W., Gearing, R. E., Brewer, K. B., Chen, X., Li, X., & He, X. (2022). Public stigma on substance users in China. Journal of Substance Use, 27(4), 398–403. https://doi.org/10.1080/14659891.2021.1953163
Brewer, K. B., Washburn, M., Gearing, R. E., Yu, M., Torres-Hostos, L. R., Giraldo-Santiago, N., & Cabrera, A. (2022). Conceptualizations of suicide and suicide-related stigma in Latino communities in the United States. The American Journal of Orthopsychiatry, 92(2), 246–255. https://doi.org/10.1037/ort0000596
Bradbury, A. (2020). Mental health stigma: The impact of age and gender on attitudes. Community Mental Health Journal, 56, 933–938. https://doi.org/10.1007/s10597-020-00559-x
Bray, J. H., & Maxwell, S. E. (1985). Multivariate analysis of variance. SAGE Publications Inc.
Brown, T. A. (2015). Confirmatory factor analysis for applied research. The Guilford Press.
Browne, J. L., Ventura, A., Mosely, K., & Speight, J. (2013). ‘I call it the blame and shame disease’: A qualitative study about perceptions of social stigma surrounding type 2 diabetes. BMJ Open, 3(11), e003384. https://doi.org/10.1136/bmjopen-2013-003384
Cabassa, L. J. (2003). Measuring acculturation: Where we are and where we need to go. Hispanic Journal of Behavioral Sciences, 25(2), 127–146. https://doi.org/10.1177/0739986309352341
Cadenhead, K. S., Minichino, A., Kelsven, S., Addington, J., Bearden, C., Cannon, T. D., Cornblatt, B. A., Mathalon, D., McGlashan, T. H., Perkins, D. O., Seidman, L. J., Tsuang, M., Walker, E. F., Woods, S. W., & Yao, J. (2019). Metabolic abnormalities and low dietary Omega 3 are associated with symptom severity and worse functioning prior to the onset of psychosis: Findings from the North American prodrome longitudinal studies consortium. Schizophrenia Research, 204, 96–103. https://doi.org/10.1016/j.schres.2018.09.022
Caplan, S. (2019). Intersection of cultural and religious beliefs about mental health: Latinos in the faith-based setting. Hispanic Health Care International, 17(1), 4–10. https://doi.org/10.1177/1540415319828265
Casas, R. N., Gonzales, E., Aldana-Aragón, E., Lara-Muñoz, M. D. C., Kopelowicz, A., Andrews, L., & López, S. R. (2014). Toward the early recognition of psychosis among Spanish-speaking adults on both sides of the U.S.-Mexico border. Psychol Serv, 11(4), 460–469. https://doi.org/10.1037/a0038017
Charlson, F. J., Ferrari, A. J., Santomauro, D. F., Diminic, S., Stockings, E., Scott, J. G., McGrath, J. J., & Whiteford, H. A. (2018). Global epidemiology and burden of schizophrenia: findings from the global burden of disease study 2016. Schizophrenia Bulletin, 44(6), 1195–1203. https://doi.org/10.1093/schbul/sby058
Choi, N. Y., Kim, H. Y., & Gruber, E. (2019). Mexican American women college students’ willingness to seek counseling: The role of religious cultural values, etiology beliefs, and stigma. Journal of Counseling Psychology, 66(5), 557–587.
Cobas, J. A., Duany, J., & Feagin, J. R. (2015). How the United States racializes Latinos: White hegemony and its consequences. Routledge.
Cohen, C. I., & Marino, L. (2014). Racial and ethnic differences in the prevalence of psychotic symptoms in the general population. Psychiatric Services, 64(11), 1103–1109. https://doi.org/10.1176/appi.ps.201200348
Cohen, J., & Cohen, P. (1983). Applied multiple regression/correlation analysis for the behavioral sciences. Lawrence Erlbaum Associates.
Collins, P. Y., von Unger, H., & Armbrister, A. (2008). Church ladies, good girls, and locas: Stigma and the intersection of gender, ethnicity, mental illness, and sexuality in relation to HIV risk. Social Science & Medicine, 67(3), 389–397. https://doi.org/10.1016/j.socscimed.2008.03.013
Corrigan, P., Schomerus, G., Shuman, V., Kraus, D., Perlick, D., Harnish, A., Kulesza, M., Kane-Willis, K., Qin, S., & Smelson, D. (2017). Developing a research agenda for understanding the stigma of addictions Part I: Lessons from the mental health stigma literature. The American Journal on Addictions, 26(1), 59–66. https://doi.org/10.1111/ajad.12458
Corrigan, P. W., Druss, B. G., & Perlick, D. A. (2014). The impact of mental illness stigma on seeking and participating in mental health care. Psychological Science in the Public Interest, 15, 37–70. https://doi.org/10.1177/1529100614531398
Corrigan, P. W., & Watson, A. C. (2002). Understanding the impact of stigma on people with mental illness. World Psychiatry: Official Journal of the World Psychiatric Association (WPA), 1(1), 16–20.
Dassori, A. M., Miller, A. L., & Saldana, D. (1995). Schizophrenia among Hispanics: Epidemiology, phenomenology, course, and outcome. Schizophrenia Bulletin, 21(2), 303–312. https://doi.org/10.1093/schbul/21.2.303
Dillon, F. R., De La Rosa, M., Rojas, P., Schwartz, S. J., & Duan, R. (2011). Attributions about addiction among Latina women. Journal of Social Work Practice in the Addictions, 11(3), 209–229.
Dorian, M., García, J. I. R., López, S. R., & Hernández, B. (2008). Acceptance and expressed emotion in Mexican American caregivers of relatives with schizophrenia. Family Process, 47(2), 215–228. https://doi.org/10.1111/j.1545-5300.2008.00249.x
Earl, T. R., Fortuna, L. R., Gao, S., Williams, D. R., Neighbors, H., Takeuchi, D., & Alegría, M. (2015). An exploration of how psychotic-like symptoms are experienced, endorsed, and understood from the national Latino and Asian American study and national survey of American life. Ethnicity & Health, 20(3), 273–292. https://doi.org/10.1080/13557858.2014.921888
Eghaneyan, B. H., & Murphy, E. R. (2020). Measuring mental illness stigma among Hispanics: A systematic review. Stigma and Health, 5(3), 351–363. https://doi.org/10.1037/sah0000207
Ellison, C. G., & Fan, D. (2007). Daily spiritual experiences and psychological well-being among US adults. Social Indicators Research, 88, 247–271.
Enders, C. K. (2010). Applied missing data analysis. The Guilford Press.
Falicov, C. J. (2009). Commentary: On the wisdom and challenges of culturally attuned treatments for Latinos. Family Process, 48(2), 292–309. https://doi.org/10.1111/j.1545-5300.2009.01282.x
Gearing, R. E. (2008). Evidence-based family psychoeducational interventions for children and adolescents with psychotic disorders. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 17(1), 2–11.
Gearing, R. E., Brewer, K. B., Cheung, M., Leung, P., Chen, W., & He, X. (2021a). Suicide in China: Community attitudes and stigma. OMEGA - Journal of Death and Dying. https://doi.org/10.1177/0030222821991313
Gearing, R. E., Washburn, M., Torres-Hostos, L. R., Carr, L. C., Cabrera, A., & Olivares, R. (2021b). Immigration policy changes and the mental health of Mexican American immigrants. Journal of Racial and Ethnic Health Disparities, 8(3), 579–588. https://doi.org/10.1007/s40615-020-00816-5
Givens, J. L., Houston, T. K., Van Voorhees, B. W., Ford, D. E., & Cooper, L. A. (2007). Ethnicity and preferences for depression treatment. General Hospital Psychiatry, 29, 182–191. https://doi.org/10.1016/j.genhosppsych.2006.11.002
Gómez-de-Regil, L., Kwapil, T. R., & Barrantes-Vidal, N. (2014). Illness perception mediates the effect of illness course on the quality of life of Mexican patients with psychosis. Applied Research in Quality of Life, 9(1), 99–112. https://doi.org/10.1007/s11482-013-9211-4
Gonzalez, J. M., Alegria, M., & Prihoda, T. J. (2005). How do attitudes toward mental health treatment vary by age, gender, and ethnicity/race in young adults? Journal of Community Psychology, 33(5), 611–629. https://doi.org/10.1002/jcop.200471
Gonzalez, J. M., Alegría, M., Prihoda, T. J., Copeland, L. A., & Zeber, J. E. (2011). How the relationship of attitudes toward mental health treatment and service use differs by age, gender, ethnicity/race and education. Social Psychiatry and Psychiatric Epidemiology, 46(1), 45–57. https://doi.org/10.1007/s00127-009-0168-4
Guarnaccia, P. J., MartínezPincay, I., Alegría, M., Shrout, P. E., Lewis-Fernández, R., & Canino, G. J. (2007). Assessing diversity among Latinos: Results from the NLAAS. Hispanic Journal of Behavioral Sciences, 29(4), 510–534. https://doi.org/10.1177/0739986307308110
Hamilton, J. E., Heads, A. M., Meyer, T. D., Desai, P. V., Okusaga, O. O., & Cho, R. Y. (2018). Ethnic differences in the diagnosis of schizophrenia and mood disorders during admission to an academic safety-net psychiatric hospital. Psychiatry Research, 267, 160–167. https://doi.org/10.1016/j.psychres.2018.05.043
Hardy, M. A. (1993). Regression with dummy variables. Sage.
Himmelstein, M. S., & Puhl, R. M. (2021). At multiple fronts: Diabetes stigma and weight stigma in adults with type 2 diabetes. Diabetic Medicine, 38(1), e14387. https://doi.org/10.1111/dme.14387
Hirai, M., Vernon, L. L., Popan, J. R., & Clum, G. A. (2015). Acculturation and enculturation, stigma toward psychological disorders, and treatment preferences in a Mexican American sample: The role of education in reducing stigma. Journal of Latina/o Psychology, 3, 88–102. https://doi.org/10.1037/lat0000035
Hirsch, L., Yang, J., Bresee, L., Jette, N., Patten, S., & Pringsheim, T. (2017). Second-generation antipsychotics and metabolic side effects: A systematic review of population-based studies. Drug Safety, 40(9), 771–781. https://doi.org/10.1007/s40264-017-0543-0
Jimenez, D. E., Bartels, S. J., Cardenas, V., & Alegría, M. (2013). Stigmatizing attitudes toward mental illness among racial/ethnic older adults in primary care. International Journal of Geriatric Psychiatry, 28, 1061–1068. https://doi.org/10.1002/gps.3928
Laursen, T. M., Nordentoft, M., & Mortensen, P. B. (2014). Excess early mortality in schizophrenia. Annual Review of Clinical Psychology, 10, 425–448. https://doi.org/10.1146/annurev-clinpsy-032813-153657
Lewis-Fernández, R., Horvitz-Lennon, M., Blanco, C., Guarnaccia, P. J., Cao, Z., & Alegría, M. (2009). Significance of endorsement of psychotic symptoms by US Latinos. Journal of Nervous and Mental Disease, 197(5), 337–347. https://doi.org/10.1097/NMD.0b013e3181a2087e
Link, B. G., Phelan, J. C., Bresnahan, M., Stueve, A., & Pescosolido, B. A. (1999a). Public conceptions of mental illness: Labels, causes, dangerousness, and social distance. American Journal of Public Health, 89(9), 1328–1333. https://doi.org/10.2105/AJPH.89.9.1328
López, S. R., Gamez, D., Mejia, Y., Calderon, V., Lopez, D., Ullman, J. B., & Kopelowicz, A. (2018). Psychosis literacy among Latinos with first-episode psychosis and their caregivers. Psychiatric Services, 69(11), 1153–1159. https://doi.org/10.1176/appi.ps.201700400
Lopez, S. R., Lara, M. D. C., Kopelowicz, A., Solano, S., Foncerrada, H., & Aguilera, A. (2009). “La CLAve” to increase psychosis literacy of Spanish-speaking community residents and family caregivers. Journal of Consulting and Clinical Psychology, 77(4), 763–774.
Luoma, J. B., Twohig, M. P., Waltz, T., Hayes, S. C., Roget, N., Padilla, M., & Fisher, G. (2007). An investigation of stigma in individuals receiving treatment for substance abuse. Addictive Behaviors, 32(7), 1331–1346. https://doi.org/10.1016/j.addbeh.2006.09.008
National Alliance on Mental Illness (2021). Mental Health By the Numbers. https://www.nami.org/mhstats#:~:text=Schizophrenia%3A%20%3C1%25%20(estimated,%25%20(estimated%2048%20million%20people)
National Institute on Mental Health (2020). Schizophrenia. https://www.nimh.nih.gov/health/topics/schizophrenia
Magaña, S. M., García, J. I. R., Hernández, M. G., & Cortez, R. (2007). Psychological distress among Latino family caregivers of adults with schizophrenia: The roles of burden and stigma. Psychiatric Services, 58(3), 378–384. https://doi.org/10.1176/appi.ps.58.3.378
Mangurian, C., Schillinger, D., Newcomer, J. W., Vittinghoff, E., Essock, S., Zhu, Z., Dyer, W., Young-Wolff, K. C., & Schmittdiel, J. (2020). Comorbid diabetes and severe mental illness: Outcomes in an integrated health care delivery system. Journal of General Internal Medicine, 35(1), 160–166. https://doi.org/10.1007/s11606-019-05489-3
Marin, G., & Gamba, R. J. (1996). A new measurement of acculturation for Hispanics: The bidimensional acculturation scale for Hispanics (BAS). Hispanic Journal of Behavioral Sciences, 18(3), 297–316.
Mascayano, F., Tapia, T., Schilling, S., Alvarado, R., Tapia, E., Lips, W., & Yang, L. H. (2016). Stigma toward mental illness in Latin America and the Caribbean: A systematic review. Revista Brasileira De Psiquiatria, 38, 73–85. https://doi.org/10.1590/1516-4446-2015-1652
McNeish, D., & Wolf, M. G. (2020). Thinking twice about sum scores. Behavior Research Methods, 52, 2287–2305. https://doi.org/10.3758/s13428-020-01398-0
Moreira-Almeida, A., & Cardeña, E. (2011). Differential diagnosis between non-pathological psychotic and spiritual experiences and mental disorders: A contribution from Latin American studies to the ICD-11. Brazilian Journal of Psychiatry, 33, s21–s28.
Nemani, K., Li, C., Olfson, M., Blessing, E. M., Razavian, N., Chen, J., Petkova, E., & Goff, D. C. (2021). Association of psychiatric disorders with mortality among patients with COVID-19. JAMA Psychiatry, 78(4), 380–386. https://doi.org/10.1001/jamapsychiatry.2020.4442
Nielsen, J., Skadhede, S., & Correll, C. U. (2010a). Antipsychotics associated with the development of type 2 diabetes in antipsychotic-naive schizophrenia patients. Neuropsychopharmacology, 35(9), 1997–2004. https://doi.org/10.1038/npp.2010.78
Oh, H., Yang, L. H., Anglin, D. M., & DeVylder, J. E. (2014). Perceived discrimination and psychotic experiences across multiple ethnic groups in the United States. Schizophrenia Research, 157(1–3), 259–265.
Olfson, M., Gerhard, T., Huang, C., Crystal, S., & Stroup, T. S. (2015). Premature mortality among adults with schizophrenia in the United States. JAMA Psychiatry, 72(12), 1172–1181. https://doi.org/10.1001/jamapsychiatry.2015.1737
Parcesepe, A. M., & Cabassa, L. J. (2013). Public stigma of mental illness in the United States: A systematic literature review. Administration and Policy in Mental Health and Mental Health Services Research, 40(5), 384–399. https://doi.org/10.1007/s10488-012-0430-z
Pescosolido, B. A., Martin, J. K., Long, J. S., Medina, T. R., Phelan, J. C., & Link, B. G. (2010). ‘“A disease like any other”’? A decade of change in public reactions to schizophrenia, depression, and alcohol dependence. The American Journal of Psychiatry, 167(11), 1321–1330. https://doi.org/10.1176/appi.ajp.2010.09121743
Rojas-Vilches, A., Negy, C., & Reig-Ferrer, A. (2011). Attitudes toward seeking therapy among Puerto Rican and Cuban American young adults and their parents. International Journal of Clinical and Health Psychology, 11, 313–341.
Savage, J. E., & Mezuk, B. (2014). Psychosocial and contextual determinants of alcohol and drug use disorders in the national Latino and Asian American study. Drug and Alcohol Dependence, 139, 71–78.
Smith, M., Hopkins, D., Peveler, R. C., Holt, R. I. G., Woodward, M., & Ismail, K. (2008). First-v. second-generation antipsychotics and risk for diabetes in schizophrenia: Systematic review and meta-analysis. The British Journal of Psychiatry, 192(6), 406–411. https://doi.org/10.1192/bjp.bp.107.037184
Turan, J. M., Elafros, M. A., Logie, C. H., Banik, S., Turan, B., Crockett, K. B., Pescosolido, B., & Murray, S. M. (2019). Challenges and opportunities in examining and addressing intersectional stigma and health. BMC Medicine, 17(1), 1–15. https://doi.org/10.1186/s12916-018-1246-9
Underwood, L. G. (2011). The daily spiritual experience scale: Overview and results. Religions, 2(1), 29–50. https://doi.org/10.3390/rel2010029
Underwood, L. G., & Teresi, J. A. (2002). The daily spiritual experience scale: Development, theoretical description, reliability, exploratory factor analysis, and preliminary construct validity using health-related data. Annals of Behavioral Medicine, 24(1), 22–33.
Valdez, C. R., Dvorscek, M. J., Budge, S. L., & Esmond, S. (2011). Provider perspectives about Latino patients: Determinants of care and implications for treatment. The Counseling Psychologist, 9(4), 497–526. https://doi.org/10.1177/0011000010385012
Yang, L. H., Chen, F. P., Sia, K. J., Lam, J., Lam, K., Ngo, H., Lee, S., Kleinman, A., & Good, B. (2014). “What matters most:” a cultural mechanism moderating structural vulnerability and moral experience of mental illness stigma. Social Science & Medicine, 1982(103), 84–93. https://doi.org/10.1016/j.socscimed.2013.09.009
Funding
This project was funded in part by the National Institutes of Health, National Institute on Drug Abuse, University of Houston Drug Abuse Research Development Program-II (R24 DA019798-09).
Author information
Authors and Affiliations
Contributions
REG—Study conceptualization, selection of study measures, creation of randomization scheme and vignette development, coordination of participant recruitment sites, manuscript editing; oversight of study research assistants and data entry, manuscript writing and editing; KBB—study conceptualization, selection of study measures, creation of randomization scheme and vignette development, data analysis, manuscript editing; MW—data entry, data analysis, manuscript editing; LCC—data analysis, manuscript writing and editing; SB—literature review, manuscript writing and editing; KM—literature review, manuscript writing and editing; LRTH—selection and translation of study measures, coordination of participant recruitment sites, manuscript editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest or competing interests to disclose.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board of the University of Houston, Approval # STUDY00000130, entitled, Engaging Latinos in Mental Health Services.
Consent to Participate
Informed consent was obtained from all individual participants included in the study. The IRB at the University of Houston granted a waiver of documented written consent for this project. Participants gave verbal consent to participate.
Consent for Publication
The authors consent for these materials to be published.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gearing, R.E., Brewer, K.B., Washburn, M. et al. Public Stigma Toward Schizophrenia Within Latino Communities in the United States. Community Ment Health J 59, 915–928 (2023). https://doi.org/10.1007/s10597-022-01075-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10597-022-01075-w