
Abstract
The homicide of a loved one is a devastating event for families. Adult and youth survivors struggle with posttraumatic stress, complicated grief, isolation, and stigma. Existing programs serving survivors of homicide victims offer needed services, but a comprehensive program is lacking. Based on an analysis of existing programs in the United States, a literature review, and the authors’ practice experience, this paper presents a comprehensive, conceptual practice model for supporting survivors of homicide victims. The program model consists of the following components: Counseling/Therapeutic Services; Case Management Services; Advocacy Services; Education/Training; Community of Survivors; and a Website/Hotline. Implications for social work practice and directions for future research are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Homicide continues to be a problem that plagues the United States. The U.S. leads the industrialized world in murders per capita. In 2012, the U.S. had a per capita homicide rate of 4.12 per 100,000 inhabitances (Uniform Crime Report). Additionally, there were 14,827 homicides in the same year (Uniform crime report 2012). Those who experience the homicide of a loved one have come to be known as survivors (Hertz et al. 2005). This name is preferable to victims because it reflects the true state of individuals and families left to carry on after such a traumatic life event. Survivors have no choice but to learn how to carry on after the murder of a loved one. The number of family members surviving a homicide is significant, although the estimates in the literature vary greatly. Ahmed and Feldman (1999) estimate that there are on average 3 surviving family members; whereas Redmond (1989a) reports a range of 7–10 family members surviving a homicide victim. Additionally, Redmond estimates between 210,000 and 300,000 adult and youth survivors.
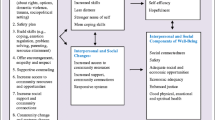
Adult and young survivors of homicide victims cope with a myriad of psychological, social, behavioral, and health-related problems. The impact of exposure to violence and homicide of a loved one on children and youth is well documented. Post-traumatic stress disorder (Fitzpatrick and Boldizar 1993; Kilpatrick and Resnick 1993; Horowitz et al. 1995; Kliewer et al. 1998; Maza and Reynolds 1999; Overstreet and Braun 2000; Clements and Burgess 2002), anxiety and depression (Aisenberg 2001; Fitzpatrick and Boldizar 1993; Horowitz et al. 1995; Maza and Reynolds 1999; Richerts and Martinez 1993) and aggressive behavior (Farrel and Bruce 1997; Kilpatrick et al. 2000) have been strongly correlated to exposure to violence and homicide. Moreover, exposure to violence has been found to put youth at a high risk for future involvement in violence either as a perpetrator or as a victim (Lipsey and Derzon 1998; Resnick et al. 2004). Surviving adult family members have been found to have high rates of post-traumatic stress disorder, anxiety, and depression (Amick-McMullan et al. 1991; Kilpatrick and Resnick 1993; Parkes 1993; Murphy, et al. 1999; Overstreet and Braun 2000; van Denderen et al. 2013), social stigma (Vessier-Batchen and Douglas 2006), and isolation (Vincent 2009).
Over time adult survivors experience the lifelong process of coping with complicated grief (Rando 1993; Spunge 1998; Armour 2002; Vessier-Batchen and Douglas 2006; van Denderen et al. 2013). Complicated grief is the enduring and agonizing process by which as survivor struggles with how to continue life with the horrible reality of the homicide of a loved one (Spunge 1998). It is associated with long-term mental health problems including: major depression, depression, anxiety, and substance abuse (Vigil and Clements 2003; Vessier-Batchen and Douglas 2006). Complicated grief has been found to overlay and coexist in complex ways with PTSD (Armour 2002; van Denderen et al. 2013).
In addition to the well-documented impact on youth and adult survivors, the homicide of a loved one has been found to impact the family as a system. A homicide significantly disrupts family functioning and relationships. Family members experience: compromised parenting, isolation, safety concerns, communication problems, family conflict, safety concerns, and loss of financial resources (Vincent 2009).
Given the severity of the impact of surviving the homicide of a loved one on adult and young family members, this paper explores the following question on the state of knowledge about survivor services programs. What survivor services programs exist in the United States? What services do they provide? What are the primary program components common across survivors services programs? This paper presents a descriptive analysis of existing survivor services programs in the United States that have an online presence and a review of the relevant literature. Additionally, it presents Chicago Survivors as a program case study. Based on the program analysis, the literature on survivors, and our practice experience with Chicago Survivors, we propose a comprehensive, conceptual program model. Finally, we discuss implications for practice with families surviving the murder of a loved one, as well as, offer directions for future research.
Literature Review and Descriptive Analysis of Existing Survivor Services
A comprehensive understanding of programs offering support services to survivors of homicide victims is lacking. We conducted a descriptive analysis of twenty survivors’ services programs throughout the United States with an online presence and reviewed the most relevant literature. In order to identify the survivor programs, we conducted an online search using the terms “Homicide Survivor Programs” and “Services for Survivors of Homicide Victims”. We only included nonprofit organizations and excluded any survivor services affiliated with state or city sponsored criminal justice systems. None of the organizations we reviewed were affiliated with any faith community or religious organization. The rational for only selecting community-based organizations is because they often provide more comprehensive services and were more likely to better inform a comprehensive conceptual model. Table 1 provides a list of the survivor services organizations included in this analysis.
The analysis focused on the types of services offered by the programs and presented the literature that offered support for each. We reviewed each program’s website, noting the programmatic components listed and described. Next, we developed an annotative summary of each program. Finally, we identified common programmatic components and services that are unique to specific organizations. The common program components include: (1) Counseling/Therapeutic Services; (2) Case Management Services; (3) Advocacy Services; (4) Education/Training; (5) Community of Survivors Services; (6) Website/Hotline. The program components identified in the analysis are presented in descending order from most to least common.
Counseling/Therapeutic Services
All twenty programs provide some form of counseling/therapy services. Most programs characterize their services as counseling. They include: immediate crisis counseling, some form of individual, family, or group counseling, including community-based therapeutic groups. Few programs characterized their services as therapeutic with only one program identifying an evidence-based group intervention with youth survivors.
Much of the literature focuses on practice methods and efficacy of counseling/therapeutic services offered to survivors. Crisis intervention (Asaro 2009; Hatton 2003; Horne 2003), individual counseling (Asaro 2009, Armour 2002, Getzel and Masters 1984), family therapy (Armour 2002, Getzel and Masters 1984), group therapy (Asaro 2009; Murphy et al 1996) have all been recommended as effective intervention modalities for adult survivors. For youth survivors, community-based group treatment is recommended (Salloum et al. 2001; Salloum and Vincent 1999; Freeman et al. 1996). However, for youth sibling survivors who may be experiencing posttraumatic stress disorder and who cannot tolerate group interaction, individual therapeutic services may be most effective (Freeman et al. 1996).
Case Management Services
Ninety-five percent (n = 19) of programs report providing case management services with survivors of homicide victims. These services consist of the provision and/or coordination with other programs to meet concrete needs. The most common of service provided is assistance with crime victim’s compensation. Other services cited, although less common, include: assistance with funeral arrangements; transportation and lodging costs, emergency financial support, crime scene clean up, and emergency food.
Few studies propose case management services as important components to a survivor program. Studies recommend that practitioners focus on “providing both concrete and psychological services in a flexible and proactive manner”. (Armour 2002, p 122) and they recommend interventions that focus on practical, concrete needs of survivors (Vincent 2009; Hatton 2003; Horne 2003; Getzel and Masters 1984).
Advocacy Services
A third program component commonly offered by programs working with survivors of homicide victims is advocacy. Ninety percent (n = 18) of programs report providing some form of advocacy, with the most common being supporting the surviving family through the criminal justice system. Advocacy with the criminal courts include: court accompaniment, case coordination through the investigation, prosecution, post-sentencing, and post-conviction support. Central to this form of advocacy is ensuring that families are informed about all aspects of the criminal justice process. Staff members serve as a liaison between the criminal investigators, state’s attorneys, and parole boards. Fewer programs 15 \ (n = 3) characterize their advocacy work as policy-oriented. Programs emphasize the pursuit to establish victim’s rights and the reform of the criminal justice system to be more supportive of survivors. Advocacy services are recommended in the literature, but primarily with the criminal justice system (Masters et al. 1988; Armour 2002; Gekoski et al. 2013).
Education/Training Services
Although it is not a direct service component, education/training services were provided by 40 % (n = 4) of the programs. Programs provide education/training to a range of community systems that interact with survivors. Programs report providing training with survivors, criminal justice officials, mental health practitioners, social workers, attorneys, community services workers, healthcare professionals, educators, clergy, and journalists. Education/training is viewed as a combination of prevention and intervention, where practitioners are taught to work more effectively with survivors and are informed about approaches to preventing violence. In the only study that speaks to training of systems that interact with survivors, Armour (2002) offers a policy recommendation where “…social institutions that interact with covictims need to be made aware of the needs of this population and develop policies and protocols for responding more sensitively” (p. 122).
Community of Survivors Services
The development and facilitation of a community of survivors is an important component to supporting survivors of homicide victims (Hertz et al. 2005). The formation of a community of survivors involves bringing together surviving families in a safe, trusted space where there are no expectations for how they should feel or be. It is an opportunity for adults and young family members to meet other survivors to form an informal supportive network. Survivors attend community events only when they feel they are ready.
Although the development of a survivor network is identified in the literature as an essential programmatic component, our analysis found that only 35 % (n = 7) of the programs report facilitating one. Although the term “community of survivors” is not found in the literature, other similarly recommended services include: “self help” groups (Hertz et al. 2005; Hatton 2003; Redmond 1989b; Rynearson 1994; Spunge 1998), and peer support groups (Asaro 2009). Additionally, Community of Survivors Services may be uniquely effective for decreasing the isolation and stigma experienced by survivors of homicide victims (Hatton 2003; Redmond 1989a; Rynearson 1994; Spunge 1998). Although not naming it as a survivor network per se, Sharpe, (2008) cited the importance of informal support networks in helping African American survivors cope effectively.
Survivor Hotline/Website
Hotlines and/or websites provide a central portal to inform survivors about the services available to them and how to access those services. All twenty of the survivor services programs have functioning websites. However, the service descriptions varied greatly across programs. Some programs provide specific detailed information on the website about the nature of services, times available, and locations. Other programs provide general information about services and a number to call for specific details. However, few of the programs (15 %, n = 3) operate a 24-h crisis hotline. Although it appears that websites and hotlines are important components of a survivor program, it is not recognized in the literature.
This descriptive analysis of survivor services programs in the United States with an online presence provides a perspective about the composition of such organizations that previously was lacking in the literature. Although programs have components in common, there is no evidence from the programs or in the literature about why this particular mix of services is most effective in supporting survivors. Identification of program components could have emerged from an obvious felt need identified by program staff. Perhaps program components could have emerged from practitioners sharing ideas at conferences and other meetings. In the survivor literature, it appears that programmatic recommendations are based primarily on anecdotal evidence. They do not appear to have emerged from empirical studies focusing on the development of evidence-based practices with the exception of adult and youth therapeutic group interventions (Salloum et al. 2001; Salloum and Vincent 1999). Whatever the origins, the commonality of the programmatic components among numerous programs offers some degree of validity as to their appropriateness for supporting survivors.
The research literature appears to validate the importance of most program components. The need for counseling and therapeutic services appears to be the most supported in the literature. A few studies also recommend case management services as an important component of a survivor services program. Studies cite the need for concrete services to augment therapy but without specifying the specific concrete services needed. Additionally, the literature appears to support the need for advocacy services but only within the context of survivor involvement with the criminal justice systems. Although not as common among survivor programs, the community of survivors receives significant support in the literature. Studies identify it as an important intervention that may augment the other services. The research literature does not appear to support the need for education/training and website/hotline services.
Based on our program analysis and literature review, there appears to be no program that implements a comprehensive program model. Programs appear to implement important components, but no program implements all components. Additionally, there appears to be an omission of survivors’ perspectives in the development of these programs. It is unclear if the survivors were consulted either in the development or continued implementation of programs. Finally, the authors acknowledge the limitations of our program analysis. The sample of twenty programs may not be exhaustive given that some programs may not have websites.
One such survivor program is Chicago Survivors. Chicago Citizen’s for Change started the program because of the lack of comprehensive, coordinated services in an urban area of great need. Chicago Survivors provides a case study in the development of our comprehensive, conceptual practice model for survivors of homicide victims.
Chicago Survivors
Chicago Citizens for Change (CCC) is a community-based organization committed to developing a comprehensive coordinated response to support families surviving the homicide of a loved one. In 2010, CCC implemented the Chicago Survivors program. Chicago Survivors provides citywide support and comprehensive referral services and case management to families following the homicide of an individual aged 26 or younger. The program accomplishes this through experienced staff, who respond immediately after a homicide. Staff offer long-term follow-up care and referral services. The program offers support to families for up to 1 year and helps surviving families navigate a complex and over-taxed social service system in Chicago. Chicago Survivor staff advocate on behalf of families with the criminal justice system, school system, media, landlords, employers, immigration system, and many others. Additionally, Chicago Survivors facilitate an active community of survivors where families come together to support one another. Program staff have developed an ongoing collaboration with the Chicago Police Department and the Cook County State’s Attorney. Through this collaboration staff provide periodic training of detectives and attorneys. Training content includes: the psychological and social impact of experiencing the homicide of a loved one, how survivors experience the criminal justice system, and what detectives and state’s attorneys can do to effectively work with survivors to work towards solving homicide cases and obtain convictions. Program staff facilitate an active website and have a plan to implement a comprehensive citywide hotline.
The development of the Chicago Survivor’s program model was informed by a number of sources. First, the model was developed with direct input from survivors. Co-author, Joy McCormack, herself a survivor, is the founder of Chicago Citizens for Change (CCC). In 2012, CCC and a local university facilitated a symposium focusing on the needs of survivors of homicide victims. Chicago Survivors staff invited surviving families and community practitioners to engage in a creative dialogue about developing comprehensive services for survivors. Additionally, Chicago Survivors’ staff continue to engage a community of survivors to inform program services. Secondly, the program model has been informed by existing programs throughout the United States. Chicago Survivors has consulted with staff of other program and conducted online research resulting in the above analysis. Finally, the program has been informed by the research literature. Survivor studies validate the inclusion of most of the Chicago Survivor program components.
This systematic research into the needs of survivors of homicide victims including an analysis of existing programs, the research literature, and a survivor program case study informed the development of the conceptual program model presented here.
Comprehensive Conceptual Program Model for Survivors of Homicide Victims
The authors propose a comprehensive conceptual services model for survivors of the homicide of a loved one. The proposed program model includes the following components: (1) Crisis Response, (2) Long-Term Family Support, (3) Community of Survivors, (4) Website/Hotline, and (5) Training and Education. Chart 1 summarizes the model.

A comprehensive program model for supporting families surviving a homicide victim
Crisis Response
A crisis response means an immediate connection with the family as soon after the homicide as possible. This phase of services, lasting 24–48 h, requires a close collaboration with law enforcement. Police detectives responding to a homicide contact the emergency hotline where a program Crisis Responder is dispatched to accompany the detective to meet the family at a location determined by law enforcement. At this point, the Crisis Responder may assist the homicide detective with death notification. In support of the family, the Crisis Responder provides: a rapid crisis assessment of need, immediate crisis counseling, accompaniment to hospitals or the morgue, assistance with funeral arrangements, and referral to crisis services such as emergency childcare and crime scene clean up as needed. At the end of the Crisis response phase, the Crisis responder conducts a supportive transfer to a Family Support Specialist to provide long-term support. The transfer at this point in support is crucial so as to not retraumatize the family. We propose a face-to-face meeting with the family, Crisis Responder, and Family Support Specialist.
Long-Term Family Support
The second phase of services offered to families surviving the homicide of a loved one involves providing 1 year of support. The Family Support Specialist first conducts a needs assessment. From the assessment, the Family Support Specialist provides: supportive counseling, advocacy, and case management services to coordinate the comprehensive services needed by the family. The Family Support Specialist will link the family with a network of supportive services including: legal, trauma/grief therapeutic, crime victim’s compensation, healthcare, housing, employment, relocation, and other services as needed. As evident from the experience of Chicago Survivors and other programs, advocacy and support through the entire criminal justice process is crucial. Family Support Specialists may mediate on behalf of the family with homicide detectives during the criminal investigation, accompany the family to the numerous court dates during the trial, and support the family through the victim impact statement process.
Community of Survivors
When a family is emotionally and psychologically ready, program staff will recommend that they connect with a Community of Survivors. Chicago Survivors facilitates events that bring surviving families together during informal gatherings to develop mutual support. Families attend events including: pot-luck dinners, memorial services, flyer distributions after a recent homicide, and vigils. The pot-luck gatherings are meant to be a safe space where families can attend with no expectations to be or feel a certain way. Families tell their stories and make connections with others in a supportive, caring environment.
Website/Hotline
In the aftermath of the homicide of a loved one, surviving families isolate themselves as a way of coping (Vincent 2009). They find it difficult to drive, take public transportation, and access needed services. Given this isolation, a Website/Hotline is a crucial program component in assisting families to begin to access support. Websites are common components among survivor services programs. However, our analysis shows a lower prevalence of hotlines. Given that families may not have ready access to the internet, a hotline can bridge that gap. In addition to linking families to support services, a hotline can be used by law enforcement to connect with program staff providing immediate crisis services, as mentioned above.
Training and Education
A final component to our conceptual program model for survivors of homicide victims is Training and Education of community institutions that come in contact with surviving families. Education and Training is focused on sensitizing individuals to the experience of survivors in order to effect change in institutions that serve survivors. Institutions identified as needing training include: law enforcement, criminal justice personnel, emergency room healthcare staff, county morgue staff, school personnel, and mental health practitioners. A larger goal of Training and Education is to effect change in these institutions in order that they develop uniform protocols for supportive interaction with surviving families and to reduce re-traumatization.
Implications for Practice
The needs of survivors of homicide victims are many and significant. Posttraumatic Stress Disorder, protracted complicated grief, secondary victimization through the court system, stigma, and social isolation make surviving the homicide of a loved one a devastating life event. A programmatic response to such an event requires a comprehensive model of support for survivors. Survivors appear to need: (1) crisis/early intervention, (2) long-term support, (3) advocacy on their behalf, (4) case management to connect with other resources, (5) to be linked with a community of survivors, and (6) access to a hotline/website to assist them in connecting with services. This paper presents such a model. The program model has a number of implications for practitioners. First, early crisis intervention services are necessary. Early intervention can ameliorate the impact of posttraumatic stress disorder (Pynoos and Eth 1986). Our model proposes an immediate response coordinated with law enforcement. Additionally, early intervention has been found to be effective in helping young sibling survivors (Freeman et al. 1996). Secondly, after the initial crisis phase, surviving families need long-term support for 12–18 months (Hatton 2003). During this period, family survivors need specialized support in the form of counseling to cope with the complex mix of trauma and complicated grief (Armour 2002). Additionally, during this phase, survivors need connection to other resources, advocacy with community systems, and a connection to a community of survivors. A third implication is the need to better develop and conceptualize the programmatic interventions, including the development of best practices for every component of the model. A fourth implication is the importance of the development of a community of survivors as an effective method of support. There appears to be limitations to what counseling and therapy can do to help support survivors. Practitioners need to develop and facilitate a network of survivors to connect family survivors with an extended, long-term support system. A fifth implication of this model is that a comprehensive program must take a family system approach (Vincent 2009), with particular focus on young sibling survivors. Practitioners need to support the family as a unit. It is necessary to support adult and child family members, but practitioners need to intervene where they see problems with familial relationships and functioning.
Finally, the development of this practice model points to questions for further research. There appears to be only a limited number of empirical studies that explore the effectiveness of interventions with parent and youth survivors of homicide victims. Murphy (2001) found mixed results in studying the effectiveness of a two-dimensional theory-based group intervention with parents who lost a child to a violent death. Whereas, Salloum et al. (2001) report reductions in PTSD using a time-limited therapeutic group curriculum with a population of African American youth. However, it was a pilot study with significant internal validity issues that require a cautious application of the findings. Further, a number of studies recommend interventions with survivors based on anecdotal clinical experience (Asaro 2009; Hertz et al. 2005; Armour 2002; Redmond 1989b; Masters et al. 1988; Getzel and Masters 1984). It appears that the current state of knowledge about what services survivors need is better understood. Future studies need to test the model presented here. How effective is an early response to survivors in mitigating early trauma? Which crisis intervention approach is most effective? Which long-term interventions are most effective in helping survivors manage the complex mix of trauma and complicated grief? What is the role of the community of survivors in effectively supporting survivors? What is the most effective intervention with youth survivors? Further, future empirical studies face some important methodological issues. First, what are the most relevant measures of effectiveness or outcomes for family survivors? Are there others (i.e. reduction in the intensity of complicated grief, improvement in daily functioning) in addition to the commonly cited reduction in posttraumatic stress disorder? A second methodological issue is the ethical issue of the use of a comparison group that denies potentially effective services to survivors. Use of waitlisted families as a comparison and delayed intervention designs are possible solutions. Thirdly, there are measurement issues when collecting data from traumatized families coping with the homicide of a loved one, especially when studying the effectiveness of early interventions. Families are struggling with early symptoms of posttraumatic stress disorder and may have difficulty completing self-report measures. Despite these methodological concerns, clearly, more needs to be known about what is the most effective mix of interventions when family survivor of the homicide of a loved one.
References
Ahmed, F.E., & Feldman, M. (1999). Survivors for violence prevention: National policy report. Unpublished Manuscript. Boston, MA: Harvard School of Public Health, Division of Public Health Practice.
Aisenberg, E. (2001). Depression among Latino and young adolescents exposed to community violence. Hispanic Journal of Behavioral Sciences, 23, 378–398.
Amick-McMullan, A., Kilpatrick, D. G., Veronen, L. J., & Smith, S. (1991). Family survivors of homicide victims: Theoretical perspectives and an exploratory study. Journal of Traumatic Stress, 2(1), 21–35.
Armour, M. P. (2002). Experiences of covictims of homicide: Implications for research and practice. Trauma, Violence, & Abuse, 3(2), 109–124.
Asaro, M. R. (2009). Working with adult homicide survivors, part II: Helping family members cope with murder. Perspectives in Psychiatric Care, 37, 115–124.
Clements, P. T., & Burgess, A. W. (2002). Children’s responses to family member homicide. Family and Community Health, 25(1), 32–42.
Farrel, A., & Bruce, S. (1997). Impact of exposure to community violence on violent behavior and emotional distress among urban adolescents. Journal of Clinical Child Psychology, 26, 2–14.
Federal Bureau of Investigation. (2012). Uniform crime reports: Murder and non-negligent manslaughter. Released Fall 2013, http://www.fbi.gov/about-us/cjis/ucr/crime-in-the-u.s/2012/crime-in-the-u.s.-2012/violent-crime/murder/murdermain.
Fitzpatrick, K. M., & Boldizar, J. P. (1993). The prevalence and consequences of exposure to violence among African–American youth. Journal of the American Academy of Child and Adolescent Psychiatry, 32, 424–430.
Freeman, L. N., Shaffer, D., & Smith, H. (1996). Neglected victims of homicide: The needs of young siblings of murder victims. American Journal of Orthopsychiatry, 66(3), 337–345.
Gekoski, A., Adler, J. R., & Gray, J. M. (2013). Interviewing women bereaved by homicide: Reports of secondary victimization by the criminal justice system. International Review of Victimology, 19(3), 307–329.
Getzel, G. S., & Masters, R. (1984). Serving families who survive homicide victims. Social Casework: The Journal of Contemporary Social Work, 65, 138–144.
Hatton, Rebecca. (2003). Homicide bereavement counseling: A survey of providers. Death Studies, 27, 427–448.
Hertz, F. H., Prothrow-Stith, D., & Chery, C. (2005). Homicide survivors: Research and practical implications. American Journal of Preventive Medicine, 29(5S2), 288–295.
Horne, C. (2003). Families of homicide victims: Service utilization patters of extra-and intrafamilial homicide survivors. Journal of Family Violence, 18(2), 75–82.
Horowitz, K., Weine, S., & Jekel, J. (1995). PTSD symptoms in urban adolescent girls: Compounded community trauma. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 1353–1361.
Kilpatrick, D. G., Acierno, R., Saunders, B., Resnick, H., & Best, C. (2000). Risk factors for adolescent substance abuse and dependence: Data from a national sample. Journal of Consulting and Clinical Psychology, 65, 1–12.
Kilpatrick, D. G., & Resnick, H. S. (1993). PTSD associated with exposure to criminal victimization in clinical and community populations. In J. R. Davidson & E. B. Foa (Eds.), Post-traumatic stress disorder in review: Recent research and future directions (pp. 113–143). Washington, DC: American Psychiatric Press.
Kliewer, W., Lepore, S. J., Oskin, D., & Johnson, P. D. (1998). The role of social support and cognitive processes in children’s adjustment to community violence. Journal of Consulting and Clinical Psychology, 66, 199–209.
Lipsey, M. W., & Derzon, J. H. (1998). Predictors of violent or serious delinquency in adolescence and early adulthood: A synthesis of longitudinal research. In R. Loeber & D. Farrington (Eds.), Serious & violent juvenile offenders: Risk factors and successful interventions (pp. 86–105). Thousand Oaks, CA: Sage Publications, Inc.
Masters, R., Friedman, L. N., & Getzel, G. (1988). Helping families of homicide victims: A multidimensional approach. Journal of Traumatic Stress, 1(1), 109–125.
Maza, J. J., & Reynolds, W. M. (1999). Exposure to violence in inner-city adolescents: Relationships of suicidal ideation, depression, and PTSD symptomology. Journal of Abnormal Child Psychology, 27(3), 203–214.
Murphy, S. A. (2001). Parent bereavement stress and preventive intervention following the violent deaths of adolescent or young adult children. Death Studies, 20, 441–452.
Murphy, S. A., Baugher, R., Lohan, J., Scheideman, J., Heerwagen, J., & Johnson, L. C. (1996). Parents’ evaluation of a perspective intervention following the sudden, violent deaths of their children. Death Studies, 20, 453–468.
Murphy, S. A., Braun, T., Tillery, L., Cain, K. C., Johnson, L. C., & Beaton, R. D. (1999). PTSD among bereaved parents following the violent deaths of their 12- to 28-year old children: A longitudinal prospective analysis. Journal of Traumatic Stress, 12(2), 273–291.
Overstreet, S., & Braun, B. S. (2000). Exposure to community violence and post-traumtic stress symptoms: Mediating factors. American Journal of Orthopsychiatry, 70(2), 263–271.
Parkes, C. M. (1993). Psychiatric problems following bereavement by homicide or manslaughter. British Journal of Psychiatry, 162, 49–54.
Pynoos, R., & Eth, S. (1986). Witness to violence: The child interview. Journal of the American Academy of Child Psychiatry, 25, 306–319.
Rando, T. A. (1993). Treatment of complicated mourning. Chicago: Research Press.
Redmond, L. M. (1989a). Surviving: When someone you loved was murdered. Clearwater, FL: Psychological Consultation and Educational Services Inc.
Redmond, L. M. (1989b). Surviving when someone you love was murdered: A professionals guide to group grief therapy for families and friends of murder victims. Clearwater, FL: Psychological Consultation and Education Services Inc.
Resnick, M. D., Ireland, M., & Borowsky, I. (2004). Youth violence perpetration: What protects? what predicts? findings from the national longitudinal study of adolescent health. Journal of Adolescent Health, 35(5), 424–434.
Richerts, J. E., & Martinez, P. (1993). Children as victims of and witnesses to violence in a Washington, DC neighborhood. In L. Leavitt & N. Fox (Eds.), Psychological effects of war and violence on children (pp. 243–278). Hillsdale, NJ: Lawrence Erlbaum Associations, Inc.
Rynearson, E. K. (1994). Psychotherapy of bereavement after homicide. The Journal of Psychotherapy Practice and Research, 3, 341–347.
Salloum, A., Avery, L., & McClain, R. P. (2001). Group psychotherapy for adolescent survivors of homicide victims: A pilot study. Journal of the American Academy of Child and Adolescent Psychiatry, 40(11), 1261–1267.
Salloum, A., & Vincent, N. (1999). Community-based groups for inner city adolescent survivors of homicide victims. Journal of Child and Adolescent Group Therapy, 9(1), 27–45.
Sharpe, T. (2008). Sources of support for African American family members of homicide victims. Journal of Ethnic & Cultural Diversity in Social Work, 17(2), 197–216.
Spunge, D. (1998). Homicide: The hidden victims-a guide for professionals. Thousand Oaks, CA: Sage.
van Denderen, M., de Keijser, J., Kleen, M., & Boelen, P. A. (2013). Psychopathology among homicidally bereaved individuals: A systematic review. Trauma, Violence, & Abuse, 20(10), 1–11.
Vessier-Batchen, M., & Douglas, D. (2006). Coping and complicated grief in survivors of homicide and suicide decedents. Journal of Forensic Nursing, 2(1), 25–32.
Vigil, G. J., & Clements, P. T. (2003). Child and adolescent homicide survivors: Complicated grief and altered worldviews. Journal of Psychosocial Nursing and Mental Health Services, 41(1), 30–39.
Vincent, N. J. (2009). The impact of community violence on the family: Disruptions in relationships and functioning. Families in Society: The Journal of Contemporary Social Services, 90(2), 137–143.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Vincent, N.J., McCormack, J. & Johnson, S. A Comprehensive Conceptual Program Model for Supporting Families Surviving a Homicide Victim. Child Adolesc Soc Work J 32, 57–64 (2015). https://doi.org/10.1007/s10560-014-0362-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10560-014-0362-4