
Abstract
During adolescence, youth may experience heightened attention bias to socially relevant stimuli; however, it is unclear if attention bias toward social threat may be exacerbated for adolescents with a history of anxiety. This study evaluated attentional bias during the Chatroom-Interact task with 25 adolescents with a history of anxiety (18F, Mage = 13.6) and 22 healthy adolescents (13F, Mage = 13.8). In this task, participants received feedback from fictional, virtual peers who either chose them (acceptance) or rejected them (rejection). Overall, participants were faster to orient toward and spent longer time dwelling on their own picture after both rejection and acceptance compared to non-feedback cues. Social feedback was associated with greater pupillary reactivity, an index of cognitive and emotional neural processing, compared to non-feedback cues. During acceptance feedback (but not during rejection feedback), anxious youth displayed greater pupil response compared to healthy youth, suggesting that positive feedback from peers may differentially influence youth with a history of an anxiety disorder.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anxiety is one of the most common problems in children and adolescents, with an estimated 15–20% of youth meeting criteria for an anxiety disorder [1]. In childhood and adolescence, anxiety disorders are often associated with both academic and social impairment [2]. Although psychotherapeutic treatments are considered efficacious for anxious youth, about 40% of anxious youth do not adequately respond to treatment [3] and many relapse following treatment [4]. Consequently, many previously-treated anxious youth still experience significant levels of anxiety and are still at elevated risk for recurrence relative to the general population. Examining how previously-treated anxious youth may differ from youth without a history of an anxiety disorder could uncover potential treatment targets that existing interventions may not address.
Cognitive Models of Anxiety Disorders
Cognitive models of anxiety have implicated biases occurring in multiple stages of information processing in the acquisition and maintenance of anxiety; however, most anxiety research focuses on biases in attention [5, 6]. Broadly, information processing refers to the steps by which information is relayed through cognitive processes such as attention, memory, and interpretation [7]. Cognitive biases arise when individuals’ information processing systematically favors or preferentially processes certain types of information. Many information-processing models of anxiety disorders consider cognitive biases to occur both automatically and strategically during information processing [5, 8,9,10].
According to Beck and Clark’s cognitive model, cognitive biases (i.e., in attention, memory, and interpretation) are theorized to contribute to the onset of anxiety disorders and, thus, are often considered to be targets for treatment. While there is strong evidence for biased attention toward threat in anxiety disorders [8], there is less support for other types of cognitive biases (e.g., memory) in anxiety disorders [9]. Additionally, attention biases have been implicated in downstream dysfunctional information processing (e.g., negative interpretation bias) in individuals with anxiety disorders, further demonstrating their importance in cognitive models of anxiety [5, 11]. While biased attentional processes have been implicated in the etiology and maintenance of anxiety disorders for decades [12, 13], there are conflicting findings about the direction of attention biases in anxiety, particularly in children [14]. Generally, attention biases are assessed using paradigms that lack ecological validity (i.e., computer paradigms that use adult faces), particularly for studying child and adolescent populations [15]. Paradigms that tap into every day social processes occurring in adolescence may better mimic real-world attentional processing and serve to validate existing models of attention bias in anxiety.
Attentional Models
The hypervigilance model of attention suggests that individuals with anxiety more easily detect threat in the environment and more quickly orient their attention toward threat compared to individuals without anxiety [5]. A meta-analytic review has shown that clinically anxious adults display hypervigilance toward external threatening stimuli compared to non-anxious adults during initial, automatic stages of processing [8]; however a recent meta-analysis showed that clinically anxious adults do not exhibit such bias across studies that examined adults before receiving an intervention designed to target attention biases [16]. While there are equivocal findings when studying attention bias in children and adolescents, studies generally reveal that anxious youth display an attention bias toward threat compared to non-anxious youth [8, 17]; however, it is unclear if the bias is occuring at the initial orienting stage of attention or later in attentional processing.
Although most research on attention bias has focused on initial orienting of attention, shifting of attention after orientation is also an important process that could be altered in youth with anxiety [18]. Both the vigilance-avoidance model [11] and the attention-maintenance model [19] have been purported to characterize anxious individuals’ pattern of attention toward threatening stimuli beyond the initial orienting stage. While the vigilance-avoidance model predicts that attention is initially directed quickly to threat and later is directed away from threat, the attention-maintenance model predicts that once attention is directed toward threatening stimuli, it takes longer to look away due to difficulty disengaging attention from threat. This model suggests that there may be a sustained form of biased processing occurring in anxious individuals. Similar to pediatric work on the hypervigilance model described above, the limited research conducted in anxious and healthy youth populations has found mixed results for both models when assessing the time course of attention. While one eye-tracking task in a sample of youth (aged 8–13) with separation anxiety disorder has tenuously supported the vigilance-avoidance model [20], other research has only shown support for the hypervigilance model (i.e., no evidence of anxious youth being significantly more avoidant than non-anxious youth at later stages) using eye-tracking studies [21,22,23,24] in samples of both children and adolescents.
Several studies have examined if problematic attention biases are reduced following psychotherapy intervention. While multiple studies have shown that attention biases toward threat are reduced following psychotherapeutic interventions in adults [25,26,27], studies of treated youth have not demonstrated that attention biases are ameliorated following therapy [28, 29]. Therefore, psychotherapy may not sufficiently mitigate attention biases to threat in anxious youth, which could leave treated anxious youth at risk for future psychopathology.
Limitations of Attention Bias Research in Youth
Discrepancies in findings in research on anxious youth may be due to limitations in the attention bias literature, most notably that research on attention biases in youth relies primarily on computer paradigms that tend to use static, adult faces. Given that adolescence is often characterized as a period of heightened sensitivity to peer relationships [30], researchers have recently begun to examine how anxious youth respond to more realistic social feedback from their own peers. However, these ecologically valid paradigms have not yet been incorporated into attention bias research. Ecologically valid paradigms can help us better understand attentional and emotional processing of peer feedback, which is of particular importance in adolescence. The developmental stage of adolescence is marked by an increased amount of time spent with peers [31] and a rise in peer rejection, due to more volatile relationships occurring during this life-stage [32]. Anxious adolescents are particularly vulnerable, given that they are at an increased risk for having poorer peer relations and experiencing peer victimization [33, 34]. Therefore, studying cognitive processes using ecologically valid peer evaluation stimuli may provide us with greater insight into how anxious and healthy youth differ in attention to real-life threatening and rewarding stimuli, such as rejection or acceptance by peers. Thus, for the social threat stimulus in this study, we used participants own photo with a large “X” superimposed, which signifies being rejected by a peer. By using the participant’s own photo rather than a photo of adult strangers, as previous research on attention bias has used, we aimed to enhance the ecological validity of attention bias tasks. Although viewing an image of yourself after being accepted or rejected by a peer differs in important ways from threat embodied in unknown happy and angry faces, it does capture a similar valence bias in attentional processing. Therefore, in order to integrate the results from this study with the wider threat bias literature we will consider self-viewing after rejection and acceptance as similar to social threat and reward bias.
While most researchers studying attention have used reaction time indices to assess attention allocation, critics have pointed out that manual reaction time studies do not delineate the true time course of attention, due to the time that it takes to enact the motor coordination needed to make a manual hand response [35]. Eye movements are guided by selective attention shifts [36], making them a more proximal measure of attention than manual, motor responses. Eye-tracking technology allows for measurement of overt, visual attention over the course of seconds. Furthermore, eye-tracking indices on attention tasks have been shown to more reliably measure attention bias compared to standard reaction time measures [37]. For these reasons, the current study used eye-tracking methodology to compute initial time to fixate and duration of time spent on socially-threatening stimuli, the participant’s own, crossed out face.
Pupillary Measurement
The present study utilized pupillary measurements as an additional assessment of cognitive and affective processing. The pupillary response is a temporally sensitive physiological measure that is thought to index overall cognitive load, including both emotional and cognitive processing [38] and is thought to capture sustained neural attention biases [39]. Pupil dilation has been shown to be associated with neural activation related to emotional reactivity (i.e. amygdala) as well as cognitive control (i.e. prefrontal cortex) [40, 41]. The pupil becomes increasingly dilated during tasks that require greater cognitive load or increased emotional intensity [41,42,43]. Pupil dilation has thus been used as a proxy for neural activity in brain regions subserving cognitive and emotional information processing, conveying information on both the time-course and magnitude of neural responses [44]. For example, after viewing negative, personally-relevant stimuli, adults with depression showed a greater sustained increase in pupil dilation compared to individuals without depression, suggesting that pupil dilation may index preservative forms of negative self-focused attention, such as rumination [38].
Examining pupil dilation after the presentation of negative social stimuli can provide complementary information on attentional processing in youth, providing a richer understanding of the intensity and time-course of neural engagement in the context of threatening stimuli. Recent research has demonstrated that anxious and healthy adolescents differ in their neural responses to peer rejection and peer acceptance. In a task similar to the current study, clinically anxious adolescents had heightened amygdala-hippocampal activation following peer rejection compared to non-anxious adolescents, but no differences between groups during peer acceptance feedback [45]. In another study, adolescents identified as having a stable, behaviorally inhibited temperament, a known risk factor for social anxiety disorder, had a blunted striatal response to peer acceptance compared to peers without a behaviorally inhibited temperament [46]. Thus, while there is evidence that youth at high-risk for anxiety and currently anxious youth have differing neural responses to peer feedback, it is unknown whether there are attentional alterations underlying these differences in neural responses. The goals of the study were to examine how youth with a history of anxiety and healthy youth vary in both their attentional and pupillary response—a peripheral index of neural activity—to socially threatening stimuli.
Researchers have begun to study eye-tracking and pupillary reactivity to peer rejection and acceptance in healthy youth. Silk et al. [47] collected eye-tracking and pupillometry measures in healthy youth (aged 9–17) to understand cognitive and emotional responses to social feedback using the same task that was used in the present study, the Chatroom-Interact task. In this task, youth are sometimes chosen (i.e. “accepted”) by fictional peers to talk about a common teen interest (e.g., music, TV), and sometimes not chosen (i.e. “rejected”). The researchers found that when healthy youth were accepted, they tended to focus on a picture of themselves for the duration of the trial. However, when they were rejected (as indicated by a large gray “X” through their self-photo), healthy youth avoided looking at their self-photo. For youth, viewing their self-photo after being rejected by a peer may be associated with negative emotion and social ‘threat’ and disengaging attention away from the threat may be protective. Therefore, the self-photo acts as either social threat or social reward, depending on the context. Furthermore, healthy youth who reported lower levels of closeness and connection during real-world social interactions with peers were more likely to have greater pupillary response in the wake of rejection, suggesting that youths’ rejection sensitivity may be related to reduced feelings of social connectedness.
Present Study
The goal of the current study was to use eye-tracking and pupillary measures during the Chatroom-Interact task to examine vigilance to and later avoidance or disengagement from social threat in youth with a history of anxiety and non-anxious youth. Anxious youth were treated for anxiety 2 years prior to the current study with either cognitive-behavioral therapy (CBT) or a supportive child-centered therapy (CCT). Although all anxious youth received treatment, there remained significant variability in levels of anxiety at the time of the present study (refer to Table 1). For all youth, we predicted that rejection feedback would capture attention; however, we expected the response to be modulated by a history of an anxiety disorder. Specifically, we expected that previously-treated anxious youth would be faster to orient to their socially threatening, self-focused stimuli relative to non-anxious youth. Due to lack of evidence for either the delayed disengagement model or vigilance-avoidance model, we did not hypothesize a specific direction of attention bias after the initial allocation of attention. Additionally, we expected that youth with a history of anxiety disorder or current anxiety disorder would display greater pupil-dilation in the wake of rejection compared to non-anxious youth, as they may experience increased rejection sensitivity [48] and thus have to recruit more neural resources to disengage their attention following rejection. Exploratory eye-tracking analyses were conducted to examine if results were specific to rejection feedback, or if they generalized to positive evaluative feedback, such as acceptance feedback. Finally, to replicate previous attention research by Silk et al. [47] using this paradigm in healthy youth, we compared rejection trials to acceptance trials across attention and pupillary indices. In line with previous research, we expected that youth would spend longer looking at their self-photo when accepted compared to when they were rejected and have greater pupillary response following rejection than compared to following acceptance by peers.
Methods
Participants
Participants were 28 youth with anxiety disorders whom, 2-years prior to the present study, completed a psychotherapy treatment through a randomized controlled trial at the University of Pittsburgh (see [49, 50] for full study procedures), and 27 healthy youth with no lifetime psychological disorders. Participants ranged in age from 11 to 16 years at the time of the present study. They were previously recruited for the original study through radio, television, and newspaper advertisements, and referrals from pediatricians, school counselors, and mental health clinics. At the pre-treatment time-point, all anxious participants met DSM-IV diagnostic criteria for generalized anxiety disorder, social phobia, and/or separation anxiety disorder as determined by the Kiddie-Schedule for Affective Disorders and Schizophrenia—Present and Lifetime version (K-SADS-PL) [51]. Healthy participants met no DSM-IV diagnostic criteria for any psychiatric disorder.
At the pre-treatment time-point, exclusion criteria for all participants included a current primary diagnosis of major depressive disorder, a current diagnosis of obsessive–compulsive disorder, post-traumatic stress disorder, conduct disorder, substance abuse or dependence, attention deficit hyperactivity disorder combined type or predominantly hyperactive-impulsive type, evidence of an autism spectrum disorder, or a lifetime diagnosis of bipolar disorder, psychotic depression, schizophrenia, or schizoaffective disorder. Exclusion criteria at the pre-treatment time-point also included an IQ below 70 as assessed by the Wechsler Abbreviated Scale of Intelligence [52], use of psychoactive medications, acute suicidality or risk for harm to self or others, and, because the larger study included a functional magnetic resonance imaging (fMRI) scan, presence of metal braces or other metal objects in their body or history of serious head injury. Finally, participants were excluded from the study if they had problems with their eyes or difficulties in vision not corrected by the use of contacts or glasses at pre-treatment and at time of the current study.
At time of the current study, five anxious participants met full criteria for a current anxiety disorder, one participant met criteria for combined-type attention deficit hyperactivity disorder (ADHD), and 16 previously-treated anxious participants met no current DSM-IV diagnostic criteria. Healthy participants continued to not meet DSM-IV diagnostic criteria for any psychological disorder.
Procedure
The study was approved by the University of Pittsburgh’s Institutional Review Board. At the pre-treatment time-point, all participants were scheduled for an assessment during which a master’s level interviewer administered the K-SADS-PL and questionnaires to the child and his/her primary caregiver. Anxious youth were subsequently randomized to treatment, with a 2:1 ratio for assignment to CBT versus CCT (see [3] for pre-treatment and therapy procedures). There remained a range of anxious symptoms at the present time point (2 years after treatment) using clinician report, child self-report, or parent-report (refer to Table 1). The K-SADS-PL and questionnaires were re-administered at the time-point of the current assessment, a 2-year follow-up. Participants also completed the Chatroom-Interact task at the time of the current assessment.
Measures
Diagnostic Assessment
On their first pre-treatment visit, each youth and his or her parent(s) were interviewed using the KSADS-PL. Parents and youth were interviewed separately, with interviewers integrating data from both informants to determine the final diagnosis. All in-terviews were carried out by trained master’s level clinicians. The results of the interview were presented at a consensus case conference with a child psychiatrist, who reviewed the findings and preliminary diagnosis and provided a final diagnosis based on DSM-IV [53] criteria. Inter-rater reliability was calculated for 16% of interviews. Reliability for anxiety diagnoses was high (Kappa = 0.97). The K-SADS-PL was administered again at post-treatment, 1, and 2-year follow-up by master’s level clinicians.
Screen for Child Anxiety Related Emotional Disorders
Anxiety severity was assessed at pre-treatment and at 2-year follow-up using the Screen for Child Anxiety Related Emotional Disorders, Child (SCARED-C) versions [54]. The full-scale, self-report measure assessed DSM-IV symptoms of panic, separation anxiety disorder, social phobia, generalized anxiety disorder, and school refusal. It has been demonstrated to have good psychometric properties in clinical [55] and community samples [56], and exhibited excellent internal consistency in the current sample; α = 0.93).
Pupil and Eye-Tracking Assessment
Participants sat approximately 68 cm from the monitor to complete the Chatroom-Interact task, which was programmed using Eprime software (Psychology Software Tools, Inc). Eye-tracking and pupil data were collected using a table-mounted RK-464 eye-tracker, which consisted of a video camera and infrared light source pointed at participants’ eyes and a device that tracked location and size of the pupil. These data were recorded at 60 Hz (every 16.7 ms) and circulated digitally from the eye-tracker to a computer that accumulated the acquired data. Participants completed a nine-point calibration procedure before beginning the Chatroom-Interact task.
Chatroom-Interact Task
The Chatroom-Interact task was designed by Silk et al. [47] to examine reactions to social acceptance and rejection from virtual peers in an online setting. The task consisted of two phases on two separate days at the 2-year follow-up. On the first day, participants were told they would interact online with several youth their own age at remote sites on their next lab visit. Participants were asked to view the smiling photos and standardized biographical profiles of the age-matched youth (virtual peers) they would have the potential to meet virtually. The photos of virtual peers were of child actors and/or youth residing in a different state who had consented to be photographed by a photographer. Participants were asked to pick the top five youth of the same sex that they would be interested in meeting, based on the photos and biographical profiles they viewed. Participants were asked to complete their own biographical profile by filling out a questionnaire and to have their photo taken so that the other virtual participants at the remote locations could review their profile and see their picture.
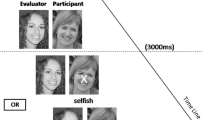
Approximately 2 weeks after the diagnostic assessment at the 2-year follow-up, participants completed the interaction phase of the task. Participants were told that they had been matched with two same-sex youth selected from the first visit and that these peers were ready to participate in a “chat game” via a remote connection. Participants reviewed the profiles and photos from the selected peers. In the task, participants reviewed pictures of the peers and their own photo on a screen, seeing their own picture and one peer’s picture on the screen concurrently. The participant and two virtual peers took turns selecting who they would rather talk to about a series of common interests (e.g., music, television). The photograph of the agent (the one choosing) was shown at the bottom left corner of the screen while the other two players’ photographs were shown in the middle of the screen. For each trial, the agent (either the participant or a virtual peer) is asked to choose who they would rather discuss a topic with (e.g., “Who would you rather talk to about music?”) for 3.3 s (Fig. 1). The question sentence was presented at the bottom of the screen. When the participant was rejected, a gray “X” was superimposed on the participants’ self-photo for 10 s. During trials in which the participant was chosen to discuss a topic (acceptance trials), the participant’s self-photo was highlighted with a gray box. Participants were asked to indicate, using a button-press, whether the person on the left or right was chosen in order to maintain task engagement. At the end of the task, participants completed 15 control trials in which they had to indicate which face (self-picture or a peer) had a dot superimposed on it using a button-press (Fig. 2). This condition was included as a visual, cognitive, and motor control.

Depiction of trial on Chatroom Interact task

Depiction of control trial on Chatroom Interact task
The task was conducted throughout six blocks. Each block was comprised of 15 trials in which a person was chosen or not chosen as the preferred person to discuss each topic. Topics were presented randomly and repeated in each block. Trials were arranged in blocks so that participants experienced two accept blocks in which they were chosen two-thirds of the time and two reject blocks in which they were rejected two-thirds of the time. During the remaining two blocks, the participants made choices who to talk to from pairs of virtual peers.
Post-task Debriefing
Following the Chatroom-Interact task, all participants were debriefed and informed that in reality they had been playing with a preset computer program. All participants were successfully deceived, as determined by a debriefing interview.
Data Cleaning and Processing
Data were cleaned using standard procedures [57], in which blinks are identified and interpolated throughout. Participants (n = 7; 5 anxious youth, 2 healthy youth) were excluded from analyses if they had less than 70% usable trials or if data exhibited drift from initial calibration (n = 1; 1 anxious youth), leaving a total of 22 anxious youth and 25 healthy youth in the final dataset. Excluded participants did not significantly differ from included participants on any demographic or clinical measurement (ps > 0.05). Included participants’ demographics are presented in Table 1.
For eye-tracking analyses, the X and Y-gaze coordinates were examined as an index of whether the participant was looking at their self-photo or the virtual peer’s photo. Latency to look at the self-photo was calculated as time taken (ms) to fixate on the self-photo after presentation of feedback stimuli. The dwell-time index was measured as the percent duration of total trial time that participants spent looking at their self-photo and percent duration of total trial time spent looking at the peer photo during feedback.
Pupil dilation was calculated by subtracting the baseline pupil diameter from the pupil diameter during the trial. Baseline pupil measurements were calculated by using the first 10 samples (167 ms) of each trial, in which participants were simply viewing the virtual peers’ photos. Mean pupil change was examined in the period in which participants looked at their self-photo in the immediate aftermath of rejection (0–2 s after receiving rejection feedback), as well as mean pupil dilation for a later portion of the trial (2–5.7 s after receiving rejection feedback). The early period was selected because previous research examining pupil dilation using the Chatroom-Interact Task found peak pupil change to occur during this time interval (0–2 s after feedback), and the late period was chosen to end at 5.7 s post feedback to increase the comparability to the previous Chatroom-Interact study [47]. Finally, for control trials, average pupil dilation was calculated across all control trials during identical early and late windows. These indices allow for examining pupillary reaction during early stages of processing and later stages of processing, in which ruminative processing may be occurring.
Data Analysis
Baseline demographic characteristics such as age, sex, and race were analyzed using analysis of variance (ANOVA) models for continuous variables and Chi square tests for nominal/categorical variables.
All analyses were conducted using data measured at the 2-year post-treatment time-point. To examine the main effect of trial-type and the interaction of history of anxiety and trial-type for latency to look at self-photo and dwell-time index, several rANOVA’s were used with history of anxiety (anxious, healthy) as the between-subject factors and trial-type (rejected or acceptance trials, control trials) as the within-subjects factor. Parallel rANOVA tests were run to probe the main effect of trial-type and the interaction of history of anxiety by trial-type for pupil dilation. Additional parallel rANOVA tests were run to directly compare rejection to acceptance trials (rather to control trials). Furthermore, sensitivity analyses were conducted to examine if excluding participants with clinical levels of anxiety changed the pattern of results.
Results
Demographics
A one-way ANOVA with a between-group factor of history of anxiety revealed no significant differences in age between the two groups, F(1, 46) = 0.11, p = 0.74. Chi square tests revealed that there were more girls in the anxious than healthy group, χ(1) = 4.63, p = 0.03, but there were no significant differences in race distribution between the two groups, χ(3) = 0.3, p = 0.35.
Rejection Analyses
Latency Analyses
The rANOVA analysis with history of anxiety (anxious, healthy) as a between-subjects variable and trial-type (rejection, control) as a within-subjects variable revealed a main effect of trial-type, F(1, 43) = 5.52, p = 0.02, ƞ 2p = 0.11 on median latency to look at self-photo. The main effect indicated that youth were faster at orienting toward their self-photo during rejection trials compared to control trials, as predicted. There was no significant interaction of history of anxiety by trial-type, F(1, 43) = 1.2, p = 0.28, ƞ 2p = 0.03, contrary to hypotheses.
Dwell-Time Analyses
The rANOVA examining the interaction of history of anxiety (anxious, healthy) by trial-type (rejection, control) on dwell-time revealed a main effect of trial-type, F(1, 45) = 21.36, p < 0.001, ƞ 2p = 0.32. As predicted, youth spent a longer time looking at the self-photo during rejection trials compared to control trials (see Table 2 for uncorrected means). There was no significant interaction of history of anxiety by trial-type, F(1, 45) = 0.003, p = 0.96, ƞ 2p = 0.00, contrary to hypotheses.
Pupil Indices
The rANOVA examining early and late pupil dilation during rejection and control trials revealed main effects of trial-type, F(1, 45) = 17.52, p < 0.01, ƞ 2p = 0.28 and F(1, 45) = 18.64, p < 0.01, ƞ 2p = 0.29, respectively, indicating there was greater pupil dilation for rejection trials compared to control trials for both early and late time periods. However, there was no significant interaction of history of anxiety by trial-type or main effect for either early, F(1, 45) = 1.73, p = 0.20, ƞ 2p = 0.04, or late periods, F(1, 45) = 2.79, p = 0.10, ƞ 2p = 0.06.
Acceptance Analyses
Latency Analyses
The rANOVA analysis to measure the main effect of trial-type and interaction of history of anxiety by trial-type for median latency to look at self-photo during acceptance versus control trials yielded no significant main effects or interaction effects, ps > 0.05.
Dwell-Time Analyses
The rANOVA analysis to measure the main effect of trial-type and interaction of history of anxiety by trial-type for the dwell-time index during acceptance and control trials revealed a main effect of trial-type, F(1, 45) = 5.27, p = 0.03, ƞ 2p = 0.11. Similar to the rejection results, youth spent a longer time looking at the self-photo on acceptance trials compared to control trials (see Table 2 for uncorrected means). There was no significant interaction of history of anxiety by trial-type, F(1, 45) = 1.12, p = 0.30, ƞ 2p = 0.02, when examining acceptance versus control trials.
Pupil Indices
The rANOVA examining early pupil dilation in acceptance and control trials, indicated an interaction of history of anxiety by trial-type, F(1, 45) = 4.86, p = 0.03. ƞ 2p = 0.10, unlike in the rejection analyses (see Fig. 3). Post-hoc pairwise comparisons revealed that the anxious youth had significantly greater early pupil dilation during acceptance trials compared to control trials, p < 0.01. Similar to the rejection trial analyses, the rANOVAs examining late pupil dilation revealed a main effects of trial-type, F(1, 45) = 13.66, p < 0.01, ƞ 2p = 0.23, indicating there was greater pupil dilation for rejection and acceptance compared to control trials for late pupil dilation. Furthermore, there was a trend-level interaction of history of anxiety by trial-type in predicting late pupil dilation, F(1, 45) = 3.92, p = 0.054, ƞ 2p = 0.08.

Effects of diagnostic group and trial-type on change in early pupil dilation. There was a significant interaction of diagnostic group by trial-type. The interaction showed that anxious children had significantly greater pupil dilation in acceptance trials compared to control trials. *p < 0.01, error bars represent ± SEM
Rejection Compared to Acceptance Analyses
Latency Analyses
The rANOVA analysis to measure the main effect of trial-type (rejection, acceptance) and interaction of history of anxiety by trial-type for median latency to look at self-photo during acceptance versus control trials revealed a main effect of trial-type, F(1, 44) = 4.96, p = 0.03, ƞ 2p = 0.10, such that youth were faster to orient to themselves during rejection trials compared to acceptance trials. There was no significant interaction of history of anxiety by trial-type, F(1, 44) = 3.03, p = 0.09, ƞ 2p = 0.06, when examining rejection versus acceptance trials.
Dwell-Time Analyses
The rANOVA analysis to measure the main effect of trial-type and interaction of history of anxiety by trial-type for the dwell-time index during rejection and acceptance trials revealed a main effect of trial-type, F(1, 45) = 45.47, p < 0.001, ƞ 2p = 0.50. Youth spent a longer time looking at their self-photo on acceptance trials compared to rejection trials, in line with the previous paper by Silk et al. [47]. There was no significant interaction of history of anxiety by trial-type, F(1, 45) = 0.44 p = 0.51, ƞ 2p = 0.01, when examining rejection versus acceptance trials.
Pupil Indices
The rANOVA analysis to measure the main effect of trial-type and interaction of history of anxiety by trial-type for pupil indices during rejection versus acceptance trials yielded no significant main effects or interaction effects, ps > 0.23, contrary to predictions.
Associations with Treatment Outcomes
Given that there were no main effects of history of anxiety, exploratory Pearson correlations were used to examine whether attentional and pupillary variables were associated with current anxiety severity and depressive severity. Dwell time, latency, and pupil indices were not associated with total anxiety (SCARED-C total score); generalized anxiety, social anxiety, and separation anxiety (scores on the SCARED-C subscales); total MFQ-C scores; or treatment response (ps > 0.09).
Sensitivity Analyses
All analyses were conducted again without the five subject that met criteria for a clinical anxiety disorder. The pattern of all results reported above were retained in the subset of participants (n = 17) who did not meet criteria for a current, clinical anxiety disorder.
Discussion
The current study examined how healthy youth and youth with a history of anxiety attend to rejection and acceptance by fictitious peers. Findings showed that, regardless of history of anxiety, negative social feedback from peers captures greater attention and is associated with greater pupillary reactivity compared to a non-feedback control condition in both youth with a history of an anxiety disorder and healthy youth. However, exploratory pupillometry analyses indicated that for positive feedback, unlike negative feedback, youth with a history of anxiety differed from healthy youth, in that anxious youth had greater pupil dilation in response to positive feedback compared to healthy youth.
In line with our predictions, both anxious and non-anxious youth fixated faster and spent a longer time fixating on their rejected self-photo (i.e., their own crossed out face), which is considered to be a social threatening stimulus, during social rejection compared to control trials. Negative emotionality associated with peer rejection may strongly capture and hold the attention of adolescents, making it difficult for them to look away from socially threatening feedback, even without deficits in attentional control. This interpretation is consistent with previous research showing that adolescents are more sensitive to rejection and social exclusion compared to preadolescents [58, 59], perhaps due to the increased prevalence of peer rejection occurring during adolescence [32, 60] and the emphasis placed on peer relationships during this developmental stage. Adolescents may spend a greater amount of time pondering why they might have been rejected, reflected in a longer time spent looking at their own crossed out, rejected face compared to looking at the face of their peer.
Findings suggest that history of an anxiety disorder did not appear to modulate response to rejection-feedback assessed via eye-tracking or pupillary measures. There could be several possible reasons for this null finding. First, findings from attention research in anxious youth have been more mixed compared to research in anxious adult populations [14, 17]. A recent meta-analysis found that while anxious youth show a significant bias toward threat-related stimuli and healthy youth do not exhibit such a bias, the difference between anxious and control groups is less pronounced in child populations compared to adult populations, and between-group differences of attention bias widens in older age groups [17]. Thus, attention biases are not as reliably found in youth and change across the span of development. However, it should be noted that most of our anxious youth did not meet current criteria for an anxiety diagnosis, which could have also affected our results. Second, it could be that biases are only elicited in certain experimental paradigms. In support of this possibility, it has been shown that attention bias effect sizes in anxious youth differ based on the paradigm utilized [17]. To this point, there were significant differences between this paradigm and the dot-probe paradigm, a more traditional assessment of attention bias. It is possible that the socially threatening stimulus used in the Chatroom-Interact paradigm might have been so captivating across all youth that subtle differences in attention between the groups were not detectable, unlike in other tasks that use photos of adult strangers, e.g., [21].
Contrary to our rejection findings, we found a group by condition interaction effect on pupillary response to acceptance trials. Specifically, anxious youth had larger pupil dilation in acceptance trials compared to control trials in the earlier part of the trial (0–2 s after feedback), which reflects initial reactivity to acceptance feedback. Healthy participants, on the other hand, did not differ in initial reactivity to acceptance versus control trials. Less research has examined reward processing compared to threat processing in anxious youth [14, 47]. In a task similar to the Chatroom-Interact task, researchers found that socially anxious adolescents (but not anxious adults or healthy adolescents or adults), showed greater striatal response when they received unexpected positive social feedback from peers [61]. Therefore, it may be that this high-risk sample of anxious youth may have been more surprised to receive positive, social feedback, given their proclivity to pessimistically anticipate social interactions [62], which may have been reflected in greater pupil dilation in anxious youth. Additionally, researchers found that young adults with depression and high rates of comorbid anxiety exhibited heightened amygdala response to peer acceptance feedback compared to the healthy control group [63]. Given that pupil dilation is innervated by limbic regions of the brain such as the amygdala and striatum [64], our pupillary findings may reflect a heightened limbic response to positive social feedback in anxious youth. This is consistent with findings that indicate that increasing levels of reward are associated with corresponding increases in pupil dilation [65]. In other studies, anxious children have demonstrated a hyperactive neural response to reward in fronto-striatal regions of the brain [45] that are implicated in reward processing and motivation [66]. Therefore, our finding that previously-treated anxious youth had significantly larger pupil dilation for acceptance compared to control trials (that was not found in healthy controls), may suggest a heightened sensitivity for reward in youth with a history of anxiety.
Finally, in order to compare results from a previous study using the same paradigm that assessed only healthy youth [57], we conducted the same attentional and pupillary analyses but compared rejection to acceptance trials. We did not replicate previous pupillary results, which found that youth had greater pupillary response in the wake of peer rejection compared to acceptance. However, we replicated the previous finding that youth spent a longer duration fixating on their self-photo during acceptance feedback compared to during rejection feedback. Focusing on positive feedback compared to negative feedback may serve as an emotion regulation strategy [57].
Limitations of the present study should be noted. First, due to our sample size (n = 47), we had limited ability to detect interactions with potential moderating variables. Post-hoc power analyses using G*Power [67] revealed that power to detect a medium effect size (Cohen’s f = 0.25) with our current variables was only 0.39; however, our power to detect a large effect (Cohen’s f = 0.40) was adequate (0.77). Future studies should examine whether age, sex, and/or puberty affect attentional processing in a larger sample of anxious and healthy youth. Age, in particular, may affect pupillary findings, as previous research has found that older youth had a greater pupillary response in the wake of peer rejection compared to younger youth [47]. Second, the majority of the anxious group (17 of 22 participants) no longer met full criteria for an anxiety disorder at the time of the assessment, limiting our capacity to generalize to currently anxious samples. Notably, our sensitivity analyses in which we excluded the five clinically anxious youth did not change our pattern of results. This suggests that history of anxiety disorder is meaningful even in the absence of current disorder. Finally, while this study provided a cross-sectional examination of attention and pupillary response to social feedback and history of anxiety, future prospective research is critical to examine how attentional and pupillary patterns in a social context may influence the longitudinal development of anxiety symptoms and disorders. Although the present study did not reveal associations between dwell time on a threatening stimulus and concurrent depressive severity, evidence from an eye-tracking version of a dot-probe paradigm administered to a subset of participants in the present study at pre-treatment (all of whom were clinically anxious at the time) showed that attentional and pupillary indices indicating avoidance of threat is predictive of depressive symptoms (but not anxiety symptoms) 2 years later [68]. Therefore, there is indication that additional longitudinal research may be helpful in identifying risk factors for internalizing symptoms.
Despite these limitations, the present findings have several strengths and potential clinical implications. This study implemented an ecologically valid paradigm to assess attentional patterns in youth, finding attention biases in circumstances of peer rejection and acceptance. The Chatroom-Interact task allowed the direct comparison of rejection and acceptance trials to control trials, which allowed us to examine rejection and acceptance effects individually. Findings regarding increased pupillary responsivity to peer acceptance in anxious compared to healthy youth may have clinical implications. Social acceptance by peers may be particularly potent for anxious children and could be used to a greater degree in order to strengthen existing treatments for anxious children and adolescents. In fact, in a study examining the efficacy of a family-based group cognitive-behavioral therapy treatment for anxious youth, parents rated their children’s lesson on rewarding brave behavior as the most useful session [69]. Future research may thus benefit from examining whether leveraging anxious youths’ sensitivity to social acceptance by peers provides therapeutic benefit.
Summary
Attention bias toward threat is considered an important mechanism in pediatric and adult anxiety disorders that may not be ameliorated following anxiety treatment; however, it remains unclear if attention bias to social threat may be exacerbated for adolescents with a history of anxiety. This study examined attention to social feedback from fictitious, virtual peers in healthy youth and youth with a history of anxiety. Results of the present study suggest that, regardless of history of anxiety, negative and positive social feedback from peers captures attention and is associated with greater pupillary reactivity compared to a non-feedback control condition in both healthy youth and youth with a history of an anxiety disorder. Youth with a history of anxiety exhibited greater pupil dilation in response to positive feedback compared to non-feedback trials, and healthy youth did not demonstrate such differences. No significant differences emerged when examining rejection feedback trials. Therefore, positive social feedback, unlike negative feedback, may differentially influence youth with a history of anxiety and could be used to a greater extent in existing psychotherapies.
References
Beesdo K, Knappe S, Pine DS (2009) Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatr Clin N Am 32:483–524. https://doi.org/10.1016/j.psc.2009.06.002
Langley AK, Bergman RL, McCracken J, Piacentini JC (2004) Impairment in childhood anxiety disorders: preliminary examination of the child anxiety impact Scale-Parent version. J Child Adolesc Psychopharmacol 14:105–114. https://doi.org/10.1089/104454604773840544
James A, Soler A, Weatherall R (2005) Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.cd004690.pub2
Wood JJ, McLeod BD, Piacentini JC, Sigman M (2009) One-year follow-up of family versus child CBT for anxiety disorders: exploring the roles of child age and parental intrusiveness. Child Psychiatry Hum Dev 40:301–316. https://doi.org/10.1007/s10578-009-0127-z
Beck AT, Clark DA (1997) An information processing model of anxiety: automatic and strategic processes. Behav Res Ther 35:49–58. https://doi.org/10.1016/S0005-7967(96)00069-1
Beck AT, Emery G, Greenberg RL (1985) Anxiety disorders and phobias: a cognitive approach. Basic, New York
Massaro D (1993) Information processing models: microscopes of the mind. Annu Rev Psychol 44:383–425. https://doi.org/10.1146/annurev.psych.44.1.383
Bar-Haim Y, Lamy D, Pergamin L et al (2007) Threat-related attentional bias in anxious and nonanxious individuals: a meta-analytic study. Psychol Bull 133:1. https://doi.org/10.1037/0033-2909.133.1.1
Mathews A, Mackintosh B (1998) A cognitive model of selective processing in anxiety. Cognit Ther Res 22:539–560
Öhman A (1996) Preferential preattentive processing of threat in anxiety: preparedness and attentional biases. Curr Controv Anxiety Disord 2:253–290
Mogg K, Bradley BP (1998) A cognitive-motivational analysis of anxiety. Behav Res Ther 36:809–848. https://doi.org/10.1016/S0005-7967(98)00063-1
Mathews A, MacLeod C (2002) Induced processing biases have causal effects on anxiety. Cogn Emot 16:331–354. https://doi.org/10.1080/02699930143000518
Beck AT (1976) Cognitive therapy and the emotional disorders. Penguin Press, New York
Shechner T, Britton JC, Pérez-Edgar K et al (2012) Attention biases, anxiety, and development: toward or away from threats or rewards? Depress Anxiety 29:282–294. https://doi.org/10.1002/da.20914
Harrison AJ, Gibb BE (2015) Attentional biases in currently depressed children: an eye-tracking study of biases in sustained attention to emotional stimuli. J Clin Child Adolesc Psychol 44:1008–1014. https://doi.org/10.1080/15374416.2014.930688
Kruijt A-W, Parsons S, Fox E (2018) A meta-analysis of bias at baseline in RCTs of attention bias modification: no evidence for dot-probe bias towards threat in clinical anxiety and PTSD. J Abnorm Psychol. https://doi.org/10.31234/osf.io/rfjup
Dudeney J, Sharpe L, Hunt C (2015) Attentional bias towards threatening stimuli in children with anxiety: a meta-analysis. Clin Psychol Rev 40:66–75. https://doi.org/10.1016/j.cpr.2015.05.007
Mogg K, Bradley BP (2005) Attentional bias in generalized anxiety disorder versus depressive disorder. Cognit Ther Res 29:29–45. https://doi.org/10.1007/s10608-005-1646-y
Fox E, Russo R, Bowles R, Dutton K (2001) Do threatening stimuli draw or hold visual attention in subclinical anxiety? J Exp Psychol Gen 130:681. https://doi.org/10.1037/0096-3445.130.4.681
In-Albon T, Kossowsky J, Schneider S (2010) Vigilance and avoidance of threat in the eye movements of children with separation anxiety disorder. J Abnorm Child Psychol 38:225–235. https://doi.org/10.1007/s10802-009-9359-4
Gamble AL, Rapee RM (2009) The time-course of attentional bias in anxious children and adolescents. J Anxiety Disord 23:841–847. https://doi.org/10.1016/j.janxdis.2009.04.001
Seefeldt WL, Krämer M, Tuschen-Caffier B, Heinrichs N (2014) Hypervigilance and avoidance in visual attention in children with social phobia. J Behav Ther Exp Psychiatry 45:105–112. https://doi.org/10.1016/j.jbtep.2013.09.004
Shechner T, Jarcho JM, Britton JC et al (2013) Attention bias of anxious youth during extended exposure of emotional face Pairs: an eye-tracking study. Depress Anxiety 30:14–21. https://doi.org/10.1002/da.21986
Waters AM, Kokkoris LL, Mogg K et al (2010) The time course of attentional bias for emotional faces in anxious children. Cogn Emot 24:1173–1181. https://doi.org/10.1080/02699930903274355
Mathews A, Mogg K, Kentish J, Eysenck M (1995) Effect of psychological treatment on cognitive bias in generalized anxiety disorder. Behav Res Ther 33:293–303. https://doi.org/10.1016/0005-7967(94)E0022-B
Mattia JI, Heimberg RG, Hope DA (1993) The revised stroop color-naming task in social phobics. Behav Res Ther 31:305–313. https://doi.org/10.1016/0005-7967(93)90029-T
Mogg K, Bradley BP, Millar N, White J (1995) A follow-up study of cognitive bias in generalized anxiety disorder. Behav Res Ther 33:927–935. https://doi.org/10.1016/0005-7967(95)00031-R
Waters AM, Mogg K, Bradley BP (2012) Direction of threat attention bias predicts treatment outcome in anxious children receiving cognitive-behavioural therapy. Behav Res Ther 50:428–434. https://doi.org/10.1016/j.brat.2012.03.006
Waters AM, Wharton TA, Zimmer-Gembeck MJ, Craske MG (2008) Threat-based cognitive biases in anxious children: comparison with non-anxious children before and after cognitive behavioural treatment. Behav Res Ther 46:358–374. https://doi.org/10.1016/j.brat.2008.01.002
Steinberg L (2005) Cognitive and affective development in adolescence. Trends Cogn Sci 9:69–74. https://doi.org/10.1016/j.tics.2004.12.005
Barnes GM, Hoffman JH, Welte JW et al (2007) Adolescents’ time use: effects on substance use, delinquency and sexual activity. J Youth Adolesc 36:697–710. https://doi.org/10.1007/s10964-006-9075-0
Wang J, Iannotti RJ, Nansel TR (2009) School bullying among adolescents in the United States: physical, verbal, relational, and cyber. J Adolesc Heal 45:368–375. https://doi.org/10.1016/j.jadohealth.2009.03.021
La Greca AM, Lopez N (1998) Social anxiety among adolescents: linkages with peer relations and friendships. J Abnorm Child Psychol 26:83–94. https://doi.org/10.1023/A:1022684520514
Storch EA, Masia-Warner C (2004) The relationship of peer victimization to social anxiety and loneliness in adolescent females. J Adolesc 27:351–362. https://doi.org/10.1016/j.adolescence.2004.03.003
Armstrong T, Olatunji BO (2012) Eye tracking of attention in the affective disorders: a meta-analytic review and synthesis. Clin Psychol Rev 32:704–723
Kowler E, Anderson E, Dosher B, Blaser E (1995) The role of attention in the programming of saccades. Vis Res 35:1897–1916. https://doi.org/10.1016/0042-6989(94)00279-U
Price RB, Kuckertz JM, Siegle GJ et al (2015) Empirical recommendations for improving the stability of the dot-probe task in clinical research. Psychol Assess 27:365–376. https://doi.org/10.1037/pas0000036
Siegle GJ, Steinhauer SR, Carter CS et al (2003) Do the seconds turn into hours? Relationships between sustained pupil dilation in response to emotional information and self-reported rumination. Cognit Ther Res 27:365–382. https://doi.org/10.1023/A:1023974602357
Price RB, Siegle GJ, Silk JS et al (2013) Sustained neural alterations in anxious youth performing an attentional bias task: a pupillometry study. Depress Anxiety 30:22–30. https://doi.org/10.1002/da.21966
Siegle GJ, Steinhauer SR, Friedman ES et al (2011) Remission prognosis for cognitive therapy for recurrent depression using the pupil: utility and neural correlates. Biol Psychiatry 69:726–733. https://doi.org/10.1016/j.biopsych.2010.12.041
Siegle GJ, Steinhauer SR, Stenger VA et al (2003) Use of concurrent pupil dilation assessment to inform interpretation and analysis of fMRI data. Neuroimage. https://doi.org/10.1016/s1053-8119(03)00298-2
Beatty J (1982) Task-evoked pupillary responses, processing load, and the structure of processing resources. Psychol Bull 91:276. https://doi.org/10.1037/0033-2909.91.2.276
Beatty J, Lucero-Wagoner B (2000) The pupillary system. Handb Psychophysiol 2:142–162
Breeden AL, Siegle GJ, Norr ME et al (2017) Coupling between spontaneous pupillary fluctuations and brain activity relates to inattentiveness. Eur J Neurosci 45:260–266. https://doi.org/10.1111/ejn.13424
Lau JYF, Guyer AE, Tone EB et al (2012) Neural responses to peer rejection in anxious adolescents: contributions from the amygdala-hippocampal complex. Int J Behav Dev 36:36–44. https://doi.org/10.1177/0165025411406854
Guyer AE, Benson B, Choate VR et al (2014) Lasting associations between early-childhood temperament and late-adolescent reward-circuitry response to peer feedback. Dev Psychopathol 26:229–243. https://doi.org/10.1017/S0954579413000941
Silk JS, Stroud LR, Siegle GJ et al (2012) Peer acceptance and rejection through the eyes of youth: pupillary, eyetracking and ecological data from the chatroom interact task. Soc Cogn Affect Neurosci 7:93–105. https://doi.org/10.1093/scan/nsr044
McDonald KL, Bowker JC, Rubin KH et al (2010) Interactions between rejection sensitivity and supportive relationships in the prediction of adolescents’ internalizing difficulties. J Youth Adolesc 39:563–574. https://doi.org/10.1007/s10964-010-9519-4
Silk JS, Tan PZ, Ladouceur CD et al (2016) A randomized clinical trial comparing individual cognitive behavioral therapy and child-centered therapy for child anxiety disorders. J Clin Child Adolesc Psychol. https://doi.org/10.1080/15374416.2016.1138408
Silk JS, Tan PZ, Ladouceur CD et al (2018) A randomized clinical trial comparing individual cognitive behavioral therapy and child-centered therapy for child anxiety disorders. J Clin Child Adolesc Psychol 47:542–554. https://doi.org/10.1080/15374416.2016.1138408
Kaufman J, Birmaher B, Brent D et al (1997) Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 36:980–988. https://doi.org/10.1097/00004583-199707000-00021
Wechsler D (1999) Manual for the Wechsler abbreviated intelligence scale (WASI). Psychol Corp, San Antonio
American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders (DSM IV). American Psychiatric Association, Washington, DC
Birmaher B, Khetarpal S, Brent D et al (1997) The screen for child anxiety related emotional disorders (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry 36:545–553. https://doi.org/10.1097/00004583-199704000-00018
Birmaher B, Brent DA, Chiappetta L et al (1999) Psychometric properties of the screen for child anxiety related emotional disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatry 38:1230–1236. https://doi.org/10.1097/00004583-199910000-00011
Hale WW, Raaijmakers Q, Muris P, Meeus W (2005) Psychometric properties of the screen for child anxiety related emotional disorders (SCARED) in the general adolescent population. J Am Acad Child Adolesc Psychiatry 44:283–290. https://doi.org/10.1097/00004583-200503000-00013
Siegle GJ, Ichikawa N, Steinhauer S (2008) Blink before and after you think: blinks occur prior to and following cognitive load indexed by pupillary responses. Psychophysiology 45:679–687. https://doi.org/10.1111/j.1469-8986.2008.00681.x
Brown BB (1990) Peer groups and peer cultures. At the threshold: the developing adolescent. Harvard University Press, Cambridge, pp 171–196
O’Brien SF, Bierman KL (1988) Conceptions and perceived influence of peer groups: interviews with preadolescents and adolescents. Child Dev 59:1360–1365. https://doi.org/10.1111/j.1467-8624.1988.tb01504.x
Coie JD, Dodge KA, Kupersmidt JB (1990) Peer group behavior and social status. In: Asher SR, Cole JD (eds) Peer rejection in childhood. Cambridge University Press, New York, pp 17–59
Jarcho JM, Romer AL, Shechner T et al (2015) Forgetting the best when predicting the worst: preliminary observations on neural circuit function in adolescent social anxiety. Dev Cogn Neurosci 13:21–31. https://doi.org/10.1016/j.dcn.2015.03.002
Morrison AS, Heimberg RG (2013) Social anxiety and social anxiety disorder. Annu Rev Clin Psychol 9:249–274. https://doi.org/10.1146/annurev-clinpsy-050212-185631
Davey CG, Allen NB, Harrison BJ, Ycel M (2011) Increased amygdala response to positive social feedback in young people with major depressive disorder. Biol Psychiatry 69:734–741. https://doi.org/10.1016/j.biopsych.2010.12.004
Koikegami H, Yoshida K (1953) Pupillary dialation induced by stimulation of the amygdaloid nuclei. Psychiatry Clin Neurosci 7:109–126. https://doi.org/10.1111/j.1440-1819.1953.tb00600.x
Bijleveld E, Custers R, Aarts H (2009) The unconscious eye opener: pupil dilation reveals strategic recruitment of resources upon presentation of subliminal reward cues. Psychol Sci 20:1313–1315. https://doi.org/10.1111/j.1467-9280.2009.02443.x
Mogenson GJ, Jones DL, Yim CY (1980) From motivation to action: functional interface between the limbic system and the motor system. Prog Neurobiol 14:69–97. https://doi.org/10.1016/0301-0082(80)90018-0
Faul F, Erdfelder E, Lang AG, Buchner A (2007) G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 39:175–191
Price RB, Rosen D, Siegle GJ et al (2016) From anxious youth to depressed adolescents: prospective prediction of 2-year depression symptoms via attentional bias measures. J Abnorm Psychol 125:267–278. https://doi.org/10.1037/abn0000127
Shortt AL, Barrett PM, Fox TL (2001) Evaluating the FRIENDS program: a cognitive-behavioral group treatment for anxious children and their parents. J Clin Child Adolesc Psychol 30:525–535. https://doi.org/10.1207/S15374424JCCP3004_09
Funding
This project was supported by National Institute of Mental Health Grants MH091327 & MH080215.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare they have no competing or potential conflicts of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants’ parents and informed assent was obtained from all individual youth participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rosen, D., Price, R.B., Ladouceur, C.D. et al. Attention to Peer Feedback Through the Eyes of Adolescents with a History of Anxiety and Healthy Adolescents. Child Psychiatry Hum Dev 50, 894–906 (2019). https://doi.org/10.1007/s10578-019-00891-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-019-00891-8