
Abstract
House dust mites (HDMs) are extensively reported as potent allergens worldwide with India being in the top row. HDM sensitization is hugely reported from India and has led to the concern of implementing proper guidelines for treatment of the sufferers. Climatic conditions and a rapid shift of life style toward a more indoor and urbanised pattern are denoted as the probable causes of increased HDM exposure and sensitization. On the contrary, the varying rate of HDM allergy from similar climate and urbanised areas throughout the world suggest the influence of genetic predisposition. At present, in India, avoidance of HDM exposure is recommended as the baseline defence. Allergen immunotherapy (AIT) guidelines are proposed in India to maintain uniformity in the diagnosis techniques and management strategies throughout the country. Considering the genetic susceptibility toward allergic diseases, the concept of ‘personalised medicine’ is preferred over the ‘mass targeted treatment’. From the Indian perspective, the present problem is Dermatophagoides pteronyssinus and D. farinae allergens are not well characterised at the molecular level. As a consequence, India is still reliant on less standardised allergen extracts. The proper identification, purification, and molecular characterization of HDM allergens can combat this problem. In this review, we aimed to portray a complete account of HDM allergy in India with respect to prevalence, probable triggers, diagnosis and therapy. We have attempted to present the current ambiguities along with the likely deciphering that would pave the way to solve HDM allergy-related queries in India.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Allergic diseases are developing as one of the major health issues in India (Singh and Kumar 2002, 2003). Approximately 25% of the Indian population is sensitized with diverse forms of allergen sources such as pollen grains, fungal spores, foods, insects and house dust mites (HDMs) (Singh and Shahi 2008; Dey et al. 2014, 2016, 2018a; Bhattacharya et al. 2018). HDMs are globally ubiquitous in human habitats and act as one of the most important source of indoor allergens (Sporik and Platts-Mills 1992; Wong et al. 2011; Dutta et al. 2017). Contact to HDM allergens may be increasing due to spending more time in the indoor environment of air conditioned home that led to reduced ventilation. Foam mattresses and carpets provide ideal habitat for the dust mites (Squillace et al. 1997; Ring 1997; Downs et al. 2001). Mite allergens can provoke symptoms by direct external contact (conjunctivitis, eczema), inhalation (rhinitis, asthma, eczema) and ingestion (urticaria, anaphylaxis) in a sensitized person (Mondal et al. 2018; Ghosh et al. 2018). Among the HDMs, members of the family Pyroglyphidae are established as the potential source of allergens that play a significant role in various allergic disorders including bronchial asthma (Podder et al. 2010). Dermatophagoides pteronyssinus (Dp) and Dermatophagoides farinae (Df) are the two pyrogliphid HDM species mostly linked to allergic diseases. Like other aeroallergens, the rate of sensitization toward HDMs varies significantly between countries, regions and even individual test centres (Calderón et al. 2015). According to a study by The Global Asthma and Allergy European Network (GA2 LEN) Dp and Df sensitisation rates were 31.3 and 28.9%, respectively, across 14 European countries (Heinzerling et al. 2009). Sensitization rates to HDM were the highest in Nordic and Mediterranean countries; specifically, sensitization to both Dp (Der p) and Df (Der f) was most prominent in Portugal (Der p: 68.8%; Der f: 68.0%) and Denmark (Der p: 51.5%; Der f: 51.8%) (Heinzerling et al. 2009). Allergy skin tests administered in the second and third National Health and Nutrition Examination Surveys (NHANES II and III) conducted in USA revealed 27.5% sensitization rate for dust mite (Arbes et al. 2005). In Latin American countries, sensitization to Dp varied from 60.7% in Cartagena (Colombia) to 91.2% in Sao Paulo (Brazil); to Df from 53.3% in Córdoba (Argentina) to 97.2% in Caracas (Venezuela); to Blomia tropicalis (Bt) from 46.5% in Mexico City (Mexico) to 93.7% in Sao Paulo (Fernández-Caldas et al. 1993). From Africa, 48 and < 60% HDM sensitivity are reported for Nigeria and Ghana, respectively, and Dp is the major reported allergen (Tham et al. 2016; Addo-Yobo et al. 2001). HDM sensitisation in childhood has also been reported from Australia and New Zealand (Sears et al. 1993; Peat et al. 1996). The overall burden of dust mite sensitization in Asia is much higher than that seen in USA and Europe, even in areas of similar climate and/or urbanization, which raises the question as to whether other factors such as genetics may play a role (Tham et al. 2016). From the Asian countries, dominance of Dp from Hong Kong (Leung et al. 2002), Malaysia (Yadav and Naidu 2015); Dp and Df from Korea (Kim et al. 2010) and Japan (Shirai et al. 2012) are mentioned to show significant sensitization rates. Dp, Df and Bt sensitization are reported from China (Zhang et al. 2012), Singapore (Kidon et al. 2005; Andiappan et al. 2014), Philippines (Albano and Ramos 2011), Taiwan (Wan et al. 2010), Vietnam (Lam et al. 2014), Pakistan (Shafique et al. 2018) and India (Tandon et al. 1988; Saha et al. 1989; Podder et al. 2006, 2010; Mondal et al. 2018).
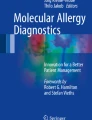
Dust mites are cosmopolitan in distribution throughout India and HDMs are reported to be the dominant allergens to cause nasobronchial allergies (Podder et al. 2009; Ghosh et al. 2018). Ample report on the present situation of HDM allergy is not yet abundant in the Indian context. A complete scenario from the impact of HDM allergy in the Indian population to the diagnosis and therapy of the patients would be beneficial for the future of allergy treatment. This review discusses the prevalence, risk factors, possible therapeutic aspects and perspectives for therapy in India through an extensive survey of HDM allergy-related published literature. The schematic workflow followed for this review is presented through Fig. 1.

Schematic workflow followed in this review article. HDM house dust mite, Dp Dermatophagoides pteronyssinus, Df Dermatophagoides farinae, Bt Blomia tropicalis, IgE immunoglobulin E, SPT skin prick test
Reports on the diversity of the domestic mites in India
Mite concentration and diversity present in the dust samples of patients’ houses are found to vary in different indoor environments (Sharma et al. 2011; Gill and Kaur 2014; Chaudhury et al. 2005). The possible reason for this could be the difference in the structure and materials of the buildings, socioeconomic status of the individuals, type of mattresses used, hygiene standard, and difference in the microclimatic conditions that contributes to the higher accumulation of mites in the house dust (Modak et al. 1991, 2004). In a survey of homes with dust mites, 60% of the dust mite population is reported from the bed, mattresses and pillows, 30% in upholstery and 10% in carpet (Sharma et al. 2011).
Previous studies suggested that the number of allergenic mites in the bed and floor dust of the patients is well correlated with intensity of the skin test reactions (Spieksma and Spieksma-Boezeman 1967). Allergen load of mites in the dust samples were found directly proportional to the severity of allergic attack in some of the typical cases. From India, Dp and Df were found to dominate in the house dust collected from patient homes (Mondal et al. 2018) and these two mites possess significant skin test reactions in the sensitized persons (Mondal et al. 2018).
India tops the list of the highest recorded HDM diversity with 12 species (Colloff 2009). Shivpuri and co-workers were the first Indian acarologists to conduct extensive and intensive studies on mites and recorded that mites could grow well in house dust at 25 °C temperature and 80% relative humidity (Shivpuri 1962, 1977; Shivpuri and Dua 1974). Since then several authors from different parts of the country reported the dominance of Dp over Df (Dixit and Mehta 1973; Nayar et al. 1974; Krishna Rao et al. 1981; Maurya et al. 1983). In contrast, Sharma et al. (2011) and Maurya and Jamil (1980) reported the predominance of Df from other parts of the country. Other domestic mites namely Bt, Acarus siro (AS), Lepidoglyphus destructor (LD), and Tyrophagus putrescentiae (TP) have been reported from different parts of India (Mondal et al. 2018). Table 1 portrays the distribution of the domestic mites from India having skin sensitization potential.
Prevalence of HDM sensitisation in India through skin prick test (SPT)
Skin prick testing is the standard for diagnosing immunoglobulin E (IgE)-mediated allergies. However, different allergen extracts and different testing procedures have been applied by different allergy centres. Thus, it has been difficult to compare results from different centres or studies across the country. It was, therefore, crucial to standardize and harmonize procedures in allergy diagnosis and treatment within India.
A multifaceted pattern of HDM sensitization was seen in various parts of India. Figure 2 represents the states and major cities of India where positive HDM sensitization is reported and details of the publications are depicted in Table 2.

Map of India indicating the regions of reported house dust mite sensitization
HDM prevalence study was done in Delhi and Allahabad during 2008–2011. SPT was performed on a total of 918 patients [548 (59.7%) males and 370 (40.3%) females] for 58 types of aeroallergens. HDM sensitivity was found in 12.4% of patients (Kumar et al. 2012). Another 8 year retrospective study (2008–2016) was carried out among 4835 patients from Delhi (Kumar et al. 2017). SPT was performed on 4263 patients consisting of 2361 (55.4%) males and 1902 (44.6%) females and this revealed 12.0% to be affected with HDM. Another aeroallergen sensitization study of childhood asthmatics was done in Allahabad city (Raj et al. 2013). 180 children above 5 years of age exhibited 7.8% sensitivity to HDM allergens. A group of 60 patients with united airway disease (UAD) from Allahabad was tested with 60 different allergens with SPT during August 2010 to July 2011 (Mishra et al. 2016); 60% was found to be SPT positive with Df extracts.
In 2011, a HDM sensitization study depicted 52.5 and 46.0% SPT reactivity for Dp and Df, respectively. This study was performed on 139 BA patients in the Bangalore region. Another Bangalore-based study (2014) involving 486 AR patients revealed HDM as the most common allergen, with positive results in 44.7% of cases (Gowda et al. 2014). From Andhra Pradesh, 73.7% HDM sensitivity was reported among 331 nasobronchial allergic patients (Lal et al. 2011). In 2012–2013, a hospital-based study was done in Central Kerala consisting of 139 patients from five districts, namely Alappuzha, Idukki, Ernakulam, Kottayam and Thrissur (Kunoor et al. 2017); 23% HDM sensitivity was reported among asthma and AR patients. In the city of Mumbai, a SPT-based investigation was performed to identify HDM sensitivity in children with allergic rhinitis, allergic wheezing and eczema. In total 92 children underwent an SPT; 49 (53.2%) showed significant positivity to one or more dust mite (Doshi and Tripathi 2016). This study revealed Dp, Df and Bt to be the most sensitised aeroallergen eliciting 65.3, 46.9 and 12.2% SPT in children, respectively.
Aeroallergen sensitivity was studied in 1050 AR patients from Udaipur during 2002–2016, and 44.2% was reported to be Df-sensitive through intradermal allergy testing (Matta et al. 2017). West Bengal, especially the city of Kolkata, is one of the most explored areas of India with respect to aeroallergen sensitization. Saha et al. (1989) probably started the evaluation of HDM sensitization in Kolkata population using SPT. Among 188 asthmatic patients, 82% reacted to Dermatophagoides mites, 80% to Df, 46% to Dp, and 43% to both species of mites. Another RAST (radioallergosorbent test)-based study reported 73 and 90% sensitivity toward Dp and Df, respectively, among urban and rural asthmatics of West Bengal (Saha 1993). In 2010, a Kolkata-based study reported Dp (75.1%), Df (63.7%) and Bt (72%) sensitivity, and Bt was reported first time from Kolkata (Podder et al. 2010).
A recent retrospective study from June 2016 to May 2018 revealed 80.3 and 84.9% sensitivity for Dp and Df, respectively, from West Bengal (Dey et al. 2018b). Three new storage mites, namely Acarus siro (AS), Lepidoglyphus destructor (LD), and Tyrophagus putrescentiae (TP), were described for the first time in Kolkata (Mondal et al. 2018). These three mites caused 33.0, 25.2 and 18.8% sensitization in Kolkata population, respectively. The same population were also sensitised for Dp, Df and Bt with sensitization rate of 81.2, 87.9 and 74.2%, respectively. A Bhopal-based study reported 74.2% sensitization for Df among 89 patients with UAD investigated during April 2013 to March 2014, with 120 different allergen extracts (Dave and Srivastava 2014). Nagpur revealed 56.6% Dp sensitization among 143 patients of AR and BA (Arbat et al. 2016). Apart from Dp and Df (49%), Blomia sp. (50.4%) showed significant SPT among the patients. Although most of the patients are from Nagpur and adjacent districts of Maharashtra, 46% were from Madhya Pradesh. Another multicentre study was undertaken to evaluate the allergen patterns in patients with severe persistent allergic rhinitis from Central India. The study group comprised 810 persons (male and female) of the age group between 6 to 63 years. Df showed 18% sensitivity (Jain and Gupta 2018).
Human genetic predisposition of HDM sensitization—recent advances in India
The impact of genetic predisposition in the allergic diseases has become an inevitable question since the same level of exposure to different individuals led to different grades of hypersensitivity or no hypersensitivity at all. Thus the susceptibility to allergies, including dust mite, substantially varies from individual to individual and genome analysis is required to answer the causes to some extent. Next generation sequencing (NGS) has taken our understanding of human genetics to the next level. Single nucleotide polymorphisms (SNPs) analyses have facilitated the selection of novel and interesting candidate genes. Extensive analysis in this regard has suggested genetic heterogeneity triggering allergic phenotypes. Genes opposing and favouring the risk of developing allergies are inherited according to the Mendelian inheritance pattern and environmental triggers interplay a pivotal role in the gene expression (Patel and Meher 2016). Genes coding for cytokines, major histocompatibility complex (MHC) IgE, stem cell factors and insulin growth factors are reported for allergic manifestations. Gene polymorphisms of the beta-adrenergic receptor, 5-lipoxygenase has also been associated to allergy risks (Borish 1999).
Apart from the identification of offending allergens, early detection of genetically predisposed individuals is also crucial for better management of the disease. Some candidate genes have been identified through genome-wide searches for candidate loci regulating atopic responses. Among these, CD14 is the most important gene reported regarding the HDM allergic responses (Vercelli et al. 2001). Tan et al. (2006) also reported the association of genetic polymorphism of CD14 gene with disease development and severity in a HDM-sensitive Chinese paediatric population. Similar study on CD14 in an Indian population revealed a significant difference in the distribution of alleles and genotypes for CD14 polymorphism with an increase in disease severity (Ghosh et al. 2018).
Potential therapeutic strategies proposed in India for HDM sensitised patients
Allergen immunotherapy (AIT) refers to an immunomodulatory method for the treatment of IgE-mediated allergic diseases. Sequentially increasing dose of antigen(s) is implied to induce a shift of the immunological response from TH2 to TH1 that is expected to decrease the sensitivity toward the offending allergens (Moingeon and Mascarell 2012). Guidelines for AIT are already available in Western countries, but a separate guideline for India is also necessitated due to a multitude of factors. AIT is believed to be a better replacement to pharmacotherapy as AIT assures long-term effect by halting the progression of allergen-induced pathology (Patel and Meher 2016). In India, immunotherapy (IT) guidelines were published by Gaur et al. (2009). These guidelines were prepared following the expert suggestions from the Indian College of Allergy, Asthma and Applied Immunology (ICAAI) along with an extensive literature study. Most of the clinical trials displayed significant improvement in allergic asthma and rhinitis or rhino-conjunctivitis patients post IT (1–5 years) compared to the baseline or placebo. However, it was strongly suggested that IT should be practiced by professional clinicians. The purpose of implementing these guidelines was to sustain a consistency in the methods of diagnosis and management, i.e., immunotherapy throughout the country. These guidelines are based on available guidelines with few alterations keeping in mind the multitude of factors in India. In 2017 update by the ICAAI prepared another revised guideline to review the recent data, updating the guidelines published in 2009 (Gaur et al. 2017). This recent guideline has recommended HDM-sensitised atopic dermatitis (AD) patients to be appropriate candidates for AIT.
Successful immunotherapy in India for HDM sensitised patients
A retrospective analysis of a prospective symptom review in patients receiving AIT has been conducted in India to determine the type, number, concentration, and combination of allergens on the efficacy of AIT. AIT involving a mixture of 5–8 allergens and HDM were administered separately to the patients. Only 42% of the patients showed improvement whereas 58% had no improvement or worsening of their symptoms. It was further analysed that the 58% of patients who did not benefit from AIT, received allergens in incorrect combination. The compatibility of allergens was determined by the protease activity of the individual allergens. High protease-containing enzymes included dust mites, fungal, and insect allergens. These results clearly highlight the impact of the nature of allergens and their combination to be used in IT (Susmita et al. 2007).
Another study proved the efficacy of HDM immunotherapy over a 15-year period in a group of 31 patients (with perennial BA, >+2 SPT and for Df extract) from the Bombay (presently Mumbai) region of India. A patient group was administered immunotherapy for continuous 5 years and then followed-up for a further 10 years. Significant improvement was noted when the global symptom scores and FEV1 values were compared with another group of 38 patients that refused immunotherapy. This improvement was sustained for at least 10 years after termination of immunotherapy (Shaikh 2005).
Possible perspectives of therapy
Recent advances in the field of molecular allergology have contributed tremendous advancement in the field of allergen biology. Considering the steady inclination in the rate of asthma and other allergic diseases, India should now focus on designing tools and strategies for the improvement of the evaluation and management of allergy. For example, Bt sensitization rate in Mumbai city was found to be 15% when measured with the use of Blo t 5 (Lim et al. 2002).
Recent progress regarding allergy treatment strongly suggests the practice of personalised immunotherapies where ‘precision medicine’ will be used according to the disease phenotype of the individual patient (Passalacqua and Canonica 2016; Ferrando et al. 2017). Thus, personalized therapy is a novel approach that launches a customized model for individual patient. The evolution of therapy from the previously used ‘mass targeted treatment’ to the ‘personalised therapy’ in the future is represented through Fig. 3.

Evolution of therapy: past and expected future (Adopted from Ferrando et al. (2017), with minor modifications)
Conclusions
The causative agents of allergy in tropical countries like India significantly differ from the complex etiology noticed in temperate countries. Although the prevalence of allergic airway diseases is substantially higher, their mono-specific cause also offers a unique opportunity to study, treat, and manage the allergic phenotypes by specifically targeting HDM allergens (Andiappan et al. 2014).
In India, HDM play a major role in the pathogenesis of allergic rhinitis and asthma. With its stable year-round tropical climate, India typically does not experience wide fluctuations in environmental or indoor allergens, so that dust mites and thus allergic disease phenotypes tend to be perennial rather than seasonal. The prevention of HDM needs to be done in order to lessen the socioeconomic and healthcare burden of allergic diseases. Immunotherapy is the only option to combat HDM allergic consequences. Accurate characterization of novel allergens is an important aspect regarding this. It refers to a multistep discovery approach consisting of identification, purification, and molecular characterization of individual allergen molecules from a particular source. As compared to the tremendous development in the field of molecular allergology worldwide, there have been only a few reports on the molecular characterization of allergens prevalent on the Indian subcontinent (Bhattacharya et al. 2018). Dp and Df being the major culprits for HDM sensitization worldwide have been extensively studied at the molecular level for the identification of allergens (Radauer et al. 2014). Numerous HDM allergens are reported from various parts of the world. However, there has not been any report on the molecular and structural nature of dust mite allergens from India. As a consequence, allergologists in India are still relying upon the less characterized and less standardized allergen extracts. Molecular studies with reference to the cross-reactivity of HDM allergens are to be performed in India for the proper diagnosis and treatment of allergies toward HDM.
References
Addo-Yobo EO, Custovic A, Taggart SC, Craven M, Bonnie B, Woodcock A (2001) Risk factors for asthma in urban Ghana. J Allergy Clin Immunol 108:363–368
Albano PM, Ramos JD (2011) Association of house dust mite-specific IgE with asthma control, medications and household pets. Asia Pac Allergy 1:145–151
Andiappan AK, Puan KJ, Lee B, Nardin A, Poidinger M, Connolly J et al (2014) Allergic airway diseases in a tropical urban environment are driven by dominant mono-specific sensitization against house dust mites. Allergy 69:501–509
Arbat A, Tirpude S, Dave MK, Bagdia S, Arbat S (2016) Purview of allergens through skin test in Central India. Environ Dis 1:99–104
Arbes SJ Jr, Gergen PJ, Elliott L, Zeldin DC (2005) Prevalences of positive skin test responses to 10 common allergens in the US population: results from the third National Health and Nutrition Examination Survey. J Allergy Clin Immunol 116:377–383
Bhattacharya K, Sircar G, Dasgupta A, Gupta Bhattacharya S (2018) Spectrum of allergens and allergen biology in India. Int Arch Allergy Immunol 177:219–237
Borish L (1999) Genetics of allergy and asthma. Ann Allergy Asthma Immunol 82:413–424
Calderón MA, Linneberg A, Kleine-Tebbe J, De Blay F, Fernandez Hernandez, de Rojas D, Virchow JC, Demoly P (2015) Respiratory allergy caused by house dust mites: what do we really know? J Allergy Clin Immunol 136:38–48
Chaudhury S, Roy I, Podder S, Gupta SK, Saha GK (2005) Diversity of synanthropic mites in Kolkata Metropolis, India. Rec Zool Surv India 104:151–159
Colloff MJ (2009) Dust mites. Springer, The Netherlands
Dave L, Srivastava N (2014) A study of sensitisation pattern to various aero-allergens by skin prick test in patients of United Airway Disease (UAD) in Bhopal, Madhya Pradesh, India. RJPBCS 5:1397–1403
Dey D, Ghosh N, Pandey N, Gupta Bhattacharya S (2014) A hospital-based survey on food allergy in the population of Kolkata, India. Int Arch Allergy Immunol 164:218–221
Dey D, Saha B, Sircar G, Ghosal K, Bhattacharya SG (2016) Mass spectrometry-based identification of allergens from Curvularia pallescens, a prevalent aerospore in India. Biochim Biophys Acta 1864:869–879
Dey D, Ghosal K, Bhattacharya SG (2018a) Aerial fungal spectrum of Kolkata, India, along with their allergenic impact on the public health: a quantitative and qualitative evaluation. Aerobiologia. https://doi.org/10.1007/s10453-018-9534-6
Dey D, Mondal P, Laha A, Sarkar T, Moitra S, Bhattacharyya S, Saha GK, Podder S (2018b) Sensitization to common aeroallergens in the atopic population of West Bengal, India: an investigation by skin prick test. Int Arch Allergy Immunol 178:60–65
Dixit IP, Mehta RS (1973) Prevalence of Dermatophagoides sp. Bogdanov, 1864 in India and its role in causation of bronchial asthma. J Assoc Phys India 21:31–37
Doshi A, Tripathi DM (2016) Early house dust mite sensitivity in Mumbai children. Indian J Pediatr 83:386–390
Downs SH, Marks GB, Sporik R, Belosouva EG, Car NG, Peat JK (2001) Continued increase in the prevalence of asthma and atopy. Arch Dis Child 84:20–23
Dutta S, Mondal P, Saha NC, Moitra S, Podder S, Ghosh A, Saha GK (2017) Role of offending out-door aero-allergen and CD14 C(-159)T polymorphism in development and severity of asthma in a Kolkata patient population. Afr Health Sci 17:1101–1109
Fernández-Caldas E, Baena-Cagnani CE, López M, Patiño C, Neffen HE, Sánchez-Medina M et al (1993) Cutaneous sensitivity to six mite species in asthmatic patients from five Latin American countries. J Invest Allergol Clin Immunol 3:245–249
Ferrando M, Bagnasco D, Varricchi G, Bernardi S, Bragantini A, Passalacqua G, Canonica GW (2017) Personalized medicine in allergy. Allergy Asthma Immunol Res 9:15–24
Gaur SN, Singh BP, Singh AB, Vijayan VK, Agarwal MK (2009) Guidelines for practice of allergen immunotherapy in India. Indian J Allergy Asthma Immunol 23:1–21
Gaur SN, Kumar R, Singh AB, Agarwal MK, Arora N (2017) Allergen immunotherapy in India: 2017-An update. Indian J Allergy Asthma Immunol 31:3–33
Ghosh A, Dutta S, Podder P, Mondal P, Laha A, Saha NC, Moitra S, Saha GK (2018) Sensitivity to house dust mites allergens with atopic asthma and its relationship with CD14 C(-159T) polymorphism in patients of West Bengal, India. J Med Entomol 55:14–19
Gill NK, Kaur H (2014) A study on the occurrence, prevalence and species composition of mite fauna in the human dwellings of Patiala city, Punjab (India). Indian J Sci Res 8:91–97
Gowda G, Lakshmi S, Parasuramalu BG, Nagaraj C, Gowda BVC, Somashekara KG (2014) A study on allergen sensitivity in patients with allergic rhinitis in Bangalore, India. J Laryngol Otol 128:892–896
Griffiths DA, Cunnington AM (1971) Dermatophagoides microceras sp. n., a description and comparison with its sibling species, D. farina Hughes, 1961. J Stored Prod Res 7:1–14
Heinzerling LM, Burbach GJ, Edenharter G, Bachert C, Bindslev-Jensen C, Bonini S et al (2009) GA(2)LEN skin test study I: GA(2)LEN harmonization of skin prick testing: novel sensitization patterns for inhalant allergens in Europe. Allergy 64:1498–1506
Jain S, Gupta SK (2018) Study of allergen patterns in patients of severe persistent allergic rhinitis in Central India based on Modified Skin Prick Test reactivity. IOSR J Dent Med Sci (IOSR-JDMS) 17:16–20
Kannan I, Rajendran P, Selvarani P, Thyagarajan SP (1996) A survey of house dust mites in Madras (India) in relation to mite density, seasonal variation and niche. Biomedicine 16:58–62
Kidon MI, Chiang WC, Liew WK, Lim SH, See Y, Goh A et al (2005) Sensitization to dust mites in children with allergic rhinitis in Singapore: does it matter if you scratch while you sneeze? Clin Exp Allergy 35:434–440
Kim BS, Jin HS, Kim HB, Lee SY, Kim JH, Kwon JW et al (2010) Airway hyperresponsiveness is associated with total serum immunoglobulin E and sensitization to aeroallergens in Korean adolescents. Pediatr Pulmonol 45:1220–1227
Krishna Rao NS, ChannaBasavanna GP (1977) Some unrecorded mites from house dust samples in Bangalore, Karnataka, India. Acarol Newslett 5:5–7
Krishna Rao NS, Khuddus CA, ChannaBasavanna GP (1973) Pyroglyphid mites in man and his surroundings. Curr Sci 42:33
Krishna Rao NS, Ranganath HR, ChannaBasavanna GP (1981) House dust mites from India. Indian J Acarol 5:85–94
Kumar R, Sharan N, Kumar M, Bisht I, Gaur SN (2012) Pattern of skin sensitivity to various aeroallergens in patients of bronchial asthma and/or allergic rhinitis in India. Indian J Allergy, Asthma Immunol 26:66–72
Kumar R, Sharan N, Kumar M, Bisht I, Gaur SN (2017) Prevalence of aeroallergens in patients of bronchial asthma and/or allergic rhinitis in India based on skin prick test reactivity. Indian J Allergy, Asthma Immunol 31:45–55
Kunoor A, Harilakshmanan P, James PT, Rakesh PS (2017) Allergen profile of patients from Central Kerala, India. Int J Pharm Bio Sci 8:588–592
Lal A, Waghray SS, Nand Kishore NN (2011) Skin prick testing and immunotherapy in nasobronchial allergy: our experience. Indian J Otolaryngol Head Neck Surg 63:132–135
Lam HT, Ekerljung L, Bjerg A, Van TTN, Lundback B, Ronmark E (2014) Sensitization to airborne allergens among adults and its impact on allergic symptoms: a population survey in northern Vietnam. Clin Translat Allergy 4:6
Leung TF, Lam CW, Chan IH, Li AM, Ha G, Tang NL et al (2002) Inhalant allergens as risk factors for the development and severity of mild-to-moderate asthma in Hong Kong Chinese children. J Asthma 39:323–330
Lim DL, Shek LP, Shaikh WA, Baratawidjaja K, Trakultivakorn M, Vichyanond P et al (2002) Pattern of sensitization to Blomia tropicalis and its recombinant allergens in four tropical asian populations. J Allergy Clin Immunol 109:S179
Matta JS, Jain P, Ved ML (2017) Study of common aero-allergen in Mewar region, Udaipur, Rajasthan, India. Int J Res Med Sci 5:410–414
Maurya KR, Jamil Z (1980) Factors affecting the distribution of house-dust mites under domestic conditions in Lucknow. Indian J Med Res 72:284–292
Maurya KR, Jamil Z, Dev B (1983) Prevalence of astigmatid mites (Acarina) in the domestic environment of north-eastern and northern India. Biol Mem 8:207–215
Mishra VD, Mahmood T, Mishra JK (2016) Identification of common allergens for united airway disease by skin prick test. Indian J Allergy, Asthma Immunol 30:76–79
Modak A, Saha GK, Tandon N, Gupta SK (1991) Dust mite fauna in houses of bronchial asthma patients—a comparative study of three zones of West Bengal. Entomon 16:115–120
Modak A, Saha GK, Tandon N, Gupta SK (2004) Faunal diversity and habitat preference of house dust mites in West Bengal in relation to nasobronchial allergic disorders. Rec Zool Surv India 102:137–146
Moingeon P, Mascarell L (2012) Novel routes for allergen immunotherapy: safety, efficacy and mode of action. Immunotherapy 4:201–212
Mondal P, Dey D, Sarkar T, Laha A, Moitra S, Bhattacharyya S, Saha NC, Saha GK, Podder S (2018) Evaluation of sensitivity toward storage mites and house dust mites among nasobronchial allergic patients of Kolkata, India. J Med Entomol. https://doi.org/10.1093/jme/tjy206
Nath P, Gupta R, Jameel Z (1974) Mite fauna in the house dust of bronchial asthmatic patients. Indian J Med Res 62:1140–1145
Nayar E, Lal M, Gupta DA (1974) The prevalence of mite Dermatophagoides pteronyssinus and its association with house dust allergy. Indian J Med Res 62:11–13
Passalacqua G, Canonica GW (2016) Allergen immunotherapy: history and future developments. Immunol Allergy Clin North Am 36:1–12
Patel S, Meher BR (2016) A review on emerging frontiers of house dust mite andcockroach allergy research. Allergol Immunopathol (Madr). https://doi.org/10.1016/j.aller.2015.11.001
Peat JK, Tovey E, Toelle BG, Haby MM, Gray EJ, Mahmic A et al (1996) House dust mite allergens. A major risk factor for childhood asthma in Australia. Am J Resp Crit Care Med 153:141–146
Podder S, Chowdhury I, Das A, Gupta SK, Saha GK (2006) Immediate hypersensitivity to common inhalants: an investigation of nasobronchial allergy patients in Kolkata, India. Allergy Clin Immunol Int: J World Allergy Org 18:114–119
Podder S, Gupta SK, Saha GK (2009) Seasonal prevalence of allergenic mites in house dust of Kolkata metropolis, India. Aerobiologia 25:39–47
Podder S, Gupta SK, Saha GK (2010) Incrimination of Blomia tropicalis as a potent allergen in house dust and its role in allergic asthma in Kolkata metropolis, India. World Allergy Organ J 3:182–187
Radauer C, Nandy A, Ferreira F, Goodman RE, Larsen JN, Lid-holm J et al (2014) Update of the WHO/IUIS Allergen Nomenclature Database based on analysis of allergen sequences. Allergy 69:413–966
Raj D, Lodha R, Pandey A, Mukherjee A, Agrawal A, Kabra Sk, And New Delhi Childhood Asthma Study Group (2013) Aeroallergen sensitization in childhood asthmatics in Northern India. Indian Pediatr 50:1113–1118
Ranganath HR, ChannaBasavanna GP (1988) House dust mites from Bangalore, India – A quantitative analysis. In: de Weck AL, Todt A (eds) Mite Allergy a Worldwide Problem. UCB Institute of Allergy, Brussels, pp 21–22
Ring J (1997) Allergy and modern society: does ‘western life style’ promote the development of allergies? Int Arch Allergy Immunol 113:7–10
Saha GK (1993) House dust mite allergy in Calcutta, India: evaluation by RAST. Ann Allergy 70:305–309
Saha GK (1997) House dust mite sensitivity among rural and urban asthmatics of West Bengal, India: a comparison. Aerobiologia 13:269–273
Saha GK, Modak A, Batabayal SK, Choudhuri DK, Maitra SB, Tandon N (1989) Clinical significance of IgE in bronchial asthma. J Indian Med Assoc 87:155–157
Saha GK, Modak A, Tandon N, Choudhuri DK (1994) Prevalence of house dust mites (Dermatophagoides spp.) in homes of asthmatic patients in Calcutta. Ann Entomol 12:13–17
Sears MR, Burrows B, Herbison GP, Holdaway MD, Flannery EM (1993) Atopy in childhood. II. Relationship to airway responsiveness, hay fever and asthma. Clin Exp Allergy 23:949–956
Shafique RH, Akhter S, Abbas S, Ismail M (2018) Sensitivity to house dust mite allergens and prevalence of allergy-causing house dust mite species in Pothwar, Pakistan. Exp Appl Acarol 74:415–426
Shaikh WA (2005) Long-term efficacy of house dust mite immunotherapy in Bronchial Asthma: a 15-year follow-up study. Allergol Int 54:443–449
Sharma D, Dutta BK, Singh AB (2011) Dust mites population in indoor houses of suspected allergic patients of South assam, India. ISRN Allergy. https://doi.org/10.5402/2011/576849
Shirai T, Yasueda H, Saito A, Taniguchi M, Akiyama K, Tsuchiya T et al (2012) Effect of exposure and sensitization to indoor allergens on asthma control level. Allergol Int 61:51–56
Shivpuri DN (1962) Comparative evaluation of the sensitivity of common methods of diagnostic antigen tests in patients of respiratory allergy. Indian J Chest Dis 4:102–108
Shivpuri DN (1977) House dust mite allergy in India. J Allergy Clin Immunol 5:19–35
Shivpuri DN, Dua KL (1974) Seasonal periodicity of house dust mite population. Allergy Appl Immunol 7:63–74
Singh AB, Kumar P (2002) Common environmental allergens causing respiratory allergy in India. Indian J Pediatr 69:245–250
Singh AB, Kumar P (2003) Aeroallergens in clinical practice of allergy in India. An overview. Ann Agric Environ Med 10:131–136
Singh AB, Shahi S (2008) Aeroallergens in clinical practice of Al-lergy in India- ARIA Asia Pacific work-shop report. Asian Pac J Allergy Immunol 26:245–256
Spieksma FT, Spieksma-Boezeman MI (1967) Themite fauna of house dust with particular reference to the house-dust mite Dermatophagoides pteronyssinus (Trouessart, 1897) (Psoroptidae:Sarcoptiformes). Acarologia 9:226–241
Sporik R, Platts-Mills TAE (1992) Epidemiology of dust-mite-related disease. Exp Appl Acarol 16:141–151
Squillace SP, Sporik RB, Rakes G et al (1997) Sensitization to dust mites as a dominant risk factor for asthma among adolescents living in central Virginia. Am J Respir Crit Care Med 156:1760–1764
Susmita J, Vijayalakshmi V, Suman Latha G, Murthy KJ (2007) Combination of allergens in specific immunotherapy for IgE mediated allergies. Lung India 24:3–5
Tan CY, Chen YL, Wu LS, Liu CF, Chang WT, Wang JY (2006) Association of CD14 promoter polymorphisms and soluble CD14 levels in mite allergen sensitization of children in Taiwan. J Hum Genet 51:59–67
Tandon N, Saha GK, Modak A, Maitra SB, Kundu SC, Batabayal SK (1988) Mites in house dust as a cause of bronchial asthma. J Assoc Phys India 36:141–144
Tham EH, Lee AJ, Bever HV (2016) Aeroallergen sensitization and allergic disease phenotypes in Asia. Asian Pac J Allergy Immunol 34:181–189
Tilak ST, Jogdand SB (1989) House dust mites. Ann Allergy 63:392–397
van Bronswijk JEMH (1973) Dermatophagoides pteronyssinus (Trouessart) in mattress and floor dust in a temperate climate (Acari: Pyroglyphidae). J Med Entomol 10:63–70
Vercelli D, Baldini M, Martinez F (2001) The monocyte/IgE connection: may polymorphisms in the CD14 gene teach us about IgE regulation? Int Arch Allergy Immunol 124:20–24
Wan KS, Yang W, Wu WF (2010) A survey of serum specific-lgE to common allergens in primary school children of Taipei City. Asian Pac J Allergy Immunol 28:1–6
Wong SF, Chong AL, Mak JW, Tan J, Ling SJ (2011) Tze Ming Ho MT (2011) Molecular identification of house dust mites and storage mites. Exp Appl Acarol 55:123–133
Yadav A, Naidu R (2015) Clinical manifestation and sensitization of allergic children from Malaysia. Asia Pac allergy 5:78–83
Zhang C, Li J, Lai X, Zheng Y, Gjesing B, Spangfort MD et al (2012) House dust mite and storage mite IgE reactivity in allergic patients from Guangzhou, China. As Pac J Allergy Immunol 30:294–300
Acknowledgements
Authors are thankful to the honourable Vice-Chancellor, University of Calcutta and Principal, Barasat Govt. College, India for providing infrastructural facilities. Funding was provided by Department of Biotechnology, Govt. of West Bengal (Sanction No. 568(Sanc.)/BT-Estt/RD-19/2015 dated 03/08/2016) to Sanjoy Podder and Science Engineering and Research Board, Govt. of India to Debarati Dey (File No.-PDF/20l7/000706, sanction diary No. SERB/F/1877/2018-20l9). Goutam Kumar Saha acknowledges the financial support under ‘UGC-UPE II Grant’ and UGC-BSR-Mid Career Award Grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dey, D., Saha, G.K. & Podder, S. A review of house dust mite allergy in India. Exp Appl Acarol 78, 1–14 (2019). https://doi.org/10.1007/s10493-019-00366-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10493-019-00366-4