
Abstract
The aim of the present study was to characterize coronary plaques by Multi-Slice Computed Tomography (Siemens sensation 16, Forcheim, Germany) before significant angiographic progression occurred and to compare them to non-progressing lesions. The MSCT-morphology of coronary plaques leading to a rapid angiographic disease progression is not yet studied. In a series of 68 patients who were scheduled for surveillance angiography 6 months later, MSCT-angiography was done shortly after the baseline catheterisation-procedure. After surveillance angiography rapid progressive lesions with an increase of the stenosis severity of >20% were identified and analysed on the baseline MSCT-scan and were compared to non-progressing lesions. Six months after coronary stenting we observed significant progression of de novo stenoses in 10/438 coronary segments. The progression of four lesions lead to angina pectoris symptoms and the remaining six lesions progressed silently. Analysis of the lesion morphology by MSCT revealed that 5/10 (50%) progressing lesions were non-calcified 3/10 (30%) were predominantly non-calcified and 2/10 (20%) were mainly calcified on the baseline MSCT-scan. In the 428 segments without disease progression atherosclerotic lesions were found in 225 segments on MSCT. Non-calcified plaques were identified in 46 (20%), predominantly non-calcified lesions in 58 (26%) and predominantly calcified lesions in 121 (54%) segments. The average number of diseased coronary segments between patients with and without lesion progression was not significantly different between progressors and non-progressors with a higher prevalence of non-calcified segments in the progressor group (1.1 vs. 0.63). Rapid progression of the angiographic stenosis severity during a 6 months period occurs most frequently in coronary segments revealing non-calcified or predominantly non-calcified plaques as determined by MSCT, whereas lesion progression is rare in predominantly calcified segments. This represents first evidence that non-calcified lesions may be involved in the process of plaque rupture.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rapid progression of the angiographic stenosis-severity is most frequently caused by the rupture of a vulnerable plaque causing subsequent vessel obstruction or in the worst case total occlusion [1]. The initial morphology of such lesions before rupture or angiographic progression is not well studied yet.
Multi-Slice CT (MSCT) has become an emerging alternative to invasive coronary angiography to detect coronary stenoses [2, 3]. It further offers the opportunity to determine important compositional and morphologic features of both obstructive and non-obstructive coronary lesions [4–8]. Thus the aim of the present study was to characterize coronary lesions by MSCT before they show angiographic disease progression and compare them to non-progressing control lesions.
Methods and patients
Into this study we included 68 patients (age 61 ± 7 years, 49 males), in whom a stent was implanted due to a de novo stenosis in up to two coronary vessels. All patients had typical stable angina pectoris or/and evidence of ischemia in non-invasive stress-tests. Patients with prior bypass-surgery or angioplasty were excluded. The presence of a distinctive risk profile (at least two major risk factors) and angiographic evidence of at least one significant lesion (>75% diameter stenosis) that was stented in the same session were mandatory criteria for inclusion into the study. Atrial fibrillation, allergy against iodine or renal insufficiency and ineffective reduction of the heart rate <65 beats per minute prior to the MSCT-scan were exclusion criteria. All patients gave informed consent. The study protocol was approved by the institutional review board.
One to two days after the invasive procedure, contrast enhanced MSCT-angiography was performed. According to the study-protocol a catheter based control angiography was scheduled 6 months after the baseline scan. In the case of new onset of symptoms the angiogram was also done earlier.
The MSCT scan was done using a Siemens sensation 16-scanner (Siemens Medical Solutions, Forchheim, Germany) using a well described protocol for non-invasive coronary angiography (Protocol for non-invasive coronary angiography, 130 cc contrast agent, Altana Solutrast 300, retrospective ECG-Gating, Collimation 16× 0.75 mm, temporal resolution 180 ms), [6, 9]. In all patients with heart rates >70 beats per minute a beta-blocker were administered before the MSCT-scan. The scan was only done if the heart rate could be reduced below 65 bpm.
All baseline angiograms as well as the surveillance angiograms after 6 months were analysed by an experienced cardiologist using the Quantcor-software package (Siemens Medical, Forchheim, Germany). Based on the AHA-segment-classification the maximum diameter stenosis was determined for all proximal and mid coronary segments. (7-segment lesions were defined as rapid progressive if the grade of stenosis of a lesion causing increased at least by 20% during the 6 months period. Segments with a stent and small (<2.0 mm diameter) or distal segments, as well as segments providing non-diagnostic image quality on MSCT were not included.
The MSCT datasets were analysed by an experienced reader immediately after the scan. Coronary segments were classified as either normal, as containing non-calcified plaques, as containing mixed plaque with either predominantly non-calcified plaque (<50% of plaque area occupied by calcium) or calcified plaques according to previous studies [4, 6, 10].
Once a rapid progressing lesion was observed on the control angiogram after 6 months the exact location of that lesion was determined in the MSCT-dataset, based on characteristic landmarks.
Results
In the 68 patients 438 of potentially 680 proximal and middle coronary segments (According to the AHA segment-model: segments 1–4, 5–7, 9, 10–11) qualified for analysis. One hundred and eighteen segments were excluded because of a stent, 61 segments due to poor image quality and 63 segments due to a vessel diameter <2.0 mm. In these segments that were not included to the analysis two stenoses progressions were observed (both clinically silent). Atherosclerotic plaque was identified in 235/438 included segments by MSCT. Non-calcified plaque was present in 51 segments, predominantly non-calcified lesions in 61 segments and predominantly calcified plaques in 123 segments.
There was no significant difference of patient related characteristics of patients with or without disease progression (Table 1). The mean diameter stenosis on QCA at baseline was 29% in non-progressing lesions (analysis was done in 45 lesions/segments, in the remaining lesions/segments QCA was not applicable due to only minor diameter reductions or no identifiable lesions on angiography) versus 33% in progressing lesions.
MSCT composition of progressing plaques
Six months after coronary stenting we observed significant progression of de novo stenoses in 10/438 coronary segments in 68 patients. In four segments progression lead to angina pectoris symptoms and six lesions progressed silently. The prospective MSCT-analysis revealed that stenosis progression was observed in 5/10 segments with non-calcified plaques (50%) in 3/10 segments (30%) with mixed plaque and in 2/10 segments (20%) with calcified plaque. In the 225 segments with atherosclerotic plaques at baseline but without disease progression after 6 months, non-calcified plaques were identified in 46 (20%), predominantly non-calcified lesions in 58 (26%) and predominantly calcified lesions in 121 (54%) segments.
Frequency of progression dependent on MSCT derived plaque composition
Segments with non-calcified and predominantly non-calcified lesions showed a higher frequency of plaque progression (8/112 = 7.1%) compared to segments with calcified lesions (2/123 = 1.6%; P < 0.05) (Figs. 1–3).

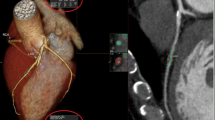
Segments containing non-calcified plaque revealed highest frequency of progression after 6 months

Lesion progression from initially 25% to 78% after 6 months. MSCT revealed a non-calcified lesion adjacent to calcified portion of the vessel wall on the baseline exam

Angiographic lesion progression from <30% to 74% after 4 months leading to acute myocardial infarction. MSCT at baseline revealed exclusively non-calcified plaque in the affected segment
Relation of the coronary plaque burden to lesion progression
The number of segments with atherosclerotic plaques in patients with and without lesion progression was 3.0 vs. 3.15, respectively (P = 0.17). The average number of segments with non-calcified plaque was 1.1 vs. 0.63 in patients with and without progression (P < 0.01). The number of calcified segments was not significantly different in the progressor and non-progressor group.
Discussion
In the present prospective observational study we have characterized plaque morphology of coronary segments before angiographic progression. Our results indicate that rapid stenosis progression most frequently occurs in segments containing non-calcified plaques or predominantly non-calcified plaques. The average number of diseased coronary segments among patients with and without lesion progression was not significantly different with a significant trend of a higher prevalence of non-calcified plaques in the progressor group.
So far only few data concerning morphologic characteristics of vulnerable lesions before rupture are known. In the only prospective evaluation Yamagishi et al. [11] have demonstrated by intravascular ultrasound, that lesions causing acute coronary syndroms within a 20 months observational period contain mainly soft tissue, show evidence of a necrotic core, large plaque burden and positive vessel wall remodelling. In histopathologic studies similar morphologic features were described retrospectively in already ruptured lesions [12]. In a recent publication Hoffmann et al. [13] demonstrated that culprit lesions in acute coronary syndromes always contain large volumes of non-calcified plaque tissue and that the prevalence of exclusively non-calcified lesions is high. In contrast they found hat culprit lesions in stable coronary artery disease were most frequently mixed or calcified with a lower prevalence of exclusively non-calcified plaques. These retrospective findings are in well concordance to our results. The findings of both studies indicate that non-calcified plaque types seem to be involved in the process leading to rapid plaque progression. This hypothesis is further underscored by findings of other studies using various imaging tools that also describe the phenomenon of multi-focal plaque instability. In a study using angioscopy, multiple lipidrich yellow plaques (vulnerable plaques) were found in patients with myocardial infarctions but not in patients with stable coronary artery disease [14]. It was further demonstrated that the number of yellow plaques is associated with the risk for future events [15]. In one of our own studies using MSCT we found a higher prevalence of non-calcified lesions in patients with myocardial infarction than in stable coronary artery disease patients [10]. In this context Hausleiter et al. [16] found recently that the presence of non-calcified coronary lesions either alone or in conjunction with calcified plaques is associated with higher CRP levels compared to patients with only calcified lesions, indicating a higher systemic inflammatory status. In the present study with a limited number of patients revealing disease progression we found no differences concerning the average number of diseased segments between progressors and non-progressors. The prevalence of non-calcified lesions was however higher in the progressor group. Future studies have to prove whether detection of non-calcified lesions that are missed by calcium scoring may improve risk stratification or may allow identification of focal plaque vulnerability, so that the additional radiation and contrast agent exposure can be justified. In our study all patients with rapid stenosis progression revealed significant calcified plaque burden apart from the progression site, which is in concorance with previous studies that indicate that the calcium score is a surrogate marker for the entire plaque burden and has significant prognostic implications [17]. Nevertheless it may be suggested that the risk for future adverse coronary events increases with the number of by MSCT identifiable non-calcified lesions and research in this direction should be motivated.
The majority of non-calcified lesions in our study did not reveal angiographic disease progression, so that there is no evidence that focal treatment of such lesions may be beneficial. In a recent publication Pundziute et al. [18] found no relation between the number of non-calcified lesions and adverse coronary events, they however observed that mixed plaques are related to unfavourable prognosis. The amount of non-calcified tissue in these mixed lesions was not further quantified. To better characterize lesions that are prone to cause adverse coronary events, more sophisticated tools that allow to assess functional, biological and morphological features, like the inflammatory status, neovascularisation, thickness of the fibrous cap and the size of the lipid core may be needed.
Limitations
The low number of progressing lesions is the major limitation of the present study, however to best of our knowledge this is one of the first studies reporting from MSCT-characteristics of plaques that subsequently lead to stenosis progression.
The present study obviously was performed in a symptomatic high-risk patient cohort with a high prevalence of both calcified and non-calcified lesions, involving almost 50% of all coronary segments. Outside of clinical studies, CT-angiography is not recommended in these patients, it is more appropriate in patient populations with an intermediate likelihood for coronary artery disease and thus our results cannot easily be transferred.
Our study was performed using a 16-slice scanner, to date scanners creating 64–256 slices per rotation with further improved temporal and spatial resolution are available, that significantly improved the clinical suitability and image quality of coronary imaging especially in patients with higher heart rates. By our strict pre-selection criteria and the inclusion of only patients with heart rates below 65 bpm we partly compensated for that limitation.
References
Virmani R, Burke AP, Kolodgie FD, Farb A (2002) Vulnerable plaque: the pathology of unstable coronary lesions. J Interv Cardiol 15:439–446
Leber AW, Knez A, Mukherjee R, White C, Huber A, Becker A, Becker CR, Reiser M, Haberl R, Steinbeck G (2001) Usefulness of calcium scoring using electron beam computed tomography and non-invasive coronary angiography in patients with suspected coronary artery disease. Am J Cardiol 88:219–223
Leschka S, Alkadhi H, Plass A, Desbiolles L, Grunenfelder J, Marincek B, Wildermuth S (2005) Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J 26:1482–1487
Leber AW, Becker A, Knez A, von Ziegler F, Sirol M, Nikolaou K, Ohnesorge B, Fayad ZA, Becker CR, Reiser M, Steinbeck G, Boekstegers P (2006) Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a comparative study using intravascular ultrasound. J Am Coll Cardiol 47:672–677
Leber AW, Knez A, von Ziegler F, Becker A, Nikolaou K, Paul S, Wintersperger B, Reiser M, Becker CR, Steinbeck G, Boekstegers P (2005) Quantification of obstructive and non-obstructive coronary lesions by 64-slice computed tomography: a comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol 46:147–154
Leber AW, Knez A, Becker A, Becker C, von Ziegler F, Nikolaou K, Rist C, Reiser M, White C, Steinbeck G, Boekstegers P (2004) Accuracy of multi-detector spiral computed tomography in identifying and differentiating the composition of coronary atherosclerotic plaques: a comparative study with intracoronary ultrasound. J Am Coll Cardiol 43:1241–1247
Achenbach S, Moselewski F, Ropers D, Ferencik M, Hoffmann U, MacNeill B, Pohle K, Baum U, Anders K, Jang IK, Daniel WG, Brady TJ (2004) Detection of calcified and non-calcified coronary atherosclerotic plaque by contrast-enhanced, submillimeter multi-detector spiral computed tomography: a segment-based comparison with intravascular ultrasound. Circulation 109:14–17
Leber AW, Knez A, Becker A, Becker C, Reiser M, Steinbeck G, Boekstegers P (2005) Visualising non-calcified coronary plaques by CT. Int J Cardiovasc Imaging 21:55–61
Ropers D, Baum U, Pohle K, Anders K, Ulzheimer S, Ohnesorge B, Schlundt C, Bautz W, Daniel WG, Achenbach S (2003) Detection of coronary artery stenoses with thin-slice multi-detector row spiral computed tomography and multi-planar reconstruction. Circulation 107:664–666
Leber AW, Knez A, White CW, Becker A, von Ziegler F, Muehling O, Becker C, Reiser M, Steinbeck G, Boekstegers P (2003) Composition of coronary atherosclerotic plaques in patients with acute myocardial infarction and stable angina pectoris determined by contrast-enhanced multi-slice computed tomography. Am J Cardiol 91:714–718
Yamagishi M, Terashima M, Awano K, Kijima M, Nakatani S, Daikoku S, Ito K, Yasumura Y, Miyatake K (2000) Morphology of vulnerable coronary plaque: insights from follow-up of patients examined by intravascular ultrasound before an acute coronary syndrome. J Am Coll Cardiol 35:106–111
Madjid M, Zarrabi A, Litovsky S, Willerson JT, Casscells W (2004) Finding vulnerable atherosclerotic plaques: is it worth the effort? Arterioscler Thromb Vasc Biol 24:1775–1782
Hoffmann U, Moselewski F, Nieman K, Jang IK, Ferencik M, Rahman AM, Cury RC, Abbara S, Joneidi-Jafari H, Achenbach S, Brady TJ (2006) Non-invasive assessment of plaque morphology and composition in culprit and stable lesions in acute coronary syndrome and stable lesions in stable angina by multi-detector computed tomography. J Am Coll Cardiol 47:1655–1662
Asakura M, Ueda Y, Yamaguchi O, Adachi T, Hirayama A, Hori M, Kodama K (2001) Extensive development of vulnerable plaques as a pan-coronary process in patients with myocardial infarction: an angioscopic study. J Am Coll Cardiol 37:1284–1288
Ohtani T, Ueda Y, Mizote I, Oyabu J, Okada K, Hirayama A, Kodama K (2006) Number of yellow plaques detected in a coronary artery is associated with future risk of acute coronary syndrome: detection of vulnerable patients by angioscopy. J Am Coll Cardiol 47:2194–2200
Hausleiter J, Meyer T, Hadamitzky M, Kastrati A, Martinoff S, Schomig A (2006) Prevalence of non-calcified coronary plaques by 64-slice computed tomography in patients with an intermediate risk for significant coronary artery disease. J Am Coll Cardiol 48:312–318
Knez A, Becker C, Becker A, Leber A, White C, Reiser M, Steinbeck G (2002) Determination of coronary calcium with multi-slice spiral computed tomography: a comparative study with electron-beam CT. Int J Cardiovasc Imaging 18:295–303
Pundziute G, Schuijf JD, Jukema JW, Boersma E, de Roos A, van der Wall EE, Bax JJ (2007) Prognostic value of multi-slice computed tomography coronary angiography in patients with known or suspected coronary artery disease. J Am Coll Cardiol 49:62–70
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Leber, A.W., von Ziegler, F., Becker, A. et al. Characteristics of coronary plaques before angiographic progression determined by Multi-Slice CT. Int J Cardiovasc Imaging 24, 423–428 (2008). https://doi.org/10.1007/s10554-007-9278-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-007-9278-9