
Abstract
Substance abuse and sexual health research tends to overlook the resiliency skills that Black adolescent girls possess. Using a strengths-based lens, this study examines the role of protective factors: (e.g. ethnic identity, social support, and psychological empowerment) on sexual risk behaviors testing drug use as a mediator among a sample of Black adolescent girls. The study uses a sample (N = 340) female adolescents (13–17 years old) who identified as being Black only and reside in a northeastern urban community in New Jersey. Structural equation modeling was employed to test the hypothesized model of the mediating role of drug use on sexual risk behaviors among this sample. Findings revealed that drug use significantly mediated the relationship between social support, ethnic identity, and psychological empowerment on sexual risk behaviors, with high ethnic identity scores having the strongest relationship on low sexual risk behaviors and low levels of drug use. Given the rise of sexually transmitted infections (STIs) in the United States among Black adolescent girls, findings from this study can contribute to development of culturally appropriate and innovative strategies to reduce risky behaviors by promoting social and cultural strengths among Black girls living in urban communities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Black adolescent girls face a significant gender paradox where they tend to use drugs at a lesser rate than Black adolescent boys and White adolescent girls, but face much harsher health consequences due to drug use such as reproductive health disparities, fertility issues, and unprotected sex leading to early pregnancy (Centers for Disease Control and Prevention, CDC, 2016; Jackson, Seth, DiClemente, & Lin, 2015). Sexual risk behaviors refers to having unprotected sex, early sexual debut (sex before age 14 years old), having sex with multiple partners, and having sex under the influence of drugs (Kann et al., 2018). Black adolescent girls between the ages of 14 and 19 have the highest rates of sexually transmitted infections (STIs) in the U.S., highest rates of early teen pregnancy, and are more likely to endure poor health outcomes associated with sexual risk behaviors compared to White and other ethnic minority adolescent girls (Anderson & Mueller, 2008; Centers for Disease Control and Prevention, CDC, 2016; Chung et al., 2017; Jackson et al., 2015; Pflieger, Cook, Niccolai, & Connell, 2013). Among adolescent girls, drug use typically aligns with numerous risk characteristics including engaging in sexual risk behaviors. Therefore, preventing drug use among Black adolescent girls may simultaneously lead to a lower likelihood of engaging in sexual risk behaviors that can reduce poor health outcomes such as diagnoses of human immunodeficiency virus (HIV) and STIs among this population (Andrade, Carroll, & Petry, 2013; Danielson et al., 2014; Guthrie, Cooper, Brown, & Metzger, 2012; Swartzendruber, Sales, Brown, DiClemente, & Rose, 2016
Due to the racist, sexist, and classist views that impact vulnerable groups in the United States, such as Black adolescent girls, they continue to be at a significant disadvantage of achieving positive health outcomes compared to their White female counterparts (Opara, 2018). As an example, Black adolescent girls are often tasked to challenge negative stereotypes that are placed on them pertaining to their sexuality and identity (Collins, Baiardi, Tate, & Rouen, 2015). Repeated exposure to these stereotypes and experiences can contribute to the oversexualization of Black adolescent girls, suggesting that Black adolescent girls should undertake and normalize risky behaviors that may involve unprotected sex and drug use (Collins et al., 2015; Wallace, Townsend, Glasgow, & Ojie, 2011). Furthermore, such norms can indirectly demean their sense of self including their connection to their racial–ethnic identity and self-esteem, which can lead to engaging in behaviors that contribute to poor health outcomes (Guzmán & Stritto, 2012; Respress, Amutah-Onukagha, & Opara, 2018). Therefore, it is apparent that innovative methods are needed to resolve the disparities that negatively impact Black adolescent girls in the United States.
Highlighting Strengths in Black Adolescent Girls to Reduce Risk
Studies that have examined sexual health and drug use among Black adolescent girls often highlight risk factors that are commonly present in urban communities such as over exposure to illicit and licit drug use, violence, lack of drug and sexual health education, and parental and peer substance abuse (Aronowitz et al., 2006; Floyd & Brown, 2013; Leventhal & Brooks-Gunn, 2000; Opara et al., 2019a, b; Voisin, Jenkins, & Takahashi, 2011). Such research, unintentionally, ignores the resiliency of Black adolescent girls and how that resiliency is nurtured, especially those that live in urban neighborhoods that are able to navigate such communities and not engage in risk-taking behaviors due to protective factors present in their environments. For example, substance use prevention initiatives have heavily focused on removing outlets that sell substances/drugs in communities and other complex challenges in urban environments (Reid, Yu, & Garcia-Reid, 2014; Rush & Urbanoski, 2019), shaming adolescent girls whom have sex, and promoting abstinence and individual behavioral change through educating youth about drug and sexual risk behaviors (Lamb & Peterson, 2012). It is important to acknowledge that the presence of risk factors does not necessarily equate to an influx of risky behaviors in Black adolescent girls living in urban neighborhoods. Yet, very few studies have examined the protective factors that have guarded Black adolescent girls in urban communities against sexual risk behaviors and drug use (Opara et al., 2019a, b; Sanchez, Hamilton, Gilbert, & Vandewater, 2018; Schinke, Di Noia, Schwinn, & Cole, 2006).
Through a strengths-based lens, components of empowerment theory can provide a framework for reducing risk and highlighting strengths for Black adolescent girls. Empowerment is a process by which individuals gain mastery and gain a critical awareness of their environment (Zimmerman, 1995). Empowerment processes and outcomes vary in their observed form because no single standard or measure can fully capture their meaning for all people in all contexts (Rappaport, 1987; Zimmerman, 1995). Empowerment researchers have focused on studying individual and contextual factors to promote and prevent drug use and sexual risk behaviors among adolescents, unlike previous work that focused heavily on the removal of individual and contextual level risk factors (Beeker, Guenther-Grey, & Raj, 1998; Reid, Hughey, & Andrew Peterson, 2003). Psychological empowerment (PE) is the individual level of analysis of empowerment, representing individual’s ability to apply control and a critical understanding of their sociopolitical environment (Zimmerman & Zahniser, 1991). PE is a construct that includes intrapersonal, interactional, and behavioral components (Zimmerman & Zahniser, 1991; Zimmerman, 2000). The intrapersonal component refers to how people think and feel about their ability to influence social and political systems that can enact positive social change. This component, also referenced as the emotional component, has received the greatest attention in extant research on PE. Intrapersonal empowerment. PE includes beliefs about one’s capability to exert control and gain a critical understanding of their sociopolitical environment. Due to this notion, a majority of empowerment researchers have focused on the interpersonal component of PE as an indicator of PE overall (Christens, Collura, & Tahir, 2013; Cooper et al., 2015; Hughey, Peterson, Lowe, & Oprescu, 2008; Miguel, Ornelas, & Maroco, 2015; Peterson, Peterson, Agre, Christens, & Morton, 2011; Lardier, Garcia‐Reid, & Reid, 2018a; Opara, Lardier Jr, Reid, & Garcia-Reid, 2019b). Therefore, to be consistent with empowerment literature and previous research, PE was operationalized as intrapersonal empowerment for this study. A significant body of research has also identified the relationship between PE and drug use among adolescents (e.g., Christens, Peterson, & Speer, 2011; Opara et al., 2019b; Lardier et al., 2018a; Peterson & Reid, 2003) solidifying the influence PE can have on reducing drug use. However, very few, if any, have focused primarily on Black adolescent girls.
Social Support
Social support is one of the most important antecedent protective factors that contributes to positive adaptation outcomes. Social support in this study is described as a three-dimensional construct that includes family, peers, and school supports (Cauce, Felner, & Primavera, 1982). Social support has been found to be extremely beneficial in improving the likelihood of positive developmental outcomes in Black adolescent girls, particularly against sexual risk taking and drug use (Carter, Caldwell, Matusko, & Jackson, 2015; Hope, Lee, Hsieh, Hurd, Sparks, & Zimmerman, 2019; Opara et al., 2019b; Schinke et al., 2006). Within a cultural context, the concept of family is a crucial part of Black families (Cross, Taylor, & Chatters, 2018; Lindsey, Joe, & Nebbitt, 2010). The contribution of positive family support is invaluable in the lives of Black adolescent girls as the lack of quality family support is associated with higher drug use rates, sexual risk behaviors, early pregnancy, and poor school outcomes (Collins & DeRigne, 2017; Hutchinson & Cederbaum, 2011; Hutchinson et al., 2012; Schinke et al., 2006). Social support from peers can also serve as a protective buffer for adolescents residing in under-resourced urban communities (2007; Garcia-Reid, Lardier Jr, Reid, & Opara, 2018; Peterson, Buser, & Westburg, 2010). Adolescent girls whom report higher levels of positive peer support, are more likely to have higher graduation rates, higher grades, perceive drug use as risky, and have lower levels of sexual risk taking (Drolet & Arcand, 2013; Garcia-Reid et al., 2018; Golden, Griffin, Metzger, & Cooper, 2018). Research has confirmed that adolescent girls tend to appreciate and respond to supportive networks which allows them to form close-knit friendships which can influence them to engage in more positive behaviors (Garcia-Reid et al., 2018; Way, 2013). When compared to Black adolescent boys who may adapt to masculine roles that prohibit them from forming intimate bonds with their peers, supportive peer networks appear to work favorably for adolescent girls (Way, 2013). Due to societal and gender norms and expectations placed on girls at an early age, social support remains a key factor in their positive development (Garcia-Reid et al., 2018; Opara, Lardier, Herrera, Garcia-Reid, & Reid, 2019a). Such norms allow adolescent girls to form meaningful friendships that have deep intimacy, providing high levels of social support more effortlessly than boys (Garcia-Reid et al., 2018). Among Black adolescent girls, Carter, Caldwell, Matusko, and Jackson (2015) found that higher levels of perceived peer support, in turn, predicted lower levels of depressive symptoms. Opara, Lardier, Herrera, Garcia-Reid, and Reid (2019a) found in their study on Black and Latina girls that Black girls reported the importance of having positive peer influences in their lives as a protective factor in not engaging in drug use. Positive peer support can offer the vital emotional and practical support needed to manage health concerns and prevent Black adolescent girls from engaging in risky behaviors such as drug use and sexual risk-taking practices.
Social resources that originate from one’s formal and informal social networks that serve specific needs are referred to as social capital (Clark, Williams, Park, Schulz, Williams, & Holt, 2018). Individuals’ relationships with family, friends, and neighbors comprise social capital. The concept of social support can be related to social capital theory as a framework that aims to understand protective and supportive structures that can serve as a buffer for adolescent girls. Social capital includes “social networks, emotional bonds and habits of reciprocity that promote trust and cooperation” (Hosen & Solovey-Hosen, 2003, p. 84). Within social capital measures, evidence was found to support a three-factor model based on residential community and neighborhood factors including interconnectedness (trust people in community, talk to others in community), social support (able to rely on others for help), and community participation (ability of self and neighbors to influence decisions in the community) (Perry, Williams, Wallerstein, & Waitzkin, 2008). Social capital has been found to be associated with and used as a measurement of how networks can provide social support (Christens et al., 2013). In addition, social capital has been theorized to relate to psychological empowerment (Christens et al., 2013). Although social capital theory can be useful in understanding how supportive structures within a community can protect Black adolescent girls from engaging in drug use and sexual risk behavior, this research seeks to move beyond social capital towards an interpersonal level of empowerment based on supportive networks.
Ethnic Identity
Ethnic identity refers to (a) self-identification with a specific ethnic group; (b) the sense of belonging and attachment to such a group; (c) the perceptions, behaviors, and feelings one has due to such membership; (d) and involvement in the cultural and social practices of the group (Phinney, 1989; Phinney, Horenczyk, Liebkind, & Vedder, 2001; Phinney & Ong, 2007). Research is beginning to emerge that reveals an association between ethnic identity and risky behaviors (Belgrave, Brome, & Hampton, 2000; Corneille & Belgrave, 2007; Lardier et al., 2018a; Sanchez et al., 2018). Thus, the notion of strengthening ethnic identity in individuals may be an effective and innovative approach to promoting healthy and positive behaviors among youth of color. A strong relationship between ethnic identity and drug use has been reported in the few studies that have examined both variables. For example, researchers found that higher levels of ethnic identity align with lower use of drugs including tobacco, alcohol, and marijuana, and with drug abstinence and drug-free attitudes (Belgrave et al., 1997, 2000; Lardier et al., 2018a; Opara et al., 2019b; Sanchez et al., 2018). Researchers have concluded that individuals who have low levels of ethnic identity are more likely to experience low self-esteem, shame, and anxiety (Rivas-Drake et al., 2014), and are more likely to use drugs and alcohol, which may be a coping mechanism for undiagnosed and untreated mental health symptoms (Fisher, Zapolski, Sheehan, & Barnes-Najor, 2017). As a protective factor, increasing one’s ethnic identity may also impact drug use through its positive relationship with self-esteem and self-worth (Fisher et al., 2017). Ethnic identity may influence drug use by improving self-esteem, reducing psychological emotions, and normalizing positive group norms and cultural values.
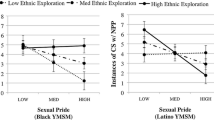
Understanding the relationship between ethnic identity and sexual risk behavior among Black adolescent girls remains limited in the literature. Belgrave, Brome, and Hampton (2000) found that ethnic identity significantly aligned with positive sexual attitudes and values after predictors such as age, family cohesion, self-esteem, and school interest were controlled for among adolescent girls. Beadnell et al. (2003) found that ethnic identity aligned with African American women not engaging in sexual risk-taking behaviors such as having sex with multiple partners and remaining abstinent from sex. Shehadeh, Rubens, Attonito, and Jennings (2018) found that among African American and Latino/a/x migrant workers, higher levels of ethnic identity aligned with lower levels of engaging in sexual risky behaviors including unprotected sex. Futhermore, interventions for sexual risk behavior prevention that are tailored to Black girls and women often focus on increasing ethnic identity and pride (e.g., DiClemente & Wingood, 1995). The association between two constructs can relate to feelings of self-worth, self-esteem, and pride of oneself, which can buffer mental health effects that may mediate the relationship between self-characteristics and sexual risk behaviors.
Current Study
The current study aims to change the deficit narrative on Black adolescent girls in prevention research. This study aims to highlight the strengths of Black adolescent girls by identifying protective factors such as psychological empowerment, social support, and ethnic identity on drug use and sexual risk behaviors. Ethnic identity, social support, and psychological empowerment (PE) were included in the model as predictors, drug use as a mediator and sexual risk behaviors as an outcome using path analysis techniques. It was hypothesized that lower levels of drug use would mediate the relationship on sexual risk behaviors due to higher levels of perceived social support, higher levels of ethnic identity, and psychological empowerment. We alternatively tested social support as a mediator based on the recent literature which supports the influence of social support on positive developmental outcomes in Black adolescents (Clark, Williams, Park, Schulz, Williams, & Knott, 2019).
Method
Participants
The study uses a sample of 340 Black female adolescents (14–17 years old; Mage = 16.1, SD = 1.16) who reside in a northeastern urban community in New Jersey. The majority of students were between 15 and 17 years of age (62%). At the time of data collection, 10% were in 10th grade, 11% were in 10th grade, 47% were in 11th grade, and 31.1% were in 12th grade. Over 70% of the sample reported receiving free or reduced school lunch, an indicator of low socioeconomic status (SES; Harwell & LeBeau, 2010).
Procedures
The study received approval from the Institutional Review Board at the Lead Principal Investigator’s University. Data used in this study were accrued for the purposes of a comprehensive needs assessment in a northeastern U.S. urban school district to aid in the development and implementation of a federal initiative to prevent drug abuse and sexual risk behaviors among racial and ethnic minority youth in an urban community (Reid & Garcia-Reid, 2013). The target city has a total of eight public high schools, and they were all selected to be a part of the study. Survey participants were recruited through physical education and health classes, as these classes are required all four years of high school in order to obtain a racially-diverse, representative sample of the students in the city. This process allowed for an equal sampling of high school students that would be representative of the school district. The participating school district allowed parent permissions slips to be sent home to all students. All students who returned permission slips and signed youth-assent forms were eligible to take the survey. We administered the survey to students during their health-education classes. Students completed a survey that consisted of approximately 222 questions during 1-h time periods in class. The survey included validated measures: social support (Cauce et al., 1982), ethnic identity (Phinney, 1989; Phinney & Ong, 2007), psychological empowerment (e.g., Christens & Peterson, 2012; Peterson et al., 2011), 30-day drug use, and sexual risk behavior (Kann et al., 2014).
Measures
Social Support
The condensed version of the Social Support Rating Scale (SSRS) measures social support or attachment to members of the community (Cauce et al., 1982). This scale consists of eight items evaluating social support among adolescents from a variety of sources, including principals, teachers, and friends. Cauce, Felner, and Primavera (1982) validated this scale among a sample of high-risk adolescents and discovered three support dimensions in the scale: family (parents and relatives), formal (e.g., teachers, principals, and state workers), and informal (e.g., friends and peers) support, which accounted for 95% of the total variance. Principal component analysis with an orthogonal varimax rotation was performed to conduct factor analysis on the eight items of the SSRS into meaningful dimensions of social support to develop this scale which showed a good model fit (Cauce et al., 1982; Cauce, Mason, Gonzales, Hiraga, & Liu, 1994).
Respondents indicated the level of helpfulness provided by each source based on a 5-point, Likert-type scale ranging from 1 = not at all helpful to 5 = very helpful. Social support scores were calculated for each participant by summing the perceived helpfulness ratings of each item (Cronbach’s α = 0.79; M = 3.04, SD = 0.80). Scale scores were the mean of the eight items. Higher responses indicate higher levels of perceived social support. The internal reliability of the scale is consistent with other studies using the SSRS (Cauce et al., 1994; Kazak & Meadows, 2013; Lardier et al., 2019a, b; Opara et al., 2019b; Peterson et al., 2011). Moreover, evidence of convergent validity was established via further analyses, which indicated high correlations of the SSRS with existing measures of parental, peer and informal supports (Ahmed, Minnaert, van der Werf, & Kuyper, 2010, 2007; Garcia-Reid et al., 2018).
Psychological Empowerment
The Sociopolitical Control Scale for Youth (SPCS-Y) is a widely used measure and indicator of psychological empowerment (Zimmerman & Zahniser, 1991). Respondents were asked to indicate their level of agreement with statements such as “I am a leader in groups” and “I can usually organize people to get things done.” Responses were recorded using a 5-point Likert-type scale ranging from the Strongly disagree (1) to Strongly agree (5).
Using confirmatory factor analysis, several studies support SPCS-Y as a one factor measure (Holden, Evans, Hinnant, & Messeri, 2005; Peterson et al., 2011) and as a two-factor measure, encompassing both leadership competence and policy control (e.g., Opara et al., 2020). Using confirmatory factor analysis, Opara, Lardier Jr, Reid, and Garcia-Reid (2019b) found that the sociopolitical control for youth had a good model fit among a sample of ethnic minority female adolescents (root mean square error of approximation = 0.03). For this study, the SPCS-Y was measured as one factor construct operationalizing psychological empowerment (Cronbach’s α = 0.88; M = 63.47, SD = 10.32). The items were summed and participants responded with overall higher composite scores of sociopolitical control. Responses ranged from a low of 17 to high of 85. Evidence of convergent validity was established based on evidence from studies that showed high correlation between sociopolitical control and related variables such as cognitive empowerment (Lardier, Opara, Garcia-Reid, & Reid, 2020; Miguel et al., 2015).
Multigroup Ethnic Identity Measure (MEIM)
The MEIM is one of the most widely used self-reported measures for ethnic identity (Phinney, 1989; Phinney & Ong, 2007). For this study, Cronbach’s α = 0.86; M = 53.81, SD = 8.91. We measured responses using a 4-point Likert-type scale ranging from Strongly disagree (1) to Strongly agree (4). Scores on the MEIM have shown evidence of good reliability as well as construct and criterion-related validity ranging from 0.81 to 0.92 (Phinney & Ong, 2007; Ponterotto, Gretchen, Utsey, Stracuzzi, & Saya Jr, 2003). Scores were totaled by summing responses, with higher scores representing greater ethnic identification (Cronbach α = 0.86). Responses on the original MEIM ranged from 20 to a maximum of 80.
The MEIM was first validated among Black youth and has been subsequently validated among diverse groups across the United States and internationally (Kazarian & Boyadjian, 2008) using confirmatory factor analysis. Results of the confirmatory factor analysis showed that the ethnic identity scale yielded a good fit across various adolescent ethnic groups (root mean square error of approximation = 0.037; Phinney & Ong, 2007; Roberts, Phinney, Masse, Chen, Roberts, & Romero, 1999). The MEIM has shown evidence of reliability and validity in African American samples (Espinosa-Hernández & Lefkowitz, 2009), particularly Black adolescent girls (Neblett Jr, Rivas‐Drake, & Umaña‐Taylor, 2012; Sanchez et al., 2018).
Sexual Risk Behavior
Six items were adapted from the National Youth Risk Behavior Survey, which assesses sexual behavior among high school aged adolescents. These items included: having ever had vaginal sex, how many times participants had sex in the past 3 months, number of lifetime sexual partners, age of first sexual intercourse, having sex under the influence of drugs and alcohol, and having unprotected sex without a condom. We considered examining each sexual behavior separately; however, that approach could have underestimated risk (e.g. Kogan et al., 2008). Respondents were asked to indicate: “How many times did you have sexual intercourse in the past three months?” with the following response options: 0 = never, 1 = 1 time, 2 = 2 times, 3 = 3–5 times, 4 = 4–5 times, 5 = 11–20 times, 6 = 20 times or more. Participants were instructed to define sexual intercourse as vaginal or anal intercourse. Participants were also asked, “How often in the past three months have you had sex while under the influence of alcohol or drugs?” with response options ranging from 0 = never to 6 = always and “How old were you when you first had sexual intercourse” with response options ranging from 10 years old to 16 years (M = 16.4 years old). Having sex before age 14 years old is considered high sexual risk behavior (Jackson et al., 2015; Kann et al., 2014). Therefore, we used categorical variables for “age of first sexual intercourse” (1 = sex before age 13 or at age 14 or older = 0; Akers et al., 2009). In addition, “number of lifetime partners” (1 = greater than 3 lifetime partners or 0 = less than 3 lifetime partners; e.g. Akers et al., 2009) were transformed into categorical variables. For this study, Cronbach’s α = 0.75; M = 7.12, SD = 3.6. Consistent with other studies, the scale has high internal reliability and validity (Peterson et al., 2010). Higher responses indicated higher levels of sexual risk behavior engagement among participants.
30-Day Drug Use
Past 30-day drug use was measured using items from the National Survey on Drug Use and Health and Youth Risk Behavior Survey. The scale consisted of three items that assessed how often participants smoked cigarettes, drank alcohol, and smoked marijuana in the past 30 days. An example of an item is, “Estimate the number of days you used marijuana or hashish in the last 30 days.” Participants responded to these items on a 7-point scale (1 = 0 days; 2 = 1–2 days; 3 = 3–5 days; 4 = 6–9 days; 5 = 10–19 days; 6 = 20–29 days; 7 = all 30 days). The sum of this scale is the mean of responses on the three items, with higher scores indicating greater frequency of use. Based on prior research, the drug-use-variable construct had a Cronbach’s α ranging from 0.89 to 0.96 (Peterson et al., 2010). For this study, Cronbach’s α = 0.78; M = 4.38, SD = 2.31. Based on prior research, the substance use construct of the drug use, developed by Youth Risk Behavior Survey (Kann, et al. 2018) has been identified to have an internal consistency and validity that ranged from 0.89 to 0.93 (Phillips et al., 2017; Peterson et al., 2010; Sanchez et al., 2018). Consistent with previous research studies in empowerment, a mean of all three items was calculated (e.g., Christens & Peterson, 2012; Garcia-Reid et al., 2013; Opara et al., 2019b). Responses ranged from 1.00 to 7.00, with 7.00 representing the use of substances during all 30 days previous to being surveyed. In this study, on average youth disclosed lower mean rates of 30-day substance use. Other illicit drug use (i.e. heroin, cocaine, ecstasy) were not included in the analyses as the prevalence rates for use were extremely low in this sample.
Several fit indices that researchers were used to determine good model fit (Hoyle, 1995). These measures included the chi-square (χ2) test, minimum discrepancy per degree of freedom, comparative fit index (CFI), Tucker–Lewis Index (TLI), root mean square error of approximation (RMSEA), Akaike information criterion, and Bayesian information criterion (West, Taylor, & Wei, 2012). Nonsignificant χ2 values indicated acceptable model-fit; however, χ2 must be considered in tandem with other fit indices, as χ2 may be a too stringent and often-unrealistic standard of GFI (West et al., 2012). Bollen–Stine (1992) bootstrap approach was used to handle potential issues of nonnormality in data, with 10,000 bootstrap resamples used, which is considered robust. Researchers have observed Bollen–Stine bootstrap procedures as an appropriate method of handling nonnormal data, particularly in larger samples (i.e., N ≥ 200; Nevitt & Hancock, 2001).
Analytic Strategy
Path analysis was conducted used (AMOS) software version 23.0 (Arbuckle, 2014). Path analysis was employed to evaluate the relationship between three observed measures—psychological empowerment, social support, and ethnic identity—with sexual risk behavior and the mediating role of drug use. Path analysis is used because variables are treated as observed and all variables are measured without error (West et al., 2012). Other studies have used this approach when analyzing observable variables on Black adolescents (i.e., Banerjee, Rivas-Drake, & Smalls-Glover, 2017; Clark et al., 2019). A latent variable approach offers the potential advantage in path analysis as it enables measurement error to be considered (Bollen & Stine, 1992). As an initial prior-to-testing structural model, bivariate correlations were computed between social support, ethnic identity, and psychological empowerment. Social support, PE, and ethnic identity negatively correlated with drug use and sexual risk behavior.
Drug use was tested as a mediator in the hypothesized model and social support was tested as a mediator in the alternative model. A mediating model must meet the following criteria: The mediating variable (e.g., drug use) must significantly relate to the independent variable (e.g., social support); the dependent variable (e.g., sexual risk behavior), and significantly relate to the mediating variable. A mediating role is suspected when a previously significant relationship between the independent variable (e.g., social support) and dependent variable (e.g., sexual risk behavior) substantially diminishes when the mediation variable (e.g., drug use) is entered into the equation.
Although an important advantage of conducting path analysis over standard regression methods is that path analyses provides model‐fit information about the consistency of the hypothesized mediational model to the data and the plausibility of causality assumptions made when constructing the mediation model (Imai, Keele, & Tingley, 2010). There are limitations present with regard to examining mediation cross‐sectionally (Kline, 2015). However, to address such limitations, sensitivity analyses with alternative modeling specifications were used to address potential methodological biases (Podsakoff, MacKenzie, & Podsakoff,, 2012), as well as assess mediation against an equally persuasive alternative model (Thompson, 2000). See Fig. 1, Model 2, for a hypothesized alternative model.

Hypothesized Model 1 and Alternative Model 2
For the current study, we draw on a sample of Black adolescent girls that live in the same urban community. As previously mentioned, path analyses were employed to evaluate the relationship between psychological empowerment, social support, and ethnic identity with sexual risk behavior and the mediating role of drug use. In particular, we aimed to answer the following questions and building upon the existing research, we hypothesized the following (Fig. 1):
Q1
What is the relationship between the three observed measures—psychological empowerment, social support, and ethnic identity—with sexual risk behavior, and what is the mediating role of 30-day drug use?
H1
Ethnic identity, social support, and psychological empowerment would be directly associated with drug use and indirectly related to sexual risk behavior.
Q2
What is the mediating role of 30-day drug use between the relationship of the three observed measures and sexual risk behavior?
H2
30-day drug use would mediate the association between ethnic identity, social support, and psychological empowerment have with sexual risk behavior.
To contribute meaningfully to the literature, we utilized an alternative modeling strategy (see Fig. 2 for alternative model) to examine associations against an alternative-theoretically supported model. Results will provide important implications for protective factors in drug use and sexual risk behavior among Black adolescent girls.

Standarized path diagram testing drug use as a mediator on sexual risk behavior as outcome (N = 340); [(χ2(4) = 5.624, p = .229) RMSEA = .035 (90% CI = [.00, .09]); GFI = .99, AGFI = .96, CFI = .99]. CMIN/DF = 1.11. *p < 0.05, **p < 0.01, ***p < 0.001. AGFI adjusted goodness‐of‐fit index, CMIN/DF discrepancy‐to‐degrees of freedom (df) ratio, GFI goodness‐of‐fit index, RMSEA root mean square error of approximation
Results
Descriptive Statistics
See Table 1 for the correlation matrix. The variable 30-drug use was correlated with all variables. Social support was correlated with all main analytic variables. Ethnic identity was correlated with all variables. Psychological empowerment was correlated with all the variables except sexual risk behavior.
Tests of normality and collinearity were examined prior to conducting main analyses. Criteria for normality included kurtosis of at no more than 3 and skewness of 0 (Field, 2013). After examining variables for normality, 30-day drug use was shown to be non-normal. Other researchers reported similar findings (e.g., Christens & Peterson, 2012; Lardier et al., 2018a). SPCS-Y, which scholars use to measure PE, social support, sexual risk behavior, and MEIM (used to measure ethnic identity) displayed normal distributions (Christens & Peterson, 2012; Peterson, Lowe, Hughey, Reid, Zimmerman, & Speer, 2006; Peterson et al., 2011; Phinney, 1989; Phinney & Ong, 2007). To summarize, all variables included in analyses were in the appropriate parameters, with the exception of 30-day drug use, which was highly skewed (3.65) and leptokurtic (16.39) as expected (Lardier et al., 2018a). Transformation procedures were not employed due to analyses being conducted in AMOS SEM software, which examines the covariance matrix through maximum likelihood (ML) estimations and reduces issues with normality and impact on parameter estimates (Hancock & Liu, 2012). A priori alpha level was set to p < 0.05 for the analyses.
Figure 2 displays the overidentified path model, which displays only statistically significant paths and presents standardized β weights. The model showed a good fit to the data, evidenced by the fit indices [(χ2(4) = 5.624, p = 0.229) RMSEA = 0.035 (90% CI = [0.00, 0.09]); TLI = 0.98; CFI = 0.99; AIC 53.64 (saturated = 65.00), and BIC 145.63 (saturated = 163.21)]. This model accounted for 42% of the variability in social support, 74% of the variability in ethnic identity, 78% of the variability in PE, 10% of the variability in 30-day drug use, and 12% of sexual risk behavior. Such variable (r2) results are not uncommon when considering that numerous variables are also likely to predict drug use and sexual risk behavior. Bollen–Stine bootstrapping results were not significant: p > 0.05 (p = 0.08), indicating that the proposed model was consistent with the sample data (Bollen & Stine, 1992).
Figure 2 indicates that social support, ethnic identity, and PE had a significant negative direct relationship with 30-day drug use as a mediator on sexual risk behavior. Social support had a direct effect on sexual risk behavior (β = − 0.11; p < 0.001). Using bias corrected bootstrap confidence intervals, the following indirect associations from psychological empowerment, ethnic identity, and social support through drug use as a mediator were significant: participation in social support on sexual risk behavior through 30-day drug use (indirect effect = − 0.17, 95% CI = 0.01–0.03, p = 0.001); PE on sexual risk behavior through 30-day drug use (indirect effect = − 0.03, 95% CI = 0.03–0.06, p = 0.001); and ethnic identity on sexual risk behavior through 30-day drug use (indirect effect = − 0.04, 95% CI = − 0.04 to − 0.22 p = 0.002). Hypothesis 1 was confirmed based on the results. Of the association between participation in social support and 30-day drug use, 30-day drug use mediated 96%, of the association between PE and sexual risk behavior, 88%, and of the association between ethnic identity and sexual risk behaviors. Furthermore, 30-day drug use was shown to have a significant positive direct relationship with sexual risk behavior (β = 0.63; p < 0.001). Hypothesis 2 was confirmed based on the results (Table 2).
When testing the alternative model specification (Fig. 1, Model 2), it was found that the overall model fit to the data was less than adequate when compared to that of the original model; specifically, fit indices were as follows: χ2(13) = 19.01, p = 0.01, and the discrepancy‐to‐df ratio, 2.51. Both were outside the range of acceptable model‐to‐data fit. The other fit indices also indicated less than adequate model fit. The RMSEA 0.13 (90% CI = 0.08, 0.15), TLI 0.92, AIC 53.32, BIC 50.84. When comparing the AIC and BIC, the hypothesized model provided the best fit to the sample data. The value of AIC was 53.64 for the hypothesized model and 51.04 for the alternative model, with the hypothesized model AIC closest to the saturated model of 65.00, which indicates that the hypothesized model provided a better fit to the sample data. The BIC was 145.63 for the hypothesized model and 156. 89 for the alternative model, with a difference greater than 10.00 present, indicating that the hypothesized model with the lower BIC had a better fit to the sample data (West et al., 2012). Bollen–Stine bootstrap results also indicated that the p value was not > 0.05 (p = 0.02), indicating that the model‐fit is poor and that issues with model specification are present with the current sample data (Enders, 2006). Consequently, bias‐corrected bootstrap confidence intervals to test indirect paths yielded non-significant results. This suggests that mediation in the alternative model was not present and no results are provided for this model. Therefore, it is reasonable to conclude that the most probable order of association is that participation in psychological empowerment, ethnic identity, and social support have a negative relationship with sexual risk behavior mediated by 30-day drug use.
Discussion
This study is one of the few to specifically measure PE in addition to social and cultural factors (e.g., social support and ethnic identity) among Black adolescent girls. Although empowerment is a protective individual-level component that contributes to better developmental outcomes, very few studies have conceptualized the construct of empowerment in Black adolescent girls. Researchers consistently showed PE to align with low occurrence of risky behaviors such as drug/substance use among youth of color (Peterson & Reid, 2003; Peterson et al., 2011). For this study, 30-day drug use was tested as a mediating variable between PE, ethnic identity, social support on sexual risk behavior. According to the results, PE, social support, and ethnic identity had a negative relationship with 30-day drug use, which significantly mediated the relationship with sexual risk behavior. This is an important finding because reducing drug use among Black adolescent girls can be an effective approach to reducing sexual risk behavior as can the presence of individual, social, and cultural factors.
Although PE is often used in empowerment research to predict developmental outcomes such as drug use among youth, very limited empirical evidence supports the association between empowerment using the intrapersonal empowerment measure (SPCS-Y) on sexual risk behaviors. However, similar studies examining the association between empowerment using other measures and sexual activity showed promising results (e.g., Reininger, Pérez, Aguirre Flores, Chen, & Rahbar, 2012). Social support was tested in the hypothesized model as an endogenous variable of and also as a mediator in the alternative model. Consistent with prior research, Black adolescent girls who had higher levels of social support and did not use drugs were also more likely to not engage in sexually risky behaviors. Research supports both the hypothesized and alternative model approaches in examining social support and its relationship on drug use and sexual risk behavior. It can be explained that social support can influence ethnic identity and empowerment among adolescent girls, therefore impacting girl’s engagement in risky behaviors (Clark et al., 2019). However, the alternative model was not a good fit to the data. Indicating that 30-day drug use as a mediator in the model had a more influential role in explaining the relationship between social support, ethnic identity, and psychological empowerment on sexual risk behavior. Researchers documented the importance of social support on sexual risk behaviors among adolescent women (Reininger et al., 2012). Consistent with prior research on the importance of familial and positive peer networks among Black adolescent girls, findings revealed that social support is a crucial protective factor (Garcia-Reid et al., 2018; Hutchinson et al., 2012; Schinke et al., 2009).
Consistent with the literature, sexual risk behavior and drug use had a significant positive relationship, suggesting adolescent girls with lower levels of drug use or no drug use were more likely to have lower levels of sexual risk behavior. Drug use appeared to have a direct negative association with ethnic identity and sexual risk behavior, indicating that the girls in this study who had high levels of ethnic identity were less likely to engage in drug use in the past 30 days. An explanation for this finding can be that Black adolescent girls who do not engage in risky behaviors may have higher levels of pride and cultural values that incline with messages of self-worth, positive role models with whom they can identify from the perspective of race and gender, and support that promotes healthy behaviors. This is consistent with literature that supports the role of ethnic identity and low drug use levels among Black adolescents (Belgrave et al., 1997, 2000; Lardier et al., 2018a; Sanchez et al., 2018).
Implications
Findings from this study provide promising results to shape research and social work practice. It is important to note that the burden to end youth substance use and reduce sexual health disparities should not fall on the shoulders of Black adolescent girls. Instead, the authors provide an alternative approach to viewing the complex phenomena and how highlighting the strengths of Black adolescent girls, their supportive networks, can be used as a prevention strategy to reducing drug use and sexual risk behaviors. The aims of this study were to highlight the strengths of Black adolescent girls and their supportive networks, discuss the importance of cultural values, and learn from the experiences of Black adolescent girls who are not engaging in risky behaviors, to inform prevention research. These findings suggested that prevention research, interventions, and programming should be informed by the experiences of Black adolescent girls by highlighting protective factors that can be incorporated to buffer risk exposure. Often substance abuse and sexual-health researchers view adolescent Black girls from a deficit perspective, highlighting the risks present in their neighborhoods and within culture and overemphasizing engagement in risky behaviors. Ignoring the factors that are present for girls who are not engaging in risky behaviors can be detrimental for Black young girls and further marginalize them as a group. Thus, this study aimed to enhance the use of cultural values and continuously discuss protective factors and strengths to step away from the risk perspective.
Research
This study supports the advancement of Black adolescent girls, whose backgrounds have been historically marginalized, to engage in roles that not only support leadership and political engagement but engage in spaces where they are supported by family, peers, and adult mentors who can assist in nurturing their needs. Because Black adolescent girls who belong to marginalized backgrounds and identities are often forced to be resilient, empowerment researchers can begin to explore the role of political engagement that fosters resilience. Empowerment researchers can begin to highlight this view using empirical evidence to encourage programming with Black adolescent girls, engaging in methods that foster critical-consciousness thinking that can support their resilience, bolster their confidence, instill pride (i.e., racial, ethnic, and gender pride), thereby improving developmental outcomes. Researchers have consistently viewed strengthening ethnic identity among Black adolescent girls as able to buffer engagement in risky behaviors (Javier et al., 2007; Opara, Rivera Rodas, Lardier Jr, Garcia-Reid, & Reid, 2020; Sanchez et al., 2018). Using research findings, it can be inferred that developing organizational activities that foster empowerment can also incorporate deep cultural values and principles that allow young girls to simultaneously become more attached to their community and self-identify while challenging structural factors that have placed them at risk historically. Thus, allowing Black adolescent girls to continue to feel more empowered and in control of their health. We encourage researchers to continue to investigate differences in ethnic identity versus racial identity and also seek to understand how differences in ethnicity/racial identity and pride can impact sexual risk behaviors and drug use.
Practice
It is important that social work clinicians acknowledge that historically marginalized families should feel valued and applauded for their work in challenging negative narratives and stereotypical beliefs about their groups. As urban Black families are more likely to live in communities that experience structural inequalities related to segregation, drug use, and violence, the ability of parents, educators, and adult allies to continue to teach their daughters’ drug-resistance strategies should be highly regarded (Opara et al., 2019a). In addition, because drug use was a significant mediator between protective factors and sexual risk behaviors, findings suggested that by preventing drug use/abuse, prevention researchers can simultaneously reduce sexual risk behaviors. The use of empowerment theory in this study highlights how diverse families, through social support, respond to historical and social inequalities by engaging in leadership and politics as a protective instrument for Black adolescents. The incorporation of this lens in prevention research and clinical practice would allow for more targeted substance-abuse and HIV/STI prevention programs. Findings encourage clinicians to highlight the strengths in families of color and move away from a deficit model. Psychological empowerment was found to be a significant protective factor for Black adolescent girls in the sample. Incorporating empowerment strategies within interventions has the potential to improve self-efficacy in adolescence as they transition into adults. Such strategies including teaching girls how to feel empowered and liberated to talk about sex with their partners and also engaging in protective sexual behaviors such using condoms while having sex (e.g. Javier, Abrams, Moore, Belgrave, 2018). Ethnic identity was shown to have a strong association with lower levels of drug use and sexual risk behavior. Research has shown the connection between ethnic identity and risk behaviors among adolescents and our study findings are consistent with research on ethnic identity (Belgrave et al., 2000; Lardier et al., 2018a; Opara et al., 2019b; Sanchez et al., 2018). Interventions that model an Africentric approach, ideally incorporating the discussion of traditional African philosophies and the historical experiences of African Americans living in the United States, can be seen as an empowering approach for Black adolescent girls. Africentric cultural values consist of a set of beliefs, values, and assumptions founded on African cultural traditions that relate to definitions of the identity and the relationship of the self with the environment (Belgrave et al., 2000; Sanchez et al., 2018). As social support was a significant finding in this study, which includes the construct of family support, peer support, and support from other adult allies (i.e., social workers and teachers), study results support the importance of family programming as a key determinant in reducing substance use and sexual risk-behavior prevention among Black adolescent girls. Using family-based interventions in community work is essential, honoring the special relationship Black adolescent girls have with their families and other supportive adults in their lives. Practitioners should begin to understand how young Black girls’ social identities intersect and operate in their lives and environments and how their strengths as young women are crucial.
Strengths and Limitations
This study moves away from deficit-focused research and examines the social and cultural factors that can serve as protective effects for young Black girls. Second, this study is part of a growing body of literature on empowerment research over the last decade that empirically tests PE using rigorous methodological techniques such as path analyses. This study also advances research on the mediating influence of drug use and its association with sexual risk behavior between social support, ethnic identity, and PE among low-income Black girls. Fifth, this study provides preliminary evidence that ethnic identity, social support, and PE are significant protective factors in reducing risky behaviors among Black adolescent girls living in an urban community. Study findings contribute significantly to not only empowerment research, but to the adaption of intersectionality theory in family science and public health research, and anti-deficit-focused prevention work for young girls and women of color living in urban communities.
Despite its strengths, a few limitations should be acknowledged. First, due to the cross-sectional nature of the survey design, it is difficult to establish a causal relationship between variables and empowerment processes and outcomes. Cross-sectional studies provide an appropriate foundation to design future longitudinal studies. Future work should aim to replicate this study with a longitudinal design. The second limitation is the testing of adolescent Black girls as a group. Black adolescent girls are not a homogenous group and have significant within-group differences. Given the various ethnicities that comprise the Black population (e.g., Caribbean and African), it is essential for researchers to collect and test differences among various ethnicities that may highlight significant findings in how ethnic groups operationalize empowerment and key protective factors that may vary by ethnic group.
The third limitation involves the measurement of PE and how it was conceptualized in the study. Although several studies that examined PE did so using the SPCS-Y, this scale only measures the intrapersonal aspects of PE (Christens & Peterson, 2012). Because empowerment theory is hierarchal and multilevel, future researchers should aim to validate and develop scales that examine all constructs present in empowerment theory. Such scales should be specifically developed for young girls of color living in urban neighborhoods.
Additionally, the measure used to operationalize drug use in the sample only measured marijuana, tobacco, and alcohol use within the past 30 days which can be seen as a limitation. For future work, we urge researchers to include other substances that may be commonly used among adolescents (e.g. e-cigarettes, marijuana vaping).
Lastly, the lack of qualitative inquiry into specific content that can aid in understanding the most important protective factors among Black girls was unavailable for the current study. Qualitative methods allow researchers to tell stories regarding the lived experiences of Black adolescent girls. A qualitative methodology allows researchers to understand what specific topics and concepts are most important to be incorporated in racial- and gender-specific prevention work for Black adolescent girls in urban neighborhoods. This study provides preliminary evidence to explore how specific protective factors such as empowerment (including policy control and leadership competency), ethnic identity, and social support can reduce substance use and sexual risk behaviors among Black girls.
Conclusion
Due to the disproportionate rates of HIV/AIDS, sexually transmitted infections, and drug use that has impacted young Black girls, it is imperative that researchers apply innovative methods in the near future. Substance-abuse and HIV/STI prevention research tends to overlook such critical intersections and diminish the protective effects that familial supports and cultural values may have on Black adolescent girls. In addition, valuing the positive influences and strengths in Black families is critical, as society often fails to celebrate Black families and instead views them through a deficit lens. Findings from this study call attention to the need to apply a family- and community-based approach to prevention work for young girls of color. Understanding the mechanisms that have protected urban adolescent Black girls who are not engaging in risky behaviors is crucial. Implications from this study include informing preventive efforts by creating interventions and programming that seeks to empower Black adolescent girls through a culturally specific, empowerment lens. In addition, this study can promote cultural factors such as ethnic identity that can be used in STI, HIV, and drug-use prevention programs.
This study aimed to highlight the importance of prevention research to move away from a deficit perspective when discussing outcomes pertaining to historically marginalized groups. Researchers should celebrate the positive influences and strengths of families whose racial and ethnic backgrounds can contribute to the change of narrative. Findings intend to celebrate the positive attributes of belonging to an ethnic group and instilling pride in such groups rather than encouraging youth to view their identities as flawed and undervalued. This study provides a unique perspective to the combination of protective factors such as empowerment, social support, and ethnic identity. Moving away from the deficit lens, it is important for researchers to understand why Black adolescent girls who live in urban neighborhoods remain abstinent or do not engage in risky behaviors. As prevention researchers, clinicians, and family scientists, we have the obligation to strengthen the family unit and encourage the use of tools and strategies that are already present in families. Such an approach allows researchers to effectively learn from Black adolescent girls and their families, as they are the experts in their lived realities. Using this approach can allow clinicians and researchers to work with Black adolescent girls to create effective and sustainable prevention programming.
References
Ahmed, W., Minnaert, A., van der Werf, G., & Kuyper, H. (2010). Perceived social support and early adolescents’ achievement: The mediational roles of motivational beliefs and emotions. Journal of Youth and Adolescence, 39(1), 36.
Akers, A. Y., Lynch, C. P., Gold, M. A., Chang, J. C. C., Doswell, W., Wiesenfeld, H. C.,…, Bost, J. (2009). Exploring the relationship among weight, race, and sexual behaviors among girls. Pediatrics, 124(5), 913-920.
Arbuckle, J. L. (2014). Amos (Version 23.0) (Computer Program). Chicago: IBM SPSS.
Anderson, J. E., & Mueller, T. E. (2008). Trends in sexual risk behavior and unprotected sex among high school students, 1991–2005: The role of substance use. Journal of School Health, 78, 575–580. https://doi.org/10.1111/j.1746-1561.2008.00348.x.
Andrade, L. F., Carroll, K. M., & Petry, N. M. (2013). Marijuana use is associated with risky sexual behaviors in treatment-seeking polysubstance abusers. American Journal of Drug and Alcohol Abuse, 39, 266–271. https://doi.org/10.3109/00952990.2013.803112.
Banerjee, M., Rivas-Drake, D., & Smalls-Glover, C. (2017). Racial–ethnic socialization and achievement: The mediating role of academic engagement. Journal of Black Psychology, 43(5), 451–463.
Beadnell, B., Stielstra, S., Baker, S., Morrison, D. M., Knox, K., Gutierrez, L., et al. (2003). Ethnic identity and sexual risk-taking among African-American women enrolled in an HIV/STD prevention intervention. Psychology, Health and Medicine, 8, 187–198. https://doi.org/10.1080/1354850031000087564.
Beeker, C., Guenther-Grey, C., & Raj, A. (1998). Community empowerment paradigm drift and the primary prevention of HIV/AIDS. Social Science and Medicine, 46, 831–842. https://doi.org/10.1016/S0277-9536(97)00208-6.
Belgrave, F. Z., Brome, D. R., & Hampton, C. (2000). The contribution of Africentric values and racial identity to the prediction of drug knowledge, attitudes, and use among African American youth. Journal of Black Psychology, 26, 386–401. https://doi.org/10.1177/0095798400026004003.
Belgrave, F. Z., Townsend, T. G., Cherry, V. R., & Cunningham, D. M. (1997). The influence of an Africentric worldview and demographic variables on drug knowledge, attitudes, and use among African American youth. Journal of Community Psychology, 25(5), 421–433.
Bollen & Stine. (1992). Structural equation models with latent variables. New York: Wiley.
Carter, R., Caldwell, C. H., Matusko, N., & Jackson, J. S. (2015). Heterosexual romantic involvement and depressive symptoms in black adolescent girls: Effects of menarche and perceived social support. Journal of Youth and Adolescence, 44(4), 940–951.
Cauce, A., Felner, R. D., & Primavera, J. (1982). Social support in high risk adolescents structural components and adaptive impact. American Journal of Community Psychology, 10, 417–428. https://doi.org/10.1007/BF00893980.
Cauce, A. M., Mason, C., Gonzales, N., Hiraga, Y., & Liu, G. (1994). Social support during adolescence: Methodological and theoretical considerations. In: Social networks and social support in childhood and adolescence (pp. 89–108). https://doi.org/10.1515/9783110866377.89.
Centers for Disease Control and Prevention. (2016). STDs in racial and ethnic minorities.https://www.cdc.gov/std/stats16/minorities.htm.
Christens, B. D., Peterson, N. A., & Speer, P. W. (2011). Community participation and psychological empowerment: Testing reciprocal causality using a cross-lagged panel design and latent constructs. Health Education and Behavior, 38, 339–347. https://doi.org/10.1177/1090198110372880.
Christens, B. D., & Peterson, N. A. (2012). The role of empowerment in youth development: A study of sociopolitical control as mediator of ecological systems’ influence on developmental outcomes. Journal of Youth and Adolescence, 41, 623–635. https://doi.org/10.1007/s10964-011-9724-9.
Christens, B. D., Collura, J. J., & Tahir, F. (2013). Critical hopefulness: A person-centered analysis of the intersection of cognitive and emotional empowerment. American Journal of Community Psychology, 52, 170–184.
Chung, T., Ye, F., Hipwell, A. E., Stepp, S. D., Miller, E., Borrero, S., et al. (2017). Alcohol and marijuana use in pathways of risk for sexually transmitted infection in white and black adolescent females. Substance Abuse, 38(1), 77–81.
Clark, E. M., Williams, R. M., Park, C. L., Schulz, E., Williams, B. R., & Holt, C. L. (2018). Personality, social capital, and depressive symptomatology among African Americans. Journal of Black Psychology, 44(5), 422–449.
Clark, E. M., Williams, R. M., Park, C. L., Schulz, E., Williams, B. R., & Knott, C. L. (2019). Explaining the relationship between personality and health in a national sample of African Americans: The mediating role of social support. Journal of Black Psychology, 45(5), 339–375.
Collins, C. C., & DeRigne, L. (2017). Cultural models of popularity, stress, social support, and violence among African American US teens living in a high-poverty community. Journal of Human Behavior in the Social Environment, 27, 215–231. https://doi.org/10.1080/10911359.2016.1270871.
Collins, M. L., Baiardi, J. M., Tate, N. H., & Rouen, P. A. (2015). Exploration of social, environmental, and familial influences on the sexual health practices of urban African American adolescents. Western Journal of Nursing Research, 37, 1441–1457. https://doi.org/10.1177/0193945914539794.
Cooper, S. M., White Johnson, R., Brown Griffin, C., Metzger, I., Avery, M., & Eaddy, H.,..., Guthrie, B. (2015). Community involvement and reduced risk behavior engagement among African American adolescents: The mediating role of empowerment beliefs. Journal of Black Psychology, 41(5), 415–437.
Corneille, M. A., & Belgrave, F. Z. (2007). Ethnic identity, neighborhood risk, and adolescent drug and sex attitudes and refusal efficacy: The urban African American girls’ experience. Journal of Drug Education, 37, 177–190. https://doi.org/10.2190/UJ17-34J7-U306-2822.
Cross, C. J., Taylor, R. J., & Chatters, L. M. (2018). Family social support networks of African American and Black Caribbean adolescents. Journal of Child and Family Studies, 27(9), 2757–2771.
Danielson, C. K., Walsh, K., McCauley, J., Ruggiero, K. J., Brown, J. L., Sales, J. M., Rose, E., Wingood, G. M., & DiClemente, R. J. (2014). HIV-related sexual risk behavior among African American adolescent girls. Journal of Women’s Health (15409996), 23(5), 413–419. https://doi-org.ezproxy.montclair.edu/10.1089/jwh.2013.4599.
DiClemente, R. J., & Wingood, G. M. (1995). A randomized controlled trial of an HIV sexual risk-reduction intervention for young African-American women. Journal of the American Medical Association, 274, 1271–1276. https://doi.org/10.1001/jama.1995.03530160023028.
Drolet, M., & Arcand, I. (2013). Positive development, sense of belonging, and support of peers among early adolescents: Perspectives of different actors. International Education Studies, 6(4), 29–38. https://doi.org/10.5539/ies.v6n4p29.
Enders, C. K. (2006). Analyzing structural equation models with missing data. Structural equation modeling: A second course, 2, 493–519.
Espinosa-Hernández, G., & Lefkowitz, E. S. (2009). Sexual behaviors and attitudes and ethnic identity during college. Journal of Sex Research, 46(5), 471–482.
Field, A. (2013). Discovering statistics using IBM SPSS statistics. Sage Publications.
Fisher, S., Zapolski, T. C., Sheehan, C., & Barnes-Najor, J. (2017). Pathway of protection: Ethnic identity, self-esteem, and substance use among multiracial youth. Addictive Behaviors, 72, 27–32. https://doi.org/10.1016/j.addbeh.2017.03.003.
Floyd, L. J., & Brown, Q. (2013). Attitudes towards and sexual partnerships with drug dealers among young adult African American females in socially disorganized communities. Journal of Drug Issues, 2, 154–165. https://doi.org/10.1177/0022042612467009.
Garcia-Reid, P. (2007). Examining social capital as a mechanism for improving school engagement among low income Hispanic girls. Youth and Society, 39, 164–181. https://doi.org/10.1177/0044118X07303263.
Garcia-Reid, P., Lardier, D. T., Jr., Reid, R. J., & Opara, I., (2018). Understanding the influence of sexual risk taking, ethnic identity, and family and peer support on school importance among Hispanic adolescents. Education and Urban Society. https://doi.org/10.1177/0013124518787827.
Golden, A. R., Griffin, C. B., Metzger, I. W., & Cooper, S. M. (2018). School racial climate and academic outcomes in African American adolescents: The protective role of peers. Journal of Black Psychology, 44, 47–73.
Guthrie, B. J., Cooper, S. M., Brown, C., & Metzger, I. (2012). Degrees of difference among minority female juvenile offenders’ psychological functioning, risk behavior engagement, and health status: A latent profile investigation. The Journal of Health Care for the Poor and Underserved, 23, 204–225.
Guzmán, B. L., & Stritto, M. E. D. (2012). The role of socio-psychological determinants in the sexual behaviors of Latina early adolescents. Sex Roles, 66(11–12), 776–789.
Hancock, G. R., & Liu, M. (2012). Bootstrapping standard errors and data-model fit statistics in structural equation modeling. In R. H. Hoyle (Ed.), Handbook of structural equation modeling (pp. 296–306). The Guilford Press.
Harwell, M., & LeBeau, B. (2010). Student eligibility for a free lunch as an SES measure in education research. Educational Researcher, 39(2), 120–131.
Hope, M. O., Lee, D. B., Hsieh, H. F., Hurd, N. M., Sparks, H. L., & Zimmerman, M. A. (2019). Violence exposure and sexual risk behaviors for African American adolescent girls: The protective role of natural mentorship and organizational religious involvement. American Journal of Community Psychology, 64(1–2), 241–254.
Holden, D. J., Evans, W. D., Hinnant, L. W., & Messeri, P. (2005). Modeling psychological empowerment among youth involved in local tobacco control efforts. Health Education & Behavior, 32(2), 264–278.
Hosen, R., & Solovey-Hosen, D. (2003). The instructional value of fostering social capital in the classroom. Journal of Instructional Psychology, 30(1), 84.
Hoyle, R. H. (1995). Structural equation modeling: Concepts, issues, and applications. Thousand Oaks, CA: Sage.
Hughey, J., Peterson, N. A., Lowe, J. B., & Oprescu, F. (2008). Empowerment and sense of community: Clarifying their relationship in community organizations. Health Education & Behavior, 35(5), 651–663.
Hutchinson, M. K., & Cederbaum, J. A. (2011). Talking to daddy’s little girl about sex: Daughters’ reports of sexual communication and support from fathers. Journal of Family Issues, 32, 550–572. https://doi.org/10.1177/0192513X10384222.
Hutchinson, M. K., Kahwa, E., Waldron, N., Hepburn Brown, C., Hamilton, P. I., Hewitt, H. H., …, Sweet Jemmott, L. (2012). Jamaican mothers’ influences of adolescent girls’ sexual beliefs and behaviors. Journal of Nursing Scholarship, 44, 27–35. https://doi.org/10.1111/j.1547-5069.2011.01431.x.
Imai, K., Keele, L., & Tingley, D. (2010). A general approach to causal mediation analysis. Psychological Methods, 15(4), 309.
Jackson, J. M., Seth, P., DiClemente, R. J., & Lin, A. (2015). Association of depressive symptoms and substance use with risky sexual behavior and sexually transmitted infections among African American female adolescents seeking sexual health care. American Journal of Public Health, 105, 2137–2142. https://doi.org/10.2105/AJPH.2014.302493.
Javier, S. J., Abrams, J. A., Moore, M. P., & Belgrave, F. Z. (2018). Condom use efficacy and sexual communication skills among African American college women. Health Promotion Practice, 19(2), 287–294.
Kann, L., Kinchen, S., Shanklin, S. L., Flint, K. H., Hawkins, J., Harris, W. A.,…,Zaza, S. (2014). Youth risk behavior surveillance—United States, 2013. Morbidity and Mortality Weekly Report, 63, 1–168. https://www.cdc.gov/mmwr/preview/mmwrhtml/ss6304a1.htm.
Kann, L., McManus, T., Harris, W. A., Shanklin, S. L., Flint, K. H., Queen, B., et al. (2018). Youth risk behavior surveillance—United States, 2017. MMWR Surveillance Summaries, 67(8), 1.
Kazak, A. E., & Meadows, A. T. (2013). Families of young adolescents who have survived cancer: Social–emotional adjustment, adaptability, and social support. Family Issues in Pediatric Psychology (pp. 37–54). New York: Routledge.
Kazarian, S. S., & Boyadjian, M. D. (2008). Validation of the multigroup ethnic identity measure among ethnic Armenian adolescents in Lebanon. Identity: An International Journal of Theory and Research, 8(4), 335–347.
Kline, R. B. (2015). Principles and practice of structural equation modeling. Guilford publications.
Kogan, S. M., Brody, G. H., Gibbons, F. X., Murry, V. M., Cutrona, C. E., Simons, R., …, DiClemente, R. (2008). The influence of role status on risky sexual behavior among African Americans during the transition to adulthood. Journal of Black Psychology, 34(3), 399–420. https://doi.org/10.1177/0095798408320716.
Lamb, S., & Peterson, Z. D. (2012). Adolescent girls’ sexual empowerment: Two feminists explore the concept. Sex Roles, 66, 703–712.
Lardier, D. T., Jr. (2019). Substance use among urban youth of color: Exploring the role of community-based predictors, ethnic identity, and intrapersonal psychological empowerment. Cultural Diversity and Ethnic Minority Psychology, 25(1), 91.
Lardier, D. T., Garcia-Reid, P., & Reid, R. J. (2018a). The interacting effects of psychological empowerment and ethnic identity on indicators of well-being among youth of color. Journal of Community Psychology, 46, 489–501. https://doi.org/10.1002/jcop.21953.
Lardier, D. T., Jr., Reid, R. J., & Garcia-Reid, P. (2018b). Validation of an abbreviated Sociopolitical Control Scale for Youth among a sample of underresourced urban youth of color. Journal of Community Psychology, 46(8), 996–1009.
Lardier, D. T., Garcia-Reid, P., & Reid, R. J. (2019a). The examination of cognitive empowerment dimensions on intrapersonal psychological empowerment, psychological sense of community, and ethnic identity among urban youth of color. The Urban Review, 51, 1–21.
Lardier, D. T., Opara, I., Bergeson, C., Herrera, A., Garcia-Reid, P., & Reid, R. J. (2019b). A study of psychological sense of community as a mediator between supportive social systems, school belongingness, and outcome behaviors among urban high school students of color. Journal of Community Psychology, 47(5), 1131–1150.
Lardier, D. T., Opara, I., & Garcia-Reid, P., & Reid, R. J. (2020). The cognitive empowerment scale: Multigroup confirmatory factor analysis among youth of color. Journal of Community Psychology. https://doi.org/10.1007/s10560-019-00647-2.
Leventhal, T., & Brooks-Gunn, J. (2000). The neighborhoods they live in: The effects of neighborhood residence on child and adolescent outcomes. Psychological Bulletin, 126, 309–337. https://doi.org/10.1037/0033-2909.126.2.309.
Lindsey, M. A., Joe, S., & Nebbitt, V. (2010). Family matters: The role of mental health stigma and social support on depressive symptoms and subsequent help seeking among African American boys. Journal of Black Psychology, 36(4), 458–482.
Miguel, M. C., Ornelas, J. H., & Maroco, J. P. (2015). Defining psychological empowerment construct: Analysis of three empowerment scales. Journal of Community Psychology, 43(7), 900–919.
Neblett, E. W., Jr., Rivas-Drake, D., & Umaña-Taylor, A. J. (2012). The promise of racial and ethnic protective factors in promoting ethnic minority youth development. Child Development Perspectives, 6(3), 295–303.
Nevitt, J., & Hancock, G. R. (2001). Performance of bootstrapping approaches to model test statistics and parameter standard error estimation in structural equation modeling. Structural Equation Modeling: A Multidisciplinary Journal, 8, 353–377. https://doi.org/10.1207/S15328007SEM0803_2.
Opara, I. (2018). Examining African American parent–daughter HIV risk communication using a Black feminist-ecological lens: Implications for intervention. Journal of Black Studies, 49, 134–151. https://doi.org/10.1177/0021934717741900.
Opara, I., Lardier, D. T., Herrera, A., Garcia-Reid, P., & Reid, R. J. (2019a). Increasing viral hepatitis knowledge among urban ethnic minority youth: Findings from a community based prevention intervention. Journal of Community Health, 45(2), 1–9.
Opara, I., Lardier, D. T., Jr., Reid, R. J., & Garcia-Reid, P. (2019b). “It all starts with the parents”: A qualitative study on protective factors for drug-use prevention among Black and Hispanic girls. Affilia Journal of Women and Social Work. https://doi.org/10.1177/0886109918822543.
Opara, I., Rivera Rodas, E. I., Lardier, D. T., Jr., Garcia-Reid, P., & Reid, R. J. (2020). Validation of the abbreviated socio-political control scale for youth (SPCS-Y) among urban girls of color. Child and Adolescent Social Work Journal. https://doi.org/10.1007/s10560-019-00624-9.
Perry, M., Williams, R. L., Wallerstein, N., & Waitzkin, H. (2008). Social capital and health care experiences among low-income individuals. American Journal of Public Health, 98(2), 330–336.
Peterson, N. A., & Reid, R. J. (2003). Paths to psychological empowerment in an urban community: Sense of community and citizen participation in substance abuse prevention activities. Journal of Community Psychology, 31, 25–38. https://doi.org/10.1002/jcop.10034.
Peterson, N. A., Lowe, J. B., Hughey, J., Reid, R. J., Zimmerman, M. A., & Speer, P. W. (2006). Measuring the intrapersonal component of psychological empowerment: Confirmatory factor analysis of the sociopolitical control scale. American Journal of Community Psychology, 38, 287–297. https://doi.org/10.1007/s10464-006-9070-3.
Peterson, C. H., Buser, T. J., & Westburg, N. G. (2010). Effects of familial attachment, social support, involvement, and self-esteem on youth substance use and sexual risk taking. Family Journal, 18, 369–376. https://doi.org/10.1177/1066480710380546.
Peterson, N. A., Peterson, C. H., Agre, L., Christens, B. D., & Morton, C. M. (2011). Measuring youth empowerment: Validation of a sociopolitical control scale for youth in an urban community context. Journal of Community Psychology, 39, 592–605. https://doi.org/10.1002/jcop.20456.
Phillips, G., II, Turner, B., Salamanca, P., Birkett, M., Hatzenbuehler, M. L., Newcomb, M., ..., Mustanski, B. (2017). Victimization as a mediator of alcohol use disparities between sexual minority subgroups and sexual majority youth using the 2015 National Youth Risk Behavior Survey. Drug and Alcohol Dependence, 178, 355–362.
Phinney, J. S. (1989). Stages of ethnic identity development in minority group adolescents. The Journal of Early Adolescence, 9, 34–49. https://doi.org/10.1177/0272431689091004.
Phinney, J. S., Horenczyk, G., Liebkind, K., & Vedder, P. (2001). Ethnic identity, immigration, and well-being: An interactional perspective. Journal of Social Issues, 57, 493–510. https://doi.org/10.1111/0022-4537.00225.
Phinney, J. S., & Ong, A. D. (2007). Conceptualization and measurement of ethnic identity: Current status and future directions. Journal of Counseling Psychology, 54, 271–281. https://doi.org/10.1037/0022-0167.54.3.271.
Pflieger, J. C., Cook, E. C., Niccolai, L. M., & Connell, C. M. (2013). Racial/ethnic differences in patterns of sexual risk behavior and rates of sexually transmitted infections among female young adults. American Journal of Public Health, 103(5), 903–909.
Podsakoff, P. M., MacKenzie, S. B., & Podsakoff, N. P. (2012). Sources of method bias in social science research and recommendations on how to control it. Annual Review of Psychology, 63, 539–569.
Ponterotto, J. G., Gretchen, D., Utsey, S. O., Stracuzzi, T., & Saya, R., Jr. (2003). The multigroup ethnic identity measure (MEIM): Psychometric review and further validity testing. Educational and Psychological Measurement, 63(3), 502–515.
Rappaport, J. (1987). Terms of empowerment/exemplars of prevention: Toward a theory for community psychology. American Journal of Community Psychology, 15, 121–148. https://doi.org/10.1007/BF00919275.
Reid, R. J., & Garcia-Reid, P. (2013). Exploring the Strategic Prevention Framework (SPF) and its application to a comprehensive substance abuse and HIV/AIDS prevention initiative: evidence from Project COPE. The International Journal of Interdisciplinary Social and Community Studies, 7(4), 13–28.
Reid, R. J., Hughey, J., & Andrew Peterson, N. (2003). Generalizing the alcohol outlet–assaultive violence link: Evidence from a US midwestern city. Substance Use & Misuse, 38(14), 1971–1982.
Reid, R. J., Yu, D., & Garcia-Reid, P. (2014). Preventing substance abuse and HIV/AIDS among urban minority youth: Evidence from a university-community partnership. Journal of Addiction Research and Therapy, 5(3), 1–5. https://doi.org/10.4172/2155-6105.1000186.
Reininger, B. M., Pérez, A., Aguirre Flores, M. I., Chen, Z., & Rahbar, M. H. (2012). Perceptions of social support, empowerment and youth risk behaviors. Journal of Primary Prevention, 33, 33–46. https://doi.org/10.1007/s10935-012-0260-5.
Respress, B. N., Amutah-Onukagha, N., & Opara, I. (2018). The effects of school-based discrimination on adolescents of color sexual health outcomes: A social determinants approach. Social Work in Public Health, 33, 134–156. https://doi.org/10.1080/19371918.2017.1378953.
Rivas-Drake, D., Syed, M., Umaña-Taylor, A., Markstrom, C., French, S., Schwartz, S. J.,…, Ethnic and Racial Identity in the 21st Century Study Group. (2014). Feeling good, happy, and proud: A meta-analysis of positive ethnic–racial affect and adjustment. Child Development, 85, 77–102. https://doi.org/10.1111/cdev.12175.
Roberts, R. E., Phinney, J. S., Masse, L. C., Chen, Y. R., Roberts, C. R., & Romero, A. (1999). The structure of ethnic identity of young adolescents from diverse ethnocultural groups. Journal of Early Adolescence, 19, 301–322. https://doi.org/10.1177/0272431699019003001.
Rush, B., & Urbanoski, K. (2019). Seven core principles of substance use treatment system design to aid in identifying strengths, gaps, and required enhancements. Journal Studies on Alcohol and Drugs, 18, 9–21.
Sanchez, D., Hamilton, E. R., Gilbert, D. J., & Vandewater, E. A. (2018). Examining Africentric cultural values, ethnic identity, and substance use abstinence in low-income, early adolescent, African American girls. Journal of Black Psychology, 44, 74–100. https://doi.org/10.1177/0095798417746265.
Schinke, S., Di Noia, J., Schwinn, T., & Cole, K. (2006). Drug abuse risk and protective factors among black urban adolescent girls: A group-randomized trial of computer-delivered mother-daughter intervention. Psychology of Addictive Behaviors, 20(4), 496.
Schinke, S. P., Fang, L., & Cole, K. C. (2009). Preventing substance use among adolescent girls: 1-Year outcomes of a computerized, mother–daughter program. Addictive Behaviors, 34, 1060–1064. https://doi.org/10.1016/j.addbeh.2009.06.007.
Shehadeh, N., Rubens, M., Attonito, J., & Jennings, T. (2018). Social support and its impact on ethnic identity and HIV risk among migrant workers. Journal of Racial and Ethnic Health Disparities, 5, 96–103. https://doi.org/10.1007/s40615-017-0347-z.
Swartzendruber, A., Sales, J. M., Brown, J. L., DiClemente, R. J., & Rose, E. S. (2016). Comparison of substance use typologies as predictors of sexual risk outcomes in African American adolescent females. Archives of Sexual Behavior, 45, 63–72.
Thompson, B. (2000). Ten commandments of structural equation modeling. In US Dept of Education, Office of Special Education Programs (OSEP) Project Directors' Conference, 1998, Washington, DC, US; A previous version of this chapter was presented at the aforementioned conference and at the same annual conference held in 1999. American Psychological Association.
Voisin, D. R., Jenkins, E. J., & Takahashi, L. (2011). Toward a conceptual model linking community violence exposure to HIV-related risk behaviors among adolescents: Directions for research. Journal of Adolescent Health, 49, 230–236.
Wallace, S. A., Townsend, T. G., Glasgow, Y. M., & Ojie, M. J. (2011). Gold diggers, video vixens, and jezebels: Stereotype images and substance use among urban African American girls. Journal of Women’s Health, 20, 1315–1324. https://doi.org/10.1089/jwh.2010.2223.
Way, N. (2013). Boys’ friendships during adolescence: Intimacy, desire, and loss. Journal of Research on Adolescence, 23, 201–213. https://doi.org/10.1111/jora.12047.
West, S. G., Taylor, A. B., & Wei, W. (2012). Model fit and model selection in structural equation modeling. In R. H. Hoyle (Ed.), Handbook of structural equation modeling (pp. 209–231). New York: Guilford Press.
Zimmerman, M. A., & Zahniser, J. H. (1991). Refinements of sphere-specific measures of perceived control: Development of a sociopolitical control scale. Journal of Community Psychology, 19, 189–204. https://doi.org/10.1002/1520-662.
Zimmerman, M. A. (1995). Psychological empowerment: Issues and illustrations. American Journal of Community Psychology, 23, 581–599. https://doi.org/10.1007/BF02506983.
Zimmerman, M. A. (2000). Empowerment theory. In J. Rappaport & E. Seidman (Eds), Handbook of community psychology (pp 43–63). Boston: Springer. https://doi.org/10.1007/978-1-4615-4193-6
Acknowledgements
This study was supported by the Drug Free Communities Grant (DFC) Initiative (Grant #SP022-19-01), funded through the Substance Abuse and Mental Health Services Administration (SAMHSA). The first author was supported with funding from a National Institute on Drug Abuse training grant (5T32 DA07233) and received partial funding support from a National Institute of Mental Health education grant (R25-MH087217). Points of view, opinions, and conclusions in this paper do not necessarily represent the official position of the U.S. Government.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
The authors of this manuscript have complied with APA ethical principles in their treatment of individuals participating in the research, program, or policy described in the manuscript. The research has been approved by Montclair State University.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Opara, I., Rodas, E. .R., Garcia-Reid, P. et al. Ethnic Identity, Empowerment, Social Support and Sexual Risk Behaviors Among Black Adolescent Girls: Examining Drug Use as a Mediator. Child Adolesc Soc Work J 39, 71–86 (2022). https://doi.org/10.1007/s10560-020-00706-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10560-020-00706-z