
Abstract
We aimed to determine whether the Framingham risk score (FRS), systematic coronary risk evaluation (SCORE), and Chinese multi-provincial cohort study (CMCS) could predict anatomic severity of coronary plaques. From January 2007 to October 2010, we performed a contrast-enhanced 64-slice or 256-slice multidetector computed tomography coronary angiography as part of a health check-up protocol in 806 asymptomatic subjects (70.5% male, 56 ± 9 year-old). Risk scores significantly correlated with calcium volume score, plaque stenosis score and plaque distribution score (P < 0.001). Of the 3 risk scores, the SCORE system showed the best correlation. Overall, 180 (22%) and 37 (5%) subjects were found to have stenosis of 50-69% and more than 70% in at-least one coronary artery segment, respectively. In the prediction of the presence of obstructive CAD (≥50% diameter stenosis), all risk scores had similar discrimination. In the prediction of severe CAD (≥70% diameter stenosis), FRS and CMCS had similar area under curves but SCORE discriminated better than FRS (P < 0.05). The optimal cutoff point to predict obstructive CAD was 9.54% for FRS, 1.05% for CMCS, and 0.95% for SCORE, whereas to predict severe CAD was 9.63, 1.05, 1.15% for FRS, CMCS, SCORE, respectively, with a sensitivity of 0.61–0.70 and a specificity of 0.55–0.66. Cardiovascular risk scores are associated with the severity and extent of coronary artery plaque. The stronger association might translate into a better discrimination using SCORE. These findings will aid in the appropriate selection or recalibration of the risk assessment system for cardiovascular disease screening.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Both risk score and plaque imaging have been proposed as important tools in risk assessment. Plaque imaging with 64-slice or 256-slice multidetector computed tomography (MDCT) has been verified by invasive coronary angiography as a good diagnostic tool in detecting obstructive coronary artery disease (CAD) [1, 2]. Moreover, consistent with previous studies using conventional angiography and intravascular ultrasound, CAD severity detected by MDCT angiography can accurately predict major adverse cardiac events for the subsequent 18 months [3, 4].
Accurate identification of individuals at risk of coronary events is highly desirable. For the purposes of cardiovascular risk assessment in healthy individuals, most clinicians use a combination of traditional risk factors. Among the various risk-estimation systems, the Framingham Risk Score (FRS) is the most commonly used to predict 10-year cardiovascular risk [5]. Because the original Framingham functions overestimated the cardiovascular risk in the Chinese population, a prediction model specific to the Chinese population has been established on the basis of the Chinese Multi-provincial Cohort Study (CMCS) [6]. Based on a substantially larger dataset that contains 205,178 persons, the Systematic COronary Risk Evaluation (SCORE) model is the risk assessment system recommended by the European Third Joint Task Force on cardiovascular disease prevention [7].
Indeed, the above 3 cardiovascular risk scores are well recognized for their associations with clinical events and acute coronary syndromes, but to be clinically useful, a cardiovascular risk-estimation system should be strongly associated with coronary plaques, especially coronary plaque distribution and stenosis severity. Data on the association of risk scores and plaque severity are limited [8, 9]. Hence, this study was performed to assess the relationship between risk scores and plaque severity and compare the accuracy of risk scores to predict obstructive CAD.
Materials and methods
Subjects
Study participants were enrolled from consecutive subjects who underwent MDCT coronary angiography as part of a general health check-up protocol at the National Taiwan University Hospital between January 2007 and October 2010. The major exclusion criteria were irregular heartbeats during the MDCT procedure, serum creatinine levels ≥2.0 mg/dL, known hypersensitivity to iodine-based contrast agents, history of exertional chest tightness or prior known CAD, overt liver disease, hypothyroidism, alcohol, or drug abuse. The ethics committee approved the study protocol and all subjects provided written informed consent. Structured questionnaires on family history, lifestyle habits, and medical history were collected, as well as anthropometric measurements, such as body weight, body height, and waist circumference. Blood pressure was measured in a resting position. All biochemical measurements, including glucose, total cholesterol, total triglycerides, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, uric acid, and creatinine concentrations were measured using a Hitachi 7450 automated analyzer (Hitachi, Tokyo, Japan). The coefficients of variation of these measurements were approximately 5%.
Cardiovascular risk assessment
The Framingham score is based on data from a sample of the Framingham Heart studies [5]. The defining risk factors for Framingham risk scores are age, cigarette smoking, blood pressure, total cholesterol, high-density lipoprotein cholesterol, and diabetes. The categories for continuous variables of age, systolic blood pressure, LDL cholesterol, and HDL cholesterol are based on the National Cholesterol Education Program Adult Treatment Panel II (ATP-II) guidelines [10]. FRS is used to predict the 10-year risk of coronary events (fatal/nonfatal myocardial infarction or sudden death). A FRS value < 10, 10% to 20, or > 20% indicates a low, intermediate, or high risk for coronary events. The CMCS score is the Chinese recalibration version of the Framingham function [6]. Thus, the discrimination of the CMCS function remains virtually the same with the original Framingham risk function. The cohort comprised of 30,121 participants aged 35–64 years from 11 Chinese provinces that were followed up for 12 years. For each patient, 10-year risk of coronary events was predicted. The SCORE risk assessment system was derived from a large (205,178 participants) data set of prospective European studies [7]. The SCORE risk used the following variables: sex, age, total cholesterol, systolic blood pressure, and smoking. The SCORE chart did not directly comprise diabetes as a variable. The score risk in diabetic patients is multiplied twofold in men and fourfold in women. SCORE predicts the 10-year risk of cardiovascular fatal events. A SCORE value higher than 5% indicates a high risk for cardiovascular fatal events.
MDCT analysis
Subjects, without contraindications, received propranolol or diltiazem targeting a heart rate of ≤ 65 bpm and nitroglycerin 0.4 mg sublingually before image acquisition. Cardiac MDCT was performed using a 64-slice scanner (LightSpeed VCT, GE Healthcare, Milwaukee, WI, USA) or a 256-slice scanner (Brilliance iCT, Philips, Eindhoven, The Netherlands). Initial unenhanced axial CT imaging of the heart was obtained with prospective ECG trigger for the purpose of coronary artery calcium scoring (Agatston method). Then, nonionic contrast media (iopromide; Ultravist 370 mgI/mL, Bayer HealthCare) was injected using a dual-barrel injector (Stellant D, Medrad). Contrastenhanced CT was performed with images obtained from the mid ascending aorta to the diaphragm. The scanning parameters for 64-slice scanner were 0.625 mm slice thickness, 120 kV tube voltage and 0.35 s tube rotation time. The scanning parameters for 256-slice scanner were 0.8 mm slice thickness, 120 kV tube voltage and 0.27 s tube rotation time. The tube current was adjusted based on subjects’ body mass index. When heart rate was ≤ 65/min, prospective ECG triggering was used and the images were obtained at 70, 75 and 80% of the cardiac cycle. When heart rate was > 65/min, retrospective gating was used and the images were reconstructed at 40, 45, 55, 70, 75 and 80% of the cardiac cycle. The estimated radiation dose using a 64-slice scanner or a 256-slice scanner was 5.1 ± 1.6 or 5.6 ± 1.7 mSv, respectively with the use of prospective ECG triggering and 16.6 ± 4.4 or 13.8 ± 4.6 mSv, respectively with the use of retrospective ECG gating.
MDCT was performed by an experienced investigator (Lee WJ) who was unaware of the subjects’ clinical information. A 17-segment model of the coronary arteries was used for the evaluation and visual semi-quantification of coronary artery plaque [3, 11]. In each coronary artery segment, coronary atherosclerosis was defined as tissue structures > 1 mm2 that existed either as (1) calcified plaques with high density compared to the contrast-enhanced vessel lumen, (2) noncalcified plaques with lower density, or (3) mixed (calcified and non-calcified morphologies). We adopted two coronary artery plaque scores constructed by Min et al. [12] to assess the severity of coronary plaques, segment-stenosis score and segment-involvement score. Briefly, the segment stenosis score was used as a measure of overall coronary artery plaque extent. Each individual coronary segment was graded as normal, mild (< 50%), moderate (50–69%), or severe (> 70%) based on extent of obstruction of coronary luminal diameter. Then the extent scores of all 17 individual segments were summed to yield a total score ranging from 0 to 51. As a measure of overall coronary artery plaque distribution, a segment involvement score was calculated as the total number of coronary artery segments exhibiting plaques, irrespective of the degree of luminal stenosis within each segment (minimum = 0; maximum = 17). The same method was used to sum segments according to plaque composition (isolated calcified, isolated noncalcified plaque, and mixed plaque). Moreover, the presence of one or more stenoses with ≥50% reduction in luminal diameter in at least one major epicardial coronary artery or its branches was defined as obstructive CAD, whereas that with ≥70% reduction in luminal diameter was defined as severe CAD.
Statistical analysis
Demographic data and risk factors are expressed as mean ± standard deviation or median (25th to 75th percentile), and frequencies are given as counts (%). Data were tested for normal distribution prior to utilization in parametric analysis. Differences in group means or proportions were assessed using analysis of variance followed by a Tukey’s test or Pearson chi-square test as appropriate. In variables not normally distributed, differences in group medians were assessed by the Kruskal–Wallis test. The associations with risk scores were assessed by the age- and sex-adjusted partial correlations and Spearman’s rho. The area under the receiver-operating characteristic curve (ROC) was used to compare the discriminatory capability among the 3 risk assessment systems. Statistical differences in the area under the receiver operating characteristic curves were compared using the non-parametric method. The 2 × 2 contingency tables divided by optimal cut-off point were generated for risk scores versus obstructive CAD or severe CAD. Cohen’s kappa was measured to check the agreement. A probability value of P < 0.05 was considered significant. All calculations were performed with SPSS statistical software (SPSS 15.0 version for windows, SPSS, Chicago, IL, USA).
Results
Baseline characteristics
The study cohort consisted of 806 subjects without exertional chest tightness or prior known CAD (Table 1). Mean age was 56 ± 9 years (range 22–83 years), and 568 (70.5%) were men. The prevalence of diabetes, hypertension, hypercholesterolemia, and smoking were 9.3, 28.8, 17.0, and 14.3%, respectively. With increasing severity of coronary stenosis, subjects were likely to be older, male and obese and had lower HDL and higher LDL, glucose, creatinine, blood pressure, C-reactive protein, calcium score and plaque scores. Subjects with obstructive CAD (≥50% diameter stenosis) were more likely to be receiving lipid-lowering drugs. Thus, the trend of a higher level of total cholesterol among patients with obstructive CAD did not reach statistical significance. No difference was observed for smoking or cardiac function between patients with and without obstructive CAD.
Coronary artery plaques
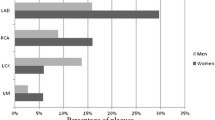
Coronary artery plaques were detected in 480 (60%) subjects. After the exclusion of 171 (1.2%) coronary segments with insufficient image quality, plaques of any type were shown in 1,389 (10%) segments. Majority of plaques were calcified (44%), followed by mixed (30%) and noncalcified (26%). However, on a per segment analysis, mixed plaques were more obstructive at the 50% thresholds (53%), as compared to noncalcified plaques (32%) and calcified plaques (15%). Moreover, at the 70% thresholds, mixed plaques (48%) and non-calcified plaques (43%) were often more obstructive than calcified plaques (10%). Within respective composition categories, mixed plaques were more obstructive at the 50% thresholds (58%), as compared to noncalcified plaques (40%) and calcified plaques (11%). At the 70% thresholds, mixed plaques (7%) and non-calcified plaques (7%) were often more obstructive than calcified plaques (1%).
Cardiovascular risk assessment
Overall, the median FRS, CMCS, and SCORE were 8.6%, 1.0%, and 0.9%, respectively (Table 1), indicating that the cohort had a low-to-intermediate risk for the development of future cardiovascular events. According to the Framingham risk score, 59.8% of subjects were at low risk, 31.1% at intermediate risk and 9.1% at high risk. An increase in the prevalence of obstructive CAD (18.6% low vs. 35.8% intermediate vs. 50.6% high) was observed across the FRS categories (P < 0.001). In contrast, only 42 (5.2%) of subjects were categorized into high risk according to SCORE risk. An increase in the prevalence of obstructive CAD (23.6% non-high vs. 66.6% high) was also observed across the SCORE categories (P < 0.001). Notably, 41.6% of patients with obstructive CAD fell into the low-risk FRS category and 25.1% of patients with no visible plaque fell into the intermediate-risk and high-risk FRS categories.
Risk scores and coronary artery disease
The correlations of various risk scores with calcium score and plaque scores were modest but significant (Table 2). Moreover, risk scores correlated better with total plaque scores than with isolated individual plaque scores. After adjustment for age and sex, risk scores correlated more strongly with segment-stenosis scores than with segment-involvement scores (Table 3). In risk scores, SCORE had a stronger association with calcium score and plaque scores than CMCS or FRS, even after controlling for age and sex. Within respective plaque composition categories, Spearman’s rho correlations with the risk scores were calcified, mixed and noncalcified, in descending order.. However, after adjustment for age and sex, the relation of risk scores to calcified plaque became insignificant. In the prediction of the presence of obstructive CAD, all risk scores had similar discrimination. The areas under the ROC curves for FRS, CMCS, and SCORE were 0.67 (95% CI, 0.62–0.71), 0.67 (95% CI, 0.63–0.71) and 0.70 (95% CI, 0.66–0.74), respectively, indicating that risk scores significantly discriminated between the presence and absence of obstructive CAD (Fig. 1). In the prediction of the presence of severe CAD (Fig. 2), FRS and CMCS had similar area under the ROC curve (0.63 [95% CI, 0.53–0.73], 0.65 [95% CI, 0.56–0.74], respectively) and SCORE discriminated better than FRS (0.71 [95% CI, 0.63–0.78] vs. 0.63 [95% CI 0.53–0.73], P < 0.05). The optimal cutoff points of risk scores to predict severe CAD was similar to or slightly higher than that to predict obstructive CAD, indicating a risk accumulation process from less obstructive CAD to severe CAD (Tables 4, 5). At the threshold set by optimal cutoff points, Cohen’s kappa was 0.23 for obstructive CAD but 0.05–0.07 for severe CAD, indicating a fair agreement between the risk scores and obstructive CAD but a weak agreement between the risk scores and severe CAD.

Receiver operating characteristic curves for various risk scores to discriminate obstructive coronary artery disease. The risk scores similarly and significantly discriminated the obstructive coronary artery disease. FRS Framingham risk score, ROC receiver operating characteristic curve, CMCS Chinese multi-provincial cohort study, SCORE systematic coronary risk evaluation

Receiver operating characteristic curves for various risk scores to discriminate severe coronary artery disease. Among the three risk scores, SCORE discriminated best for the severe coronary artery disease. FRS Framingham risk score, ROC receiver operating characteristic curve, CMCS Chinese multi-provincial cohort study, SCORE systematic coronary risk evaluation
Clinical outcomes
Overall, 180 (22.3%) and 37 (4.6%) were found to have moderate stenosis (50–69%) and severe stenosis (≥70%) in at-least one coronary artery segment, respectively. Stress/rest thallium-201 myocardial perfusion imaging or treadmill exercise testing was performed in 101 (56%) subjects with moderate stenosis and 21 (57%) subjects with severe stenosis. Of the subjects with stress testing, myocardial ischemia was found in 15 (15%) with moderate stenosis and 15 (71%) with severe stenosis. In subjects with evidence of myocardial ischemia, 10 (71%) with moderate stenosis and 14 (93%) with severe stenosis underwent percutaneous coronary intervention. In these 24 patients, the sensitivity, specificity, accuracy, PPV and NPV of MDCT were 85, 100, 92, 100 and 85%, respectively to detect significantly stenotic lesions (≥50% diameter stenosis), using invasive coronary angiography as the standard of reference on a per-segment analysis.
Discussion
To the best of our knowledge, this is the first study that reports on the comparison of various cardiovascular risk scores with CAD severity, using 64-slice or 256-slice MDCT, in a cohort of apparently healthy individuals without a history of coronary interventions. The main findings are the following: (1) the cohort had a low-to-intermediate risk for the development of future cardiovascular events but a relatively high prevalence of obstructive CAD; (2) risk scores correlated well with calcium scores and plaque scores; (3) risk scores significantly predicted obstructive CAD but the discrimination accuracy of risk scores changed with advancing CAD.
MDCT coronary angiography in individuals without known CAD is an effective noninvasive alternative to invasive coronary angiography to detect obstructive CAD. In patients with suspected but undocumented CAD, the prevalence of obstructive CAD demonstrated by MDCT is 18–35% [3, 8, 9, 13, 14] in whites. A similar prevalence rate of obstructive CAD (27%) was found in the present study. Moreover, Johnson et al. found 9% of 1,653 patients without previously known CAD (66% male, 53 ± 10 year-old, >90% white, median FRS 8%) had severe CAD [8], whereas only 4.6% of subjects had severe CAD in the present study, indicating that Chinese have less severe CAD than whites under similar Framingham risk score. In Asian studies, Jeong et al [15] studied 1,529 middle-aged asymptomatic Korean adults with 64-slice CT scan. Obstructive CAD was identified in 52 (9.3%) individuals. Iwasaki et al [16] investigated the prevalence of coronary plaques in the Japanese population with a low-to-intermediate risk for coronary artery disease. Obstructive CAD was detected in 91 patients (21.9%). Thus, the prevalence of obstructive CAD detected by MDCT differs widely among various populations in Asia.
In the prognosis study by Chow et al. [3] with 64-slice MDCT, patients with obstructive CAD had an annual coronary event rate of 2.7% (i.e. 10-year risk 27%). In contrast, the present study cohort had a median 10-year risk of 8.6% by FRS, significantly lower than the data by Chow et al [3]. These findings suggest Chinese have similar CAD prevalence but less 10-year coronary events compared to whites. This difference would be explained by the slower progression of coronary artery calcification and the low age-standardized death certification rates from coronary artery disease [17, 18]. Notably, coronary events are not just a matter of stenosis severity but also of plaque stability [3, 19, 20]. Whether Chinese have more stable plaques than whites needs further studies, which may inform clinical interpretation and provide a rationale for more aggressive risk factor modification, even in asymptomatic subjects with low-to-moderate risk [21].
We found that risk scores correlated well with calcium scores and plaque scores, especially the segment-stenosis score of the total plaques. This finding suggests that the actual target which clinical risk scores measure is the total plaque extent and stenosis severity. However, the major determinants of coronary plaques in the coronary events are a large plaque burden, a small luminal area and a thin-cap fibroatheroma, as determined by intravascular ultrasonography [22]. Thin-cap fibroatheromas are most frequently observed in mixed plaques as compared with noncalcified and calcified plaques [23]. In the present study, risk scores correlated well but not good enough with the severity of mixed plaques. This clearly indicates that risk scores currently miss a substantial number of factors responsible for major adverse cardiovascular events.
Calcium score and plaque scores provide incremental prognostic value over risk scores to predict coronary events [3, 12, 13, 24]. We observed that calcium score and plaque scores were modestly correlated with risk scores as follows in descending order: SCORE, CMCS, and FRS. Coronary artery calcium and plaque are parts of CAD development and occur exclusively in atherosclerotic CAD and are absent in normal arteries [25]. The progression of coronary calcium and artery plaque associates with increased risk of coronary events, whereas stable calcium score and plaque associates with lower risk of coronary events [3, 26]. Based on these findings, one may speculate that the risk score which is well correlated with calcium and plaque scores may have additional benefits in risk assessment. This speculation could be partly verified by the observation that the discrimination accuracy of SCORE was better than CMCS and FRS, especially in the prediction of severe CAD, a condition associated with higher calcium and plaque scores.
Obstructive CAD precedes the coronary events [22]. If a risk assessment system can predict that the contemporary severity of CAD existed, then it may better predict future coronary events as well. In the present study, the areas under the curves of cardiovascular risk scores to discriminate the presence of obstructive or severe CAD are in the region of 0.63–0.71. However, the usual areas under curves of risk scores to discriminate coronary events have been reported to be in the region of 0.75–0.80 [5–7], indicating that the risk scores predict coronary events better than obstructive CAD. With advancing age, coronary arteries become narrower with more calcification and plaques. Since risk scores have a significant relationship with calcium score and total plaque scores, increased coronary calcium and plaque over time may partly explain why the area under the curve is larger for the prediction of coronary events than for the prediction of the present obstructive CAD.
In the present study, the risk score categories divided by optimal cut-off point had a fair agreement with obstructive CAD but a weak agreement with severe CAD. Similar kappa values between the FRS risk categories and the plaque categories have been described by others [8]. Cohen’s kappa, a measure of agreement corrected for chance is dependent on the quality of the test and on the prevalence of the disease in the population in which the test is applied. Both 64-slice or 256-slice MDCT possesses high diagnostic accuracy for detection of obstructive coronary stenosis at both thresholds of 50 and 70% stenosis [1, 2]. On the other hand, we found a total of 14.6% of subjects received statin treatment for hyperlipidemia, especially in subjects with obstructive CAD. Obviously, statin therapy significantly lowers the risk scores by decreasing the total cholesterol or LDL level. However, even with high-dose statin therapy, it still takes 18–24 months to diminish atheroma volume by 0.4–1% [27, 28]. Thus, the risk scores likely underestimate plaque extent in patients receiving the lipid-lowering drug for less than a decade. After all, the weak agreement with severe CAD could be attributed to statin use and low disease prevalence.
Study limitations
Several study limitations should be considered when interpreting these findings. First, invasive coronary angiography and MDCT differ significantly in estimating the presence and nature of CAD [29]. Overall correlation between invasive coronary angiography and MDCT for detection of CAD was poor (kappa = 0.25). The false-positive rate of MDCT for detecting significant coronary artery stenosis was high (55.8%) [15]. However, plaque volumes measured by 64-slice MDCT and intravascular ultrasound correlate well (r = 0.84, P < 0.0001), without systematic underestimation [30]. The sensitivity and specificity of MDCT to detect stenoses greater than 50% by invasive coronary angiography are excellent with the administration of nitroglycerin before imaging. Second, the study population was not a representative sample from the general population, which limited external generalization. Participants in our study were Chinese and FRS was known to overestimate Chinese’ cardiovascular risk; thus, the value of FRS was higher than that of CMCS or SCORE. With this limitation in mind, FRS had similar discrimination accuracy to the other scores for detecting obstructive CAD. Thus, FRS is still a useful tool for risk stratification in the Chinese population. Further studies are needed to demonstrate whether the results could be applicable to different racial groups. Finally, we did not have data on the outcomes related to CAD severity to determine which risk scores might be more predictive of coronary events.
Conclusion
In asymptomatic ethnic Chinese population, risk scores could significantly predict the presence of obstructive CAD. Of the 3 risk scores, SCORE system correlated best with coronary calcium and plaque severity. This association might translate into better discrimination in predicting severe CAD. These findings will aid in the appropriate selection or recalibration of the risk assessment system in cardiovascular disease screening. Further evaluation of coronary artery system using MDCT will be needed in patients who have higher cardiovascular risk scores.
References
Budoff MJ, Dowe D, Jollis JG, et al (2008) Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 52(21):1724–1732
Chao SP, Law WY, Kuo CJ et al (2010) The diagnostic accuracy of 256-row computed tomographic angiography compared with invasive coronary angiography in patients with suspected coronary artery disease. Eur Heart J 31(15):1916–1923
Chow BJ, Wells GA, Chen L et al (2010) Prognostic value of 64-slice cardiac computed tomography severity of coronary artery disease, coronary atherosclerosis, and left ventricular ejection fraction. J Am Coll Cardiol 55(10):1017–1028
Hadamitzky M, Freissmuth B, Meyer T et al (2009) Prognostic value of coronary computed tomographic angiography for prediction of cardiac events in patients with suspected coronary artery disease. JACC Cardiovasc Imaging 2(4):404–411
Wilson PW, D’Agostino RB, Levy D et al (1998) Prediction of coronary heart disease using risk factor categories. Circulation 97(18):1837–1847
Liu J, Hong Y, D’Agostino RB Sr et al (2004) Predictive value for the Chinese population of the Framingham CHD risk assessment tool compared with the Chinese multi-provincial cohort study. JAMA 291(21):2591–2599
Conroy RM, Pyorala K, Fitzgerald AP et al (2003) Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J 24(11):987–1003
Johnson KM, Dowe DA, Brink JA (2009) Traditional clinical risk assessment tools do not accurately predict coronary atherosclerotic plaque burden: a CT angiography study. AJR Am J Roentgenol 192(1):235–243
Nucifora G, Schuijf JD, van Werkhoven JM et al (2009) Prevalence of coronary artery disease across the Framingham risk categories: coronary artery calcium scoring and MSCT coronary angiography. J Nucl Cardiol 16(3):368–375
Grundy SM, Bilheimer D, Chait A et al (1993) Summary of the second report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel II). JAMA 269(23):3015–3023
Hoffmann U, Moselewski F, Cury RC et al (2004) Predictive value of 16-slice multidetector spiral computed tomography to detect significant obstructive coronary artery disease in patients at high risk for coronary artery disease: patient-versus segment-based analysis. Circulation 110(17):2638–2643
Min JK, Shaw LJ, Devereux RB et al (2007) Prognostic value of multidetector coronary computed tomographic angiography for prediction of all-cause mortality. J Am Coll Cardiol 50(12):1161–1170
Russo V, Zavalloni A, Bacchi Reggiani ML et al (2010) Incremental prognostic value of coronary CT angiography in patients with suspected coronary artery disease. Circ Cardiovasc Imaging 3(4):351–359
Maffei E, Seitun S, Nieman K, et al (2010) Assessment of coronary artery disease and calcified coronary plaque burden by computed tomography in patients with and without diabetes mellitus. Eur Radiol (in press). doi:10.1007/s00330-00010-01996-z
Jeong HC, Ahn Y, Ko JS et al (2010) The role of 64-slice multi-detector computed tomography in the detection of subclinical atherosclerosis of the coronary artery. Int J Cardiovasc Imaging 26(Suppl 2):253–259
Iwasaki K, Matsumoto T, Aono H et al (2011) Prevalence of subclinical atherosclerosis in asymptomatic patients with low-to-intermediate risk by 64-slice computed tomography. Coron Artery Dis 22(1):18–25
Kronmal RA, McClelland RL, Detrano R et al (2007) Risk factors for the progression of coronary artery calcification in asymptomatic subjects: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 115(21):2722–2730
Levi F, Lucchini F, Negri E et al (2002) Trends in mortality from cardiovascular and cerebrovascular diseases in Europe and other areas of the world. Heart 88(2):119–124
van Werkhoven JM, Schuijf JD, Gaemperli O et al (2009) Incremental prognostic value of multi-slice computed tomography coronary angiography over coronary artery calcium scoring in patients with suspected coronary artery disease. Eur Heart J 30(21):2622–2629
Min JK, Feignoux J, Treutenaere J et al (2010) The prognostic value of multidetector coronary CT angiography for the prediction of major adverse cardiovascular events: a multicenter observational cohort study. Int J Cardiovasc Imaging 26(6):721–728
Maffei E, Seitun S, Martini C et al (2010) CT coronary angiography and exercise ECG in a population with chest pain and low-to-intermediate pre-test likelihood of coronary artery disease. Heart 96(24):1973–1979
Stone GW, Maehara A, Lansky AJ et al (2011) A prospective natural-history study of coronary atherosclerosis. N Engl J Med 364(3):226–235
Pundziute G, Schuijf JD, Jukema JW et al (2008) Head-to-head comparison of coronary plaque evaluation between multislice computed tomography and intravascular ultrasound radiofrequency data analysis. JACC Cardiovasc Interv 1(2):176–182
Shaw LJ, Raggi P, Schisterman E et al (2003) Prognostic value of cardiac risk factors and coronary artery calcium screening for all-cause mortality. Radiology 228(3):826–833
Greenland P, Bonow RO, Brundage BH, et al (2007) ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 49(3):378–402
Raggi P, Callister TQ, Shaw LJ (2004) Progression of coronary artery calcium and risk of first myocardial infarction in patients receiving cholesterol-lowering therapy. Arterioscler Thromb Vasc Biol 24(7):1272–1277
Nissen SE, Tuzcu EM, Schoenhagen P et al (2004) Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. JAMA 291(9):1071–1080
Nissen SE, Nicholls SJ, Sipahi I et al (2006) Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA 295(13):1556–1565
Butler J, Shapiro M, Reiber J et al (2007) Extent and distribution of coronary artery disease: a comparative study of invasive versus noninvasive angiography with computed angiography. Am Heart J 153(3):378–384
Ugolini P, Pressacco J, Lesperance J et al (2009) Evaluation of coronary atheroma by 64-slice multidetector computed tomography: comparison with intravascular ultrasound and angiography. Can J Cardiol 25(11):641–647
Acknowledgments
The study was partly supported by grants from the National Taiwan University Hospital and Department of Health, Taiwan (DOH99-TD-B-111-001). The authors appreciate the cooperation of the participants and also thank the staff of the Health Management Center in National Taiwan University Hospital for their help.
Conflicts of interest
The authors state that there are no conflicts of interest to be disclosed.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors Bai-Chin Lee and Wen-Jeng Lee contributed equally to this study.
Rights and permissions
About this article
Cite this article
Lee, BC., Lee, WJ., Hsu, HC. et al. Using clinical cardiovascular risk scores to predict coronary artery plaque severity and stenosis detected by CT coronary angiography in asymptomatic Chinese subjects. Int J Cardiovasc Imaging 27, 669–678 (2011). https://doi.org/10.1007/s10554-011-9874-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-011-9874-6