
Abstract
Spirituality and the big five personality traits may be risk or protective factors for coping with stress. We hypothesized young adults who reported higher spirituality ratings would demonstrate lower sympathetic nervous system arousal and better emotional coping when exposed to a laboratory stressor compared to those who rated themselves lower in spirituality. We also compared spirituality groups on trait anger, neuroticism, conscientiousness, extraversion, agreeableness and openness to experience. Eighty participants completed trait-state anger, personality and spirituality questionnaires and were grouped into low, average and high spirituality. Participants’ physiological responses were monitored before and during a stressful event. Significant differences were found between low, average and high spirituality groups’ respiration rate and emotional response to the stressor. Significant differences were also found between spirituality groups in extraversion, agreeableness, conscientiousness, trait anger and neuroticism. Females reported higher levels of spirituality and conscientiousness than males.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is overwhelming evidence that higher ratings of stress are related to increased risk for illness and death (Taylor 2008). Research on the big five personality traits also supports the idea that these traits may serve as important risk or protective factors for wellness, recovery from illness and lower mortality rates (Taylor 2008). The big five personality traits include neuroticism, extraversion, agreeableness, conscientiousness and openness to new experiences. Furthermore, a growing body of research reveals a statistically significant, positive relationship between higher levels of reported spirituality, religiousness and better health (Oman et al. 2006). In this decade, there has been a call for researchers to begin investigating how spirituality plays a role in everyday life in contrast to the earlier, broad approach linking spirituality and religiousness to health and illness (Sherman and Plante 2001).
There continues to be debate on defining and distinguishing spirituality from religiosity (Richards and Bergin 2005). In this paper, we focus on spirituality. It is beyond the parameters of this paper to review the enormous literature on issues related to definitions of religiosity and spirituality. We are using a very broad-based definition of spirituality that views spirituality on a continuum from very low to very high spirituality. Spirituality is an orientation toward feeling and/or wanting to be connected to something bigger than oneself and the search for the sacred in life. Richards and Bergin (2005) suggest the “essential characteristics of spiritual people are that they enjoy loving and genuine closeness, harmony and connection with God and spiritual realities… without this personal connection, the practice or experience may be religious, but not spiritual” (p. 22). We think of religion as the ‘language’ of spirituality or the expression of spirituality as it relates to particular religious traditions and culture. Religious expressions can be private or public and include beliefs, practices and feelings (Pargament 1999). Qualitative observations of individuals’ report of spirituality include the notion that spirituality and religiosity are not the same phenomena, although most people agree they are related.
In line with the idea that spirituality and religiosity are related but different experiences a variety of scales are available that attempt to capture these differences (Sherman and Simonton 2001). Most scales however, combine aspects of spirituality and religiosity. Sherman and Simonton (2001) describe general measures of religiousness as ones that assess a person’s characteristic involvement in spirituality or religion. Aspects of an individual’s experience that might be included in an assessment are spiritual experiences, level of faith, and religious motivation and commitment (Sherman and Simonton 2001). In this study, we used a scale from the Resilience Questionnaire (RQ) to assess spirituality (Sideroff 2004). We chose this scale, as the items were consistent with our operational definition of spirituality described in the preceding paragraph.
Some researchers propose that people who are more spiritual are more likely to be involved in a faith community that promotes moderate and healthy lifestyles and social support. People with higher levels of spirituality may also be more optimistic and more likely to persist when coping with the challenges of life. There has been a great deal of research supporting the idea that people who meditate tend to have better physical and mental health (Oman et al. 2006). However, not all people who rate themselves as spiritual engage in meditative experiences. Although there has been research exploring the psychophysiological functioning of people who engage in meditative practices; we have not been able to find any research on the psychophysiological functioning of individuals who rate themselves as highly spiritual whether or not they mediate.
The concurrent relationship between spirituality and personality has been well documented but there has been little work on how these characteristics develop over time (Wink et al. 2007). In general, research findings suggest that people who rate themselves high on spirituality tend to rate themselves high on personality traits that are protective health factors such as conscientiousness, agreeableness and extraversion and low on health risk factors such as neuroticism (Simpson et al. 2007). Piedmont (1999) presents a review of studies assessing personality traits and spirituality and data from two separate studies that provide a convincing argument that spirituality or what he calls ‘spiritual transcendence’ represents a potential sixth domain of personality. More research studies are needed to further understand the relationship between the big five personality traits and self-report of spirituality. How distinct are these aspects of human experience and how might they interact to encourage or discourage the emergence of different types of coping mechanisms? What is the developmental nature of spiritual orientation and personality? A study by Wink et al. (2007) is a recent example of one that addresses the interaction and development of personality and spirituality. Their research suggests that some personality traits such as ‘openness to experience’ in adolescence predicted spiritual seeking in later life.
In a recent summary of spirituality and personality research, Simpson et al. (2007) conclude this research area is relatively new and much of the work to date is correlational. An example of a study that provides a randomized, controlled attempt to reduce stress in health professionals using passage meditation—a spiritual intervention called the Eight-Point Program (EPP)—found that the benefits of the intervention were greater for those who rated themselves as less spiritual than participants with higher spirituality ratings (Easwaran 1978/1991; Oman et al. 2006). They also conclude that future studies should exam potential physiological stress and disease markers associated with changes in spirituality using EPP.
In our study, we use quasi-experimental methodology in order to determine whether young adults who report higher or lower levels of spirituality respond differently in a stressful situation. We hypothesized that participants with higher ratings of spirituality would experience lower sympathetic nervous system arousal and negative emotional coping when exposed to a laboratory stressor compared to participants with lower ratings of spirituality. We were particularly interested in evaluating sympathetic nervous system response and anger to a stressful event. We are not aware of any other controlled research studies that have assessed self-report of spirituality prior to exposure to a stressful stimulus that included both emotional and physiological coping responses.
Based on previous research that suggests significant relationships between spirituality and personality characteristics, we also hypothesized that groups with higher ratings of spirituality would report lower levels of neuroticism and trait anger and higher levels of agreeableness and conscientiousness.
Methods
Participants
Eighty college students, participated; 26 males and 54 females, M age = 18.50, SD = .84. Sixty-eight percent were Caucasian, 18% African-American, 9% Asian, 3% Native American, and 2%’other’. Participants received 5% grade credit in their psychology courses for participation in the study. The Institutional Review Board of the university approved the study and the ethical standards of the American Psychological Association were upheld in conducting the study.
Measures and Apparatus
Measures included a demographic questionnaire, State-Trait Anger Expression Inventory-2 (STAIX-2), NEO Personality Inventory-Revised, Resilience Questionnaire, and physiological assessment of heart rate, respiration and skin conductance. A cognitive speed test was used to elicit sympathetic nervous system arousal. Measures and apparatus are described below.
Demographic Questionnaire
The demographic questionnaire included information regarding gender, race, age, academic performance, class level, etc.
State-Trait Anger Expression Inventory
The State-Trait Anger Expression Inventory-2 (STAXI-2) was used to measure state and trait anger. The STAXI-2 is a self-report survey, which scores experience of anger along multiple axes: State and Trait Anger (S-Ang and T-Ang) as well as Anger Control and Anger Expression. The full STAXI-2 is a 57-item self-report instrument, with six scales and five subscales. (Spielberger 1999). The STAX-I has been demonstrated to correlate “strongly” with the Buss-Durkee Hostility Inventory and Overt Hostility scales of the MMPI. (Spielberger 1999) arguing for convergent validity.
Revised NEO Personality Inventory
The NEO PI-R was developed using personality descriptors and factor analyzing them until 5 general domains were found. The domains are often referred to as the “Big Five” personality traits. Costa and McCrae (1992) called these domains Neuroticism (N), Extraversion (E), Openness (O), Agreeableness (A), and Conscientiousness (C). The NEO PI-R form S consists of 240 items that are rated on a 5-point Likert scale from Strongly Disagree to Strongly Agree, and yields an overall score for each domain. Costa and McCrae (1992) report convergent validity between individual scales from the NEO PI-R and similar scales from other measures of personality such as the Wiggins’ Revised Interpersonal Adjective Scales, Edwards Personal Preference Schedule, Eysenck Personality Inventory, State-Trait Personality Inventory and more.
Resilience Questionnaire: Spirituality Scale
We used this scale as the operational definition of spirituality for this study and created the three spirituality groups, low, average and high, using the scores from this scale. Researchers often use a subscale from a questionnaire to determine levels of the independent variable they are interested in studying. Classic examples would be studies using subscales such as the Depression or Anxiety scales of the Minnesota Multiphasic Personality Inventory to group participants into different levels of symptomalogy under study.
Sideroff (2004) created RQ to assess nine components of resilience: physiological, emotional, cognitive, relationship with self, relationship with others, relationships with something greater, presence, flexibility and power. We used the ‘relationship with something greater’ scale as the ‘spirituality scale’ for this study because it assesses a broad sense of individual spirituality. This component has two dimensions: perspective and connection. Items are rated from 0 (not at all true) to 4 (very true). The Spirituality Scale and the Total Resilience Score was significantly correlated, r = .76, p = .000. The Spirituality Scale was significantly correlated (p = .00) with all of the other scales, correlations ranging from r = .36 to r = .62 and was not significantly correlated with the cognitive scale r = .21, p = .07. Because the RQ defines spirituality as ‘relationship with something greater than oneself’ we believed that this scale would serve the purpose of identifying those individuals who rated themselves as low, average, or high on the broad-based definition of spirituality that we were interested in studying.
Physiological Monitoring
A small testing room containing a recliner, chair and side table was used. A 40-watt desk lamp softly lighted the room. Heart rate was measured by placing EKG gel electrodes on the chest, providing the best signal quality. The negative lead was placed on the right shoulder, the positive lead at the xphoid process and the ground lead on the left shoulder. An abdominal placement for respiration was used by strapping the respiration sensor’s Velcro fastener across the participant, at the belly-button level with the rubber tube placed on the front. The strap was adjusted so that there was a slight tension when the participant fully breathed out. A second respiration sensor for thoracic breathing was wrapped around the participant just below the armpit level. Each electrode of the skin conductance sensor was strapped around the finger pads of the index and annular fingers. The electrodes were placed on the palm side of the finger. Heart rate, respiration and skin conductance were monitored using a Procomp+ encoder. Leads for each monitor were routed through a Procomp+ encoder, and data was processed, observed and recorded with the use of CardioPro 2.0 software.
Mentally Challenging Test
A brief, “cognitive speed test” was administered to elicit sympathetic nervous system arousal, simulating a negative stressor (Labbé et al. 2007). The test took about 10 min and contained 80 simple calculations and 16 difficult mathematical operations to be completed in 45 s, 8 number memory items (9–10 string of single digits), 12 difficult verbal analogies, and spelling 14 difficult words. The participant was required to respond verbally to the items.
Procedure
Participants were evaluated one at a time and the procedure took about 1 h for each participant. A graduate research assistant administered the demographic questionnaire, NEO PI-R, STAXI-2, and the RQ. The participant was then hooked up to the physiological sensors for physiological monitoring. A 10 min baseline recording of heart rate, skin conductance and respiration was made. The graduate assistant then administered the CMT and physiological recording continued during this time period. The STAXI-2 State Anger scale was administered after the CMT was completed and the participant was asked to rate his/her performance on the test. Participants were then unhooked from the physiological sensors and were debriefed about the study.
Results
Three groups were created using scores on the spirituality scale of the RQ. Participants’ who had scores less than one standard deviation or more below the mean were placed in the ‘low spirituality’ group and those with scores one standard deviation or more above the mean were place in the ‘high’ spirituality’ group. All other participants were placed in the ‘average spirituality’ group. See Tables 1 and 2 for means and standard deviations of demographic variables, personality and physiological variables for the three groups.
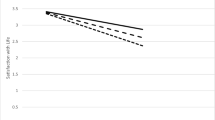
An analysis of variance with repeated measures between groups with low, average and high spirituality scores resulted in significant differences between groups in respiration F(2,77) = 3.66, p = .03 and state anger F(2,77) = 3.97, p = .02 and no significant differences between groups in heart rate F(2,77) = .52, p = .60 and skin conductance F(2,77) = .27, p = .76. See Figs. 1 and 2 for significant differences between groups in respiration and state anger.

Baseline respiration rate and respiration rate during stress for low, average, and high spirituality groups

State anger scores before and after being stressed for low, average and high spirituality groups
An analysis of variance between groups with low, average, high spirituality scores resulted in no differences in self rating of performance on the CMT F(2,77) = .81, p = .45 and actual performance scores F(2,77) = 1.32, p = .27.
Multiple analysis of variance between groups with low, average and high spirituality scores resulted in significant differences between groups in trait anger F(2,77) = 3.35, p = .04; neuroticism F(2,77) = 12.72, p = .000; extraversion F(2,77) = 5.34, p = .007; agreeableness F(2,77) = 8.28, p = .001; and conscientiousness F(2,77) = 7.79, p = .001 but no differences between groups in openness to experience F(2,77) = .56, p = .58.
One-Way Analyses of Variance found significant differences between males and females on conscientiousness scores F (1,78) = 5.21, p = .025, and spirituality scores F (1,78) = 4.91, p = .03, with women demonstrating higher levels of spirituality and conscientiousness.
Discussion
The results of the study provide mixed support for our hypothesis that participants with higher spirituality scores would report less state anger and lower sympathetic nervous system response when responding to a stressor than participants with lower ratings of spirituality. We did find that participants with higher ratings of spirituality had lower state anger and respiration rate to a stressful event compared to participants who scored lower on the spirituality score. However, no significance differences between groups were found for heart rate and skin conductance.
The results provide very significant support for our second hypothesis as participants with higher spirituality scores reported more health protective personality traits—extraversion, agreeableness and conscientiousness—than participants with lower ratings of spirituality. Participants with higher spirituality scores reported significantly lower levels of neuroticism and trait anger compared to participants with lower spirituality scores. These findings are consistent with new, prospective research that indicates personality traits can be risk or protective factors for health and illness (Taylor 2008).
A methodological problem is the unequal numbers of participants in the three spirituality groups with much smaller number of participants in the lower and higher spirituality groups. In addition, it may have been helpful to include a measure of state anxiety to assess whether some participants became anxious during the test as well as angrier.
Although we used a college sample, we recruited a racially diverse sample with 32% of participants being non-white and all the participants were less than 20 years of age. This is a real strength of this study since there are only a few studies of the psychophysiological assessment of older adolescents with this many participants. Moreover, many of the studies on spirituality and health tend to be predominantly with white participants.
Finally, there are no other studies that we are aware of that assess ratings of spirituality and then measure autonomic nervous system response during a stress experience. As mentioned in the beginning of this paper, Sherman and Plante (2001) call for research that moves beyond broad based studies between spirituality and health to begin understanding possible mechanisms underlying this relationship. We found that individuals with higher ratings of spirituality had significantly lower respiration rates before and during a stressful experience. New research suggests respiration has effects on emotional as well as health related problems (Moss 2008). It may be that people who rate themselves as more spiritual experience day to day interactions in a more positive and trusting way—encouraging greater parasympathetic dominance including slower respiration rate. Future studies need to examine not only the rate of respiration, but also the quality of respiration. Holding one’s breath, frequent sighing or slow, diaphragmatic breathing can result in lower respiration rate. Slow, diaphragmatic breathing is more indicative of relaxation and overall lower sympathetic nervous system arousal. Whereas a variety of other factors, including greater sympathetic nervous system arousal, and negative emotional states such as boredom and anxiety can cause one to hold his breath or frequent sighing, resulting in lower respiration rate. Also, note that the participants did speak during some parts of the stress test. However, since all participants spoke about the same amount during the test, the effects of speaking on respiration may be considered a constant and not a concern in interpreting the results of differences between the groups.
In general, the findings of this study are consistent with other research reports assessing personality, spirituality and health—further research is warranted to explore the relationships between psychophysiological responses, spirituality and personality traits in response to stress. The results of this study are also consistent with recent reports of research suggesting that individuals with lower and moderate levels of spirituality demonstrated greater stress and mental health benefits from a meditation-based spiritual intervention than highly spiritual participants (Oman et al. 2006). Ludwig and Kabat-Zinn (2008) report there is a recent explosion of research on mindfulness-based interventions demonstrating benefits for a wide array of problems. These evidence-based practices address spiritual aspects of the participants. Examples of interventions that include enhancing one’s spirituality are mindfulness-based stress reduction, mindfulness based cognitive therapy, dialectical behavior therapy and acceptance and commitment therapy. Studying the effects of increasing spirituality may help us understand process variables that contribute to the effectiveness of these interventions.
We think there should be continued exploration of the concepts of spirituality and religiosity and measurement issues related to these concepts. It is time to begin developing testable models to determine how spirituality may influence anxiety and other negative emotional and physiological states. Moreover, how this relationship may increase or decrease specific health risks and/or help a person cope more effectively with illness.
References
Costa, P. T., & McCrae, R. R. (1992). NEO PI-R: Professional manual. Lutz, FL: Psychological Assessment Resources Inc.
Easwaran, E. (1991). Meditation: A simple eight-point program for translating spiritual ideals into daily life (2nd ed.). Tomales, CA: Nilgiri Press. (Original work published 1978).
Labbé, E., Schmidt, N., Babin, J., & Pharr, M. (2007). Coping with stress: The effectiveness of different types of music. Applied Psychophysiology and Biofeedback, 32(3/4), 163–168.
Ludwig, D. S., & Kabat-Zinn, J. (2008). Mindfulness in medicine. Journal of the American Medical Association, 300(11), 1350–1352.
Moss, D. (2008). Special issue: The psychophysiology of respiration and the effects of breath training. Biofeedback, 36(2), 43–44.
Oman, D., Hedberg, J., & Thoresen, C. E. (2006). Passage meditation reduces perceived stress in health professionals: A randomized, controlled trial. Journal of Consulting and Clinical Psychology, 74(4), 714–719.
Pargament, K. I. (1999). The psychology of religion and spirituality: Yes and no. International Journal for the Psychology of Religion, 9, 3–16.
Piedmont, R. L. (1999). Does spirituality represent the sixth factor of personality? Spiritual transcendence and the five-factor model. Journal of Personality, 67(6), 985–1013.
Richards, P. S., & Bergin, A. E. (2005). A spiritual strategy for counseling and psychotherapy (2nd ed.). Washington, DC: American Psychological Association.
Sherman, A. C., & Plante, T. G. (2001). Conclusions and future directions for research on faith and health. In Sherman. Plante (Ed.), Faith and health: Psychological perspectives. New York, NY: Guilford Press.
Sherman, A. C., & Simonton, S. (2001). Assessment of religiousness and spirituality in health research. In Sherman. Plante (Ed.), Faith and health: Psychological perspectives. New York, NY: Guilford Press.
Sideroff, S. E. (2004). Resilience: A functional approach to stress. California Biofeedback, 20(1), 1–4.
Simpson, D. B., Newman, J. L., & Fuqua, D. R. (2007). Spirituality and personality: Accumulating evidence. Journal of Psychology and Christianity, 26(1), 35–44.
Spielberger, C. D. (1999). STAXI-2 state-trait anger expression inventory-2 professional manual. Lutz, FL: Psychological Assessment Resources, Inc.
Taylor, S. E. (2008). Health psychology (7th ed.). New York, NY: McGraw-Hill.
Wink, P., Ciciolla, L., Dillon, M., & Tracy, A. (2007). Religiousness, spiritual seeking, and personality: Findings from a longitudinal study. Journal of Personality, 75(5), 1051–1064.
Acknowledgements
This project was supported by Grant # 2001-SI-FX-0006 awarded b y the Office of Juvenile Justice and Delinquency Prevention, Office of Justice Programs, US Department of Justice.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Labbé, E.E., Fobes, A. Evaluating the Interplay Between Spirituality, Personality and Stress. Appl Psychophysiol Biofeedback 35, 141–146 (2010). https://doi.org/10.1007/s10484-009-9119-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10484-009-9119-9