
Abstract
Objective
Using the case–control data from the Selected Cancers Study, the authors assessed whether cigarette smoking increases the risk of primary liver cancer in the US.
Methods
Cases were men who were pathologically diagnosed with primary liver cancer during 1984–1988, were 31–59 years old, and lived in the areas covered by eight US cancer registries (n = 168). Controls were men without a history of primary liver cancer who were selected by random-digit telephone dialing (n = 1910).
Results
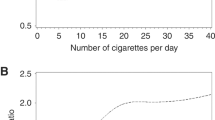
Relative to non-smokers, the risks of liver cancer were 1.85 (95% confidence interval (CI), 1.05–3.25) and 1.49 (95% CI, 0.83–2.68) for former and current smokers, respectively. The adjusted odds ratio (OR) estimates were 0.96, 1.43, 1.80, and 1.87 for smoking for less than 15, 15–24, 25–34 and 35 or more years, respectively (p for trend = 0.039). The OR estimates were 1.41 (95% CI, 0.74–2.68), 1.67 (95% CI, 0.93–2.98), and 1.83 (95% CI, 0.89–3.76) for less than 1, 1–2, and 2 or more packs smoked per day (p for trend = 0.068).
Conclusions
Cigarette smoking may be a factor that contributes somewhat to the occurrence of primary liver cancer among men in the United States, a country with low risk of liver cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There are geographic variations in liver cancer occurrence. Eastern and South Eastern Asia, Middle Africa, and some countries of Western Africa are the areas of high risk; most parts of Europe, Central America, Western Asia, and Northern Africa are areas of intermediate risk; and Northern Europe, United States, Canada, and Australia have low risk [1–3]. Liver cancer is rare before the age of 50 years in countries at low risk, while it has high incidence at middle age in countries at high risk [1, 3], suggesting differences in exposure to etiological factors in different areas. Infectious hepatitis and dietary aflatoxin exposure are well-documented risk factors for liver cancer in high-risk areas [4]. In low-risk areas, other risk factors may play a larger role.
Several investigations have studied the question of whether cigarette smoking is a risk factor for liver cancer [5–22]. Some cohort studies in high-risk areas showed a positive association, with odds ratio (OR) estimates for cigarette smoking and primary liver cancer including 1.4 (95% confidence interval (CI), 1.3–1.6) [5] in current smoking men relative to non-smoking men, 1.50 (95% CI, 1.29–1.74), 3.3 (95% CI, 1.2–9.5), 1.55 (95% CI, 1.06–2.26), and 2.23 (95% CI, 1.53–3.23) for current smokers compared with non-smokers [6–9], and 3.14 (95% CI, 1.82–5.42) for daily smoking compared with non-smoking [10]. Some case–control studies also found an association between cigarette smoking and liver cancer [11–15]. However, a number of cohort and case–control studies in high-risk areas were unable to demonstrate the hypothesized association [16–22] or to identify a dose-response relationship between smoking and liver cancer [13, 18, 20].
The United States is a low-risk country, where well-documented risk factors such as hepatitis virus infection and dietary aflatoxin exposure are less prevalent. It is important to study cigarette smoking in low-risk areas, not only because smoking may have larger effects on the occurrence of liver cancer in these areas, but also because it may be easier to delineate the role of cigarette smoking as a result of low “noise” from such factors as hepatitis infection and aflatoxin exposure. In fact, studies in the US have generated more consistent results. In contrast to case–control studies by Austin et al. and Stemhagen et al. [23, 24] in which no association between cigarette smoking and liver cancer was identified, other studies found a positive association. An early US study, a small case–control investigation in Caucasians and African Americans, showed that cases were more than twice likely to be current smokers than controls [25]. Subsequent case–control and cohort studies found OR estimates ranging from 2 to 3 [26–29] for current smoking compared with non-smoking. A recent study showed an OR estimate of about 1.6, comparing current or recent ex-smokers to non-smokers [30]. Some studies have also found that increasing smoking quantity [26] or duration [27, 31] could increase the risk of liver cancer, while some studies have found that the effects of smoking might be stronger among alcohol users [31]. However, the results on the dose-effect were not consistent [23, 30]. Also, while similar effects of smoking were found in men and women in some studies [28], an association was identified only in elderly women in others [26]. Unfortunately, many reported studies have not been able to sufficiently consider potentially confounding factors such as medical history of diseases and occupational exposures, and only a few studies in the US [28, 31] have examined possible effect modification by other risk factors such as alcohol consumption, hepatitis, or obesity.
The Selected Cancers Study was a large case–control study conducted in US men in which information on smoking and many potential confounders was available. Using the data from this study, we examined the cigarette smoking-liver cancer relationship in US men. In particular, we assessed the smoking-liver cancer relation by smoking quantity and duration, controlling for potential confounders and taking into account effect modification by other risk factors.
Methods
Details of the Selected Cancers Study have been described elsewhere [32]. The cancers investigated in the study included lymphoma, primary liver cancer, nasal cancer, nasopharyngeal cancer, and sarcoma. Men diagnosed with these cancers during 1984–1988 were included if they were 31–59 years old and lived in the areas covered by eight cancer registries in the US. Controls were men who were frequency matched to lymphoma cases by geographic area covered by cancer registry and 5-year date-of-birth intervals, and were selected through random-digit telephone dialing.
A total of 310 men were reported with liver cancer during the study period. Among these patients, 263 were interviewed and 233 had a specimen available for diagnosis. A total of 168 patients were confirmed to have primary liver cancer by a pathology review panel. Of the 168 patients, 123 were “definite” primary liver cancer cases and 45 were “probable” cases. A total of 138 cases had hepatocellular carcinoma and 30 cases had other histologic types. A total of 2,299 men were identified to be eligible as controls through random-digit-dialing, among whom 83.1% completed the interview (n=1910) and were used in the analysis. Informed consent was obtained from each study subject in the original study and the ethical guidelines were conformed.
Surviving cases and controls were interviewed on the phone by trained personnel. In-person interviews were performed only when necessary to ensure subject’s participation (8.3% of cases and 1.9% of controls). About 109 of the cases were deceased at the time of interview. Proxy interviews were done for the deceased cases (64.9%). The information collected primarily included demographic characteristics (date of birth, ethnic background, education level, marital status, religion preference, and family income), relevant medical history (malaria, mononucleosis, systemic lupus erythematosis, allergy, tonsillectomy, appendectomy, immunodeficiency, hepatitis, cirrhosis, multiple sclerosis, chicken pox, arthritis, and so on), occupations (working with or around chemical solvents, wood, asbestos, or dust), exposure to radiation, exposure to pesticides, chemotherapy, personal habits (smoking and alcohol consumption), drug abuse, and military service history.
Logistic regression analysis [33] was used to analyze the relationship between cigarette smoking and primary liver cancer. We first analyzed whether a subject had ever smoked is related to primary liver cancer. In the analysis, matching variables (age and resident area in terms of cancer registry) and the presence of a phone in the home four months prior to interview were always included in the models because of their possible complex effects on study results. Other variables were selected as potential confounders if they were significantly (p < 0.05) associated with the risk of liver cancer in the data or could logically be thought to confound the smoking-liver cancer relationship. We then examined the smoking-liver cancer relationship in terms of current/past smoking status, years for which a subject smoked, packs that a subject smoked per day, and pack-years (daily number of packs of cigarettes smoked multiplied by the number of years the subject smoked). Furthermore, we assessed whether the possible effects of smoking could be modified by age, ethnicity (Asian versus other ethnic groups), alcohol consumption, and history of hepatitis and cirrhosis diagnosed three years prior to the reference date. Since risk factor profiles may differ between different histological types of cancer, we repeated the analyses for hepatocellular carcinoma in order to minimize the potential effects due to the mixture of various histological types. Other histological types were not analyzed because of the small number of cases.
Results
Demographic characteristics of the cases and controls are presented in Table 1. Cases tended to be older. While about 22% and 38% of control men were in the age groups of younger than 40 years and older than 50 years respectively, the corresponding proportions were about 13% and 57% among men with primary liver cancer. The ethnic distributions of the cases and controls were strikingly different, with cases being much less likely to be White (48.2 vs. 81.5%), much more likely to be Asian (25.6 vs. 3.5%) and more likely to be Black (15.5% vs. 7.8%) than controls. While the proportion of never-married men was similar between the two groups, men with liver cancer tended to have a lower education level and annual household income than controls.
The case and control groups also differed with respect to smoking. About 79% of the cases had ever smoked cigarettes regularly while about 67% of the controls had done so. The proportions of ex-smokers and current smokers were 40.6 and 39.4 among cases and 38.5 and 28.2 among controls, respectively.
The results from logistic regression are shown in Table 2 for all liver cancers. After adjustment for potential confounders, cases were about 1.7 times more likely to have regularly smoked cigarettes than controls (95% CI, 0.99–2.82). The corresponding estimates were 1.49 (95% CI, 0.83–2.68) and 1.85 (95% CI, 1.05–3.25) for current smokers and ex-smokers. In terms of dose, there appeared to be a dose-response relationship between liver cancer and quantity smoked with adjusted OR estimates of 0.96, 1.43, 1.80, and 1.87 for smoking less than 15, 15–24, 25–34, and 35 or more years (p for trend = 0.039), respectively, and 1.41, 1.67, and 1.83 for smoking less than one pack, 1–1.9 packs, and 2 or more packs per day (p for trend = 0.068), respectively. When pack-years were used as a measure, the odds ratio estimates were 1.07, 1.51, 1.74, and 1.58 for smoking less than 15, 15–29, 30–44, and 45 or more pack-years (p for trend = 0.101), respectively. The effects of smoking were not significantly modified by age, ethnicity, alcohol consumption, hepatitis diagnosed three years before the reference date, and cirrhosis diagnosed three years prior to the reference date (data not shown).
Table 3 shows the results of the logistic regression limited to the hepatocellular carcinoma cases. The odds ratios for hepatocellular carcinoma in relation to smoking status, number of years, number of packs, and pack-years tended to be lower than those in Table 2.
Discussion
This study found that cigarette smoking might be weakly associated with liver cancer in US men, especially with increasing duration of smoking and probably with increasing number packs smoked. However, the estimates of the association tended to be lower, and the dose-effect relationship tended to be less obvious when the analysis was restricted to hepatocellular carcinoma cases only. This may be related to the sampling variation due to a smaller sample size when hepatocellular carcinoma was analyzed alone. Another possibility is that cigarette smoking might be more of a risk factor for other histologic types of primary liver cancer than for hepatocellular carcinoma.
There are two major concerns in the evaluation of the study findings: the inclusion of some probable (rather than confirmed) liver cancer patients, and the use of some proxy interviews in the case group. If probable cases were not liver cancer patients, an association between cigarette smoking and liver cancer might be under- or over-estimated, depending upon the relation between smoking and the medical conditions that appeared as liver cancer. Since a substantial proportion of cases were deceased at the time of study, and data were therefore collected on them through proxy interviews with next of kin, data quality might differ between cases and controls, biassing the study results. To evaluate the potential impacts of these two factors, we repeated analyses using only confirmed cases and excluding proxy interviews. In these analyses, the directions of the odds ratios remained the same, but none of the confidence intervals excluded unity, primarily because the sample size was smaller. However, almost all odds ratio point estimates tended to be higher when data from proxy interviews were excluded, suggesting that next of kin might underreport smoking habits of the deceased cases. Hence, the association between smoking and primary liver cancer in this study might be somewhat underestimated in the group as a whole.
There was a possibility of residual confounding. In the data analysis, we were unable to control for some risk factors of liver cancer, such as exposure to aflatoxin and family history of primary liver cancer. Lack of adjustment for aflatoxin exposure might not have substantially affected our results, because this factor is less prevalent in the US. Men with Asian background, who were over-represented in the case group, might be exposed to aflatoxin and cigarette smoking to a greater extent than men of other ethnic backgrounds. However, ethnic background was adjusted for in our analyses, thus nullifying this concern. Family history of primary liver cancer may be associated with liver cancer and with smoking. Thus, the possibility of residual confounding by family history of primary liver cancer cannot be excluded. The effective control of the possible confounding effects of family history of liver cancer requires large numbers of liver cancer cases and controls.
Previous studies in the US have been relatively consistent in finding an association between cigarette smoking and primary liver cancer. However, potential confounding was often insufficiently controlled for in these studies, as only demographic variables [26, 27] or a few additional variables (hepatitis/cirrhosis [25, 28], diabetes (28, 30) or alcohol consumption [23, 25, 26, 28, 30, 31]) were considered in them. Our study controlled for additional potential confounders, including medical history of more diseases, occupational exposures and radiation exposure, and this may be partly responsible for our association appearing weaker than those in most previous studies. This may suggest the importance of controlling for potential confounders in discerning the smoking-liver cancer relationship, although the true association in our study might have been stronger if only direct interviews were used for all cases. Our study also examined whether other risk factors might modify the smoking-liver cancer relationship. As suggested in some previous studies [34 , 35], the smoking-liver cancer relationship may differ depending upon other factors such as alcohol consumption and hepatitis. However, we found no effect modification by age, race, alcohol consumption, and histories of hepatitis and cirrhosis. This differs from results from a few US studies which identified effect modification by age [26], alcohol consumption [31], viral hepatitis [28], or obesity [31], but agrees with a few other US studies that did not find effect modification by alcohol consumption [23, 30]. Both men and women were included in some of these studies [26, 28].
Several possibilities may account for a higher risk among former smokers than current smokers in our study. If current smoking cases were less likely to respond to the study compared with current smoking controls, current smokers might be more underrepresented in the case group, leading to a diluted measure of association. On the other hand, a diluted measure of association might also result if current smokers were more likely to smoke filter cigarettes than former smokers and the risk of cancer associated with filter cigarettes is lower than that with nonfilter cigarettes as shown in some studies [36–38]. Also, former smokers might have quit as a result of health problems that might be associated with higher exposure to smoking or decreased resistance to the effects of tobacco. In addition, potential differences between current and former smokers with respect to other risk factors for liver cancer cannot be excluded.
The association between cigarette smoking and liver cancer has been considered as a causal one in a recent publication by the International Agency for Research on Cancer [39] and may be biologically plausible. Liver is a major organ that metabolizes and transforms many chemicals in the body. Tobacco smoke contains more than 40 chemical compounds that are biologically active and often metabolized in the liver [8]. For example, polycyclic aromatic hydrocarbons, nitrosamines and aromatic amines, all of which are carcinogenic [40], are processed by hepatic enzymes [8]. Therefore, the liver may be a target of many chemical materials included in tobacco smoke. Animal experiments have shown that when rodents are exposed to smoke or its components, the occurrence of primary liver cancer increases [41] and that cigarette smoke can enhance the intensity of metabolic activation of the carcinogenic material, 2-amino-3,8-dimethylimidazo [4,5-f] quinoxaline [42]. In human studies, cigarette smoke was related to increasing serum α-1-antitrypsin [43, 44], which is linked to increased risk of heptocellular carcinoma [45, 46]. This may explain the smoking-liver cancer association. Experimental studies have shown that cigarette smoke may modify the risk of hepatocellular carcinoma related to tumor-suppressor gene, such as p53 [47], and increase the expression of oncogenes such as neu [48]. The results of these studies suggest the possibility that cigarette smoking may induce or promote carcinogenic changes of liver cancer. Epidemiological studies with the use of biomarkers are warranted for further clarifying the smoking-liver cancer relationship.
References
London W, McGlynn K (1996) Liver cancer In: Schottenfeld D, Fraumeni J Jr (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 772–793
Bosch FX, Ribes J (2000) Epidemiology of liver cancer in Europe. Can J Gastroenterol 14:621–630
Bosch FX, Ribes J, Cleries R, Diaz M (2005) Epidemiology of hepatocellular carcinoma. Clin Liver Dis 9:191–211, v
Stuver S, Trichopoulos D (2002) Cancer of the liver and biliary tract. In: Adami H, Hunter D, Trichopoulos D (eds) Textbook of cancer epidemiology. Oxford University Press, Inc., New York
Jee SH, Ohrr H, Sull JW, Samet JM (2004) Cigarette smoking, alcohol drinking, hepatitis B, and risk for hepatocellular carcinoma in Korea. J Natl Cancer Inst 96:1851–1856
Yun YH, Jung KW, Bae JM et al (2005) Cigarette smoking and cancer incidence risk in adult men: National Health Insurance Corporation Study. Cancer Detect Prev 29:15–24
Mizoue T, Tokui N, Nishisaka K et al (2000) Prospective study on the relation of cigarette smoking with cancer of the liver and stomach in an endemic region. Int J Epidemiol 29:232–237
Wang LY, You SL, Lu SN et al (2003) Risk of hepatocellular carcinoma and habits of alcohol drinking, betel quid chewing and cigarette smoking: a cohort of 2416 HBsAg-seropositive and 9421 HBsAg-seronegative male residents in Taiwan. Cancer Causes Control 14:241–250
Goodman MT, Moriwaki H, Vaeth M, Akiba S, Hayabuchi H, Mabuchi K (1995) Prospective cohort study of risk factors for primary liver cancer in Hiroshima and Nagasaki, Japan. Epidemiology 6:36–41
Hirayama T (1989) A large-scale cohort study on risk factors for primary liver cancer, with special reference to the role of cigarette smoking. Cancer Chemother Pharmacol 23(Suppl):S114–S117
Tanaka K, Hirohata T, Fukuda K, Shibata A, Tsukuma H, Hiyama T (1995) Risk factors for hepatocellular carcinoma among Japanese women. Cancer Causes Control 6:91–98
Chen CJ, Liang KY, Chang AS et al (1991) Effects of hepatitis B virus, alcohol drinking, cigarette smoking and familial tendency on hepatocellular carcinoma. Hepatology 13:398–406
Tsukuma H, Hiyama T, Oshima A et al (1990) A case–control study of hepatocellular carcinoma in Osaka, Japan. Int J Cancer 45:231–236
Tanaka K, Hirohata T, Takeshita S (1988) Blood transfusion, alcohol consumption, and cigarette smoking in causation of hepatocellular carcinoma: a case–control study in Fukuoka, Japan. Jpn J Cancer Res 79:1075–1082
Mukaiya M, Nishi M, Miyake H, Hirata K (1998) Chronic liver diseases for the risk of hepatocellular carcinoma: a case–control study in Japan. Etiologic association of alcohol consumption, cigarette smoking and the development of chronic liver diseases. Hepatogastroenterology 45:2328–2332
Mori M, Hara M, Wada I et al (2000) Prospective study of hepatitis B and C viral infections, cigarette smoking, alcohol consumption, and other factors associated with hepatocellular carcinoma risk in Japan. Am J Epidemiol 151:131–139
Pyong SJ, Tsukuma H, Hiyama T (1994) Case–control study of hepatocellular carcinoma among Koreans living in Osaka, Japan. Jpn J Cancer Res 85:674–679
Tanaka K, Hirohata T, Takeshita S et al (1992) Hepatitis B virus, cigarette smoking and alcohol consumption in the development of hepatocellular carcinoma: a case–control study in Fukuoka, Japan. Int J Cancer 51:509–514
Choi SY, Kahyo H (1991) Effect of cigarette smoking and alcohol consumption in the aetiology of cancer of the oral cavity, pharynx and larynx. Int J Epidemiol 20:878–885
Shibata A, Fukuda K, Toshima H, Tashiro H, Hirohata T (1990) The role of cigarette smoking and drinking in the development of liver cancer: 28 years of observations on male cohort members in a farming and fishing area. Cancer Detect Prev 14:617–23
Kiyosawa K, Imai H, Sodeyama T et al (1989) Comparison of anamnestic history, alcohol intake and smoking, nutritional status, and liver dysfunction between thorotrast patients who developed primary liver cancer and those who did not. Environ Res 49:166–72
Lu SN, Lin TM, Chen CJ et al (1988) A case–control study of primary hepatocellular carcinoma in Taiwan. Cancer 62:2051–2055
Austin H, Delzell E, Grufferman S et al (1986) A case–control study of hepatocellular carcinoma and the hepatitis B virus, cigarette smoking, and alcohol consumption. Cancer Res 46:962–966
Stemhagen A, Slade J, Altman R, Bill J (1983) Occupational risk factors and liver cancer. A retrospective case–control study of primary liver cancer in New Jersey. Am J Epidemiol 117:443–454
Yu MC, Mack T, Hanisch R, Peters RL, Henderson BE, Pike MC (1983) Hepatitis, alcohol consumption, cigarette smoking, and hepatocellular carcinoma in Los Angeles. Cancer Res 43:6077–6079
Yu H, Harris RE, Kabat GC, Wynder EL (1988) Cigarette smoking, alcohol consumption and primary liver cancer: a case–control study in the USA. Int J Cancer 42:325–328
Hsing AW, McLaughlin JK, Hrubec Z, Blot WJ, Fraumeni JF, Jr (1990) Cigarette smoking and liver cancer among US veterans. Cancer Causes Control 1:217–221
Yu MC, Tong MJ, Govindarajan S, Henderson BE (1991) Nonviral risk factors for hepatocellular carcinoma in a low-risk population, the non-Asians of Los Angeles County, California. J Natl Cancer Inst 83:1820–1826
Birth control pills, cigarettes, alcohol linked to liver cancer. Oncology (Williston Park) (1992) 6:101
Yuan JM, Govindarajan S, Arakawa K, Yu MC (2004) Synergism of alcohol, diabetes, and viral hepatitis on the risk of hepatocellular carcinoma in blacks and whites in the U.S. Cancer 101:1009–1017
Marrero JA, Fontana RJ, Fu S, Conjeevaram HS, Su GL, Lok AS (2005) Alcohol, tobacco and obesity are synergistic risk factors for hepatocellular carcinoma. J Hepatol 42:218–224
The Selected Cancers Cooperative Study Group (1990) The association of selected cancers with service in the US military in Vietnam. III. Hodgkin’s disease, nasal cancer, nasopharyngeal cancer, and primary liver cancer. Arch Intern Med 150:2495–2505
Hosmer D, Jr, Lemeshow S (1989) Applied logistic regression. Jihn Wiley & Sons, New York
Trichopoulos D, MacMahon B, Sparros L, Merikas G (1980) Smoking and hepatitis B-negative primary hepatocellular carcinoma. J Natl Cancer Inst 65:111–114
Kuper H, Tzonou A, Kaklamani E et al (2000) Tobacco smoking, alcohol consumption and their interaction in the causation of hepatocellular carcinoma. Int J Cancer 85:498–502
Lee PN, Sanders E (2004) Does increased cigarette consumption nullify any reduction in lung cancer risk associated with low-tar filter cigarettes? Inhal Toxicol 16:817–833
Marugame T, Sobue T, Nakayama T et al (2004) Filter cigarette smoking and lung cancer risk a hospital-based case–control study in Japan. Br J Cancer 90:646–651
Launoy G, Milan C, Faivre J, Pienkowski P, Gignoux M (2000) Tobacco type and risk of squamous cell cancer of the oesophagus in males: a French multicentre case–control study. Int J Epidemiol 29:36–42
IARC Working Group on the Evaluation of Carcinogenic Risks to Humans (2004). Tobacco smoke and involuntary smoking. IARC Monogr Eval Carcinog Risks Hum 83:1–1438
Baron J, Rohan T (1996) Tobacco. In: Schottenfeld D, Fraumeni J Jr (eds) Cancer epidemiology and prevention. Oxford University Press, New York, pp 269–289
Hecht SS, Chen CB, Ohmori T, Hoffmann D (1980) Comparative carcinogenicity in F344 rats of the tobacco-specific nitrosamines, N′-nitrosonornicotine and 4-(N-methyl-N-nitrosamino)-1-(3-pyridyl)-1-butanone. Cancer Res 40:298–302
Mori Y, Koide A, Kobayashi Y, Furukawa F, Hirose M, Nishikawa A (2003) Effects of cigarette smoke and a heterocyclic amine, MeIQx on cytochrome P-450, mutagenic activation of various carcinogens and glucuronidation in rat liver. Mutagenesis 18:87–93
Petridou E, Chapuis-Cellier C, Roukas K, Lan SJ, Tzonou A, Trichopoulos D (1993) Tobacco smoking and other factors in relation to serum alpha-1-antitrypsin. Hum Biol 65:425–432
Lellouch J, Claude JR, Thevenin M (1979) [Smoking and serum alpha 1-antitrypsin in 1296 healthy men (author’s transl)]. Clin Chim Acta 95:337–345
Sparos L, Tountas Y, Chapuis-Cellier C, Theodoropoulos G, Trichopoulos D (1984) Alpha 1-antitrypsin levels and phenotypes and hepatitis B serology in liver cancer. Br J Cancer 49:567–570
Fargion S, Klasen EC, Lalatta F, Sangalli G, Tommasini M, Fiorelli G (1981) Alpha 1-antitrypsin in patients with hepatocellular carcinoma and chronic active hepatitis. Clin Genet 19:134–139
Yu MW, Yang SY, Chiu YH, Chiang YC, Liaw YF, Chen CJ (1999) A p53 genetic polymorphism as a modulator of hepatocellular carcinoma risk in relation to chronic liver disease, familial tendency, and cigarette smoking in hepatitis B carriers. Hepatology 29:697–702
Yu MW, Chen CJ, Luo JC, Brandt-Rauf PW, Carney WP, Santella RM (1994) Correlations of chronic hepatitis B virus infection and cigarette smoking with elevated expression of neu oncoprotein in the development of hepatocellular carcinoma. Cancer Res 54:5106–5110
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhu, K., Moriarty, C., Caplan, L.S. et al. Cigarette smoking and primary liver cancer: a population-based case–control study in US men. Cancer Causes Control 18, 315–321 (2007). https://doi.org/10.1007/s10552-006-0105-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-006-0105-8