
Abstract
Experiencing a disaster has significant negative effects on psychological adjustment. Case study accounts point to two consistent trends in slowly-evolving environmental disasters: (a) patterns of negative social dynamics, and (b) relatively worse psychological outcomes than in natural disasters. Researchers have begun to explicitly postulate that the social consequences of slowly-evolving environmental disasters (e.g., community conflict) have their own effects on victims’ psychological outcomes. This study tested a model of the relationship between those social consequences and psychological adjustment of victims of a slowly-evolving environmental disaster, specifically those whose health has been compromised by the amphibole asbestos disaster in Libby, MT. Results indicate that experiencing greater community conflict about the disaster was associated with greater family conflict about the disaster which, in turn, was associated with greater social constraints on talking with others about their disease, both directly and indirectly through experiencing stigmatization. Experiencing greater social constraints was associated with worse psychological adjustment, both directly and indirectly through failed social support. Findings have implications for understanding pathways by which social responses create negative effects on mental health in slowly-evolving environmental disasters. These pathways suggest points for prevention and response (e.g., social support, stigmatization of victims) for communities experiencing slowly-evolving environmental disasters.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Two well-established findings in the larger disaster literature are: (a) experiencing a disaster has substantial negative consequences for psychological adjustment, and (b) these consequences are worse in disasters involving human culpability than in natural disasters (Baum 1991; Norris et al. 2002). Furthermore, evidence indicates that health threats need only be perceived, not substantiated, in order to have these long-lasting psychological consequences (e.g., Baum 1991). Historical and case study accounts of slowly-evolving environmental disasters (e.g., Love Canal, Centralia mine fire) point to (a) patterns of negative or toxic social dynamics emerging in communities that experience these disasters (e.g., Levine 1982; Kroll-Smith and Couch 1990; respectively), and (b) the likelihood of relatively worse psychological outcomes than in natural disasters (Norris et al. 2002). Only quite recently have researchers begun to explicitly postulate that social consequences of slowly-evolving environmental disasters have their own effects on psychological adjustment, whether direct or interactive with other disaster losses (e.g., physical health, economic) (e.g., Cline et al. 2009).
Based on prior research (e.g., Cline et al. 2010; Orom et al. 2012) in the Libby, Montana community, we developed a model for characterizing the components of the toxic social environment that emerged and relationships among them. Although scholars have made general and relatively consistent observations that community dynamics such as conflict and, less often cited, stigmatization of victims and their advocates, emerge in this type of disaster, the literature reflects little attempt to systematically observe and measure the impact of these dynamics on psychological adjustment. The present study does so. The present study tested a model of the influence of social dynamics during a slowly-evolving environmental disaster on psychological adjustment among people most vulnerable to the psychological impact of the disaster—those whose physical health has been compromised by toxic exposures, in this case, to Libby amphibole asbestos.
Premise: The Nature of the Disaster Matters
A key assumption of our research program is that different kinds of disasters create unique stressors and, thus, influence the nature of institutional, community, and public health and health care responses needed (see Cline et al. 2010; Cline et al. in press). The class of disasters represented in the present study is addressed by multiple names in the literature. The term slow-motion technological disasters (Cline et al. 2010; Hernandez and Sedler 2003) references the slow evolution of consequences (slow-motion) and human culpability (Baum et al. 1983a; Bolin 1993; Murphy 1985; Taylor 1991). The term chronic technological disasters (Couch and Kroll-Smith 1985; Kroll-Smith and Couch 1990) focuses on disasters’ slow and insidious development (Erikson 1994) while emphasizing their length (time from detection to ultimate consequences), difficult detection, and health risks (chronic), as well as human culpability (e.g. Baum et al. 1983b). The term ecological disaster (Havenaar 2002) focuses on human-caused disasters that profoundly affect actual and perceived human safety (Havenaar et al. 2002). Many toxic environmental exposures share these characteristics of difficult detection, human causality, and slowly-evolving and uncertain health consequences. Hereafter we use the term slowly-evolving environmental disaster to refer to this class of disasters.
Libby, MT: Epicenter of a Slowly-Evolving Environmental Disaster
Libby, a rural town in northwest Montana, has a population of about 10,000 within a four-mile radius (U.S. Census Bureau 2010). For decades, a vermiculite mine and two processing plants were operated locally; from 1963 until its closing in 1990, the mine was operated by W.R. Grace Company. Vermiculite from the mine was contaminated with a particularly toxic form of asbestos referred to as Libby amphibole asbestos (Whitehouse 2004).
In addition to the miners and processing plant workers, Libby residents were exposed to asbestos by dust brought home on workers’ clothes, ambient air, contaminated building materials and insulation, and the common practice of adding the asbestos-contaminated vermiculite to garden soil. Additional occupational exposures included providing contracted services to the mine (e.g., vending machine, truck maintenance) and harvesting and milling timber in the Libby area (Hart et al. 2007; Ward et al. 2006). Recent research indicates that lung disease can result from very low levels of exposure to Libby amphibole asbestos (U.S. Environmental Protection Agency (EPA) 2012). Due to the latency period for diagnosing asbestos-related disease (ARD) (from 10 to 40 years or longer; Whitehouse 2004; Wright et al. 2002), this disaster continues to unfold and its magnitude continues to grow.
Amphibole asbestos exposure is associated with increased risk for mesothelioma, lung cancer, pleural disease, and asbestosis, and appears to be associated with autoimmune disease (Noonan et al. 2006; Pfau et al. 2005) and gastrointestinal cancers (Frumkin and Berlin 1988). More than 400 have died from ARD in Libby (Center for Asbestos Related Disease (CARD), personal communication, April 2013). More than 30 cases of mesothelioma have been diagnosed in the Libby population (Whitehouse et al. 2008). Mesothelioma is an extremely rare, aggressive, and fatal cancer nearly always attributable to asbestos exposure (Bourdès et al. 2000; U.S. Cancer Statistics Working Group 2007), and in particular, to amphibole asbestos exposure (Agency for Toxic Substances and Disease Registry 2001; Boffetta and Trichopoulos 2002).
Beyond the physical health consequences of the disaster, our previous research revealed that community members with ARD had significantly worse psychological adjustment than family members of people with ARD and those with no personal experience with ARD (in themselves or their families) (Orom et al. 2008).
A Model for Understanding the Role of a Toxic Social Environment on Mental Health
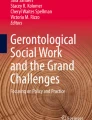
Only recently have researchers begun to make explicit theoretical propositions relating toxic social environments that emerge in slowly-evolving disasters to mental health outcomes (Cline et al. 2009; Palinkas 2012). Our model (see Fig. 1) predicts that community and family conflict, stigma, and failed social support play significant roles in directly and indirectly influencing psychological adjustment. We review relevant literature, including our previous research that provides the basis for the hypothesized pathways through which community conflict may influence psychological adjustment.

A model of hypothesized relationships among factors comprising a toxic social environment and psychological adjustment
Psychological Adjustment to Slowly-Evolving Environmental Disasters
Victims of slowly-evolving environmental disasters, like victims of natural disasters, are at risk for mental health problems (e.g., depression, anxiety, PTSD, distress) (Norris et al. 2002). For example, more than 43 % of victims of the Exxon Valdez oil spill, compared to 23 % of non-victims, had one or more psychological disorders (specifically depression, generalized anxiety disorder, or PTSD) one year after the oil spill (Palinkas et al. 1993). These psychological consequences persisted; six years later disaster victims had substantially higher than normative rates for depression, anxiety, and PTSD (Arata et al. 2000). Indeed, a review of studies assessing the psychological consequences of disasters invoking human culpability concluded that their psychological consequences are worse than for natural disasters (Norris et al. 2002). Few efforts have been made to create explanatory models of the causes of that poor adjustment to slowly-evolving environmental disasters (c.f., Palinkas 2012). None, to date, has focused on the condition that sets them apart from natural disasters, and thereby creates potentially worse negative psychological consequences for victims, that is, community conflict about the disaster.
Community and Family Conflict
Our model posits that community conflict about causes, consequences of, legitimacy of health threats from, appropriate responses to, and culpability for environmental disasters results in negative psychological adjustment among community residents. Community conflict has long been documented in environmental disasters (e.g., Cuthbertson and Nigg 1987; Kaniasty and Norris 2004). Reports from Love Canal (e.g., Levine 1982) and the Centralia mine fire (Couch and Kroll-Smith 1985) reflect a pattern of emergent social conflict about the seriousness, scope, and potential health consequences of those disasters. Erikson’s (1994) and Edelstein’s (2004) reviews from the Chernobyl and Legler (a case of groundwater contamination) report community conflict. In his analyses of what he calls “a new species of disaster,” Erikson suggests that this divisiveness creates an additional source of disaster-related trauma. In particular, Edelstein notes that community conflict affects families and those threats to social relationships, in turn, enhance people’s perceptions of the severity of the disaster. The resulting trauma of conflict can be so great that victims may experience “a loss of confidence in the scaffolding of family and community” (p. 242). Thus, understanding the full impact of slowly-evolving environmental disasters requires consideration of social processes, how the disaster wears—and tears at—the social fabric of the community via conflict processes.
The Libby community also has experienced widespread community- and family-level conflict as a result of the asbestos disaster (e.g., see Cline et al. 2010; Orom et al. 2012). In our previous focus group research, all of our participants (people with ARD, family members of people with ARD, and people with no personal experience with ARD) provided numerous and consistent accounts of disaster-related interpersonal conflict, including in their own families (Cline et al. 2010; Orom et al. 2012).
Participants with ARD recounted instances of disaster-related family conflict reflecting two relatively distinct patterns: open/conflictual and silent/conflictual (Orom et al. 2012). Participants in both the ARD and Family groups discussed family disagreements about the scope and seriousness of the health consequences of the asbestos exposure and the legitimacy of illness claims. An example of open family conflict was given by one ARD participant who said, “I had a brother-in-law that really bad-mouthed my wife, saying that she was fakin’ it.” Another example involved a man with ARD who had worked at the mine; after his children were diagnosed with ARD they blamed him for their illness. They said: “Look Dad, what you gave to us” (Orom et al. 2012). Conflict in other families was indicated by avoiding discussion about the legitimacy of the health threat in order to avoid arguing (see Orom et al. 2012). For example, a family member of a person diagnosed with ARD said, “But we just try not to, you know, get into discussions about it because there’s usually an argument…” Ample non-disaster related research supports the conclusion that interpersonal conflict, including family conflict, is associated with lower psychological well-being (e.g., Herrenkohl et al. 2012; Rook 1984; Sharma et al. 2010). We hypothesize that community conflict, mediated through family conflict, is associated with psychological adjustment, via the specific pathways described below.
Social Dynamics Associated with Stigma
Goffman (1963) defines stigma as an “attribute that is deeply discrediting” (p. 3). More than a personal characteristic, stigma denotes a type of relationship between those defined as “normal” and those “marked” as different and, thereby, deficient. Stigma leads to patterns of interpersonal communication between “mixed contacts” with significant negative consequences for the stigmatized (e.g., negative attitudes, avoidance, blame, character assassination; see Biernat and Dovidio 2000; Jones et al. 1984). In Libby, a well-established history of openly denigrating asbestos advocates (who themselves often have ARD) is evidenced in historical and documentary accounts of the disaster (see, e.g., Brown and Brown 2002; Carr and Hawes-Davis 2007; Schneider and McCumber 2004). The most vocal advocates have been cast, particularly by community members who do not have personal experience with ARD, as attention seekers (they often appear in news coverage) and as seeking financial gain (i.e., via lawsuits and settlements with W.R. Grace). People with ARD who witness this derisive treatment of advocates likely assume that they too will be the victims of stigmatizing responses from the community because of their disease.
In previous research, we demonstrated that discussions of stigma were common in focus groups of people with ARD, family members of people with ARD, and those with no personal experience with ARD (see Cline et al. 2010). (No significant differences, on the basis of experience with ARD, were found in the likelihood of discussing stigma.) In fact, among 70 categories coded in a social support analysis, the most commonly discussed topic was stigma (a barrier to support), accounting for more than one-fifth of all thought units related to social support.
Disease and disability often constitute the mark that results in individuals being labeled as “different” (de Monteflores 1993). Such is the case of ARD in Libby (see Cline et al. 2008b). Focus group members with ARD reflected both fear of being stigmatized by, and numerous personal accounts of stigmatizing responses from, community members (Cline et al. 2008b). They reported being cast as “not really sick” and being blamed for their illnesses. Discussions among family and non-ARD participants often associated people with ARD with frivolous lawsuits and blamed them for the economic decline of the community that occurred when W.R. Grace Company and other companies left the community. People with ARD were stigmatized as dishonest, lazy, lacking family values, and being “gold-diggers” (see Cline et al. 2008b).
The effects of conflict on psychological adjustment may be mediated by stigma. Both community and family conflict divide the social world into “us” and “them” and denigrate “them.” Some evidence also implicates family conflict in stigma (e.g., Badr and Taylor 2006; Miles et al. 2007). Given these dynamics, we hypothesize that conflict at both the community and family levels are associated with stigma. Stigma, in turn, is expected to be associated with psychological adjustment. Outside of the disaster literature, ample research indicates that being branded with, or identifying with, stigmatizing identities is associated with lower psychological well-being (Major and O’Brien 2005). Thus, we hypothesize that experiencing greater levels of stigma is directly associated with relatively worse psychological adjustment.
Social Constraints
Scholars have hypothesized that stigma can inhibit discussion about personal traumatic experiences, a phenomenon labeled “social constraints” (Lepore et al. 1996). Social constraints on disclosure are conditions that lead individuals to “refrain from or modify their disclosure of stress- or trauma-related thoughts, feelings or concerns” (Lepore and Revenson 2007, p. 315). Empirical research supports the association between experiencing stigma and perceiving social constraints (e.g., Chapple et al. 2004; Major and Gramzow 1999; Rzepa et al. 2011).
Evidence from our focus groups in Libby (Cline et al. 2008b) indicated that people with ARD felt the need to constrain discussions about their disease. Specifically, they appeared to avoid talking about their disease in order to avoid taking on a stigmatized identity. For example, one ARD participant recounted concealment of disease among best friends: “And there’s lots of people that are afraid to admit they have it to anyone… one of my best friends I saw her at Dr. Black’s office [at CARD] and I said, ‘Well, what are you doing here?’ And she said, ‘Well what are you doing here?’ And I said, ‘I have asbestos. What are you doing here?’ She said, ‘So am I.’ (whispered) Like it’s a secret.” Thus, based on the larger literature, and our previous research, we hypothesize that the experience of stigma associated with ARD predicts social constraints.
A wealth of previous research also indicates that the psychological wellbeing of people who have experienced trauma depends, at least in part, on processing that trauma with others (e.g., Belsher et al. 2012; Lepore et al. 2000). However, the ability to engage in that type of supportive interaction can be constrained because victims lack supportive others with whom they can talk or because they expect and receive negative responses (Lepore et al. 1996). Evidence of this dynamic was reported by an ARD participant in our previous research: “It’s very isolating. I have very few people I can speak about this disease with.” Thus, based on the larger literature, and our previous research (Cline et al. 2008b), we hypothesize that social constraints are directly related to failed social support.
Evidence indicates that social constraints have significant implications for psychological adjustment both directly (e.g., Belsher et al. 2012; Varni et al. 2012) and indirectly. We hypothesize that experiencing greater levels of social constraints is associated with worse psychological adjustment. Further, we hypothesize that social constraints are indirectly related to psychological adjustment through failed social support as described below.
Social Support
Ironically, as social constraints function to protect the stigmatized (by keeping a stigmatizing condition “secret”), they enhance personal risk by precluding access to potentially available social support. The stigmatized are left with a kind of “interpersonal roulette” in which disclosure is required to gain the social support needed, but disclosure of a stigmatizing illness may well result in rejection and ostracism (e.g., Cline and McKenzie 1996, 2000; Zacharioudakis 2001). In our previous research in Libby, people with ARD repeatedly reported negative consequences of disclosing their disease (see Cline et al. 2010; Cline et al. 2008b). Those experiences, and witnessing denigration of local advocates, made many with ARD wary of disclosing their disease status even to close friends (see Cline et al. 2010; Cline et al. 2008b). Social constraints may negatively affect psychological adjustment by reducing social support (c.f., Beals et al. 2009), perhaps by reducing opportunities for people to elicit social support. Thus, we hypothesize that the association between stigma and failed social support is mediated by social constraints.
A main theme in ARD discussions was social support losses in the asbestos disaster context (in stark contrast to evidence of widespread social support in their community in non-disaster related contexts) (Cline et al. 2006, 2008a, 2010). Evidence indicates that social support provides an ameliorative or protective role in psychological responses to both natural and human-caused disasters (Norris et al. 2002). Social support generally tends to be inversely associated with psychological outcomes such as distress, depression, and anxiety. Therefore, we hypothesize that social support losses contribute directly to negative psychological adjustment.
Summary of Hypotheses Regarding Psychological Adjustment
In summary, our model hypothesizes that five constructs (community conflict, family conflict, stigma, social constraints, and failed social support) account for a significant amount of variability in psychological adjustment to slowly-evolving environmental disasters. The model hypothesizes pathways through which community conflict affects psychological adjustment. See Fig. 1. The first set of hypotheses addresses the role of community conflict.
-
H1a: Those who experience a higher degree of community conflict experience a relatively higher degree of family conflict.
-
H1b: Those who experience a higher degree of community conflict experience relatively greater stigmatization.
-
H1c: Those who experience a higher degree of community conflict are relatively more socially constrained.
The second set of hypotheses addresses the role of family conflict.
-
H2a: Those who experience a greater degree of family conflict experience relatively greater stigmatization.
-
H2b: Those who experience a greater degree of family conflict are relatively more socially constrained.
The third set of hypotheses addresses the relationship between stigma and social constraints and psychological adjustment.
-
H3a: Those who experience a greater degree of stigma are relatively more socially constrained.
-
H3b: Those who experience a greater degree of stigma experience relatively worse psychological adjustment.
The fourth set of hypotheses addresses the relationship between social constraints and failed social support and psychological adjustment.
-
H4a: Those who are more socially constrained experience relatively worse psychological adjustment.
-
H4b: Those who are more socially constrained experience relatively greater failed social support.
The fifth hypothesis addresses the relationship between failed social support and psychological adjustment.
-
H5: Those who experience greater failed social support experience relatively worse psychological adjustment.
We tested our model of the role of the toxic social environment in psychological adjustment to slowly-evolving environmental disasters on the victims most vulnerable to the negative psychological consequences of a toxic social environment, those whose health has been compromised by the disaster.
Methods
Data analyzed in the present study were collected as part of a larger investigation, “The Voices of Libby” project, designed to quantitatively assess knowledge, attitudes, psychological responses, risk perceptions, pathways of exposure, and social processes associated with the Libby disaster. Data came from two sources: responses from 140 individuals diagnosed with ARD who completed surveys as part of a population-based sample, and 68 patients previously diagnosed with ARD from a sample drawn from CARD, a clinic dedicated solely to asbestos disease that has both a clinical and research mission. The study was reviewed and approved by the Institutional Review Board and the Protocol and Monitoring Committee affiliated with the first author’s institutions.
Sample/Participants
Community Sample
A total of 1,011 surveys were mailed to randomly-selected households in the Libby, MT zip code area. The cover letter for the survey asked that “the adult (21 years or older) who now lives there and has most recently celebrated his/her birthday” complete the survey. The response rate for the community sample was 52 % (n = 528). Of the 528 surveys, 140 were from people diagnosed with ARD.
CARD Patient Sample
One hundred surveys were mailed to randomly selected CARD patients who had been diagnosed with ARD and who had previously agreed to be contacted about research projects. The response rate for the patient sample was 69 % (n = 68).
Participant Characteristics
Of the 208 respondents, 125 (60.4 %) participants were male. The majority were married (71.6 %), non-Hispanic Whites (96.2 %) with an annual household income of less than $40,000 (71.9 %). About half (49.8 %) had completed high school. About a third (34.5 %) reported living alone, whereas the majority (58.6 %) reported having one or more adults (age 21 or older) living in the same household. The majority had some (34.6 %) or most (26.3 %) relatives living in the Libby area. The two samples did not differ significantly on any demographic characteristics. Table 1 summarizes participant characteristics.
Survey Instrument
The survey instrument included a cover letter that contained the elements of an Information Sheet and served as the informed consent document. Three forms of the survey booklet were created in order to control for effects of question order.
Measures
The instrument included items to measure (a) community conflict, (b) family conflict, (c) stigma, (d) social constraints, (e) failed social support, and (f) psychological adjustment.
Community Conflict
Based on focus group results, three items (α = .71) were designed to assess various domains of community conflict (e.g., responsibility for asbestos exposure). Respondents rated items on a scale from “1” (Totally Disagree) to “7” (Totally Agree). Items included: “The community is in conflict about asbestos issues;” and “The community is divided about who should be held responsible for residents’ asbestos exposure.”
Family Conflict
Based on focus group results, four items were designed to assess family conflict related to asbestos issues (α = .71). Respondents rated items on a scale from “1” (Totally Disagree) to “7” (Totally Agree). Items included: “Members of our family argue over asbestos-related issues;” and “Our family avoids talking about asbestos-related issues.”
Stigma
Three items were developed to assess stigmatizing social responses based on prior measures (Fife and Wright 2000; Wright et al. 2007) (α = .92). Respondents rated items on a scale from “1” (Totally Disagree) to “7” (Totally Agree). Items included, “I have been hurt by people’s reactions to learning that I have ARD;” and “I feel others avoid me because of my illness.”
Social Constraints
Social constraints were measured by four items from Lepore et al.’s (1996) measure of social constraints and one additional item (i.e., “I have hidden the fact that I have asbestos-related disease because I didn’t know how others would react”) (α = .91). Items included, “I felt that I needed to keep my feelings about my disease to myself because they made me feel uncomfortable” and “When I talked about my disease, others did not want to hear it.” Respondents rated items on a scale from “1” (Totally Disagree) to “7” (Totally Agree).
Failed Social Support
Failed social support was measured using three items that assessed needed but failed social support in the disaster context (α = .82). The items addressed three support functions—practical help, accurate information, and emotional support. Items included, “In the context of asbestos-related issues, I have needed but I didn’t get practical help (e.g., chores, transportation, food, money),” and “In the context of asbestos-related issues, I have needed but I didn’t get emotional support (e.g., listening, understanding, empathy).” Respondents rated items on a scale from “1” (Totally Disagree) to “7” (Totally Agree).
Psychological Adjustment
Psychological adjustment was assessed with single items for depression, anxiety, and stress (α = .91). Items included, “Because of asbestos-related issues, I often feel depressed;” and “I experience a lot of stress because of asbestos-related issues.” Respondents rated items on a scale from “1” (Totally Disagree) to “7” (Totally Agree). A higher value indicated worse psychological adjustment.
Procedures
Surveys were mailed to the community and patient samples. Following Dillman’s (1978, 2000) method, community-based promotion of the survey occurred via posters, radio announcements, and newspaper advertising and articles. Households or patients received numerous mailings (an announcement letter informing them of the survey, the actual survey and a pre-addressed stamped envelope and a bounce-back postcard, a second mailing of the survey to those who did not respond to the first mailing, and a “Thank You” reminder postcard). The bounce-back postcards (a) permitted tracking of completed responses, and (b) were used for drawings for gift certificates at a local grocery.
Analysis
Structural equation modeling (SEM) analysis was conducted using AMOS 20.0 to test the hypothesized relationships (see Fig. 1). To evaluate the hypothesized research model, the following commonly used indices of model fit were examined: χ 2, the degrees of freedom (df), comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Because χ 2 values are sensitive to the sample size (Kline 1998), the ratio of χ 2 to degree of freedom was assessed. When the ratio is less than 5, it is conventionally accepted as a good fit (Wheaton et al. 1977). To judge model fit, Hu and Bentler’s (1999) joint criteria approach was used: CFI ≥ .96 and SRMR ≤ .10 or RMSEA ≤ .06 and SRMR ≤ .10.
For most variables the number of missing values was low (less than 10 of 208 responses). The number of missing values ranged between 2 and 27 across all measures. Missing values were imputed with the use of maximum likelihood estimation available in AMOS 20.0. Normality, kurtosis, and skewness were acceptable for all variables. Prior to SEM analysis, a bivariate correlation analysis was conducted to check for multicollinearity among independent variables. No two variables yielded correlation coefficient values greater than .70, indicating no significant multicollinearity problems.
Results
Structural Model Testing
Maximum likelihood estimation was employed to estimate the hypothesized research model. The χ 2 was significant for the hypothesized model, χ 2 (180) = 316.6, p < .001; but the ratio of χ 2 to df was acceptable at 1.77 (316.6/179). Overall the model showed an adequate fit of the data with CFI = .95, RMSEA = .06, and SRMR = .06.
Hypothesis Testing
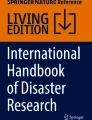
Figure 2 presents results for hypothesis testing from the SEM analysis. The measurement model is not shown for ease and clarity of understanding. The first set of hypotheses examined the role of community conflict. We predicted that those who experience greater community conflict experience greater family conflict. That association was significant (β = .44, p < .001). Thus, H1a was supported. We also predicted that those who experience greater community conflict are relatively more stigmatized (H1b) and socially constrained (H1c). Results did not support H1b (β = .12, p = .20) and H1c (β = .06, p = .38).

SEM results for the model of hypothesized relationships among factors comprising a toxic social environment and psychological adjustment. Note **p < .01; ***p < .001; df = degree of freedom; CFI comparative fit index, RMSEA root mean square error of approximation, SRMR standardized root mean square residual. Solid lines indicate statistically significant paths whereas dotted lines indicate non-statistically significant paths. Reported values are standardized coefficients
The second set of hypotheses proposed that those who experience greater family conflict are relatively more socially constrained (H2a) and stigmatized (H2b). Both hypotheses were supported. Family conflict was a significant predictor of both stigma (β = .53, p < .001) and social constraints (β = .26, p < .01).
The third set of hypotheses predicted that those who experience more stigma as a result of ARD are more socially constrained (H3a) and experience worse psychological adjustment (H3b). Analyses showed that stigma was significantly and positively associated with social constraints (β = .59, p < .001). Thus, H3a was supported. However, stigma was not a significantly associated with psychological adjustment (β = .12, p = .028). Therefore, H3b was not supported.
The fourth set of hypotheses investigated the association between social constraints, failed social support, and psychological adjustment. We predicted that psychological adjustment is worse for those who are more socially constrained (H4a). We proposed that those who are more socially constrained would report greater failed social support (H4b). Analyses supported both H4a and H4b. That is, social constraints were significantly associated with both psychological adjustment (β = .34, p < .01) and failed social support (β = .50, p < .001).
Finally, the fifth hypothesis predicted that those who report greater failed social support experience worse psychological adjustment. Results showed that failed social support was significantly associated with psychological adjustment (β = .21, p < .01). Thus, H5 was supported.
The direct, indirect, and total effects of each predictor on each outcome variable are shown in Table 2. Greater community conflict was associated with worse psychological adjustment, mediated by a pathway that included family conflict, social constraints, stigma, and failed support. Specifically, community conflict was associated with family conflict and family conflict was associated with social constraints directly, and indirectly through stigma. The association between stigma and social support was mediated through social constraints. Social constraints, in turn, were associated with psychological adjustment both directly, and indirectly through failed social support.
Discussion
This study builds on previous research conducted in the Libby, MT community, the larger literature on the social processes associated with serious chronic illness (e.g., stigma, social constraints, and social support) and their associations with psychological consequences of those illnesses, and the larger literature regarding social dynamics associated with slowly-evolving environmental disasters. Our previous research (Cline et al. 2010; Orom et al. 2012) identified conflict, stigma, and failed social support as the key social dynamics emerging in communities experiencing slowly-evolving environmental disasters. These share some commonality with the community dynamics identified by Palinkas (2012) as driving significant psychiatric, physical health, and behavioral outcomes of oil spills. Although these dynamics, particularly conflict, have been observed in case studies of other slowly-evolving disasters, little research has attempted to systematically measure these social dynamics during an ongoing disaster. In this study, we attempted to measure the community’s social dynamics and to assess relationships among them as well as their relationships with psychological adjustment. Results clarify likely paths whereby a community’s social environment influences mental health.
Key Contributions
Results support the conclusion that in a slowly-evolving environmental disaster, key elements of the community’s social dynamics function to create a toxic social environment. Taken together, the results provide a coherent model to explain previously fragmented explanations of the role of the components of the social environment in responses to slowly-evolving environmental disasters.
Conflict was the most commonly identified social dynamic associated with slowly-evolving disasters in previous research. The disaster literature generally has addressed “conflict” or “social conflict” and thus seemed to imply conflict broadly-conceived at a community level. However, present results paint community conflict as “the triggering dynamic” in a cascade of social dynamics associated with psychological adjustment, rather than a factor directly associated with psychological adjustment. Community conflict was not directly associated with stigmatizing dynamics or social constraints, as had been predicted. However, our measure of community conflict was brief and thus may have failed to capture experiences of community conflict that are associated with stigma or social constraints.
Despite this, community conflict played a key role in psychological adjustment through its role in heightened family conflict. Community conflict may be associated with family conflict because disagreement about the causes, consequences and culpability for the disaster take place in the context of interpersonal relationships, including family relationships. We previously noted that families affected by asbestos-related disease reported arguments about the causes of disease, discrediting and alienating of victims, and family silence around the disease (Orom et al. 2012).
Just as individuals use private narratives to make sense of traumatic events, communities engage discursively in meaning making about traumatic events, including disasters (Mohatt et al. 2014). Emergent public narratives can promote resilience by strengthening group identity, sustaining cultural coherence and continuity, and representing memories of overcoming adversity (Mohatt et al. 2014); but they can also transmit unresolved psychological trauma from generation to generation (Braveheart et al. 2011; Whitbeck et al. 2004).
In Libby, two irreconcilable public narratives emerged about the causes and consequences of the Libby disaster. Some community members depict the disaster as a story of corporate greed and government betrayal, the perceived consequence of which is a growing list of dreaded illnesses affecting the longevity and quality of life of those who have lived in Libby and among generations to come. Other community members depict the disaster as a story of individual greed, where opportunistic residents are taking advantage of an uncertain health threat to win settlement money at the expense of the town’s reputation as a safe place to live and work. In this narrative, the real disaster is measured by the financial cost of lost property values and jobs, losses perceived to be associated with publicity about asbestos exposure. Cox and Perry’s (2011) analysis of two communities affected by a catastrophic wildfire in British Columbia, Canada, provides another example of competing public narratives. The dominant narrative of the fire was that residents were able to efficiently recover by overcoming material and economic setbacks. This narrative gained traction, in part, because private and governmental disaster response strategies prioritized distribution of goods and financial resources. However, other residents also told stories of greater suffering and loss of identity and social support, although their experiences tended to be subjugated to the dominant narrative. Both case studies illustrate the multivocality of public narratives. The community conflict observed so frequently in slowly-evolving environmental disasters may be reciprocally related to the development of irreconcilable narratives which feed further community conflict. The narratives also illustrate representations of the disasters as opportunities for growth or reflecting a deep pool of unresolved grief or anger.
In creating our model, we considered stigmatizing social processes. We assessed both the experience of being stigmatized and social constraints, the latter typically considered a social by-product of having a stigmatizing condition. Much stigma literature attributes negative mental health outcomes directly to stigma. In contrast, in our model, stigma was indirectly associated with psychological adjustment. Stigma’s association with psychological adjustment was mediated by social constraints. This finding suggests the importance of considering the intervening role of social constraints in psychological responses to slowly-evolving disasters.
Interventions to improve psychological adjustment that focus on altering stigmatizing communication from others or changing others’ stigmatizing stereotypes may be inadequate if, indeed, the stigmatized person’s concealment and defensive posture toward others is driving his/her negative psychological consequences. Certainly more research is needed to assess the relative roles of stigma and social constraints in psychological adjustment. If further research confirms the present findings, then in addition to targeting stigmatizing communication by others, interventions to improve psychological adjustment might focus on enabling those with stigmatizing conditions to identify potentially compassionate disclosure targets and to selectively disclose and discuss their conditions accordingly, rather than being generally open or generally closed regarding their condition. Such a strategy might facilitate access to social support.
Written emotional disclosure can buffer the negative psychological effects of social constraints on psychological distress (Zakowski et al. 2004). Although therapeutic journaling may be an effective individual-level intervention for those experiencing slowly-evolving environmental disasters, more ideally, a community-level intervention could encourage more open sharing of victims’ challenges and needs and thereby have the potential to reduce the very stigmatizing responses that victims may be trying to avoid via social constraints. For example, using Photovoice, people develop narrative explanations of personally significant visual images, engage in self-reflection and community discourse and change in the process (Catalani and Minkler 2010; Wang and Burris 1997). Participants in Photovoice have been found to engage in deep self-reflection, gain an increased sense of control over their lives, and feel empowered to make change in their communities (Foster-Fishman et al. 2005). A randomized controlled trial of an anti-stigma Photovoice intervention for a population using psychiatric services combined the Photovoice process with education about stigma and reduced self-stigma, increased coping with stigma, and increased community activism (Russinova et al. 2014). Photovoice has been used with women with HIV/AIDS, demonstrating that stigmatized groups are empowered by and can participate in Photovoice while protecting their public identities (Teti et al. 2012, 2013). A strategy such as Photovoice, could provide a safe environment for confronting diverse perspectives and creating empowering narratives (Foster-Fishman et al. 2005).
Through Photovoice, disaster victims could represent their experiences to themselves and others, elicit empathic responses in community audiences, and potentially reduce both stigmatization and social constraints on the part of victims. Future research might explore whether Photovoice, perhaps in combination with education about stigma, might be an effective community-level intervention in slowly-evolving environmental disasters to reduce stigmatization of victims, reduce social constraints among victims, and decrease community and interpersonal conflict. That said, public discourse about a slowly-evolving environmental disaster also has the potential to provide a platform for exacerbating conflict; therefore, any intervention would need to be carefully pilot-tested to ensure avoidance of unintended harmful effects.
One of the best established findings in the larger disaster literature, echoed in accounts of slowly-evolving environmental disasters, including our prior research (see Cline et al. 2010), is the critical role of social support in psychological adjustment among disaster victims (see Norris et al. 2002). Despite this well-established finding, relatively little is known about factors that facilitate or impede provision of social support in this context. Literature points to failed or reduced social support responses within the community as characteristic in slowly-evolving disasters (e.g., Cline et al. 2010; Palinkas 2012) rather than the emergent altruistic community often found in response to natural disasters (Cuthbertson and Nigg 1987; Kaniasty and Norris 2004). Present results indicated a direct relationship between failed social support and psychological adjustment. However, social constraints had a more powerful direct effect than did failed social support on psychological adjustment, along with an indirect effect mediated by failed social support.
In summary, relative to prior literature on responses to slowly-evolving environmental disasters, present results cast light especially on family-level conflict and social constraints as playing potentially important roles in mental health outcomes. To the extent that these findings are replicated by future research, strategies for responding to mental health issues associated with slowly-evolving environmental disasters might include assessing the following as risk factors: (a) individuals whose families and/or interpersonal networks are at greatest risk for conflict and (b) individuals who resist discussing their health issues and related needs.
Implications
The EPA has called the Libby situation the worst environmental disaster in U.S. history (Sullivan 2007). This disaster likely mirrors the kinds of social environment that evolved at Love Canal, in Centralia, and at potentially numerous other sites involving environmental disasters and, especially Superfund sites. Today, nearly half of the country’s population lives within 10 miles of designated or proposed Superfund sites, sites designated for cleanup due to public health consequences of toxic exposure (Sapien 2007; see Edelstein 2004). We have argued that different types of disasters require different kinds of responses. Current models for disaster responses, based on rapid-onset disasters, do not apply well to slowly-evolving disasters. Our research may contribute to building a comprehensive response model by accounting for the social environmental factors that particularly enhance risk in this type of disaster. At a minimum, this research should alert responders—agency, community, and health care—of the potentially toxic social environment and its mental health risks for the most fragile victims, those whose health has been compromised by the disaster.
Limitations and Implications for Future Research
The present study is a snapshot in time. We assessed the social environmental factors at one point in time. Thus, we cannot infer causality from our results. A longitudinal study would clarify causal relationships in our conceptual model.
Although the sample included only people with ARD, they likely varied substantially in disease severity and in the degree to which their disease is progressive. Based on research on chronic illnesses in general, we would expect that disease severity has a direct effect on psychological adjustment. We also expect that the factors comprising the toxic social environment may moderate that effect. That is, we suspect that as disease severity worsens, the social environment plays an exacerbating role in mental health outcomes. A longitudinal study would enable us to address this hypothesized relationship.
The relationship between psychological co-morbidities and disease status has not been studied in people with ARD. However, depression and anxiety are associated with exacerbations and worse prognosis, including increased risk for death, in people with COPD (Atlantis et al. 2013). The same may be true for ARD; therefore, in the absence of curative medical interventions for ARD (American Thoracic Society 1990; Boffetta and Trichopoulos 2002), addressing psychological co-morbidity may be an important strategy for helping people with ARD to maintain physical functioning and quality of life.
Some research has identified prevalence of autoimmune disorders as associated with exposure to the Libby amphibole asbestos (e.g., Pfau et al. 2005). Pfau and colleagues’ research opens the door to speculation that pleural disease itself, the most common health consequence of exposure to the Libby amphibole asbestos might possibly be an autoimmune response. Because stress plays a role in autoimmune responses, and the toxic social environment we discovered is likely a profound stressor in the Libby community, future longitudinal work should at least explore the possibility that the larger social environment may actually influence disease severity. Research on other diseases, including asthma (e.g., Williams et al. 2009; Wright 2011), has supported the conclusion that a stressful social environment may have important physical health consequences in addition to mental health consequences.
In our present research we identified social processes that contribute to worse psychological adaptation in people whose health has been negatively affected by a slowly-evolving environmental disaster; our approach was rooted in our focus group participants’ narratives that repeatedly and consistently focused on toxic social processes. However, intervention might also be informed by identifying factors that protect and/or promote psychological adjustment. Other researchers have given considerable attention to community resources and strengths that might increase the capacity for adapting to disasters (e.g., Almedom and Tumwine 2008; Castleden et al. 2011; Norris et al. 2008; O’Sullivan et al. 2013). This resilience paradigm commonly has been applied to natural and rapid-onset human-caused disasters, but not to slowly-evolving environmental disasters (c.f., Aronoff and Gunter 1992); the latter are widely-recognized as having distinct social dynamics (e.g., Couch and Kroll-Smith 1985, Cuthbertson and Nigg 1987; Kaniasty and Norris 2004; Levine 1982). Community resilience refers to a community’s ability to adapt to, and thrive after a disruption or crisis such as a natural disaster (Leykin et al. 2013; Norris et al. 2008). According to Norris and colleagues, community resilience is supported by four multidimensional “adaptive capacities:” economic development and diversity, social capital, a solid and trusted communication infrastructure, and community competence.
In future research we might examine if components of social capital, the resources available to individuals and communities as a result of social networks (Bourdieu 1986), or community competence, communities’ skills, and confidence to engage in collective problem solving (Norris et al. 2008) can buffer against community conflict that typically emerges in slowly-evolving environmental disasters. For example, community conflict might be partially prevented in communities wealthy in grassroots social capital and a history of cooperation among organizations to achieve common purposes. In this case, interconnectedness and trust might limit inter-organizational conflict and give community members greater say in the recovery process which can be dominated by outside organizations and uninformed by local knowledge (Couch and Coles 2011). Similarly, communities high in community competence, including collective efficacy for overcoming community challenges should be more capable of coordinating a collective response to protect citizens. The willingness of local government to establish clear priorities and act on behalf of the health and well-being of citizens presumably would be a critical determinant of resilience (Leykin et al. 2013) and an important element of community competence. Based primarily on analysis of local newspaper stories and interviews with key informants, Aronoff and Gunter (1992) argued that efficient and effective government problem-solving stemmed off community conflict in Gratiot County, MI, upon the discovery of PBB contamination in that region. As there has been little application of the resilience paradigm to slowly-evolving environmental disasters, future work on the social dynamics of this class of disasters might test the role of communities’ adaptive capacities in buffering community conflict and possibly having positive downstream effects on psychological adjustment among disaster victims.
The present study highlighted the importance of family conflict in the social environment that contributes to issues in psychological adjustment. However, we did not have a baseline measure of family functioning. One possibility is that families’ experience of disaster-related conflict is driven by previously established patterns of family conflict—and thus the disaster and associated community-level conflict simply exacerbate already existing dynamics. Future research should include baseline assessments of family functioning. Further, families do not constitute the only probable source of interpersonal conflict or, in contrast, compassionate responses to disclosure and social support. Future research should consider the role of conflict among friends and members of faith communities as well.
Finally, some measures in the present study were limited in length due to the fact that questions were asked as part of a much larger survey that assessed a wide array of disaster-related variables. However, single-item measures of psychological adjustment (i.e., depression, anxiety, and stress) can have strong validity and good sensitivity and are particularly useful in clinical diagnostic contexts where lengthy measures may not be feasible (Ayalon et al. 2010; Connor et al. 2007; Elo et al. 2003). Both more robust measures (e.g., failed social support, psychological adjustment) and more reliable measures (e.g., community conflict, family conflict) would likely strengthen results and should be developed and used in future longitudinal research.
References
Agency for Toxic Substances and Disease Registry. (2001). Toxicological profile for asbestos (update). Atlanta, GA: U.S. Department of Health and Human Services.
Almedom, A. M., & Tumwine, J. K. (2008). Resilience to disasters: A paradigm shift from vulnerability to strength. African Health Sciences, 8, S1–S4.
American Thoracic Society. (1990). Health effects of tremolite. The American Review of Respiratory Disease, 142, 1453–1458.
Arata, C. M., Picou, S., Johnson, G. D., & McNally, T. S. (2000). Coping with technological disaster: An application of the conservation of resources model to the Exxon Valdez oil spill. Journal of Traumatic Stress, 13, 23–39.
Aronoff, M., & Gunter, V. (1992). It’s hard to keep a good town down: Local recovery efforts in the aftermath of toxic contamination. Organization & Environment, 6, 83–97.
Atlantis, E., Fahey, P., Cochrane, B., & Smith, S. (2013). Bidirectional associations between clinically relevant depression or anxiety and chronic obstructive pulmonary disease (COPD): A systematic review and meta-analysis. Chest, 144, 766–777. doi:10.1378/chest.12-1911.
Ayalon, L., Goldfracht, M., & Bech, P. (2010). ‘Do you think you suffer from depression?’ Reevaluating the use of a single item question for the screening of depression in older primary care patients. International Journal of Geriatric Psychiatry, 25, 497–502. doi:10.1002/gps.2368.
Badr, H., & Taylor, C. L. C. (2006). Social constraints and spousal communication in lung cancer. Psycho-Oncology, 15, 673–683.
Baum, A. (1991). Toxins, technology, and natural disasters. In G. R. VamdenBos & B. K. Bryant (Eds.), Cataclysms, crises, and catastrophes: Psychology in action (pp. 9–53). Washington, DC: American Psychological Association.
Baum, A., Fleming, R., & Davidson, L. M. (1983a). Natural disaster and technological catastrophe. Environment and Behavior, 15, 333–354.
Baum, A., Gatchel, R. J., & Schaeffer, M. A. (1983b). Emotional, behavioral, and physiological effects of chronic stress at Three Mile Island. Journal of Consulting and Clinical Psychology, 51, 365–372.
Beals, K. P., Peplau, L. A., & Gable, S. L. (2009). Stigma management and well-being: The role of perceive social support, emotional processing, and suppression. Personality and Social Psychology Bulletin, 35, 867–879. doi:10.1177/0146167209334783.
Belsher, B. E., Ruzek, J. I., Bongar, B., & Corova, M. J. (2012). Social constraints, posttraumatic cognitions, and posttraumatic stress disorder in treatment-seeking trauma survivors: Evidence for a social-cognitive processing model. Psychological Trauma: Theory, Research, Practice, and Policy, 4, 386–391. doi:10.1037/a0024362.
Biernat, M., & Dovidio, J. F. (2000). Stigma and stereotypes. In T. F. Heatherton, R. E. Kleck, M. R. Hebl, & J. G. Hull (Eds.), The social psychology of stigma (pp. 88–125). New York, NY: The Gilford Press.
Boffetta, P., & Trichopoulos, D. (2002). Cancer of the lung, larynx, and pleura. In H. Adami, D. Hunter, & D. Trichopoulos (Eds.), Textbook of cancer epidemiology (pp. 248–280). New York: Oxford University Press.
Bolin, R. (1993). Natural and technological disasters: Evidence of psychopathology. In A.-M. A. Ghadirian & H. E. Lehmann (Eds.), Environment and psychopathology (pp. 121–140). New York: Springer.
Bourdès, V., Boffetta, P., & Pisani, P. (2000). Environmental exposure to asbestos and risk of pleural mesothelioma: Review and meta-analysis. European Journal of Epidemiology, 16, 411–417.
Bourdieu, P. (1986). The forms of capital. In J. G. Richardson (Ed.), Handbook of theory and research for the sociology of education (pp. 241–258). New York: Greenwood Press.
Braveheart, M. Y. H., Chase, J., Elkins, J., & Altschul, D. B. (2011). Historical trauma among indigenous peoples of the Americas: Concepts, research, and clinical considerations. Journal of Psychoactive Drugs, 43, 282–290.
Brown, M., & Brown, K., (Producers) & Brown, M. (Director). (2002). Dust to dust [Motion picture]. Arlington, TX: Michael Brown Productions, Inc.
Carr, D. G., & Hawes-Davis, D. (Producers and Directors). (2007). Libby, Montana [Motion picture]. Missoula, MT: High Plains Films.
Castleden, M., McKee, M., Murray, V., & Leonardi, G. (2011). Resilience thinking in health protection. Journal of Public Health, 33, 369–377. doi:10.1093/pubmed/fdr027.
Catalani, C., & Minkler, M. (2010). Photovoice: A review of the literature in health and public health. Health Education and Behavior, 37, 424–451. doi:10.1177/1090198109342084.
Chapple, A., Ziebland, S., & McPherson, A. (2004). Stigma, shame, and blame experienced by patients with lung cancer: Qualitative study. BMJ, 328, 1470–1473.
Cline, R. J. W., Berry-Bobovski, L., Coleman, D. K., Silk, K. J., Hernandez, T., Black, B., Schwartz, A., & Ruckdeschel, J. C. (2006, November). When everyone needs help: Social support processes associated with a slow-motion technological disaster. Presented at the annual meeting of the American Public Health Association, Boston, MA.
Cline, R. J. W., & McKenzie, N. J. (1996). HIV/AIDS, women, and threads of discrimination: A tapestry of disenfranchisement. In E. B. Ray (Ed.), Communication and disenfranchisement: Social health issues and implications (pp. 365–386). Mahwah, NJ: Erlbaum.
Cline, R. J. W., & McKenzie, N. J. (2000). Interpersonal roulette and HIV/AIDS as disability: Stigma and social support in tension. In D. O. Braithwaite & T. L. Thompson (Eds.), Handbook of communication and people with disabilities: Research and application (pp. 467–483). Mahwah, NJ: Erlbaum.
Cline, R. J. W., Orom, H., Berry-Bobovski, L., Hernandez, T., Black, C. B., Schwartz, A. G., et al. (2010). Community-level social support responses in a slow-motion technological disaster: The case of Libby, Montana. American Journal of Community Psychology, 46, 1–18. doi:10.1007/s10464-010-9329-6.
Cline, R. J. W., Orom, H., Berry-Bobovski, L., Sayir, A., Hernandez, T., Black, B., et al. (2008a, October). Social support processes during a slow-motion technological disaster: The deterioration of a previously altruistic community. Presented at the annual meeting of the National Communication Association, San Diego, CA.
Cline, R. J. W., Orom, H., Child, J., Hernandez, T., & Black, B. (in press). Social support functions during a slowly-evolving environmental disaster: The case of amphibole asbestos exposure in Libby, Montana. Health Communication.
Cline, R. J. W., Orom, H., Hernandez, T., Black, B., Berry-Bobovski, L., Schwartz, A. G., et al. (2009, November). Toxic social environments: A model for understanding and responding to slow-motion technological disasters based on the case of amphibole-asbestos exposure in Libby, Montana. Presented at the annual meeting of the American Public Health Association, Philadelphia, PA.
Cline, R. J. W., Orom, H., Sayir, A., Berry-Bobovski, L., Silk, K. J., Broadway, S. C., et al. (2008b, October). Us-them relationships in a slow-motion technological disaster. Dynamics and consequences of stigma associated with asbestos-related disease in Libby, MT. Presented at the annual meeting of the American Public Health Association, San Diego, CA.
Connor, K. M., Vaishnavi, S., Davidson, J. R., Sheehan, D. V., & Sheehan, K. H. (2007). Perceived stress in anxiety disorders and the general population: A study of the Sheehan stress vulnerability scale. Psychiatry Research, 151, 249–254.
Couch, S. R., & Coles, C. J. (2011). Community stress, psychosocial hazards, and EPA decision-making in communities impacted by chronic technological disasters. Environmental Justice, 101(S1), S140–S148. doi:10.2105/AJPH.2010.300039.
Couch, S. R., & Kroll-Smith, J. S. (1985). The chronic technical disaster: Toward a scientific perspective. Social Science Quarterly, 66, 564–575.
Cox, R. S., & Perry, K.-M. E. (2011). Like a fish out of water: Reconsidering disaster recovery and the role of place and social capital in community disaster resilience. American Journal of Community Psychology, 48, 395–411. doi:10.1007/s10464-011-9427-0.
Cuthbertson, B. H., & Nigg, J. M. (1987). Technological disaster and the nontherapeutic community. Environment and Behavior, 19, 462–483.
de Monteflores, C. (1993). Notes on the management of difference. In L. D. Garnets & D. C. Kimmel (Eds.), Psychological perspectives on lesbian and gay male experiences (pp. 218–247). New York, NY: Columbia University Press.
Dillman, D. A. (1978). Mail and telephone surveys: The total design method. New York, NY: John Wiley & Sons.
Dillman, D. A. (2000). Mail and internet surveys: The tailored design method (2nd ed.). New York, NY: John Wiley & Sons.
Edelstein, M. R. (2004). Contaminated communities: Coping with residential toxic exposure (2nd ed.). Cambridge, MA: Westview Press.
Elo, A.-L., Leppänen, A., & Jahkola, A. (2003). Validity of a single-item measure of stress symptoms. Scandinavian Journal of Work, Environment & Health, 29, 444–451.
Erikson, K. (1994). A new species of trouble: Explorations in disaster, trauma, and community. New York: W. W. Norton.
Fife, B. L., & Wright, E. R. (2000). The dimensionality of stigma: A comparison of its impact on the self of persons with HIV/AIDS and cancer. Journal of Health and Social Behavior, 41, 50–67.
Foster-Fishman, P., Nowell, B., Deacon, Z., Nievar, M. A., & McCann, P. (2005). Using methods that matter: The impact of reflection, dialogue, and voice. American Journal of Community Psychology, 36, 275–291.
Frumkin, H., & Berlin, J. (1988). Asbestos exposure and gastrointestinal malignancy review and meta-analysis. American Journal of Industrial Medicine, 14, 79–95.
Goffman, E. (1963). Stigma: Notes on the management of spoiled identity. New York, NY: Simon & Schuster Inc.
Hart, J. F., Ward, T. J., Spear, T. M., Crispen, K., & Zolnikov, T. R. (2007). Evaluation of asbestos exposures during firewood-harvesting simulations in Libby, MT, USA—Preliminary data. Annals of Occupational Hygiene, 51, 717–723. doi:10.1093/annhyg/mem052.
Havenaar, J. M. (2002). Ecological disaster: A concern for the future. In J. M. Havenaar, J. G. Cwikel, & E. J. Bromet (Eds.), Toxic turmoil: Psychological and societal consequences of ecological disasters (pp. 3–18). New York: Kluwer Academic/Plenum Publishers.
Havenaar, J. M., Cwikel, J. G., & Bromet, E. J. (2002). Epilogue: Lessons learned and unresolved issues. In J. M. Havenaar, J. G. Cwikel, & E. J. Bromet (Eds.), Toxic turmoil: Psychological and societal consequences of ecological disasters (pp. 259–271). New York: Kluwer Academic/Plenum Publishers.
Hernandez, T., & Sedler, L. (2003). Addressing the psychosocial elements of slow-motion technological disasters [training manual]. Libby, MT: Center for Asbestos Related Disease.
Herrenkohl, T. I., Lee, J. O., Kosterman, R., & Hawkins, J. D. (2012). Family influences related to adult substance use and mental health problems: A developmental analysis of child and adolescent predictors. Journal of Adolescent Health, 51(2), 129–135.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariances structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55.
Jones, E. E., Farina, A., Hastorf, A. H., Marhus, H., Miller, D. T., & Scott, R. A. (1984). Social stigma: The psychology of marked relationships. New York: W. H. Freeman and Company.
Kaniasty, K., & Norris, F. H. (2004). Social support in the aftermath of disasters, catastrophes, and acts of terrorism: Altruistic, overwhelmed, uncertain, antagonistic, and patriotic communities. In R. J. Ursano, A. E. Norwood, & C. S. Fullerton (Eds.), Bioterrorism: Psychological and public health interventions (pp. 200–229). Cambridge: Cambridge University Press.
Kline, L. B. (1998). Principles and practice of structural equation modeling. New York: Guilford.
Kroll-Smith, S., & Couch, S. R. (1990). The real disaster is above ground: A mine fire and social conflict. Lexington, KY: The University of Kentucky Press.
Lepore, S. J., Ragan, J. D., & Jones, S. (2000). Talking facilitates cognitive–emotional processes of adaptation to an acute stressor. Journal of Personality and Social Psychology, 78, 499–508. doi:10.1037/0022-3514.78.3.499.
Lepore, S. J., & Revenson, T. A. (2007). Social constraints on disclosure and adjustment to cancer. Social and Personality Psychology Compass, 1, 313–333. doi:10.1111/j.1751-9004.2007.00013.x.
Lepore, S. J., Silver, R. C., Wortman, C. B., & Wayment, H. A. (1996). Social constraints, intrusive thoughts, and depressive symptoms among bereaved mothers. Journal of Personality and Social Psychology, 70, 271–282.
Levine, A. G. (1982). Love canal, science, politics, and people. Lexington, MA: Lexington Books.
Leykin, D., Lahad, M., Cohen, O., Goldberg, A., & Aharonson-Daniel, L. (2013). Conjoint community resiliency assessment measure-28/10 items (CCRAM28 and CCRAM10): A self-report tool for assessing community resilience. American Journal of Community Psychology, 52, 313–323. doi:10.1007/s10464-013-9596-0.
Major, B., & Gramzow, R. H. (1999). Abortion as stigma: Cognitive and emotional implications of concealment. Journal of Personality and Social Psychology, 77, 735–745. doi:10.1037/0022-3514.77.4.735.
Major, B., & O’Brien, L. T. (2005). The social psychology of stigma. Annual Review of Psychology, 56, 393–421.
Miles, M. S., Holditch-Davis, D., Pederson, C., Eron, J., Jr, & Schwartz, T. (2007). Emotional distress in African American women with HIV. Journal of Prevention & Intervention in the Community, 33, 35–50.
Mohatt, N. V., Thompson, A. B., Thai, N. D., & Tebes, J. K. (2014). Historical trauma as public narrative: A conceptual review of how history impacts present-day health. Social Science and Medicine, 106, 128–136. doi:10.1016/j.socscimed.2014.01.043.
Murphy, S. A. (1985). The conceptual bases for disaster research and intervention. In J. Laube & S. A. Murphy (Eds.), Perspectives on disaster recovery (pp. 3–21). Norwalk: Appleton-Century-Crofts.
Noonan, C. W., Pfau, J. C., Larson, T. C., & Spence, M. R. (2006). Nested case-control study of autoimmune disease in an asbestos-exposed population. Environmental Health Perspectives, 114, 1243–1247.
Norris, F. H., Friedman, M. J., Watson, P. J., Byrne, C. M., Diaz, E., & Kaniasty, K. (2002). 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry, 65, 207–239.
Norris, F. H., Stevens, S. P., Pfefferbaum, B., Wyche, K. F., & Pfefferbaum, R. L. (2008). Community resilience as a metaphor, theory, set of capacities, and strategy for disaster readiness. American Journal of Community Psychology, 41, 127–150. doi:10.1007/s10464-007-9156-6.
O’Sullivan, T. L., Kuziemsky, C., Toal-Sullivan, D., & Corneil, W. (2013). Unraveling the complexities of disaster management: A framework for critical social infrastructure to promote population health and resilience. Social Science and Medicine, 93, 238–246. doi:10.1016/j.socscimed.2012.07.0401-9.
Orom, H., Cline, R. J. W., Hernandez, T., Berry-Bobovski, L., Schwartz, A. G., & Ruckdeschel, J. C. (2012). A typology of communication dynamics in families living a slow-motion technological disaster. Journal of Family Issues, 33, 1299–1323. doi:10.1177/0192513X11430821.
Orom, H., Cline, R. J. W., Sayir, A., Hernandez, T., Broadway, S. C., Silk, K. J., & Schwartz, A. G. (2008, October). Community-wide disaster alert: Psychological consequences of living a slow-motion technological disaster. Presented at the annual meeting of the American Public Health Association, San Diego, CA.
Palinkas, L. (2012). A conceptual framework for understanding the mental health impacts of oil spills: Lessons from the Exxon Valdez oil spill. Psychiatry, 75, 203–222. doi:10.1521/psyc.2012.75.3.203.
Palinkas, L. A., Downs, M. A., Peterson, J. S., & Russell, J. (1993). Social, cultural, and psychological impacts of the Exxon Valdez oil spill. Human Organization, 52(1), 1–13.
Pfau, J. C., Sentissi, J. J., Weller, G., & Putnam, E. A. (2005). Assessment of autoimmune responses associated with asbestos exposure in Libby, Montana, USA. Environmental Health Perspectives, 113, 25–30.
Rook, K. S. (1984). The negative side of social interaction. Impact on psychological well-being. Journal of Personality and Social Psychology, 46, 1097–1108.
Russinova, Z., Rogers, E. S., Gagne, C., Bloch, P., Drake, K. M., & Mueser, K. T. (2014). A randomized controlled trial of a peer-run antistigma photovoice intervention. Psychiatric Services, 65, 242–246. doi:10.1176/appi.ps.201200572.
Rzepa, T., Zaba, R., & Silny, W. (2011). Management of the stressful stigma attached to sexually transmitted disease (preliminary report). Ginekologia Polska, 82, 675–679.
Sapien, J. (2007, April 26). Superfund today: Massive undertaking to clean up hazardous waste sites has lost both momentum and funding. The Center for Public Integrity: Investigative Journalism in the Public Interest. Retrieved from http://www.publicintegrity.org/superfund/report.aspx?aid=851.
Schneider, A., & McCumber, D. (2004). An air that kills: How the asbestos poisoning of Libby, Montana, uncovered a national scandal. New York: Berkley Books.
Sharma, A., Sharma, J., & Malhotra, D. (2010). The learnt factors in stress: The role of family environment. Journal of the Indian Academy of Applied Psychology, 36, 215–223.
Sullivan, P. (2007, January 24). Les Skramstad: Mont. miner exposed asbestos poisoning. The Washington Post, p. B07.
Taylor, A. J. W. (1991). Symposium: Counselling in disaster situations: The field of disasters and disaster stress. British Journal of Guidance and Counselling, 19, 1–7.
Teti, M., Murray, C., Johnson, L., & Binson, D. (2012). Photovoice as a community-based participatory research method among women living with HIV/AIDS: Ethical opportunities and challenges. Journal of Empirical Research on Human Research Ethics, 7, 34–43. doi:10.1525/jer.2012.7.4.34.
Teti, M., Pichon, L., Kabel, A., Farnan, R., & Binson, D. (2013). Taking pictures to take control: Photovoice as a tool to facilitate empowerment among poor and racial/ethnic minority women with HIV. Journal of the Association of Nurses in AIDS Care, 24, 539–553. doi:10.1016/j.jana.2013.05.001.
U.S. Cancer Statistics Working Group. (2007). United States cancer statistics: 1999–2004 Incidence and mortality web-based report. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute. Retrieved from http://apps.nccd.cdc.gov/uscs/Table.aspx?Group=TableAll&Year=2004&Display=n.
U.S. Census Bureau. (2010). American factfinder. Retrieved from http://factfinder2.census. http://www.gov/faces/tableservices/jsf/pages/productview.xhtml?src=bkmk.
U.S. Environmental Protection Agency. (2012). IRIS toxicological review of Libby amphibole asbestos (External Review Draft). Submitted to Science Advisory Board (SAB). U.S. Environmental Protection Agency, Washington, DC, EPA/635/R-11/002A.
Varni, S. E., Miller, C. T., McCuin, T., & Solomon, S. E. (2012). Disengagement and engagement coping with HIV/AIDS stigma and psychological well-Being of people with HIV/AIDS. Journal of Social and Clinical Psychology, 3, 123–150.
Wang, C., & Burris, M. A. (1997). Photovoice: Concept, methodology, and use for participatory needs assessment. Health Education & Behavior, 24, 369–387.
Ward, T. J., Spear, T., Hart, J., Noonan, C., Holian, A., Getman, M., et al. (2006). Trees as reservoirs for amphibole fibers in Libby, Montana. Science of the Total Environment, 367, 460–465.
Wheaton, B., Muthen, B., Alwin, D. R., & Summers, G. F. (1977). Assessing reliability and stability in panel models. In D. R. Heise (Ed.), Sociological methodology 1977 (pp. 84–136). San Francisco, CA: Jossey-Bass.
Whitbeck, L. B., Adams, G. W., Hoyt, D. R., & Chen, X. (2004). Conceptualizing and measuring historical trauma among American Indian people. American Journal of Community Psychology, 33, 119–130.
Whitehouse, A. C. (2004). Asbestos-related pleural disease due to tremolite associated with progressive loss of lung function: Serial observations in 123 miners, family members, and residents of Libby, Montana. American Journal of Industrial Medicine, 46, 219–225.
Whitehouse, A. C., Black, C. B., Heppe, M. S., Ruckdeschel, J., & Levin, S. M. (2008). Environmental exposure to Libby asbestos and mesotheliomas. American Journal of Industrial Medicine, 51, 877–880. doi:10.1002/ajim.20620.
Williams, D. R., Sternthal, M., & Wright, R. J. (2009). Social determinants: Taking the social context of asthma seriously. Pediatrics, 123(Suppl 3), S174–S184. doi:10.1542/peds.2008-2233H.
Wright, R. J. (2011). Epidemiology of stress and asthma: from constricting communities and fragile families to epigenetics. Immunology and Allergy Clinics of North America, 31, 19–39. doi:10.1016/j.iac.2010.09.011.
Wright, K., Naar-King, S., Lam, P., Templin, T., & Frey, M. (2007). Stigma scale revised: Reliability and validity of a brief measure of stigma for HIV+ youth. Journal of Adolescent Health, 40, 96–98.
Wright, R. S., Abraham, J. L., Harber, P., Burnett, B. R., Morris, P., & West, P. (2002). Fatal asbestosis 50 years after brief high intensity exposure in a vermiculite expansion plant. American Journal of Respiratory and Critical Care Medicine, 165, 1145–1149.
Zacharioudakis, M. (2001). Doing psychotherapy with patients with genital herpes: Issues and interventions. Scandinavian Journal of Behaviour Therapy, 30, 108–133.
Zakowski, S. G., Ramati, A., Morton, C., Johnson, P., & Flanigan, R. (2004). Written emotional disclosure buffers the effects of social constraints on distress among cancer patients. Health Psychology, 23, 555–563. doi:10.1037/0278-6133.23.6.555.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cline, R.J.W., Orom, H., Chung, J.E. et al. The Role of Social Toxicity in Responses to a Slowly-Evolving Environmental Disaster: The Case of Amphibole Asbestos Exposure in Libby, Montana, USA. Am J Community Psychol 54, 12–27 (2014). https://doi.org/10.1007/s10464-014-9660-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10464-014-9660-4