
Abstract
Many adult anxiety problems emerge in adolescence. Investigating how adolescent anxiety arises and abates is critical for understanding and preventing adult psychiatric problems. Drawing threat interpretations from ambiguous material is linked to adolescent anxiety but little research has clarified the causal nature of this relationship. Work in adults using Cognitive Bias Modification of Interpretations (CBM-I) training show that manipulating negative interpretational style alters negative affect. Conversely, ‘boosting’ positive interpretations improves affect. Here, we extend CBM-I investigations to adolescents. Thirty-nine adolescents (13–18 years), varying in trait anxiety and self-efficacy, were randomly allocated to receive positive or negative training. Training-congruent differences emerged for subsequent interpretation style. Induced negative biases predicted a decline in positive affect in low self-efficacious adolescents only. Tentatively, our data suggest that cognitive biases predict adolescent affective symptoms in vulnerable individuals. The acquisition of positive cognitions through training has implications for prevention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adolescence marks a period of vulnerability for the emergence of anxiety problems [1, 2]. Untreated, adolescent anxiety can generate considerable personal, social and economic costs. This has prompted calls for research into early preventative interventions [3]. Identifying effective early interventions relies on a better understanding of the risk processes by which adolescent anxiety problems arise but also subside. Here we address these challenges by assessing whether negative cognitions precipitate symptoms and conversely, whether boosting positive cognitions reduce symptoms in adolescents. This approach draws on two sets of findings. First, paralleling adult findings [4], growing data implicate cognitive biases in child and adolescent anxiety, particularly in the tendency to draw negative interpretations from ambiguous material [5–8]. Second, recent adult studies show that inducing functionally similar biases using computerised training can alter mood. These data therefore suggest that negative interpretative styles causally predict anxiety problems but also that promoting positive interpretative styles improves symptoms [9]. If such findings from training studies also hold for adolescent populations, they are ideally placed for identifying early preventative interventions to attenuate later debilitating outcomes. More particularly, these interventions would target early risk factors in the development of anxiety problems. This study therefore aims to assess the plasticity of cognitive styles using negative and positive training tasks in adolescents.
Cognitive bias modification of interpretation (CBM-I) training tasks present participants with a series of scenarios describing everyday experiences [10]. The valence of each scenario remains ambiguous until participants complete a word fragment at the end of the scenario that ‘disambiguates’ the meaning of the scenario. Depending on the training condition, word completion resolves the scenario in a positive or negative direction. This resolution of ambiguity is reinforced by a comprehension question which matches the valence of the training condition. After repeated exposure to these scenarios, participants receiving positive CBM-I are more likely to endorse positive interpretations of novel ambiguous scenarios than those receiving negative CBM-I, an effect that has been widely replicated in adults [11–17]. Moreover, induced negative interpretative styles are correlated with increases in state anxiety and reduction in positive affect [16, 18], while induced positive interpretative styles are associated with attenuations of negative affect and improvements in positive affect [13]. Extending positive training to symptomatic samples (e.g. high trait anxiety/depression) has yielded similar beneficial effects on mood [19], negative thought intrusions [20, 21] and anxiety [22–27], presumably through modification of cognitive biases.
Only a handful of studies have assessed CBM-I training effects in youth [28–30]. Most have focused on pre-adolescent children using age-appropriate training methods which are not directly comparable with those used in adults. Muris and colleagues [28] showed that 8–12 year old children trained to select negative interpretations of ambiguous situations encountered during a fictional space journey interpreted subsequent situations as more threatening than positively-trained participants. However this effect only characterized vulnerable children; that is, those with high trait anxiety. While a follow-up study replicated training effects on subsequent interpretations, these were no longer moderated by trait anxiety [29]. Effects of this study’s training paradigm on affective change were not assessed. In another study, effects of ‘benign’ (positive) CBM-I training were compared to a ‘no training’ condition in 10–11 year old children with high social anxiety [30]. Those who received the benign training endorsed fewer negative interpretations of new ambiguous situations relative to their control counterparts. Moreover, trained participants reported fewer social anxiety symptoms. Thus, consistent findings across studies provide support for the plasticity of cognitive biases in pre-adolescent children.
To our knowledge, two studies have investigated the plasticity of adolescent cognitive biases and their effects on mood [31, 32]. Clarifying the effects of CBM-I on in adolescents is important for several reasons. Vast biological, cognitive and social changes occur in adolescence [33]. These developmental differences preclude simple extrapolation of adult and even child data to understanding adolescent emotions. Indeed, adolescence is a period of protracted brain development [34], with increasing maturation of prefrontal cortex regions. Gradual changes also occur across a number of cognitive domains: abstract reasoning and formal operational thought [35], executive function [36], decision-making [37], social cognition [38] and the cognitive control of responses towards rewarding [39] and threatening stimuli [40]. In addition, researchers have hypothesized that cognitive schema continue to consolidate across adolescence [41]. These changes may emerge as a function of cognitive development [42], and from new and repeated learning experiences [41], which may occur through exposure to changing environments [43]. Given these developmental differences, it is unsurprising that linkages between cognitive biases and symptoms may vary across childhood, adolescence and adulthood. Exemplifying this, some studies investigating age differences in the role of attributional style in predicting depressive outcomes across development show that negative attributions only act as a trait-like diathesis, enhancing depressive responses to stress, in adolescence but not in childhood [44, 45].
A second reason for considering CBM-I in adolescence independently from adults is that animal studies suggest this as a developmentally-sensitive period during which disruptions to maturing brain circuits and associated information-processing can have life-long consequences for emotional problems [46]. These findings raise the intriguing question of whether interventions administered in adolescence are particularly effective in protecting against negative outcomes. Both adolescent CBM-I studies used training tasks similar in structure but different in content to the adult paradigm [10]. While adolescents read scenarios and completed word fragments, these scenarios were made more age-appropriate than those described in the original training set [10]; for example, making friends at a new school, being asked out on a date, being asked by a teacher to stay behind class. Both studies replicated adult findings of the training effects on subsequent interpretations of new ambiguous materials but effects on mood were less clear [31, 32]. In one study, positive training resulted in a significant decrease in negative affect, but negative training only led to a significant decrease in positive affect in male participants [32]. In the other study, there were no effects on state anxiety before and after training [31]. Trait anxiety did not moderate training effects on cognitive or affective measures in either study. Though encouraging, these adolescent data are preliminary and require replication.
The aims of the present study were therefore to extend these initial findings to a new sample of adolescents, a period of unique developmental changes in biology, cognition and the social environment. Using our adapted adult training methods for adolescents [32], we predicted that positive training would result in greater endorsement of positive interpretations of novel ambiguous situations, while negative training would invite the opposite pattern of effects. Data from a new sample would also clarify the more mixed findings on mood changes pre- to post-training. Thus, we examined the effects of positive and negative CBM-I on changes in both positive and negative affect. Third, given that various adult studies and two of the four studies of youth have emphasized the effectiveness of training in participants with pre-existing levels of and anxiety problems, with stronger training effects among vulnerable individuals, we explored the moderating role of differences in anxious temperaments and self-efficacy on training effects. Self-efficacy is the capacity to manage threatening events or situations: low self-efficacious individuals are less confident in their ability to cope with difficult situations. Thus these individuals are vulnerable for developing emotional symptoms following negative events [47].
Method
Participants
Thirty-six adolescents (64% female, 86% Caucasian) aged 13–18 years (mean age: 16.49, SD: 1.47) were recruited from schools in Oxfordshire and Buckinghamshire. Participants were asked if they had a current or past diagnosis of a mood or anxiety disorder, with those responding in the affirmative being excluded from the study. This was done for two reasons. First, for ethical reasons, we did not want to include adolescents with a history of anxiety problems in the negative training condition, a possibility, given our random allocation of participants to each training condition. As these are the first data to explore negative training, we were unsure whether any adverse effects of training would occur and persist in a group of vulnerable adolescents. Second, there is still relatively little data collected on the effectiveness of our training tool in eliciting cognitive biases and affective change in adolescents. We therefore considered these data as ‘proof of principle’ that cognitive biases could be manipulated through external training interventions, before applying these to clinical samples. As adolescents with mood and anxiety disorders form a heterogeneous group, varying in severity and length of episodes, number of prior episodes, treatment history, family history, and co-morbid psychiatric conditions, we did not want these confounding variables to affect interpretation of training-related differences on cognition and mood. We therefore restricted our sample to only adolescents with symptoms varying in the normal range.
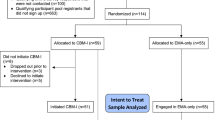
Participants were randomly allocated to the positive (n = 17) or negative (n = 19) CBM-I training group. There were no significant differences between the groups in terms of gender, age, trait anxiety or self-efficacy (all P > .309; see Table 1). The ethnicity of the groups was not balanced (P = .024), but all participants spoke English as their first language. To ensure that group differences in ethnicity across conditions did not confound group differences on post-training cognitive and affective measures, preliminary analysis investigated whether results varied when non-Caucasian participants were excluded from the analysis. As results remained the same, data from all participants were used in the final analysis.
Overview of Procedures
Study procedures followed those of our previous study (See Fig. 1; 32). These were approved by the Central University Research Ethics Committee of the University of Oxford. Participants were not informed of the purpose of the training paradigm prior to training but were fully debriefed at the end of the study. Participants under the age of 16 years provided written assent, with a parent or legal guardian providing informed consent on their behalf. Consistent with British Psychological Society guidelines for professional practice, young people between the ages of 16–18 were able to give consent independently of parental responsibility. Therefore these participants provided informed written consent. Nonetheless, we also wrote to parents to inform them of the nature of the research and of their child’s interest in becoming involved prior to their participation.

Overview of experimental procedures and examples of training and test materials. CBM-I cognitive bias modication of interpretations training; VAS visual analogue scale; T1 time 1; T2 time 2; T3 time 3; T4 time 4
To maximise the effects of CBM-I training, we instructed participants to read and imagine each training scenario as if it was happening to themselves [18]. To make the use of imagery explicit, all participants received two ‘imagery’ exercises prior to training [32]. The first involved imagining coming home from school while the second involved imagining biting into a lemon. Following training, participants completed a 10-min filler task, to allow group differences in mood that emerged through training to dissipate. This procedure is standard in most CBM-I studies [10], allowing group differences in the interpretation of new ambiguous events to be assessed without confounds associated with mood differences. The filler task was a picture rating task in which participants rated 60 emotionally neutral pictures on a Visual Analogue Scale (VAS) between ‘very unpleasant’ (0 cm) and ‘very pleasant’ (9.8 cm). None of the participants guessed the true purpose of the study or reported distress beyond the debriefing session. Both CBM-I training and the test of induced bias was carried out on a laptop computer using E-Prime 2.0 [48].
CBM-I Training Task
In our previous study we developed an adolescent version of the CBM-I training task by including scenarios relevant to adolescents, such as social relationships, school and extra-curricular pursuits [32]. These scenarios were piloted in 3 adolescents aged 14–16 years for readability and relevance.
The CBM-I training task consisted of one practice trial followed by 60 recorded trials, presented as five blocks of 12. Each trial presented a short description of an everyday scenario which remained emotionally ambiguous until the final word, which was presented as a word fragment on the following screen. Participants had to identify the word from the fragment as quickly as possible by typing its first missing letter. This word resolved the ambiguity of the scenario, leading to a positive interpretation for the majority of trials in the positive condition, and a negative interpretation for the majority of trials in the negative condition. In each condition, five scenarios (one in each block of 12 trials) resolved with the opposite valence (negative in the positive condition and vice versa) and five scenarios (again one in each block of 12 trials) resolved neutrally. These items were included to obscure the purpose of the training. Once the word fragment was correctly completed, participants were asked a comprehension question for which the correct answer (yes or no) was based on the intended emotional interpretation of the training scenario. Participants only viewed the comprehension question if they had completed the word fragment correctly. All comprehension questions were followed by feedback (“correct” or “wrong”). Therefore both the word fragment completion and comprehension question reinforced the intended emotional valence of the scenario. Participants were instructed to respond to the comprehension questions as quickly and accurately as possible. An example of an ambiguous scenario is: “During maths, you are asked by the teacher to write the homework on the board. When you have finished, your teacher looks at it with an expression of “agr–m-nt” (positive condition) or “disagr–m-nt” (negative condition). The comprehension question following this item is: “Does your teacher approve of your work?” The correct response is “Yes” for participants receiving positive training and “No” for those receiving negative training. The order of scenarios in each block was randomised across participants.
Assessment of Training Effects on Interpretation Bias
The test consisted of two phases (Fig. 1). In the first phase, ten ambiguous scenarios were presented, each with a title. Participants were given the same instructions as in the training phase. Unlike training items, completing word fragments did not disambiguate the emotional valence of the scenarios; the comprehension questions also had no emotional content. In the second phase, participants viewed the title of each scenario they had seen, followed by four statements relating to that scenario. Participants were informed that the sentences resembled the scenario, but none would be an exact match. They were instructed to rate statements on their similarity to the scenarios viewed in the first phase on a scale from 1 to 4 (1: not similar at all; 2: not so similar; 3: similar; 4: very similar). These statements, ordered randomly, included one positive and one negative interpretation of the scenario (targets). The other two statements were also positively and negatively valenced but were not valid interpretations of the previously presented scenarios (foils).
Bias induction was successful if the negative CBM-I training group rated negative targets as more similar to the original ambiguous scenarios, and the positive CBM-I training group rated positive targets as more similar. This pattern of results suggests that the novel ambiguous situations were interpreted consistently with the valence of the training [10]. Similarity of foils assessed whether training induced a general affective bias towards items of a particular valence.
Assessment of Training Effects on Mood Changes
Mood was assessed at four time-points during the study (T1–T4) using VAS versions of the Positive and Negative Affect Scale for Children (PANAS-C; [49]). Eight emotions from the original PANAS-C formed a negative affect VAS (nervous, sad, upset, worried, anxious, miserable, scared, gloomy) while 4 items formed a positive affect scale (happy, calm, cheerful, energetic). Participants indicated how much of each emotion they were feeling at that moment, on a line between “not (emotion) at all” (0 cm) and “very (emotion)” (9.8 cm). VASs can be effective in detecting the influence of an intervention on a dependent variable [50].
Questionnaire Measures
All participants completed the Trait scale of the State Trait Anxiety Inventory for Children (STAI-T-C)[51]. This comprises 20 items, where participants rate how frequently common anxiety symptoms apply to them (e.g. “I worry too much”). This measure has high internal reliability (Cronbach’s α = .91) and correlates well with other measures of child and adolescent anxiety, such as the Revised Children’s Manifest Anxiety Scale [52].
Participants also completed the Self-Efficacy Questionnaire for Children (SEQ-C)[53]. The SEQ-C is a 24-item measure of self-efficacy measuring perceptions of personal strength in the academic, social and emotional domains. Participants read questions about their personal abilities (e.g. “How well can you control your feelings?”) and indicated their answers on a five point scale (1: not at all, 5: very well). Previous investigations of self-efficacy have excluded three of the SEQ-C questionnaire items from their analyses because they did not load convincingly on a particular domain of self efficacy in factor analysis [53]. To maintain consistency, the same three items were excluded in this study. This measure has high internal reliability (Cronbach’s α = .88) [53]. Criterion validity has been established through negative correlations with psychological problems and positive correlations with measures of life satisfaction [54].
Statistical Analyses
All paired- and independent- sample t-tests were two-tailed. Wherever assumptions of normality were violated, log transforms were used in the analysis. Independent sample t-tests were first carried out to assess training differences on task performance including reaction times (RTs) to completion of word fragments and comprehension questions, and the percentage of correctly answered comprehension questions. Next, we carried out an independent sample t-test on the positive and negative mood ratings at all time points to assess baseline differences in mood or any confound of mood differences immediately before the interpretation bias test.
To examine training effects on interpretations of new ambiguous material, a 2 × 2 × 2 mixed measures analysis of variance (ANOVA) assessed the effects of two within-subjects factors (recognition statement type: target vs. foil; recognition statement valence: positive vs. negative) and one between-subjects factor (training group: positive vs. negative condition) on similarity ratings. Subsequent analyses included either: gender (male, female), trait anxiety group (above median vs. below median) and self-efficacy group (above median vs. below median) as additional between-subject factors. The Greenhouse–Geisser (G–G) correction was applied. Effect sizes of within-group and between-group differences on negative and positive targets were estimated with Cohen’s d. To examine training effects on mood change, 2 × 2 × 2 mixed measures ANOVAs were performed, with time as a within subjects-factor (T1 vs. T2) and training group (positive vs. negative) as between-subjects factors. Again, subsequent analysis included gender, trait anxiety and self-efficacy as between-subject factors. The G–G correction was applied. Analyses were carried out separately for positive and negative affect consistent with our previous study [32].
Results
Training Effects on Task Performance
No significant differences were found between training groups on average RTs to word fragments (t(34) = −.27, P = .79) or comprehension question completion (t(34) = .16, P = .88) (Table 1). Nor were there differences in the percentage of comprehension questions answered correctly (t(34) = .93, P = .36).
Training Effects on Interpretation Bias
A main effect of recognition statement type emerged (F(1,34) = 62.05, P < .001), suggesting that similarity ratings were higher for targets than foils. We also found a 2-way interaction between training group and recognition statement valence (F(1,34) = 11.74, P < .01), that was further modified by recognition statement type (F(1,34) = 8.09, P < .01). To decompose these two- and three-way interactions, separate analyses were conducted for targets and for foils. For targets, the mixed-measures ANOVA showed a significant interaction between training group and valence of the recognition statement (F(1,30) = 16.34, P < .001). Figure 2 illustrates this interaction as positive targets (PT) being rated as significantly more similar to original scenarios than negative targets (NT) in those who had received positive training (t(16) = -2.47, P = .025; PT Mean = 2.62, NT Mean = 2.23, Cohen’s d = .76). Individuals who had received negative training gave higher similarity ratings to NT than PT (t(18) = 2.69, P = .015; NT Mean = 2.77, PT Mean = 2.25, Cohen’s d = .97). The difference in the ratings of NT between training groups and PT between training groups were also significant (NT: t(34) = -3.10, P = .004, Cohen’s d = 1.03; PT: t(34) = 2.15, P = .039, Cohen’s d = .71).

Similarity ratings for positive and negative targets and foils acorss training groups in the testing phase. Higher similarity ratings reflect greater resemblance of the item to the ambiguous situation. *P < .5, **P < .1
For foils, a significant training-group-by-recognition-valence interaction also emerged (F(1,30) = 10.37, P = .003). Positively-trained individuals gave higher recognition ratings to positive foils (PF) than negative foils (NF) (t(16) = -3.11, P = .015; PF Mean = 2.23, NF Mean = 1.90), as shown in Fig. 2. Negatively-trained adolescents showed a trend for rating NF as more similar to the original scenarios than PF (PF Mean = 1.97, NF Mean = 2.10). For both target and foil data, no other significant main or interaction effects emerged, including for gender, trait anxiety group and self-efficacy group.
Training Effects on Mood Measures
Negative affect scores at all time-points were skewed so data were log transformed prior to analysis. Groups differed in negative affect at T1 (t(34) = 2.37, P = .024), with the positive group reporting more negative affect before training (Table 2). No differences were found for positive affect at T1 Table 2.
For positive affect, there were no significant effects of time, training group or their interaction. Neither gender nor trait anxiety group exerted main effects or interacted with these variables. However there was a significant 3-way interaction between time, training group and self-efficacy (F(1,31) = 4.76, P = .037). Figure 3 shows that of the individuals who received negative training, those who reported lower self-efficacy showed a significant reduction in positive affect from pre- to post-training (t(6) = 3.50, P = .013, T1 Mean = 6.67, T2 Mean = 5.30). Changes in positive affect were not significant in negatively-trained high self-efficacious individuals. Nor were there significant changes in positive affect from T1 to T2 among positively-trained individuals.

The three-way interaction between positive affect (time 1 vs. time 2), training group (positive vs. negative) and self-efficacy group (below median vs. above median)
These results did not characterise changes in negative affect.
Discussion
Several novel findings emerge from these data. First, clear support for previous findings emerged [31, 32], notably that negative and positive interpretation biases can be successfully induced in adolescents using CBM-I training. Thus these data are consistent with prior findings in adults and pre-adolescent children. Following positive CBM-I participants endorsed positive interpretations as more similar to previously viewed ambiguous scenarios than negative interpretations in a surprise recognition test. The opposite pattern of similarity ratings was observed following negative CBM-I. These findings could not be explained by participants making mood-congruent judgements, as there were no significant differences in mood between the two training groups at the time of bias testing. Additionally, no significant difference in ability on the training task was found between training groups, as indicated by RTs to word fragments and comprehension questions, and percentage of comprehension questions answered correctly. ‘Target’ ratings of similarity to the originally-presented scenario were higher (i.e. rated as more similar to the original scenarios) than ‘foil’ similarity ratings, suggesting that the results are based on an induced interpretation bias rather than general affective priming from the training task. Training effects were not modified by gender, trait anxiety, or self-efficacy.
The second key finding was that while there were no overall changes in positive and negative affect associated with training across participants, significant reductions in positive affect characterized adolescents with low self-efficacy following negative training. These effects occurred independently of trait anxiety. Adolescents reporting lower self-efficacy were more susceptible to the attenuation of positive mood following negative training. However, they did not differ on the strength of the cognitive bias induced. Thus differences in mood change were unlikely to relate to differences in induced bias.
Our data promise to inform theories and therapies of adolescent anxiety problems. Data from both this and other training tasks persuasively suggest that child and adolescent cognitive biases are plastic [28–32]. Moreover, our effect sizes relating to induced biases through training were generally large (Cohen’s d = .70–1.03). This is consistent with a large body of research showing that cognitive biases can be acquired through social modelling procedures, such as between parents and their offspring [55]. Ours and other data extend these findings by suggesting that cognitive styles can be explicitly taught, through repeated exposure and reinforcement learning. These findings lend further credence to the aspect of cognitive-behavioural therapy that explicitly targets cognitive bias change, by providing a controlled, experimental model of processes that contribute to therapeutic change.
Perhaps initially a little disappointing, our findings do not show that cognitive change serves as a precursor to mood change in general across all adolescents. This is not particularly surprising taken in context of adult data: although instances of training effects on mood change have been found [56, 57], others have reported no effects on mood [14, 16, 58, 59] or mixed results [17, 21, 60]. Even when mood-change differences are present, it is not clear whether these manifest through changes in negative affect or positive affect. It is also not clear if mood effects occur because of the induced cognitive bias although more sophisticated mediation analysis suggests that this is plausible [27]. These mixed findings with respect to mood effects complicate inferences about the causality of the interpretation bias in anxiety. What appears more consistent from adult findings is that training affects stress reactivity [61]: cognitive biases do not act directly on short-term fluctuations in mood, but instead, as postulated by stress-diathesis theories, induce changes in stress responsiveness. Such parallel data in adolescents are lacking but form the basis of exciting new investigations. Our adolescent data do however show that a subset of individuals manifest reductions in positive affect following negative bias induction. As low self-efficacy may comprise a vulnerability factor for mood and anxiety problems [47] it is interesting that adolescents with lower self-efficacy responded with reductions in positive affect after exposure to negative interpretations of situations. If these data are replicated, then improving self-efficacy might be an important focus for preventing negative emotional reactions to stressful events in the general adolescent population, but in cognitively-vulnerable individuals in particular.
While these findings carry a number of interesting implications, some caveats need to be considered. First, the sample size was small and may have decreased the capacity to detect weak effects of training group differences on mood change across all adolescents. It is also unclear whether the current adolescents were representative of the general population. As adolescents were told that the task involved reading a number of scenarios, our volunteer sample may have self-selected on the basis of reading ability. To examine training effects in a broader range of adolescents with differing cognitive capacities, including younger participants, future studies could develop auditory training tasks, although caution over differences as a function of training modality needs to be considered [62]. Second, adolescents assigned to positive training reported significantly higher mean negative affect prior to bias induction. As baseline differences normalised after training, it remains possible that initial high levels of negative affect in the positive training condition masked any potential group differences in changes in negative affect. Third, we included no baseline measures of interpretation bias, relying instead on post-training differences on interpretational style. Finally, because of issues relating to the length of testing, we only used visual analogue scales, using items from the PANAS-C to measure mood changes in the study. Future studies should replicate these findings with more valid measures of mood, such as the complete version of the PANAS-C [49].
The plasticity of training biases, particularly positive ones in this age range, are encouraging for the planning of new therapeutic and preventative techniques for young people. While current psychological interventions such as CBT are effective, outcomes can also be highly variable [63]. Availability and access to CBT in youth may also be limited [64]. Tentatively, our data are suggestive that training effects on cognitive biases impinge equally across all adolescents: males and females, those with low and high self-efficacy, and those with low and high trait anxiety. Training tasks such as CBM-I could therefore be applied as an evidence-based adjunct intervention to CBT, for example serving as a ‘booster’ that targets cognitive bias specifically between sessions. Alternatively, CBM-I could be used as a prevention tool in adolescents at-risk for anxiety problems. Logistically, the ease with which CBM-I can be computerised will no doubt increase its appeal for a younger, computer-literate audience. However before CBM-I can be used more widely as a clinical tool, several outstanding questions need to be resolved. First, the current data do not speak to the long-term effects of training. Nor do they inform the generalizability of training to the interpretation of real-life ambiguous social situations and to mood changes associated with stressful social situations. The number of training sessions required to induce long-term cognitive and affective change will also need to be investigated. Finally, the effectiveness of CBM-I will need to be verified in clinical samples, where more extreme levels of trait anxiety and self-efficacy are present. These can be achieved using multi-session randomised controlled trial studies, designs that have already been applied to other cognitive training packages, such as attention bias modification tasks with exciting results [65]. While adolescent CBM-I research is still in its infancy, it clearly has the potential to transform current psychological interventions.
Summary
In the present study, we investigated whether a new, adolescent, computerised cognitive training package was effective at generating positive and negative interpretations of ambiguous information. We also assessed whether these induced biases altered mood change. As expected, adolescents assigned to receive positive training drew more positive interpretations of new ambiguous information than adolescents who had received negative training. Reductions in positive mood following negative training only characterised adolescents with low self-efficacy. If replicated, these data support a causal link between negative cognitive biases and mood in vulnerable adolescents. Perhaps more importantly, these data point to the potential of a new tool that can be applied in clinical settings, either as an early treatment or preventative intervention of adolescent anxiety.
References
Gregory AM et al (2007) Juvenile mental health histories of adults with anxiety disorders. Am J Psychiatry 164:301–308
Kim-Cohen J et al (2003) Prior juvenile diagnoses in adults with mental disorder: developmental follow-back of a prospective-longitudinal cohort. Arch Gen Psychiatry 60:709–717
Sahakian BJ, Malloch G, Kennard C (2010) A UK strategy for mental health and wellbeing. Lancet 375(9729):1854–1855
Beck AT, Clark DA (1997) An information processing model of anxiety: automatic and strategic processes. Behav Res Ther 35:49–58
Hadwin J et al (1997) Cognitive processing and trait anxiety in typically developing children: evidence for an interpretation bias. J Abnorm Psychol 106:486–490
Taghavi MR et al (2000) Interpretation of ambiguous emotional information in clinically anxious children and adolescents. Cogn Emot 14:809–822
Waters AM et al (2008) Threat interpretation bias as vulnerability factor in childhood anxiety disorders. Behav Res Ther 46:39–47
Prinstein MJ, Cheah CS, Guyer AE (2005) Peer victimization cue interpretation and internalizing symptoms: preliminary concurrent and longitudinal findings for children and adolescents. J Clin Child Adolesc Psychol 34(1):11–24
Mathews A, MacLeod C (2005) Cognitive vulnerability to emotional disorders. Annu Rev Clin Psychol 1:167–195
Mathews A, Mackintosh B (2000) Induced emotional interpretation bias and anxiety. J Abnorm Psychol 109:602–615
Hirsch CR, Mathews A, Clark DM (2007) Inducing an interpretation bias changes self-imagery: a preliminary investigation. Behav Res Ther 45:2173–2181
Hoppitt L et al (2010) Cognitive bias modification: the critical role of active training in modifying emotional responses. Behav Ther 41:73–81
Salemink EM, van den Hout M, Kindt M (2007) Trained interpretive bias: validity and effects on anxiety. J Behav Ther Exp Psychiatry 38:212–224
Yiend J, Mackintosh B, Mathews A (2005) Enduring consequences of experimentally induced biases in interpretation. Behav Res Ther 43:779–797
Salemink E, van den Hout M (2010) Trained interpretive bias survives mood change. J Behav Ther Exp Psychiatry 41:310–315
Mackintosh B et al (2006) Induced biases in emotional interpretation influence stress vulnerability and endure despite changes in context. Behav Ther 37:209–222
Holmes EA et al (2006) Positive interpretation training: effects of mental imagery versus verbal training on positive mood. Behav Ther 37:237–247
Holmes EA, Lang TJ, Shah DM (2009) Developing interpretation bias modification as a “cognitive vaccine” for depressed mood: imagining positive events makes you feel better than thinking about them verbally. J Abnorm Psychol 118:76–88
Blackwell SE, Holmes EA (2010) Modifying interpretation and imagination in clinical depression: A single case series using cognitive bias modification. Appl Cog Psychol 24:338–350
Hayes S et al (2010) The effects of modifying interpretation bias on worry in generalized anxiety disorder. Behav Res Ther 48:171–178
Hirsch CR, Hayes S, Mathews A (200) Looking at the bright side: accessing benign meanings reduces worry. J Abnorm Psychol 118:44–54
Amir N, Bomyea J, Beard C (2010) The effect of single-session interpretation modification on attention bias in socially anxious individuals. J Anx Disord 24:178–182
Beard C, Amir N (2008) A multi-session interpretation modification program: change in interpretation and social anxiety. Behav Res Ther 46:1135–1141
Mathews A et al (2007) Inducing a benign interpretational bias reduces trait anxiety. J Behav Ther Exp Psychiatry 38:225–236
Murphy R et al (2007) Facilitating a benign interpretation bias in a high socially anxious population. Behav Res Ther 45:1517–1529
Steinman SA, Teachman BA (2010) Modifying interpretations among individuals high in anxiety sensitivity. J Anx Disord 24:71–78
Salemink E, van den Hout M, Kindt M (2009) Effects of positive interpretive bias modification in highly anxious individuals. J Anx Disord 23:676–683
Muris P, Huijding J, Mayer B, Hameetman M (2008) A space odyssey: experimental manipulation of threat perception and anxiety-related interpretation bias in children. Child Psychiatry Hum Dev 39:469–480
Muris P, Huijding J, Mayer B, Remmerswaal D, Vreden S (2009) Ground control to major tom: experimental manipulation of anxiety-related interpretation bias by means of the “space odyssey” paradigm and effects on avoidance tendencies in children. J Anx Disord 23:333–340
Vassilopoulos SR, Banerjee R, Prantzalou C (2009) Experimental modification of interpretation bias in socially anxious children: changes in interpretation anticipated interpersonal anxiety and social anxiety symptoms. Behav Res Ther 47:1085–1089
Salemink E, Wiers RW (2011) Modifying threat-related interpretive bias in adolescents. J Abnorm Child Psychol. doi:10.1007/s10802-011-9523-5
Lothmann C, Chan SY, Holmes EA, Lau JY (2011) Cognitive bias modification training in adolescents: effects on interpretation biases and mood. J Child Psychol Psychiatry 52:24–32
Somerville LH, Jones RM, Casey BJ (2010) A time of change: behavioral and neural correlates of adolescent sensitivity to appetitive and aversive environmental cues. Brain Cogn 72:124–133
Gogtay N et al (2004) Dynamic mapping of human cortical development during childhood through early adulthood. Proc Natl Acad Sci USA 101:8174–8179
Marini Z, Case R (1994) The development of abstract reasoning about the physical and social world. Child Dev 65:147–159
Crone EA et al (2006) Brain regions mediating flexible rule use during development. J Neurosci 26:11239–11247
Crone EA, van der Molen MW (2004) Developmental changes in real life decision making: performance on a gambling task previously shown to depend on the ventromedial prefrontal cortex. Dev Neuropsychol 25:251–279
Dumontheil I, Apperly IA, Blakemore SJ (2010) Online usage of theory of mind continues to develop in late adolescence. Dev Sci 13:331–338
Van Leijenhorst L et al (2010) Adolescent risky decision-making: neurocognitive development of reward and control regions. Neuroimage 51:345–355
Lau JY et al (2011) Distinct neural signatures of threat learning in adolescents and adults. Proc Natl Acad Sci USA 108:4500–4505
Hammen C, Zupan BA (1984) Self-schemas depression and the processing of personal information in children. J Exp Child Psychol 37:598–608
Nolen-Hoeksema S, Girgus JS, Seligman ME (1992) Predictors and consequences of childhood depressive symptoms: a 5-year longitudinal study. J Abnorm Psychol 101:405–422
Lau JY, Eley TC (2006) Changes in genetic and environmental influences on depressive symptoms across adolescence and young adulthood. Br J Psychiatry 189:422–427
Turner JE, Cole DA (1994) Developmental differences in cognitive diatheses for child depression. J Abnorm Child Psychol 22:15–32
Cole DA, Turner JE (1993) Models of cognitive mediation and moderation in child depression. J Abnorm Psychol 102:271–281
Leonardo ED, Hen R (2008) Anxiety as a developmental disorder. Neuropsychopharm 33:134–140
Bandura A (1977) Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 84:191–215
Psychology Software Tools E-Prime 20 2005. (Computer Software)
Laurent J et al (1999) A measure of positive and negative affect for children: scale development and preliminary validation. Psychol Assess 11:326–338
Grant S et al (1999) A comparison of the reproducibility and the sensitivity to change of visual analogue scales Borg scales and Likert scales in normal subjects during submaximal exercise. Chest 116:1208–1217
Spielberger CD (1973) State-trait anxiety inventory for children. Palo Alto Calif, Consulting Psychologists Press, USA
Muris P et al (2002) Three traditional and three new childhood anxiety questionnaires: their reliability and validity in a normal adolescent sample. Behav Res Ther 40:753–772
Muris P (2001) A brief questionnaire for measuring self-efficacy in youths. J Psychopathol Behav Assess 23:145–149
Suldo SM, Shaeffer EJ (2007) Evaluation of the self-efficacy questionnaire for children in two samples of American adolescents. J Psychoed Assess 25:341–355
Goodman SH, Gotlib IH (1999) Risk for psychopathology in the children of depressed mothers: a developmental model for understanding mechanisms of transmission. Psychol Rev 106:458–490
Salemink E, van den Houdt M, Kindt M (2007) Trained interpretive bias: validity and effects on anxiety. J Behav Ther Exp Psychiatry 38:212–224
Holmes EA, Mathews A (2005) Mental imagery and emotion: a special relationship? Emotion 5:489–497
Teachman BA, Addison LM (2007) Training non-threatening interpretation in spider fear. Cog Ther Res 32:448–459
Wilson EJ et al (2006) The causal role of interpretive bias in anxiety reactivity. J Abnorm Psychol 115:103–111
Salemink E, van den Hout M, Kindt M (2007) Trained interpretive bias and anxiety. Behav Res Ther 45:329–340
Mathews A, MacLeod C (2002) Induced processing biases have causal effects on anxiety. Cogn Emot 16:331–354
Standage H, Ashwin C, Fox E (2009) Comparing visual and auditory presentation for the modification of interpretation bias. J Behav Ther Exp Psychiatry 40:558–570
James A, Soler A, Weatherall R (2005) Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database Syst Rev 4:CD004690
Stallard P, Udwin O, Goodard M, Hibbert S (2007) The availability of cognitive behaviour therapy within specialist child and adolescent mental health services (CAMHS): a national survey. Behav Cog Psychother 35:501–505
Bar-Haim Y, Morag I, Glickman S (2011) Training anxious children to disengage attention from threat: a randomized controlled trial. J Child Psychol Psychiatry Jan 19. doi:10.1111/j.1469-7610.2011.02368.x. (Epub ahead of print)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lau, J.Y.F., Molyneaux, E., Telman, M.D. et al. The Plasticity of Adolescent Cognitions: Data from a Novel Cognitive Bias Modification Training Task. Child Psychiatry Hum Dev 42, 679–693 (2011). https://doi.org/10.1007/s10578-011-0244-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-011-0244-3