
Abstract
A randomized trial compared effects of a Family Critical Time Intervention (FCTI) to usual care for children in 200 newly homeless families in which mothers had diagnosable mental illness or substance problems. Adapted from an evidence-based practice to prevent chronic homelessness for adults with mental illnesses, FCTI combines housing and structured, time-limited case management to connect families leaving shelter with community services. Families were followed at five time points over 24 months. Data on 311 children—99 ages 1.5–5 years, 113 ages 6–10 years, and 99 ages 11–16 years—included mother-, teacher-, and child-reports of mental health, school experiences, and psychosocial well-being. Analyses used hierarchical linear modeling to investigate intervention effects and changes in child functioning over time. Referral to FCTI reduced internalizing and externalizing problems in preschool-aged children and externalizing for adolescents 11–16. The intervention led to declines in self-reported school troubles for children 6–10 and 11–16. Both experimental and control children in all age groups showed reductions in symptoms over time. Although experimental results were scattered, they suggest that FCTI has the potential to improve mental health and school outcomes for children experiencing homelessness.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Homelessness has been associated with poor mental health, behavioral problems, and adverse educational experiences for children. An extensive body of research shows that children assessed during episodes of homelessness report more internalizing and externalizing symptoms than normative samples, but differences from other poor children are less pronounced (Buckner 2008). Symptoms decline over time, which suggests that children recover from the acute threat associated with inadequate housing (Buckner et al. 2004; Shinn et al. 2008). A similar pattern exists for educational outcomes, where homelessness and mobility are associated with poor academic achievement, along with grade retention and problems with teachers (Cutuli et al. 2013; Fantuzzo et al. 2012; Fowler et al. 2014; Herbers et al. 2012; Masten et al. 2014; Miller 2011; Voight et al. 2012). However, much family homelessness occurs before children enter school. Research is mixed as to whether later mobility and homelessness have transient or enduring associations with educational outcomes (Rafferty et al. 2004; Voight et al. 2012). The stressful experiences that accumulate with homelessness and extreme poverty strain abilities to cope and regulate behavior in childhood (Masten et al. 1993). Homelessness represents the far end of the socioeconomic spectrum that exposes youth to a host of environmental risks, including harsher and less nurturing parenting from parents under stress, parent–child separation, and stressful life event (Buckner 2008; Kilmer et al. 2012; Rafferty and Shinn 1991).
Interventions are needed that end homelessness and support healthy child development among families at risk for homelessness and instability. Service providers struggle to develop programs that engage homeless families and address local housing, employment, and social conditions. There is limited evidence about what programs work best. Studies typically lack experimental designs to isolate program effects, and fail to consider child outcomes or assess children directly (cf. Bassuk et al. 2014). Building better approaches to support healthy child development among inadequately housed families requires a stronger empirical base.
Rigorously designed evaluations of homeless services for adults provide potentially useful models of intervention. The Critical Time Intervention (CTI) employs time-limited case management to support severely mentally ill men and women at risk for recurrent homelessness. Randomized controlled trials show after 18 months that adults assigned to CTI spend less time homeless (Herman et al. 2011; Susser et al. 1997), report reductions in psychiatric symptoms (Herman et al. 2000), exhibit lower risk for psychiatric hospitalization (Tomita and Herman 2012), and save significant costs to the homelessness service system (Jones et al. 2003). This study examines an adaptation of CTI targeting homeless families with mental health problems.
Family Critical Time Intervention
Family Critical Time Intervention (FCTI) represents a community-based service model for families using homeless shelters (Felix and Samuels 2006). Multidisciplinary teams that include a case manager, supervisory staff, and a community psychiatrist trained in FCTI and Motivational Interviewing work to strengthen family members’ long-term ties to social services and supportive relationships with extended families and friends. The intervention targets the critical time of transition from the shelter to housing in the community. FCTI progresses through three distinct 3-month intervention phases (Susser et al. 1997). The first phase, Transition to Community, begins when families arrive at the shelter. A case manager completes a thorough family assessment that includes caregiver and child strengths and challenges and then works intensely with the mother, meeting as often as three times per week, to link the family with community resources at local agencies. The second phase, Try-Out, tests and adjusts the support systems established while at the shelter during the family’s move into the community. There is less contact, as families are encouraged to take more control over following through with services and programs on their own. The case manager observes where the mother and family need more or fewer supports and services. The case manager aims to develop trust with the mother while maintaining boundaries around service delivery and provides her with trial and error experiences of connecting with resources in a positive manner. In the final phase, Transfer to Care, the case manager reduces contact further, as families are encouraged to take full responsibility for accessing services. The case manager works with the mother to review and bolster the family’s support system to ensure long-term community-based linkages.
Present Study
The present study compares the FCTI model with usual care for families experiencing both homelessness and mental health problems in Westchester County in a randomized longitudinal experiment. The FCTI model contrasts with usual care in the County at the time of the intervention with respect to both services and housing. FCTI provides time-limited services focused on transitioning families from the shelter to the community. FCTI differs from usual care in three ways. First, families receive continuous case management from a single worker with training in FCTI, whereas typical services reassign caseworkers during and after shelter stays. Second, FCTI case managers carry lower caseloads of 12 families evenly divided by phase of intervention. Shelter caseworkers in the usual care condition had caseloads approximately twice this size, and County social services workers who served usual care families after they left shelter had caseloads four times as large. Third, FCTI families move from shelters to permanent housing as soon as possible. Families in usual care had access to scatter-site subsidized housing only after meeting the caseworker’s standards for housing readiness. Fidelity to the FCTI model was assured by weekly meetings between FCTI workers and the originators of the model.
This paper examines mental health and school outcomes of the experiment over a 2-year period for children 1.5–16 years of age. The broad age range of children allowed tests of how the intervention performed at different developmental phases. Multiple informants reported on child functioning, including children, parents, and teachers. We expected homeless children’s well-being in both experimental and control groups would improve as families put the disruptions of homelessness behind them (Shinn et al. 2008). With respect to interventions, we predicted that FCTI would lead to greater improvements in children’s mental health (reductions in internalizing and externalizing symptoms), and in school outcomes including attitudes, behaviors, and experiences at school. We also anticipated that FCTI would reduce exposure to stressful life events and increase children’s integration into communities, and that it would reduce parent–child separations. Homeless families disproportionately experience child out-of-home placements (Cowal et al. 2002; Park et al. 2004), and stressful events have been more powerful predictors of children’s mental health than prior homelessness in other studies (Buckner et al. 2004; Shinn et al. 2008). Community integration for families is one goal of FCTI, although there is no explicit effort to enhance integration for children. To understand potential mechanisms through which the intervention affects children, we tested whether effects were mediated by time spent in permanent housing and parenting, which FCTI is designed to support and which may enhance children’s resilience (Cutuli and Herbers 2014).
Methods
Participants
This study of children was embedded in a larger experiment evaluating the effectiveness of FCTI for high-risk families entering the homeless shelter system in Westchester County, NY. Shelter staff screened mothers for mental health or substance abuse problems using the Mini International Neuropsychiatric Interview (Sheehan et al. 1998). To be eligible for the study, mothers had to have a diagnosable mental illness or substance abuse problem and care for at least one child aged 1.5–16 years. Mothers speaking languages other than English or Spanish or entering domestic violence family shelters were excluded for logistics and safety reasons.
A total of 200 families with follow-up data (95 % of those enrolled) were included in comparisons of FCTI treatment (n = 97) and usual care control (n = 103) conditions. The average age of mothers was 30.8 years (SD = 8.4). Most identified as African American (65 %), followed by white (25 %), refused (12 %), American Indian or Alaskan Native (10 %), and Asian American (1 %); 26 % additionally identified as Hispanic or Latina. At baseline, most were unemployed (82 %), never married (72 %), and not currently living with a spouse or partner (84 %). Mothers’ average income in the 30 days prior to their baseline interview was $746 (SD = $504). Approximately one-third (36 %) of mothers had never received mental health services.
Trained interviewers collected data at baseline (within 2 weeks of shelter entry), and 3, 9, 15, and 24 months thereafter. At the baseline interview, mothers reported on mental health and school attendance for one randomly selected child. After additional funding was secured to study children (usually at the 3-month assessment but at 9 months for early enrollees), we randomly selected additional children, one in each age group 1.5–5, 6–10, and 11–16 not already represented, if present in the family. The 311 child participants, by age at initial assessment, included 99 1.5–5 year olds (M = 3.4, SD = 1.2), 113 6–10 years (M = 8.0, SD = 1.4), and 99 11–16 year olds (M = 13.3, SD = 1.8) and 153 girls and 158 boys. Mothers responded to an expanded set of questions about all three target children, and children ages 6–16 also completed interviews at each follow-up point.
Random Assignment and Retention
Families stratified by number of children were randomly assigned to the treatment or control conditions through rolling enrollment following the baseline interview. (Larger families tended to use different shelters than smaller families, and take longer to find permanent housing.) Informed consent was separate for screening, study participation, and each follow-up interview. No family refused the screening but 13 eligible families declined to participate in the experiment.
Baseline data were available for 198 mothers, of which 145 (73 %) completed three or four interviews after baseline, 31 (16 %) completed two, and 22 (11 %) completed one post baseline interview. Self-report data were available for 173 children, 92 ages 6–10 years, and 81 ages 11–16 years. This comprised 82 % of children in the older age groups (children under six were not interviewed). Among the 173 older children, 101 (58 %) completed three or four interviews, 39 (23 %) completed two, and 33 (19 %) completed one.
Integrity of randomization was tested comparing baseline treatment and control conditions on mothers’ age, education, employment status, number of children, marital or partner status, global mental health functioning, total income in the previous 30 days, mother reports of the initial target child’s internalizing and externalizing behaviors (all three age groups), and number of school days missed in the previous 30 days (two oldest age groups). In 16 tests, two differences between groups reached p < .10: control mothers reported more income in the previous 30 days than FCTI mothers, $811 versus $671, t(198) = 1.98, p < .05, and control children ages 1.5–5 had higher internalizing scores than children in the FCTI group, t(62) = 2.09, p < .05. None of these baseline characteristics, group assignment, or their interactions predicted dropout (absence of follow-up data) at p < .10.
With the permission of mothers, teachers of children 6 years or older (English teachers if the child had multiple teachers) completed brief questionnaires on students at the end of the fall and spring semesters. Because Westchester has 48 school districts we did not attempt to work through districts and principals, but used information provided by mothers to contact teachers, share maternal consent, and offer a $15 incentive for completion of either a paper or web-based assessment. With phone calls and written reminders, we collected teacher reports for 120 (53 FCTI, 67 control) school-age children from 95 families (48 % of those eligible by age). Teachers were blind to the purpose of the study and to group assignment.
Measures
Internalizing and Externalizing Behaviors
Mothers completed the Child Behavior Checklist (Achenbach and Rescorla 2001a, b) on the initial target child at baseline and on all target children thereafter. Because of the broad age range, we converted raw scores into T-scores that account for age and gender norms. Youth ages 11–16 reported on their own internalizing and externalizing behaviors with the Youth Self-Report (Achenbach and Rescorla 2001b). Using the Teacher Report Form (Achenbach and Rescorla 2001b), teachers reported externalizing behaviors but not internalizing symptoms, which are harder to observe. Scales demonstrated adequate reliability (Cronbach’s α = 0.84–0.96 across ages and informants). All measures have been used previously with homeless children (e.g., Shinn et al. 2008).
Depressive Symptoms
Youth ages 6–10 completed the Children’s Depression Inventory (CDI; Kovacs 1985). For each of the 27 items, children selected one of 3 alternatives such as I hate myself, I do not like myself, I like myself coded on a 0–2 scale. Responses were summed so that higher scores represented more depressive symptoms: α = 0.80.
School/Child Care Attendance
Mothers, children six and older, and teachers reported how many days the child missed school or child care in the previous month. We truncated counts at 15 days.
Positive School/Child Care Attitudes and Experiences
Mothers reported how much their child liked school or child care on a five-point scale from 0 (not at all) to 4 (very much) (Riley 2001). Children six and older completed a 19-item positive school attitudes index with a three-point response scale from 1 (never) to 3 (always). Sample items are “my teacher understands me,” “kids in my class are nice,” and “school is boring” (reversed): α = 0.88–0.89. Mothers also described each child’s experience in school or child care on a three-point scale from 0 (mostly negative experiences) to 2 (mostly positive experiences). This measure has previously differentiated homeless from housed children (Rafferty et al. 2004).
School/Child Care Trouble
Mothers of children six and older answered four questions, e.g., “In the last 4 weeks that your child was in school, how often did he/she get in trouble at school?” on a five-point scale from 0 (never) to 4 (always) α = 0.66–0.74. For children ages 1.5–5, mothers answered one dichotomous item about whether or not youth got into trouble at child care. For children six and older, a self-reported school trouble binary variable was coded one if the child answered yes to any of three questions about getting suspended, being sent to the principal’s office, or having a note sent home in the past month the child was in school.
School Effort and Performance
Children six and older rated school effort based on Riley (2001); “how you did your homework” and “how hard you tried to work during the school day” in the last month on a scale from 1 (could have done a lot better) to 4 (did very well, could not do better), Pearson r = 0.35–0.53. Mothers rated performance of children six and older in up to seven subjects on a four-point scale ranged from 0 (failing) to 3 (above average). The large number of school districts precluded collection of consistent academic achievement records.
Teacher-Rated Behavior and Learning
Teachers rated three items from the Teacher Report Form (Achenbach and Rescorla 2001b) regarding the child’s effort, behavior, and learning. The seven-point response scale ranged from 0 (much less) to 6 (much more compared to typical pupils of the same age), α = 0.87.
Negative Life Events
Children aged 6 years and older reported on occurrence of 16 negative life events in the previous 6 months. Examples included “Were you/family member/friend mugged or robbed or beaten up,” and “Did a parent get arrested or get in trouble with the law?” The measure (based on Seidman 1991 for a multi-ethnic sample of poor urban youth) was a count of items reported, truncated to five due to high positive skew.
Community Integration
Mothers of children ages 6–10 reported the frequency of their child’s involvement in school, neighborhood, and religious institutions in the previous 3 months on a 17-item index developed for a multi-ethnic sample of poor urban youth (Seidman 1991). Children ages 11–16 responded for themselves. Examples include how often the child helped out neighbors or attended youth groups at church, rated on a five-point scale from 0 (never) to 4 (almost every day). Items were summed to create a total score, α = 0.67–0.80.
Child Separation
This was a binary variable that reflected the mother’s separation from any minor child (not just a target child) since the previous interview across eight indicators including absence of a child from the family enumeration, any reported foster-care stay, and separations of a month or more for other reasons. A total of 41 % of mothers (an average of 22 % at each observation period) experienced a separation from at least one child.
Permanent Housing
Proportion of time families spent in permanent housing for each observation period was computed based on the Residential Timeline Follow-back Calendar (New Hampshire Dartmouth Psychiatric Research Center 1995), which has shown reliability and validity even for single homeless individuals with complex residential histories (Tsemberis et al. 2007). Interviewers asked the mother where her family stayed the night before and how long they had stayed there, and continued backward until the time of the previous interview.
Parenting Practices
Mothers completed a revised version of the Child Rearing Practices Report yielding nurturance and restrictiveness scales (Rickel and Biasatti 1982). Sample items included “I believe that children should not have secrets from their mothers” (restrictiveness), α = 0.85; “My children and I have nice, warm intimate moments together” (nurturance) α = 0.86. Responses ranged from 1 (definitely false for yourself) to 5 (definitely true for yourself).
Data Analytic Strategy
Data were analyzed using hierarchical linear modeling (HLM; Raudenbush and Bryk 2002), with a focus on group differences between FCTI and control families and Group × Time interactions, which reflect differential patterns of change over time for the two groups. Main effects of Time reflect the extent to which children’s problems receded (or were exacerbated) for all families as they moved from shelter to conventional housing.
HLM accounts for the statistical dependence of multiple time points within individuals by separating within-person variance (over repeated interviews) from between-person variance. We created a unique regression equation (level-1) for each participant with the outcome expressed as a function of time and time squared. We then specified each level-1 coefficient, including the intercept, with a separate level-2 equation, composed of time-invariant (between-person) predictors, including treatment group, age at baseline, race, and gender. Because main effects of group assignment are evaluated at the level-1 intercept (that is, when Time = 0), we centered Time at 9 months. Thus, the main effect of group assignment was evaluated at 9 months, which was when the FCTI ended and maximum group differences were expected. Analyses first examined the relationship of outcome variables to Time, Time2, level-2 main effects of group assignment, child sex, child baseline age, mother’s race/ethnicity, and Group × Time and Group × Time2 interactions. We then removed variables in the following order if their p value was above .10: Group × Time2 interaction, Time2 main effect, Group × Time interaction, and mother’s race/ethnicity main effect. All models included main effects of Time, group assignment, child’s sex, and child’s baseline age regardless of significance.
Mediation analyses examined whether significant treatment effects on outcomes were conditioned on: (1) proportion of time spent in permanent housing, and (2) mothers’ restrictiveness or nurturance towards their children. Analyses were conducted when a group main effect existed. Mediated moderation analyses were conducted when group assignment interacted with Time or Time2 (Muller et al. 2005), and indirect effects were computed, as suggested by MacKinnon and Dwyer (1993). Because mediation occurred less often than expected by chance, in the interests of brevity, results are not discussed further.
Results
Sample Description and Housing Experiences
At the baseline assessment, shortly after entering shelter with their families, youth exhibited slightly higher levels of emotional and behavioral problems than normative samples. Mean T-scores for mother-reported internalizing (M = 55.2, SD = 11.4) and externalizing (M = 55.8, SD = 11.3) problems fell close to national averages, however, more than a quarter of youth exhibited scores in the clinical range (T ≥ 64) for internalizing (25.4 %) and externalizing (24.9 %), and 22.8 % of youth had scores in the clinical range for both domains. Youth missed a considerable number of school days in the month prior to baseline assessment according to mothers (M = 4.49 absences, SD = 4.38). When first assessed directly at the 3 month follow-up, 12.8 % of youth ages 6–10 reported depression symptoms that exceeded the cutoff score of 13 for clinical problems (M = 7.2, SD = 5.9). Fewer adolescents ages 11–16 reported clinically elevated internalizing (8.2 %) and externalizing (4.9 %) behaviors with average T scores close to national norms (internalizing M = 50.0, SD = 9.7 and externalizing M = 48.1, SD = 11.2).
Families in the FCTI treatment group spent 43 % of the first 3 months after random assignment and 91 % of the next 6 months in conventional housing in the community compared to 8 and 45 % for families in the usual care control group. FCTI services ended at 9 months, and housing patterns for treatment and control groups converged. Families in the FCTI group spent 89 % of the time from 9 to 15 months and 86 % of the time from 15 to 24 months in community housing, compared to 76 and 73 % in the control group.
Children Ages 1.5–5 Years
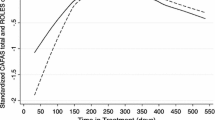
Table 1 shows experimental effects for children ages 1.5–5, controlling for child’s age and sex and mother’s race/ethnicity (not shown). With respect to mental health, FCTI reduced both internalizing and externalizing behaviors. For internalizing, there were also significant Time and Time2 effects and a marginally significant Group × Time2 effect. As shown in Fig. 1, children assigned to FCTI experienced fewer internalizing behaviors than children in the control group until 24 months, when both groups had similar levels. The greatest difference between the two groups (0.6 standard deviations) was at 9 months, the point where we expected maximum intervention effects (FCTI = 49.2, Control = 41.9). For externalizing, the group difference in T-scores favoring the FCTI group was 6.2 (0.5 standard deviations). There was also a quadratic effect of Time such that externalizing behaviors declined until 15 months, and then rose slightly. The overall decrease in T-scores from 0 to 24 months was 3.4 (0.3 standard deviations).

Group × Time interactions for children ages 1.5–5. Internalizing behavior scores (mother-reported)
There were no reliable differences between experimental conditions in any measure of child care or school for children 1.5–5. Mothers reported that children liked child care or school (M = 3.5 on a 4-point scale across all time points). The probability of children experiencing child care/school trouble increased over time, from 0.21 at 3 months to 0.43 at 24 months. Absences marginally decreased over time in this age group such that children missed 1.4 fewer days per month at 24 than at 3 months. No mother reported that a child had mostly negative experiences in school and across time 75 % reported mostly positive experiences.
Children Ages 6–10 Years
Table 2 shows experimental effects for children ages 6–10. There were no intervention effects on mental health in this age group but there were significant improvements over time across both treatment conditions on mother-reported internalizing and externalizing (4.5 T-Score points or 0.4 standard deviations, and 4.0 or 0.3 standard deviations from 0 to 24 months) and child-reported depressive symptoms (1.3 points or 0.2 standard deviations from 3 to 24 months).
Among school variables reported by mothers, there was a significant Time main effect, a marginally significant Time2 effect, and a significant Group × Time2 interaction for absences. As shown in Fig. 2a, mothers in both groups reported the highest number of absences in the previous 30 days at baseline, when families had just become homeless (FCTI = 4.1, control = 3.1). Absences decreased (and were nearly identical) in the two groups through the 15-month assessment, and then rebounded somewhat in the experimental group (absences = 3.4) at 24 months, but continued to decrease in the control group (absences = 1.0). Academic performance as reported by mothers improved over time in both groups from an average of 2.0 at 3 months to 2.2 at 24 months (0.3 standard deviations, or improvement from average to above average in one out of five classes). Mothers reported that children liked school (M = 3.2 on a 0–4 scale where 4 = very much), rarely got into trouble at school (M = 0.7 on a 0–4 scale where 0 = never), and had generally positive experiences in school (M = 1.7 on a 0–2 scale where 2 is mostly positive experiences). There were no differences between groups or across time.

Group × Time interactions for children ages 6–10. a Number of school absences (mother-reported). b Probability of school trouble (child-reported)
For child-reported school variables, there was a significant Group × Time interaction predicting school trouble. As Fig. 2b shows, children in FCTI started higher, but decreased over time, whereas the control group increased, so that experimental group children were half as likely as control group children to report school trouble by 24 months (0.14 vs. 0.33). School effort, as reported by children increased an average of 0.3 points (0.4 standard deviations) from 3 to 24 months. The average score across time was 3.1 where 3 = did about as well as you could, and did not vary by group. Children also reported generally positive school attitudes (M = 2.6 on a 1–3 scale), with no reliable differences by group or time, for this variable, for child-reported absences (M = 2.5 days over the last month), or negative life events (M = 1.4 over 6 months).
Children Ages 11–16 Years
Table 3 shows experimental effects for children ages 11–16. As for children ages 6–10, mothers’ reports of internalizing behaviors showed main and quadratic effects of Time: scores declined until 15 months and then slightly increased. The overall decrease in T-scores was 3.7 (0.3 standard deviations). For child reports, internalizing decreased steadily over time for a total of 4.7 points (0.4 standard deviations). For externalizing behaviors reported by the mother, there were significant Time and Group × Time effects (see Fig. 3a) favoring the experimental group. Specifically, externalizing declined for children in the FCTI group, but remained fairly constant in the control group. At 24 months, the difference between the two groups was 6.2 (0.5 standard deviations). There were no effects on externalizing in children’s self-reports.

Group × Time interactions for children ages 11–16. a Externalizing behavior scores (mother-reported). b Probability of school trouble (child-reported)
For school outcomes, both mothers and children in the FCTI group reported 1.0 fewer absence per month than their control group counterparts (marginally significant in each case). Overall, mothers rated children’s school experiences as 2.5, midway between 2 both positive and negative experiences and 3 mostly positive experiences. Children in the FCTI group had marginally more positive experiences than control children (0.2 higher, or 0.3 standard deviations). Mothers also reported that the FCTI group performed significantly better (M = 2.0 vs. 1.8 or 0.3 standard deviations) or improvement in one of five classes from below average to average). For child reports, in addition to absences, there was a Group × Time interaction in the prediction of school trouble. As shown in Fig. 3b, both groups started out at the same level (42 % reported a trouble), but the FCTI group decreased more over time so that by 24 months, only 6 % of the FCTI group compared with 37 % of the control group reported a trouble. There were no differences in this variable by mother report, and neither mothers nor children reported differences in school attitudes, with liking (M = 2.8 by mother report) close to three pretty much and positive attitudes (M = 2.4 by youth report) midway between sometimes and always. Children in this age group reported school effort (M = 2.7) midway between could have done a little better and did about as well as you could, with no differences by time or group.
There were no intervention effects on secondary outcomes, but across conditions a reduction of an average of 0.6 negative life events (0.4 standard deviations) over the course of the study, and also a reduction in community integration by 5.3 (0.5 standard deviations).
Cross-Age Effects
There were no group differences on teacher ratings of youth externalizing behaviors, absences, or positive behavior and learning, averaged across assessments. Nor were there effects of intervention or time on parent–child separation. These were tested using HLM at the level of families, with observation points nested within families because mothers reported on separations from any child, not just target children.
Discussion
This study is one of the first to describe not just adverse outcomes among homeless children, but positive effects of an intervention to alleviate them. FCTI led to improvements or accelerated improvements with time on 15 % of children’s outcomes at p < .05, with effect sizes ranging up to three-fifths of a standard deviation. Assignment to FCTI rather than usual care led to improvements of 0.4 standard deviations in internalizing and 0.2 in externalizing for children ages 1.5–5, to 1.0 fewer absences per month for children ages 11–16 by both mother and child report, to 0.4 standard deviations improvement in school experiences and 0.2 standard deviations in school performance for children ages 11–16. Interaction effects showed substantial reductions in the probability of FCTI children reporting getting in trouble in school for both ages 11–16 (0.42–0.06) and ages 6–10 (0.32–0.14), with no comparable decreases, or even increases, in the control group. Mother-reported externalizing scores decreased for the oldest FCTI group by 0.5 standard deviations, while the scores for the control group held constant. Only one interaction with time favored the control group (mother-reported absences from school for children ages 6–10, only at 24 months).
Although no effects were observed for the majority of variables, the fact that treatment differences overwhelmingly favored the experimental group and occurred across different reporters suggests that they were not simply due to chance. Moreover, post hoc power analyses that account for observed sample sizes within age groups suggest adequate power to reliably detect moderate intervention benefits over time. Smaller effects on child outcomes might have gone unnoticed. Additionally, this trial occurred in a service-rich homeless system that connects most families to subsidized housing upon discharge from shelters. Larger effects may emerge in contexts that provide less housing assistance or fewer services to families in usual care.
Effects observed here were more numerous than effects on children over 20 months in the Family Options Study, a multi-site trial of three housing and service interventions compared to usual care for families recruited in homeless shelters. In that study, priority offers of permanent housing subsidies, typically a housing choice voucher without additional services, led to large reductions in homelessness and improvements in housing stability, family preservation, and adult well-being, along with reduced employment, but had very few effects on child outcomes, notably reductions in school mobility and absenteeism, relative to usual care. Temporary “rapid re-housing” subsidies also reduced absences relative to usual care; service-rich transitional housing had no effects on children beyond chance (Gubits et al. 2015). The Family Options study did not find effects of any intervention on children’s mental health, which were prominent effects here, and could not examine associations with time, since there was just one assessment 20 months after families entered shelter. It is not clear whether the differences between studies had to do with the nature of the FCT intervention in connecting families to community services, or the fact that mothers in the present study had diagnosable mental illness or substance problems. Children in the Family Options study, like those in the FCTI study, scored above national norms on a (different) parental-report measure of behavior problems.
It is disappointing that FCT intervention effects were not strong enough to be observed by teachers, however, difficulty in recruiting teachers reduced power for these tests. There were also no effects on separation of children from their mothers. Closer interactions with caseworkers may both support mothers and subject them to greater scrutiny with countervailing effects on this outcome. Reducing separations, which occurred in 41 % of families, remains an elusive goal. Barrow and Lawinski (2009), who interviewed mothers in our sample who were separated from children before shelter entry, suggest that both structural conditions that precipitate family crises and the competing demands of multiple agencies involved in families’ lives must be addressed.
Children in both FCTI and control groups showed improvements over time, especially in mental health. This pattern could reflect recovery from the temporary disruption of shelter entry and whatever adverse circumstances precipitated it. Given that improvement generally continued for 2 years, the pattern could also be interpreted as causal, with increasing stability in children’s lives leading to better mental health and school outcomes in both groups. This finding is consistent with earlier research suggesting that adverse effects of homelessness on children dissipate over time (Buckner et al. 1999; Shinn et al. 2008). As Buckner (2008) suggests, improvements may depend on a shelter system that offers housing, supports, and reintegration into communities for families in both groups.
Although this study had notable strengths, including assigning families randomly to interventions, following them over time, and using multiple reporters, it also had some weaknesses. We had relatively small numbers of children in each of the three age groups. Subsequent research should have larger sample sizes (or focus on families with children in a particular age range), and might be done in places where the usual standard of care involves fewer resources, so that experimental contrasts will be sharper. Our findings are restricted to families in which the mother has a mental illness or substance problem. Other families may flourish with fewer supports (Gubits et al. 2015; Shinn et al. 1998).
Despite these limitations, the study suggests that the FCTI, adopted from the earlier Critical Time Intervention with homeless single adults with serious mental illness was helpful is supporting families in which the mother had a diagnosable mental illness or substance problem. The intervention both improved outcomes for children directly and accelerated broader improvements associated with the passage of time.
References
Achenbach, T. A., & Rescorla, L. A. (2001a). Manual for the ASEBA preschool-age forms & profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families.
Achenbach, T. M., & Rescorla, L. A. (2001b). Manual for the ASEBA school-age forms and profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families.
Barrow, S. M., & Lawinski, T. (2009). Contexts of mother–child separations in homeless families. Analysis of Social Issues and Public Policy, 9, 1–20.
Bassuk, E. L., DeCandia, C., Tsertsvadze, A., & Richard, M. K. (2014). The effectiveness of housing interventions and housing and service interventions on ending family homelessness: A systematic review. American Journal of Orthopsychiatry, 84(5), 457–474.
Buckner, J. C. (2008). Understanding the impact of homelessness on children. American Behavioral Scientist, 51, 721–736.
Buckner, J. C., Bassuk, E., Weinreb, L., & Brooks, M. (1999). Homelessness and its relation to the mental health and behavior of low-income school aged children. Developmental Psychology, 35, 246–257.
Buckner, J. C., Beardslee, W. R., & Bassuk, E. L. (2004). Exposure to violence and low income children’s mental health: Direct, moderated, and mediated relations. American Journal of Orthopsychiatry, 74, 413–423.
Cowal, K., Shinn, M., Weitzman, B. C., Stojanovic, D., & Labay, L. (2002). Mother–child separations among homeless and housed families receiving public assistance in New York City. American Journal of Community Psychology, 30, 711–730.
Cutuli, J. J., Desjardins, C. D., Herbers, J. E., Long, J. D., Heistad, D., Chan, C., et al. (2013). Academic achievement trajectories of homeless and highly mobile students: Resilience in the context of chronic and acute risk. Child Development, 84, 841–857.
Cutuli, J. J., & Herbers, J. E. (2014). Promoting resilience for children who experience family homelessness: Opportunities to encourage developmental competence. Cityscape, 16(1), 113–139.
Fantuzzo, J., LeBoeuf, W. A., Chen, C., Rouse, H. L., & Culhane, D. P. (2012). The unique and combined effects of homelessness and school mobility on the educational outcomes of young children. Educational Researcher, 41, 393–402.
Felix, A., & Samuels, J. (2006). Families in shelters. In P. Gillig & H. McQuistion (Eds.), Clinical guide to the treatment of the mentally ill homeless person (pp. 35–49). Washington, DC: American Psychiatric Publishing Inc.
Fowler, P. J., Henry, D. B., Schoeny, M., Chavira, D., & Taylor, J. (2014). Developmental timing of housing mobility: Longitudinal effects on externalizing behaviors among at-risk youth. Journal of the American Academy of Child and Adolescent Psychiatry, 53(2), 199–208.
Gubits, D., Shinn, M., Bell, S., Wood, M., Dastrup, S., Solari, C. D., et al. (2015). Family options study: Short-term impacts of housing and services interventions for homelsss families. Washington, DC: U.S. Department of Housing and Urban Development.
Herbers, J. E., Cutuli, J. J., Supkoff, L. M., Heistad, D., Chan, C., Hinz, E., & Masten, A. S. (2012). Early reading skills and academic achievement trajectories of students facing poverty, homelessness, and high residential mobility. Educational Researcher, 41, 366–374.
Herman, D., Conover, S., Gorroochurn, P., Hinterland, K., Hoepner, L., & Susser, E. (2011). Randomized trial of critical time intervention to prevent homelessness after hospital discharge. Psychiatric Services, 62, 713–719.
Herman, D., Opler, L., Felix, A., Valencia, E., Wyatt, R., & Susser, E. (2000). A “critical time” intervention with mentally ill homeless men: Impact on psychiatric symptoms. Journal of Nervous and Mental Disease, 188, 135–140.
Jones, K., Colson, P. W., Holter, M. C., Lin, S., Valencia, E., Susser, E., et al. (2003). Cost-effectiveness of critical time intervention to reduce homelessness among persons with mental illness. Psychiatric Services, 54, 884–890.
Kilmer, R. R., Cook, J. R., Crusto, C., Strater, K. P., & Haber, M. G. (2012). Understanding the ecology and development of children and families experiencing homelessness: Implications for practice, supportive services, and policy. American Journal of Orthopsychiatry, 82(3), 389–401.
Kovacs, M. (1985). The children’s depression inventory. Psychopharmacology Bulletin, 21, 995–999.
MacKinnon, D. P., & Dwyer, J. H. (1993). Estimating mediated effects in prevention studies. Evaluation Review, 17, 144–158.
Masten, A. S., Cutuli, J. J., Herbers, J. E., Hinz, E., Obradović, J., & Wenzel, A. J. (2014). Academic risk and resilience in the context of homelessness. Child Development Perspectives, 8(4), 201–206.
Masten, A. S., Miliotis, D., Graham-Bermann, S. A., Ramirez, M., & Neemann, J. (1993). Children in homeless families: Risks to mental health and development. Journal of Consulting and Clinical Psychology, 61, 335–343.
Miller, P. (2011). A critical analysis of the research on student homelessness. Review of Educational Research, 81(3), 308–337.
Muller, D., Judd, C. M., & Yzerbyt, V. Y. (2005). When moderation is mediated and mediation is moderated. Journal of Personality and Social Psychology, 89, 852–863.
New Hampshire Dartmouth Psychiatric Research Center. (1995). Residential follow-back calendar. Lebanon, NH: Dartmouth Medical School.
Park, J. M., Metraux, S., Broadbar, G., & Culhane, D. P. (2004). Child welfare involvement among children in homeless families. Child Welfare, 83, 423–436.
Rafferty, Y., & Shinn, M. (1991). The impact of homelessness on children. American Psychologist, 46, 1170–1179.
Rafferty, Y., Shinn, M., & Weitzman, B. C. (2004). Academic achievement among formerly homeless adolescents and their continuously housed peers. Journal of School Psychology, 42, 179–199.
Raudenbush, S. W., & Bryk, A. S. (2002). Hierarchical linear models: Applications and data analysis methods (2nd ed.). Thousand Oaks, CA: Sage.
Rickel, A. U., & Biasatti, L. L. (1982). Modification of the block child rearing practices report. Journal of Clinical Psychology, 38, 129–134.
Riley, A. (2001). Effects on children of treating maternal depression. Baltimore: Bloomberg School of Hygiene and Public Health (Unpublished research instrument for study).
Seidman, E. (1991). Growing up the hard way: Pathways of urban adolescents. American Journal of Community Psychology, 19, 173–201.
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., et al. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychology, 59, 22–33.
Shinn, M., Schteingart, J. S., Williams, N. P., Carlin-Mathis, J., Bialo-Karagis, N., Becker-Klein, R., & Weitzman, B. C. (2008). Long-term associations of homelessness with children’s well-being. American Behavioral Scientist, 51, 789–810.
Shinn, M., Weitzman, B. C., Stojanovic, D., Knickman, J. R., Jimenez, L., Duchon, L., et al. (1998). Predictors of homelessness among families in New York City: From shelter request to housing stability. American Journal of Public Health, 88, 1651–1657.
Susser, E., Valencia, E., Conover, S., Felix, A., Tsai, W.-Y., & Wyatt, R. J. (1997). Preventing recurrent homelessness among mentally ill men: A “critical time” intervention after discharge from a shelter. American Journal of Public Health, 87, 256–262.
Tomita, A., & Herman, D. (2012). The impact of critical time intervention in reducing psychiatric rehospitalization after hospital discharge. Psychiatric Services, 63, 935–937.
Tsemberis, S., McHugo, G., Williams, V., Hanrahan, P., & Stefancic, A. (2007). Measuring homelessness and residential stability: The residential time-line follow-back inventory. Journal of Community Psychology, 35, 29–42.
Voight, A., Shinn, M. B., & Nation, M. (2012). The longitudinal effects of residential mobility on the academic achievement of urban elementary and middle school students. Educational Researcher, 41, 385–392.
Acknowledgments
The research reported here was funded by SAMHSA Grant 6 UD1 SM530654 and NIMH Grant 1 R01 MH0671484.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Shinn, M., Samuels, J., Fischer, S.N. et al. Longitudinal Impact of a Family Critical Time Intervention on Children in High-Risk Families Experiencing Homelessness: A Randomized Trial. Am J Community Psychol 56, 205–216 (2015). https://doi.org/10.1007/s10464-015-9742-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10464-015-9742-y