
Abstract
The incidence of breast cancer, as well as other chronic disease, increases with age, older breast cancer patients being more likely than younger to suffer from other diseases at time of diagnosis. Our objective was to assess the effect of comorbidity on mortality after early breast cancer. 62,591 women diagnosed with early breast cancer 1990–2008 were identified using the Danish Breast Cancer Cooperative Group Registry. Data were linked to the Danish National Patient Register and the Danish Register of Causes of Death. Main outcome measures were mortality from all causes, breast cancer, and non-breast cancer causes in relation to Charlson comorbidity index (CCI). Compared with patients without comorbidity (CCI 0), the presence of comorbidity increased the risk of dying from breast cancer as well as other causes with adjusted hazard ratios (HRs) for all-cause mortality of 1.45 (CI 95% 1.40–1.51) for CCI 1, 1.52 (95% CI 1.45–1.60) for CCI 2, and 2.21 (95% CI 2.08–2.35) for CCI 3+. Equivalent HRs for breast cancer-specific mortality were 1.30 (95% CI, 1.24–1.36) for CCI 1, 1.31 (95% CI 1.23–1.39) for CCI 2, and 1.79 (95% CI, 1.66–1.93) for CCI 3+ (all P values < 0.0001). For patients with CCI 0, 5-year overall survival increased over time from 72.5% (95% CI, 71.7–73.3%) in 1990–1994 to 81.6% (95% CI, 80.9–82.2) in 2000–2004, whereas the 5-year overall survival remained stable around 43% among the patients with CCI 3+. This population-based cohort study shows that compared with patients without comorbidity, the risk of dying from breast cancer as well as other causes increased significantly with increasing CCI score. While survival improved over time for patients without comorbidity, no improvement was seen among patients with severe comorbidity (CCI 3+).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the most frequent malignant disease among women with more than a million new cases diagnosed each year worldwide [1]. The incidence of breast cancer, as well as other chronic diseases, increases with age, with older breast cancer patients being more likely than younger to suffer from other diseases at time of diagnosis [2]. Comorbidity can be defined as the presence of one or more chronic health conditions etiologically different from the disease under study, in this case breast cancer [3].
Several studies from Europe and North America have shown that comorbidity increases overall mortality [4]. In 49,616 breast cancer patients aged 67 years or older diagnosed during 1992–2003 identified from the SEER-Medicare database, adjusted hazard ratios (HRs) were 1.3 (95% confidence interval (CI) 1.2–1.4) for death from breast cancer, and 2.6 (95% CI 2.5–2.8) for death from other causes among patients with a Charlson comorbidity index (CCI) score of two or more compared with patients without comorbidity [5]. Similar results were obtained from a Dutch study, including 7,978 breast cancer patients diagnosed during 1995–2001, with HR for overall mortality of 1.4 (95% CI 1.3–1.5) for CCI 2+ [6]. Two prior studies from Denmark have examined the effect of comorbidity on overall mortality, death from breast cancer, and death from other causes. Among 25,897 breast cancer patients diagnosed between 1983 and 1999, adjusted HRs were 1.52 (95% CI 1.25–1.85) for death from breast cancer and 5.77 (95% CI 4.77–6.97) for death from other causes among patients with CCI 2+ compared with those without comorbidity [7]. In a study of 9,300 breast cancer patients from four counties in North Jutland, a trend of increasing overall survival from 1995 to 2006 was found in patients with a CCI less than three, whereas overall survival decreased with time among patients with CCI 3+ [8]. In this article, we update the results on the effect of comorbidity on overall mortality, mortality from breast cancer, and from other causes, with information from the Danish population of patients with early-stage breast cancer diagnosed between 1990 and 2008.
Materials and methods
Data collection and study factors
We performed a population-based cohort study by linking the following Danish registries using the unique personal identification number: the Danish Breast Cancer Cooperative Group (DBCG) Registry, the Danish National Patient Register (NPR), the Central Population Registry (CPR), and the Danish Register of Causes of Death (RCD). The study population included 62,591 women diagnosed with early breast cancer in Denmark during 1990–2008.
Since 1977, the multidisciplinary DBCG has provided diagnostic and therapeutic procedures and successive treatment guidelines in primary invasive breast cancer on a nationwide basis in Denmark. Diagnostic, therapeutic, and follow-up data have been collected prospectively in the DBCG Registry by the use of standardized forms. Clinical follow-up data including adjuvant treatment are limited to 10 years after diagnosis and restricted to patients enrolled in a protocolled treatment program, but using the same procedure for all patients regardless of whether the patient participated in a randomized trial [9]. Almost complete follow-up for all patients concerning vital state are achieved through linkage to the CPR. Completeness of data in the DBCG has been validated by linkage to the Danish Cancer Registry and the National Pathology Registry showing high agreement with data concerning adjuvant treatment, and the result on type of first event and time to first event. An age limit of 74 years in treatment guidelines persisted until 2002 resulting in lack of information on adjuvant treatment of women 75 years or older before the year 2002 [9]. Information on comorbidity was obtained for each woman in the study cohort by linkage to the NPR which has collected data on all somatic hospital admissions since 1977 and data on outpatients and emergency patients since 1995. NPR includes, on an individual level, information from all hospitalizations, including dates of admission and discharge and up to 20 discharge diagnoses per hospitalization. The NPR covers the entire nation, and routine collection of data according to procedures prescribed by the Danish National Board of Health does support standardization and good quality of data. The Danish population is very homogeneous with regard to race and religion and stable; so loss to follow-up due to migration is a minor problem since the CPR and the unique person identification are both very accurate [10]. Several studies have validated selected discharge diagnoses in the NPR and showed that it had a moderate-to-high predictive value for epilepsy and that it is a valuable tool for epidemiologic research in regard to other diagnoses [11–13]. Comorbidity was measured using the CCI [14] developed to predict 1-year mortality in medical inpatients and subsequently validated among breast cancer patients, and against other comorbidity indices [15, 16]. The CCI provides an overall score for comorbidity based on composite values weighted by level of severity assigned to 19 selected conditions scoring for 1–6 and the score was grouped as 0, 1, 2, or 3+. The CCI in the present study was based on hospital contacts with diagnoses other than breast cancer from 10 years before the breast cancer diagnosis up to the breast cancer diagnosis. Diagnoses of other malignancies in the two months period preceding the breast cancer diagnoses were excluded.
Information on vital status and migration was obtained from the CPR and, for those who had died, we obtained causes of death from the RCD, which holds information from death certificates. Causes of death were classified as death due to breast cancer or to other (non-breast cancer) causes.
Statistical analysis
Associations between CCI score and other characteristics were analyzed by Chi-square tests. Follow-up was calculated as median-estimated potential follow-up [17].
Overall survival was calculated as the time from date of surgery until death, irrespective of cause of death, or end of follow-up (December 31, 2008), estimated using the Kaplan–Meier method.
Cumulative incidences in the presence of competing risk were estimated for the risk of recurrence, the risk of death from breast cancer, and the risk of death from other causes, as first event, taking into account contra-lateral invasive breast cancer and second primary non-breast cancer as competing risks [18, 19]. Analysis included the patients included in the DBCG treatment protocol.
The Cox proportional hazards regression model [20] was used to assess the adjusted influence of CCI, with CCI score 0 as reference, on overall, breast cancer-specific, and non-breast cancer survivals with time since diagnosis as the underlying time scale. Adjustment factors were age, menopausal status, tumor size, nodal status, deep fascia invasion, vascular invasion, histological type and grade, hormone receptor status, year at diagnosis, type of surgery, and allocated adjuvant treatment. The assumptions of proportional hazards were assessed by Schoenfeld residuals. The hazard rates of histological type and grade as well as hormone receptor status were not proportional, and therefore stratification was used. Interaction between CCI score and year of diagnosis was investigated in the multivariate Cox model using the Wald test. All P values are two-sided. Statistical analyses were performed with the SAS v9.1 statistical software (SAS Institute, Inc., Cary, NC).
Results
The proportion of breast cancer patients with CCI score 1 or more increased significantly with calendar time (P < 0.0001) from 14% during 1990–1993 to 26% during 2006–2008, and with age at diagnosis (P < 0.0001) (Table 1). Among patients aged 60 or more years, almost a third (29%) had one, or more comorbid conditions. In a stratified analysis of calendar time and age, there was a significant trend of increasing comorbidity with calendar time in all age groups, e.g., in women aged 40–49, CCI 3+ increased from 0.4% during 1990–1993 to 2.0% during 2006–2008, and in women aged 70–79, CCI 3+ increased from 3.2% during 1990–1993 to 8.7% during 2006–2008.
Comorbidity score was associated with the primary treatment of breast cancer (Table 2). Surgery was limited to a biopsy only in 15% of patients with CCI 3+ compared with 4% of patients with CCI 0, while indications for radiotherapy did not vary across CCI. Information on medical adjuvant treatment was lacking for a substantial proportion of the cohort (28%) and for more than 50% of patients with CCI 2 or more.
Tumor characteristics were not available for 3,057 patients who had biopsy only, leaving a total of 59,534 with known tumor characteristics (Table 3). Patients with a CCI 3+ had fewer lymph nodes removed, but more lymph node metastases. Apart from this, no major differences were observed in tumor size, estrogen receptor (ER) status, histological type, and grade, or fascia invasion according to comorbidity score.
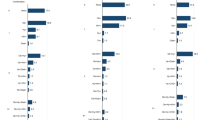
With a median-estimated potential follow-up of 8.2 years, a total of 22,282 (36%) breast cancer patients had died, 16,316 classified as deaths from breast cancer, and 5,966 as deaths from other causes. Time to first event, either recurrence of breast cancer, or death due to breast cancer, or death due to other causes, was analyzed in a competing risk setting among 45,253 patients receiving treatment according to protocol (Fig. 1). The risk of recurrence decreased with increasing CCI, the 10-year estimates being 22.5% for CCI 0, 18.8% for CCI 1, 16.0% for CCI 2, and 11.7% for CCI 3+, whereas the risk of breast cancer death as a first event increased significantly with increasing CCI score, with 10-year cumulative incidences of 5.4% for CCI 0 increasing to 21.7% for CCI 3+. Similarly, increasing cumulative incidence of death due to other causes as a first event was seen with increasing CCI score (10.0, 15.2, and 27.9% for CCI score 1, 2, and 3+, respectively), whereas the cumulative incidence was low for patients with CCI score 0 with a 10-year cumulative incidence of 2.6% (Fig. 1).

Cumulative incidence of first event for either recurrence of breast cancer, death due to breast cancer, or death due to other causes in the presence of competing risk including 45,253 women enrolled in protocolled treatment programs
In a multivariate analysis with adjustment for known prognostic factors, comorbidity had an independent prognostic effect on the risk of dying from breast cancer as well as from other causes (Table 4). Compared with patients without comorbidity (CCI 0), presence of comorbidity increased the risk of dying with adjusted HRs for all-cause mortality of 1.45 (CI 95% 1.40–1.51) for CCI 1, 1.52 (95% CI 1.45–1.60) for CCI 2, and 2.21 (95% CI 2.08–2.35) for CCI 3+. Equivalent HRs for breast cancer-specific mortality was 1.30 (95% CI, 1.24–1.36) for CCI 1, 1.31 (95% CI 1.23–1.39) for CCI 2, and 1.79 for CCI 3+ (95% CI, 1.66–1.93) (all P values < 0.0001).
Overall survival decreased significantly with increasing CCI score (Table 5). For patients with CCI 0, 5-year overall survival increased from 72.5% (95% CI, 71.7–73.3%) in 1990–1994 to 81.6% (95% CI, 80.9–82.2) in 2000–2004, whereas the overall survival remained stable around 43% among patients with CCI 3+, showing no improvement in survival over time for patients with CCI 3+. The interaction between year of diagnosis and CCI score was tested in the multivariate Cox model confirming (P = 0.01, data not shown).
Discussion
This population-based cohort study, using information from the national registries, of women in Denmark diagnosed with breast cancer in the period 1990–2008, shows that an increasing proportion of breast cancer patients suffer from comorbidity at diagnosis and that such comorbidity affects survival in terms of breast cancer-specific mortality, non-breast cancer mortality, as well as all-cause mortality. Even mild comorbidity (CCI 1) increased the risk of dying from breast cancer by 30%.
In the early 1990s, comorbidity was not that frequent (14%) but increased over time to being present in about a quarter of all patients (26%) by the end of 2008. It is possible that part of this increase can be explained by the addition of outpatients and emergency patient visits in the NPR. Although the prevalence of comorbidity increased with age, and more than half of the patients being 60 years or older, the trend with calendar time was seen in all age groups. This finding is new as we are not aware of other studies reporting similar findings.
Comorbidity affected the likelihood of proper breast cancer surgery, patients with high comorbidity scores being more likely to undergo biopsy only. One explanation may be contraindications for general anesthesia. Among those with proper surgery, the frequency of mastectomies was higher in patients with CCI 3+, probably due to age since number of comorbidities increase with age. Other studies have reported that comorbidity did not affect choice of surgery when contraindications were not present [21, 22]. However, patients with high comorbidity had fewer lymph nodes removed indicating less extensive surgery in the axilla. Louwman et al. [23] reported that axillary dissection in relation to breast conserving surgery decreased from 97 to 78% in patients having none or more than one comorbid conditions, respectively, and the frequency decreased further with patient age [23]. Similarly, other studies have shown that older women with comorbidity were more likely to receive non-standard primary therapy [21, 24].
Owing to missing information, the analysis of adjuvant medical treatment and CCI becomes more complex because of a connection between CCI 0 and patients treated in DBCG protocols. This needs to be analyzed separately in a future study. In a recent review, the majority of studies reported decreased use of chemotherapy (CT) and inferior survival for patients with comorbidity compared to those without [25]. The likelihood of receiving CT was greater among women who were younger, white, had lower comorbidity score, more advanced disease and were ER-negative [26].
The observed increase in overall survival for patients with a CCI less than 3 is likely to be due to a continuous improvement of treatment. Population-based mammography screening was introduced in Denmark in 2007 and cannot explain the improved prognosis. For patients with a CCI score of 3 or more, though, there was no change in overall survival from 1990 to 2008 indicating that patients with severe comorbidity did not benefit from the improved treatment observed for other breast cancer patients. These findings confirm the results of an earlier Danish study based on a subset of the population [8].
Other studies have shown that breast cancer patients who receive less than standard care are at excess risk for disease recurrence and mortality [27, 28]. In our competing risk analysis, the risk of a recurrence decreased with increasing comorbidity probably because patients with a high CCI were more likely to die either from breast cancer or other causes before they developed a recurrence. Within 10 years, almost a third of breast cancer patients with CCI 3+ had died of causes other than breast cancer. When we adjusted for the effects of other prognostic factors in a multivariate analysis, comorbidity had an independent prognostic effect on breast cancer mortality as well as non-breast mortality. Several other registry-based retrospective studies have shown that comorbidity is associated with increased HRs for death of all causes when adjusting for age and stage [6, 22, 23]. With respect to breast cancer-specific mortality, our results confirm those obtained by Schonberg et al. [5] in patients aged 67 [5] or older and Dalton et al. [7] among patients aged less than 70 years of an increased risk of breast cancer-specific mortality with increasing comorbidity.
This raises some intriguing questions in relation to choice of breast cancer treatment in patients with severe comorbidity. On the one hand, their risk of dying from breast cancer is high if they do not receive guideline treatment, but on the other hand, they may not live sufficiently long because of their comorbidity to benefit from the treatment.
This study has several strengths. It has a considerable size, including more than 60,000 breast cancer patients. It is based on the entire Danish population with complete follow-up for vital status and causes of death. It covers a recent time period, 1990–2008, making the results relevant for the patients we treat today. We were able to include detailed information on patient and disease characteristics, and the information on comorbidity derived from national registries with complete registration of hospitalizations and causes of death. The CCI has been widely used and validated in a cohort of breast cancer patients, as well as against other comorbidity measures. It is a simple, valid, and highly suitable method for measuring comorbidity that can be used in clinical research when mortality is the outcome of interest, but may under-detect significant problems resulting in non-lethal endpoints, making our results comparable to those of other studies [29, 30].
However, this study has limitations too. The DBCG does not hold information on medical adjuvant treatment among patients who were not included into treatment protocols according to national treatment guidelines provided by the DBCG [9]. This could for example be related to the presence of comorbidity which can be a contraindication for protocol treatment, as well as age, with patient being 75 years or older not included in treatment guidelines until 2002. The breast cancer patients are followed for 10 years, limiting the analysis of first events such as recurrence to the first 10 years after diagnosis. Using the NPR could give rise to non-differential misclassification if the discharge diagnoses had not been registered correctly. The NPR does not include information on comorbidity that did not require hospital admission, and conditions treated solely by general practitioners are not included. However, the disorders included in the CCI are generally of such a serious nature, that most would at some point in the 10-year period before the breast cancer diagnosis lead to hospitalization or outpatient contact. Using registry-based information to categorize comorbidity according to the CCI does not take into account the significance of specific combinations of comorbid conditions, and it does not incorporate functional status and the relative severity of conditions leading to possible over- or underestimation of comorbidity [29, 30]. A risk of differential misclassification, when retrieving causes of death from the RCD could occur. With a possible tendency to state breast cancer as cause of death when a patient is having that diagnose in the medical chart, especially when death is close to the cancer diagnosis. Finally, we were not able to adjust for lifestyle factors such as obesity, alcohol consumption, and use of estrogen supplement which have been shown to affect breast cancer prognosis [31, 32].
The results of this study demonstrate a need for further research into the effects of breast cancer treatment in women with comorbidity.
Conclusion
Comorbidity is an increasing problem with a quarter of all women diagnosed with breast cancer suffering from one or more comorbidities. Overall survival did not improve over time for those having severe comorbidity as opposed to patients with no comorbidity. When adjusting for other known prognostic factors, comorbidity had an independent prognostic effect on breast cancer-specific mortality as well as non-breast cancer mortality.
Abbreviations
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- CCI:
-
The Charlson comorbidity index
- DBCG:
-
The Danish Breast Cancer Cooperative Group
- RCD:
-
The Danish Registers of Causes of Death
- CPR:
-
The Central Population Registry
- ER:
-
Estrogen receptor
- CT:
-
Chemotherapy
- E:
-
Endocrine therapy
References
Hawfield A, Lovato J, Covington D, Kimmick G (2006) Retrospective study of the effect of comorbidity on use of adjuvant chemotherapy in older women with breast cancer in a tertiary care setting. Crit Rev Oncol Hematol 59:250–255
Newschaffer CJ, Bush TL, Penberthy LT (1997) Comorbidity measurement in elderly female breast cancer patients with administrative and medical records data. J Clin Epidemiol 50:725–733
Land LH, Dalton SO, Jørgensen TL, Ewertz M (2011) Comorbidity and survival after early breast cancer. A review. Crit Rev Oncol/Hematol. doi:10.1016/j.critrevonc.2011.03.001
Schonberg M, Marcantonio E, Silliman RA, Ngo L, McCarthy EP (2010) Breast cancer among the oldest old: tumor characteristics, treatment choices and survival. J.Clin Oncol 28(12):2038–2045
Janssen-Heijnen MLG, Houterman S, Lemmens VEPP, Louwman MWJ, Maas HAAM, Coebergh JW (2005) Prognostic impact of increasing age and co-morbidity in cancer patients: A population-based approach. Crit Rev Oncol Hematol 55:231–240
Dalton SO, Ross L, During M, Carlsen K, Mortensen PB, Lynch J, Johansen C (2007) Influence of socioeconomic factors on survival after breast cancer–a nationwide cohort study of women diagnosed with breast cancer in Denmark 1983–1999. Int J Cancer 121:2524–2531
Cronin-Fenton DP, Norgaard M, Jacobsen J, Garne JP, Ewertz M, Lash TL, Sorensen HT (2007) Comorbidity and survival of Danish breast cancer patients from 1995 to 2005. Br J Cancer 96:1462–1468
Møller S, Jensen MB, Ejlertsen B, Bjerre KD, Larsen M, Hansen HB, Christiansen P, Mouridsen HT (2008) The clinical database and the treatment guidelines of the Danish Breast Cancer Cooperative Group (DBCG); its 30-years experience and future promise. Acta Oncol 47:506–524
Andersen TF, Madsen M, Olsen JH (1999) The Danish National Hospital Register; Dan. Med. Bull., pp 263–268
Christensen J, Vestergaard M, Olsen J, Sidenius P (2007) Validation of epilepsy diagnoses in the Danish National Hospital Register. Epilepsy Res 75:162–170
Vestergaard M, Obel C, Henriksen TB, Christensen J, Madsen KM, Østergaard JR, Olsen J (2006) The Danish National Hospital Register is a valuable study base for epidemiologic research in febrile seizures. J Clin Epidemiol 59:61–66
Moth G, Vedsted P, Schiøtz PO (2007) National registry diagnoses agree with medical records on hospitalized asthmatic children. Acta Paediatr 96:1470–1473
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Klabunde CN, Legler JM, Warren JL, Baldwin LM, Schrag D (2007) A refined comorbidity measurement algorithm for claims-based studies of breast, prostate, colorectal, and lung cancer patients. Ann Epidemiol 17:584–590
Extermann M (2000) Measurement and impact of comorbidity in older cancer patients. Crit Rev Oncol Hematol 35:181–200
Schemper M, Smith TL (1996) A note on quantifying follow-up in studies of failure time. Control Clin Trials 17:343–346
Gray RJ (1988) A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann Stat 16:1141–1154
Gooley TA, Leisenring W, Storer BE (1999) Estimation of failure probabilities in the presence of competing risks. Stat Med 18:695–706
Cox RD (1972) Regression models and life-tables (with discussion). J Roy Stat Soc 34:187–220
Yancik R, Wesley MN, Ries LAG, Havlik RJ, Edwards BK, Yates JW (2001) Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. JAMA 285:885–892
Houterman S, Janssen-heijnen M, Verheij C, Louwman W, Vreugdenhil G, Sangen MVD, Coebergh J (2004) Comorbidity has negligible impact on treatment and complications but influences survival in breast cancer patients. Br J Cancer 90:2332–2337
Louwman WJ, Janssen-Heijnen MLG, Houterman S, Voogd AC, van der Sangen MJC, Nieuwenhuijzen GAP, Coebergh JWW (2005) Less extensive treatment and inferior prognosis for breast cancer patient with comorbidity: A population-based study. Eur J Cancer 41:779–785
Enger SM, Thwin SS, Silliman RA (2011) Breast cancer treatment of older women in integrated health care settings. J Clin Oncol 24:4377–4383
Lee L, Cheung WY, Atkinson E, Krzyzanowska MK (2011) Impact of comorbidity on chemotherapy use and outcome in solid tumors: A Systematic Review. J Clin Oncol 29(1):106–117
Giordano SH, Duan Z, Kuo YF, Hortobagyi GN, Goodwin JS (2006) Use and outcomes of adjuvant chemotherapy in older women with breast cancer. J Clin Oncol 24:2750–2756
Lash TL, Silliman RA, Guadagnoli E, Mor V (2000) The effect of less than definitive care on breast carcinoma recurrence and mortality. Cancer 89:1739–1747
Bouchardy C, Rapiti E, Blagojevic S, Vlastos AT, Vlastos G (2007) Older female cancer patients: importance, causes, and consequences of undertreatment. J Clin Oncol 25:1858–1869
de Groot V, Beckerman H, Lankhorst GJ, Bouter LM (2003) How to measure comorbidity: a critical review of available methods. J Clin Epidemiol 56:221–229
Extermann M (2000) Measuring comorbidity in older cancer patients. Eur J Cancer 36:453–471
Ewertz M, Jensen M, Cold S (2011) Effect of obesity on prognosis after early-stage breast cancer. J Clin Oncol 29(1):25–31
Larsen SB, Olsen A, Lynch J, Dalton SO (2011) Socioeconomic position and lifestyle in relation to breast cancer incidence among postmenopausal women: A prospective cohort study, Denmark, 1993–2006. doi:10.1016/j.canep.2010.12.05
Acknowledgments
The present study was supported by a grant from the Danish Cancer Society.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Land, L.H., Dalton, S.O., Jensen, MB. et al. Impact of comorbidity on mortality: a cohort study of 62,591 Danish women diagnosed with early breast cancer, 1990–2008. Breast Cancer Res Treat 131, 1013–1020 (2012). https://doi.org/10.1007/s10549-011-1819-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-011-1819-1