
Abstract
We evaluated the feasibility, acceptability, and preliminary efficacy of an economic and relationship-strengthening intervention to reduce heavy alcohol use among couples living with HIV in Malawi (Mlambe). Mlambe consisted of training on financial literacy and relationship skills, combined with 1:1 matched savings accounts to invest in an income-generating activity. In a randomized controlled trial, we compared Mlambe to enhanced usual care (EUC). We enrolled 78 married couples having a partner on antiretroviral therapy (ART) who reported heavy alcohol use based on the AUDIT-C. Using targets of 75%, primary outcomes included retention rates at 10 and 15-months, session attendance rates, and satisfaction with Mlambe. Exploratory outcomes were heavy alcohol use (AUDIT-C and/or PEth positive), number of drinking days in the past month, AUDIT-C score, optimal adherence to ART (95% or higher), and viral suppression. We exceeded our targets for feasibility and acceptability metrics. Retention rates were 96% at 15-months. Session attendance and satisfaction levels were both 100%. From baseline to 15-months, Mlambe participants reported decreases in mean number of drinking days (from 6.8 to 2.1) and AUDIT-C scores (from 7.5 to 3.1); while ART adherence rates improved across the same period (from 63.2 to 73.9%). Participants in Mlambe, as compared to those in EUC, had lower rates of heavy alcohol use (89.5% vs. 97.2%) and higher rates of viral suppression (100% vs. 91.9%) at 10-months. Differences between arms were not statistically significant in this small pilot study. Mlambe was highly feasible and acceptable, and shows promise for reducing heavy alcohol use and viral non-suppression among couples with HIV in a larger efficacy study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Heavy alcohol use, defined as drinking above the recommended limits, and its negative consequences are a major health threat for people living with HIV (PLWH). The prevalence of heavy alcohol use is higher among PLWH as compared to the general population [1] and is associated with lower adherence to antiretroviral therapy (ART) and poor HIV clinical outcomes [2,3,4,5,6]. Although the majority of adults abstain from alcohol use, sub-Saharan Africa has some of the highest per capita alcohol consumption rates in the world among those who drink [7].
Among people affected by HIV in sub-Saharan Africa, the key drivers and consequences of heavy alcohol use are economic, social, and dyadic. Unemployment and coping with a stressful, low-wage job are linked to heavy alcohol use [8,9,10]. In couples, research has found that partners can influence each other’s alcohol use, and alcohol use can be both a cause and result of relationship distress [11]. For example, heavy alcohol use is positively associated with negative communication styles and mistrust in South African couples [12]. In Malawi, men reported difficulties taking HIV medications when drinking, however, their female partners, most of whom did not drink, faced adherence challenges from their husband’s drinking through intimate partner violence (IPV) and food insecurity [13]. Partners can also mitigate the harms of alcohol use by helping manage alcohol use and ART adherence even during alcohol consumption [14], suggesting that partners should be involved in alcohol interventions.
Despite the importance of multi-level determinants of heavy alcohol use, most alcohol interventions have intervened with individuals using approaches such as cognitive behavioral therapy or motivational interviewing [15] and found mixed results in sub-Saharan Africa [16]. Economic-strengthening interventions could have meaningful impacts on alcohol use, especially with couples, who could reinforce financial material and collaborate around finances. Savings-based interventions combined with financial literacy training (FLT) may provide a sustainable option by helping PLWH break the cycle of poverty through investments, liquid assets, and lifelong financial knowledge [17,18,19]. In Uganda, the Suubi intervention provided incentivized savings accounts combined with FLT to facilitate savings and investments. Suubi had positive impacts on mental health, family cohesion, sexual risk-taking, and virologic suppression among adolescents living with or at risk for HIV [20,21,22].
Relationship-strengthening interventions have also been effective at reducing alcohol use and addressing HIV-related behaviors across settings. In the US, behavioral couples therapy was more effective than an individual-based approach by addressing the relationship dynamics that often intersect with alcohol use [23]. In South Africa, the Couples Health Co-Op intervention reinforced positive dimensions of couples’ relationships with skill-building exercises on communication and sex and found that men in the couples arm were less likely to report heavy alcohol use as compared to the control arm of male-only groups [24].
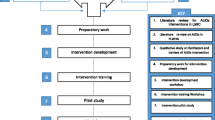
There is also growing evidence that economic-strengthening interventions can be a valuable addition to psychological approaches to HIV treatment [25]. We posit that gaining relationship skills will help couples work together on financial goals and reduce alcohol use, while increasing savings and financial stability will alleviate stress on couples, encourage planning for the future, and reduce drinking, thereby enhancing couple functioning. We developed the Mlambe intervention for Malawian couples by adapting and integrating two efficacious interventions focused on strengthening household economics and relationship dynamics. Relationship-strengthening activities were based on a successful intervention with couples in South Africa called Uthando Lwethu, which consisted of relationship education and skills, and increased uptake of couples HIV counseling and testing [26]. Economic strengthening activities were based on Suubi in Uganda, which consisted of incentivized, couple savings accounts, and FLT [21, 27, 28]. The intervention development process for Mlambe has been described elsewhere [29].
In this study, we report on the results of a pilot randomized controlled trial (RCT) of Mlambe conducted with couples having at least one partner on ART who reported heavy alcohol use. Our primary outcomes focused on the feasibility and acceptability of Mlambe. We also explored the preliminary effects of Mlambe on secondary outcomes of alcohol use, ART adherence, and viral suppression. No formal hypotheses are presented given our primary interest in feasibility and acceptability in this pilot study.
Methods
Study Setting
In Malawi, men are the primary alcohol users; among men who drink (30% of men), 51% meet criteria for heavy drinking [30]. Malawi’s poverty levels are high with 71% of adults living on $2 USD or less per day [31]. Only 34% of Malawians have access to the formal banking sector for which financial literacy is a major barrier [32]. This study took place in the Zomba district of Malawi where 15% of adults are living with HIV [33].
Inclusion Criteria
Couples were eligible if: 1) in a non-polygamous marital union; (2) aged 18 or older; (3) had at least one partner with a positive AUDIT-C screen in the prior three months (score of ≥ 4 for men and ≥ 3 for women) and on ART for at least six months (referred to as the “index patient” for clarity). Partners living with HIV must have disclosed their status to the spouse. We excluded couples who reported severe IPV in the past 3 months [34] and/or feared that their safety would be at risk through participation.
Recruitment
Participants were recruited at three health centers in the Zomba district: an urban, public HIV clinic at the district hospital; a rural, privately-funded but government-supported community hospital; and a peri-urban, public health center. Research assistants presented study information at the health information talks in the waiting rooms of HIV clinics. Index patients approached the research assistants if interested. If the index patient was interested and eligible, research assistants gave patients an information card to give to their spouse and set up a phone appointment to screen the partner. If the partner was interested and eligible, the couple was scheduled for their first appointment to obtain informed consent in the local language of Chichewa. Research assistants participated in a multi-week training described elsewhere [29] and were certified in Good Clinical Practice (GCP) guidelines.
Randomization
Couples were randomized to either: (1) Mlambe; or (2) enhanced usual care (EUC). To ensure balance in study arms over time, we used block randomization with randomly permuted block sizes using a computer-generated and secure process. We randomized 78 couples in blocks of 20 with three blocks composed of homogeneous groups of couples from the three clinic sites and a fourth block comprising of a mix of couples from all three sites. After twenty couples per block were enrolled, we held a randomization ceremony for each block in which couples received their assignment [29].
Ethical Approval
This study received ethical approval from the institutional review board at the University of California San Francisco and the National Health Science Research Committee in Malawi. The study was registered at ClinicalTrials.gov (NCT #04906616). We followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines for multi-arm parallel group trial design [35].
Interventions
Mlambe is described elsewhere [29]. In brief, Mlambe consisted of ten monthly sessions delivered by a pair of facilitators. Prior to the first session, couples set up a joint banking account at a commercial bank in which they could start making deposits. Couples were incentivized with a 1:1 match for each Malawi Kwacha saved up to $10 USD per month. Sessions took place in community-based locations equipped with a conference room. A structured manual was followed to deliver sessions on economic and relationship-strengthening activities, which included sessions on banking services, budgeting, savings and asset building, debt management, alcohol use, relationship and power dynamics, and couple communication skills. In the last session, community-based extension workers employed by the Malawian government were invited to advise couples on best practices for starting an income-generating activity (IGA) such as animal husbandry or a produce stand, and continued to meet with couples at their homes thereafter. To start their family-based IGA, couples accessed the combined savings and matched component and could invest the money into the business of their choice.
In the EUC control arm, couples received 10–15 min of brief alcohol counseling modelled after the WHO brief intervention [36] in addition to usual care. Usual care was defined by the Malawi Ministry of Health guidelines for the clinical management of HIV in adults [37]. This includes monitoring for alcohol-related non-adherence, treatment failure, and liver disease or failure as part of routine care. In selecting the control, we chose to balance our ethical obligation to provide basic health information on alcohol use (minimal in this setting), while maximizing the generalizability of our findings to inform a future RCT, which will employ a EUC control group. Clinical trial experts recommend the usual care condition over other designs such as a time-and-attention control (TAC) when the long-term goal is to inform implementation science and scale-up [38, 39]. Our long-term goal will be to test the effectiveness of a scalable alcohol intervention. Moreover, because TAC designs have an active but different intervention, there is the risk of positively-biased intervention results because the comparison arm can distract participants from making reductions in alcohol use they would have otherwise made.
Data Collection
We conducted assessments at baseline, 10-months, and 15-months after starting intervention sessions. The 10-month visit occurred after completing all intervention sessions; the 15-month visit occurred after starting their family-based IGA. Couples completed a brief satisfaction questionnaire after each intervention session to rate satisfaction (as a couple) on a five-point Likert scale and whether they would recommend the session to a friend or relative. Attendance logs were completed after each session, including an indicator of whether both partners were present. Savings deposits, withdrawals, and the matched contribution was tracked in a ledger. Interviewer-administered surveys were conducted using REDCap® forms programmed onto tablet devices.
Questionnaires asked about socio-demographics, couple characteristics (e.g., relationship duration), food insecurity [40], and relationship dynamics, including intimacy [41], trust [42], equality/shared power [43], unity [44], relationship and sexual satisfaction [45, 46], intimate partner violence [47], partner social support [48], and couple communication [49]. Measures of alcohol use included the AUDIT-C [50] and timeline follow-back [51] to capture the number of drinking days in the past month. ART adherence was based on a low-literacy version of the Visual Analog Scale/VAS [52]. All measures were translated into Chichewa and back-translated to English to verify translations. Measures were tested with HIV-affected couples in our formative study and had high reliability [52, 53]. Both partners living with HIV were asked about their ART adherence and included in the analysis. Index patients (not partners) were only included in analyses on heavy alcohol use and viral suppression.
We also conducted 60–90 min exit interviews (with partners separately) with a subset of 25 couples to understand experiences with the intervention, and to explore mechanisms of behavior change around alcohol use. A team of five researchers coded the English transcripts using broad codes (e.g., overall experience, knowledge gained, types of intervention effects) and examined patterns within and across the dyads using framework analysis [54].
Laboratory Testing
At the 10-month visit, whole blood samples were collected from index patients to test for plasma viral load and phosphatidylethanol (PEth), an alcohol biomarker. We prepared dried blood spots (DBS) by pipetting whole blood onto Whatman 903 cards. DBS cards were stored at room temperature in locked cabinets and transported to a commercial laboratory in the United States for PEth quantification (16:0/18:1 analog), with lower limit of quantification of 8 ng/ml [55]. PEth is well-correlated with breathalyzer-assessed daily drinking [56] and the volume of alcohol consumed in the past 21 days [57]. Viral load tests were performed on plasma samples at an accredited laboratory onsite using the Abbott Real-time m2000, Abbott Alinity, or Hologic Aptima Panther for HIV-1 RNA with lower limits of detection under 40 copies/ml.
Primary Outcomes: Feasibility and Acceptability
The primary goal of the pilot trial was to assess feasibility and acceptability of Mlambe using the following metrics and a priori targets: recruitment rate (number of couples enrolled over six months; target: 80 couples), randomization rate (proportion of enrolled couples who are randomized; target: 75%), satisfaction levels (proportion of couples who report being satisfied or very satisfied with Mlambe: target: 75%), session completion rates (proportion of couples who attend 100% of sessions; target: 75%), and retention at 10-month and 15-month follow-up visits (proportion of couples who complete follow-up surveys; target: 75%). We also assessed fidelity to the intervention by having the manager or facilitators complete detailed checklists after each session to document activities conducted. As a second check, we audio-recorded all sessions and had an independent research assistant listen to a random selection of recordings (20%) and complete the same checklists. We set a target of 80% for fidelity.
Secondary Outcomes: Alcohol use and HIV Treatment Outcomes
Although we were not powered to examine treatment effects, we explored the effect of Mlambe on the number of drinking days in the past 30 (assessed via the timeline follow-back), heavy alcohol use (i.e., positive AUDIT-C score in the past three months and/or a PEth value ≥ 35 ng/ml, a recommended cutoff value [58]), raw AUDIT-C score (0–12), optimal ART adherence (95% or higher on the VAS), and viral suppression (less than 200 copies/ml per HIV clinical guidelines).
Sample Size
Formal tests of health outcomes and attempts to obtain valid estimates of effect sizes are not statistically justified for pilot studies [59,60,61,62,63,64] due to smaller sample sizes and design adjustments necessary to maximize recruitment, retention, and other outcomes. We targeted an a priori sample size of N = 80 couples (40 couples per arm) for practical reasons and because of our focus on feasibility and acceptability rather than hypothesis-testing or estimating effect sizes.
Statistical Analysis
We computed descriptive statistics to capture measures of central tendency for continuous variables and proportions for binary variables, by visit and by treatment arm. We computed simple statistics (e.g., proportions) on our main feasibility and acceptability indicators above.
To explore the effect of Mlambe on the secondary outcome of number of drinking days, we used mixed-effects negative binomial regression models including all three timepoints. Negative binomial models are recommended for count-based outcomes such as number of drinking days [65]. For the AUDIT-C score, we used linear mixed-effects models including all three timepoints. Models above included a random effect for participants and fixed effects for timepoint and study arm, interaction of time and arm, and sex of the index patient. For optimal adherence to ART, we used mixed-effects logistic regression models including all three timepoints. The model included all participants on ART to maximize use of the sample and because we hypothesized that both partners could benefit from the intervention. To account for individuals nested within couples, we also included a random effect for the dyad. We also explored the whether the effects were moderated by respondent type (i.e., index patient versus partner).
To explore effects on biomarker-based outcomes captured only at 10-months (e.g., heavy alcohol use), we used logistic regression models with treatment arm as the main predictor. Biomarker data were collected only on index patients, not partners. The model for viral suppression could not be fit due to small cell sizes and thus we used a chi-square test to examine differences in viral suppression by treatment arm and report Pearson chi-square and Fisher’s exact p-values. All analyses used an intent-to-treat approach to include every participant within the analysis based on their original randomization group. Statistical analyses were conducted in Stata 18.
Results
Sample Characteristics
Among the 78 couples (156 individuals) randomized, the mean age was 43.5 years and most (78%) had a primary school education or less (see Table 1). With the exception of physical IPV there were no differences between treatment arms on baseline characteristics as shown in Table 1. On average, couples had been together for 13.7 years and most were sero-concordant positive (84.4%). Almost all index patients were male (96.1%). Of those who drank alcohol, the most common types of alcohol consumed were locally-made spirits (e.g., Kachasu; 63%), locally-made beer (39%), sorghum beer (28%), commercially-made spirits (17%), and bottled beer (7%).
Study Participation
Over a six-month period starting in May of 2021, 89 couples were screened for eligibility and of those, 94% were enrolled and completed baseline assessments (see Fig. 1). No couples were excluded based on IPV or safety concerns. Of those enrolled, 93% (N = 78 couples) were randomized to intervention or control (39 couples per arm); we exceeded our randomization rate of 75%. Of the 156 individuals within 78 couples who were randomized, 96.8% of participants (N = 151) were retained at 10 months. At the 15-month visit, 96.8% of participants were retained (N = 151). Thus, we exceeded our retention target of 75%. Retention rates for intervention and control at 10-months were 98.% and 94.8%, respectively. At 15-months, corresponding retention rates were 97.4% and 96.1%, respectively. There was no evidence of differential attrition by study arm at 10-month (χ2 = 1.84; p = 0.17) or 15-month visits (χ2 = 0.21; p = 0.64). No adverse events related to study participation occurred over the study period.

CONSORT diagram for randomized controlled trial of the Mlambe intervention versus an enhanced usual care (EUC) control arm
Attendance
Eleven couples missed at least one session but made up the session(s). Reasons for missing a session included the husband was travelling for work, funeral attendance, sickness, the husband had consumed too much alcohol the night before, and arguments within the couple. Thus, there was 100% attendance across the ten sessions. We exceeded our attendance target of 75%.
Satisfaction Levels
Following each intervention session, all couples (100%) reported that they were satisfied or very satisfied with the session and would recommend the session to a friend or relative. Satisfaction levels remained at 100% at follow-up visits. We exceeded our satisfaction target of 75%.
Fidelity
Checklist data was tabulated to calculate fidelity, which was 100%. This was confirmed by an independent research assistant who listened to a random selection of audio-recorded sessions. We exceeded our fidelity target of 80%.
Financial Behaviors
All couples obtained national ID cards and successfully open a joint bank account before the first session. The mean number of deposits made (out of ten) was 7.8. Over the course of the 10-month savings period, the mean cumulative savings across all intervention couples was $77.50, ranging from $22-$194 USD. This equates to an average of $7.75 USD per month. When including the match component, the mean total savings was approximately $145, ranging from $44-$292 USD. By the 15-month visit, all couples started an IGA which included the purchase of livestock (e.g., chickens, goats), agricultural inputs (e.g., fertilizer, seeds) for a produce business, purchase of maize to sell at a higher price, and a bicycle taxi to provide village transport.
Exploratory Effects on Secondary Outcomes
Means and proportions for secondary outcomes are listed in Table 2. Mlambe index participants reported an average of 2.7 and 2.1 drinking days at 10 and 15-month follow-up visits, compared to 6.8 at baseline (see Table 2; Fig. 2). As shown in Table 3 (main effects only), there was a decline in the number of drinking days at 10 months (IRR = 0.44; p < 0.001) and 15 months (IRR = 0.27, p < 0.001) as compared to baseline, but no difference between study arms in drinking days (IRR = 1.08; p = 0.649). Mlambe participants reported mean AUDIT-C scores of 5.1 and 3.1 at 10-months and 15-months, compared to 7.5 at baseline (see Table 2). Thus, there was a decline in AUDIT-C score at 10 months (see Table 3; B=-2.67; p < 0.001) and 15-months (B=-4.47; p < 0.001), but no difference between study arms in AUDIT-C score (B = 0.12; p = 0.741). We also tested for an interaction between time and treatment arm and did not find an effect.

Self-reported alcohol use and adherence to ART over the study period. (A) Mean self-reported number of drinking days in the past 30 with 95% confidence intervals (index patients, N = 78). (B) Percentage reporting optimal ART adherence (all participants on ART, N = 141) with 95% confidence intervals
For Mlambe participants on ART, 73.1% and 73.9% reported optimal adherence at follow-up visits, compared to 63.2% at baseline (Table 2; Fig. 2). As shown in Table 3, the odds of optimal adherence were higher at 10-months (OR = 1.69; p = 0.112) and 15-months (OR = 2.14; p = 0.02) as compared to baseline, but there was no difference between study arms in adherence (OR = 0.65; p = 0.401). We tested for an interaction between time and treatment arm, and for an interaction between treatment arm and respondent type (index patient versus partner), and did not find effects.
In the models for heavy alcohol use (PEth and/or AUDIT-C positive), the odds of heavy drinking were 76% lower in the Mlambe arm as compared to EUC (89.5% vs. 97.2%; OR = 0.24; p = 0.216) but differences were not statistically significant. For viral suppression, chi-square test results showed greater rates of viral suppression in the intervention arm (100%; viral load < 200 copies/ml) as compared to control arm (91.9%; χ2 = 3.2; p = 0.07; Fisher’s exact p = 0.115) but differences were not statistically significant. For the men in the control arm who were not suppressed, the mean viral load value was 43,988 copies/ml (range: 2,326 − 126,786), suggesting viremia and likely viral failure [66].
Exit Interview Findings
Couples in Mlambe described a variety of changes in patterns of alcohol use, including prolonged periods of abstinence, switching to less potent forms of alcohol use (e.g., from Kachasu to fermented sorghum beer), reducing the number of drinks in one sitting, drinking at home instead of at alcohol establishments, coming home earlier from drinking sessions, and reducing the length of binge periods. Often these patterns were confirmed by their wives, who were viewed by the field team as being reliable, honest, and forthcoming due to being highly committed to reducing their husband’s alcohol use.
Discussion
This pilot trial provides strong evidence in support of the feasibility and acceptability of Mlambe. We met and often exceeded our feasibility and acceptability targets: 80 couples were recruited in six months, we had 100% attendance at 10 sessions, 100% of couples were satisfied with Mlambe, and we retained 96% of couples after a relatively long follow-up period of 15 months. Of note, banking services are limited in rural areas of Malawi and couples had low engagement with the formal banking sector at baseline, however, most were able to save every month and save enough to start an IGA for their family. We also successfully hired and trained two facilitators with no previous experience delivering such an intervention and we were able to maintain high fidelity to the intervention.
While we were not powered to examine alcohol and HIV treatment outcomes, we found reductions in self-reported alcohol use and improvements in ART adherence over time. It is possible that changes in self-reports could be attributed in part to social desirability bias, as other alcohol studies have found [67]. We also initiated the study soon after the COVID-19 pandemic began and it is possible that effects of the intervention were attenuated by other pandemic-related conditions such as stress, economic insecurity, and potential increases in alcohol use as shown in another study from Uganda [68]. For the biomarker-enhanced alcohol outcome, the prevalence of heavy alcohol use was lower by 8% points in the Mlambe arm as compared to EUC. We also found that viral suppression rates were higher in the Mlambe arm by 9% points than EUC. However, given that these differences did not achieve statistical significance, the observed difference could be due to chance. Rates of viral suppression in Malawi are also high with widespread use of dolutegravir [66] and our findings for viral suppression are consistent with other alcohol studies in sub-Saharan Africa [67]. We did not collect viral load at baseline to be able to examine change over time and although randomization should have removed differences between arms, there is still the low likelihood that the intervention arm had higher levels of viral suppression to start. Nevertheless, the findings may indicate the potential for Mlambe to close the remaining gap from 95 to 100% viral suppression in line with global AIDS targets [69]. We did not recruit couples with unsuppressed viral load or exclude those with severe alcohol use because our goal was to maximize reach of the intervention in a setting with few alcohol services and thus the effect of Mlambe on participants with lower severity of alcohol use and higher ART adherence may have been dampened. Future studies with larger samples sizes could explore the types of participants who may benefit the most, which we were not powered for.
Finally, exit interviews highlighted that some participants switched from highly-potent spirits to less harmful forms of alcohol (e.g., sorghum beer) and may not have reduced drinking frequency [54]. This important behavioral change and harm reduction approach used by participants would not necessarily be detected in our alcohol use measures, including PEth. Many wives indicated that they saw a positive change in their husbands’ drinking behaviors and improvements in their couple relationships–which was supported by findings that couples in the Mlambe arm reported greater increases in relationship quality as compared to EUC [70]. Future analyses of mediators in a larger sample could help to confirm the hypothesized, behavioral pathways linking alcohol use with HIV outcomes.
Strengths included the collection of dyadic data from both partners, an alternative alcohol counseling intervention as the control arm, a diverse sample of couples from urban, peri-urban, and rural areas, use of biomarkers to supplement self-reports, and a relatively long follow-up period with high retention. Given the limitations of small studies, we only collected biomarkers at 10-months among index partners (and not partners) and could not control for baseline values or include partners’ viral suppression status in the analysis. Other limitations included the small sample size and insufficient statistical power to detect effects on secondary health outcomes. There is a continued need for rigorous trials to evaluate economic and relationship-strengthening interventions for HIV and health outcomes, which are currently lacking [71]. Finally, our intervention was designed as a package of services that includes education, skills, and savings and asset generation and thus is it not possible to disentangle which elements had the largest impact on behaviors, however, other studies are currently investigating this issue [72].
Despite these limitations, this study contributes new knowledge that an economic and relationship-strengthening intervention is feasible to implement with lay counselors and with couples in a resource-poor and rural setting. While the piloted intervention is comparably more intensive than other brief interventions, it fills an important gap present in alcohol and HIV-related services and addresses economic determinants of heavy alcohol use that have been largely ignored to date. A full-scale efficacy trial is needed to evaluate alcohol use and HIV treatment outcomes in a larger sample of couples, and to identify the types of couples who may benefit the most from an intensive intervention (e.g., higher conflict couples), and to assess the cost-effectiveness and future scale-up issues for Mlambe. Economic and relationship-strengthening interventions that promote couples to increase income levels and assets will be critical for achieving UNAIDS 95-95-95 goals and reducing poverty, which remains a fundamental driver of HIV globally.
Data Availability
Not available due to the potential to identify participants.
Code Availability
Not applicable.
References
Schneider M, Chersich M, Temmerman M, Degomme O, Parry CD. The impact of alcohol on HIV prevention and treatment for South africans in primary healthcare. Curationis. 2014;37(1):1–8.
Hahn JA, Samet JH. Alcohol and HIV disease progression: weighing the evidence. Curr HIV/AIDS Rep. 2010;7(4):226–33.
Williams EC, Hahn JA, Saitz R et al. Alcohol use and human immunodeficiency virus (HIV) infection: current knowledge, implications, and future directions. Alcoholism: Clinical and Experimental Research. 2016;40(10):2056-72.
Salmon-Ceron D, Lewden C, Morlat P, et al. Liver disease as a major cause of death among HIV infected patients: role of hepatitis C and B viruses and alcohol. J Hepatol. 2005;42(6):799–805.
Braithwaite RS, Bryant KJ. Influence of alcohol consumption on adherence to and toxicity of antiretroviral therapy and survival. Alcohol Res Health. 2010;33(3):280.
Velloza J, Kemp CG, Aunon FM, et al. Alcohol use and antiretroviral therapy non-adherence among adults living with HIV/AIDS in sub-saharan Africa: a systematic review and meta-analysis. AIDS Behav. 2020;24:1727–42.
World Health Organization. Global status report on alcohol and health 2018. World Health Organization; 2019.
Kalichman SC, Simbayi LC, Kagee A, et al. Associations of poverty, substance use, and HIV transmission risk behaviors in three South African communities. Soc Sci Med. 2006;62(7):1641–9.
Dunkle KL, Jewkes RK, Brown HC, et al. Transactional sex among women in Soweto, South Africa: prevalence, risk factors and association with HIV infection. Soc Sci Med. 2004;59:1581–92.
Setlalentoa B, Pisa P, Thekisho G, Ryke E, Loots Du T. The social aspects of alcohol misuse/abuse in South Africa. South Afr J Clin Nutr. 2010;23(sup2):11–5.
Rodriguez LM, Neighbors C, Knee CR. Problematic alcohol use and marital distress: an interdependence theory perspective. Addict Res Theory. 2014;22(4):294–312.
Woolf-King SE, Conroy AA, Fritz K et al. Alcohol use and relationship quality among South African couples. Subst Use Misuse. 2018:1–10.
Conroy AA, McKenna SA, Ruark A. Couple interdependence impacts alcohol use and adherence to antiretroviral therapy in Malawi. AIDS Behav. 2019;23(1):201–10.
Conroy AA, McKenna SA, Leddy A, et al. If she is Drunk, I don’t want her to take it: Partner beliefs and Influence on Use of Alcohol and antiretroviral therapy in South African couples. AIDS Behav. 2017;21(7):1885–91.
Brown JL, DeMartini KS, Sales JM, Swartzendruber AL, DiClemente RJ. Interventions to reduce alcohol use among HIV-infected individuals: a review and critique of the literature. Curr HIV/AIDS Rep. 2013;10(4):356–70.
Scott-Sheldon LA, Carey KB, Johnson BT, Carey MP, Team MR. Behavioral interventions targeting alcohol use among people living with HIV/AIDS: a systematic review and meta-analysis. AIDS Behav. 2017;21(2):126–43.
Swann M. Economic strengthening for retention in HIV care and adherence to antiretroviral therapy: a review of the evidence. AIDS Care. 2018;30(sup3):85–98.
Swann M. Economic strengthening for HIV prevention and risk reduction: a review of the evidence. AIDS Care. 2018;30(sup3):37–84.
Allen H, Panetta D. Savings groups: what are they. Washington DC: SEEP Network; 2010. p. 2.
Ssewamala FM, Han C-K, Neilands TB. Asset ownership and health and mental health functioning among AIDS-orphaned adolescents: findings from a randomized clinical trial in rural Uganda. Soc Sci Med. 2009;69(2):191–8.
Bermudez LG, Ssewamala FM, Neilands TB et al. Does economic strengthening improve viral suppression among adolescents living with HIV? Results from a Cluster Randomized Trial in Uganda. AIDS Behav. 2018:1–10.
Ksoll C, Lilleør HB, Lønborg JH, Rasmussen OD. Impact of Village Savings and Loan associations: evidence from a cluster randomized trial. J Dev Econ. 2016;120:70–85.
Klostermann KC, Fals-Stewart W. Intimate partner violence and alcohol use: exploring the role of drinking in partner violence and its implications for intervention. Aggress Violent Beh. 2006;11(6):587–97.
Wechsberg WM, El-Bassel N, Carney T et al. Adapting an evidence-based HIV behavioral intervention for South African couples. Substance abuse treatment, prevention, and policy. 2015;10(1):6.
Operario D, Kuo C, Sosa-Rubí SG, Gálarraga O. Conditional economic incentives for reducing HIV risk behaviors: integration of psychology and behavioral economics. Health Psychol. 2013;32(9):932.
Darbes LA, McGrath NM, Hosegood V, et al. Results of a couples-based randomized controlled trial aimed to increase testing for HIV. JAIDS J Acquir Immune Defic Syndr. 2019;80(4):404–13.
Ssewamala FM, Bermudez LG, Neilands TB, et al. Suubi4Her: a study protocol to examine the impact and cost associated with a combination intervention to prevent HIV risk behavior and improve mental health functioning among adolescent girls in Uganda. BMC Public Health. 2018;18(1):693.
Ssewamala FM, Neilands TB, Waldfogel J, Ismayilova L. The impact of a comprehensive microfinance intervention on depression levels of AIDS-orphaned children in Uganda. J Adolesc Health. 2012;50(4):346–52.
Conroy AA, Tebbetts S, Darbes LA et al. Development of an economic and relationship-strengthening intervention for Alcohol drinkers living with HIV in Malawi. AIDS Behav. 2022:1–16.
World Health Organization. Global status report on alcohol and health. Geneva, Switzerland: World Health Organization; 2014.
World Bank Group. Republic of Malawi Poverty Assessment. https://openknowledge.worldbank.org/handle/10986/26488. 2017.
UNCTAD. Access to Financial Services in Malawi: Policies and Challenges. 2014.
MDHS. Malawi demographic and health survey 2015-16. Maryland: NSO and ORC Macro; 2016.
World Health Organization. Researching violence against women: practical guidelines for researchers and activists. World Health Organization; 2005.
Juszczak E, Altman DG, Hopewell S, Schulz K. Reporting of multi-arm parallel-group randomized trials: extension of the CONSORT 2010 statement. JAMA. 2019;321(16):1610–20.
Babor TF, Higgins-Biddle JC, Organization WH. Brief intervention for hazardous and harmful drinking: a manual for use in primary care. 2001.
Ministry of Health Malawi. 4rd Edition of the Malawi guidelines for Clinical Management of HIV in children and adults. Malawi: Lilongwe; 2018.
Silverman HJ, Miller FG. Control group selection in critical care randomized controlled trials evaluating interventional strategies: an ethical assessment. Crit Care Med. 2004;32(3):852–7.
Vickers AJ, de Craen AJ. Why use placebos in clinical trials? A narrative review of the methodological literature. J Clin Epidemiol. 2000;53(2):157–61.
Coates J, Swindale A, Bilinsky P. Household Food Insecurity Access Scale (HFIAS) for measurement of food access: indicator guide: version 3. 2007.
Sternberg RJ. Construct validation of a triangular love scale. Eur J Social Psychol. 1997;27(3):313–35.
Larzelere RE, Huston TL. The dyadic trust scale: toward understanding interpersonal trust in close relationships. J Marriage Fam. 1980:595–604.
Kurdek LA. The deterioration of relationship quality for gay and lesbian cohabiting couples: a five-year prospective longitudinal study. Personal Relationships. 1996;3(4):417–42.
Aron A, McLaughlin-Volpe T, Mashek D, et al. Including others in the self. Eur Rev Social Psychol. 2004;15(1):101–32.
Conroy AA, Ruark A, Neilands TB, et al. Development and validation of the couple sexual satisfaction scale for HIV and Sexual Health Research. Arch Sex Behav. 2021;50:3297–311.
Funk JL, Rogge RD. Testing the ruler with item response theory: increasing precision of measurement for relationship satisfaction with the couples satisfaction index. J Fam Psychol. 2007;21(4):572.
Garcia-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts CH. Prevalence of intimate partner violence: findings from the WHO multi-country study on women’s health and domestic violence. Lancet. 2006;368(9543):1260–9.
Cutrona CE, Russell DW. The provisions of social relationships and adaptation to stress. Adv Personal Relationships. 1987;1(1):37–67.
Christensen A, Shenk JL. Communication, conflict, and psychological distance in nondistressed, clinic, and divorcing couples. J Consult Clin Psychol. 1991;59(3):458.
Bradley KA, DeBenedetti AF, Volk RJ, et al. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcoholism: Clin Experimental Res. 2007;31(7):1208–17.
Sobell LC, Sobell MB. Timeline follow-back: a technique for assessing self-reported alcohol consumption. Measuring alcohol consumption: Psychosocial and biochemical methods. 1992:41–72.
Conroy AA, McKenna S, Ruark A, et al. Relationship dynamics are Associated with Self-reported adherence but not an Objective Adherence measure in Malawi. AIDS Behav. 2022;26(11):3551–62.
Conroy AA, Leddy AM, Darbes LA, et al. Bidirectional violence is associated with poor engagement in HIV care and treatment in Malawian couples. J Interpers Violence. 2022;37(7–8):NP4258–77.
Gutin S, Jere J, Mulauzi N et al. Perceived impacts of Mlambe intervention on alcohol use, relationship dynamics, household economics, and HIV treatment adherence in Malawian couples. Presented at the AIDS Impact Conference, Stockholm, Sweden. June 12–14, 2023. 2023.
Jones J, Jones M, Plate C, Lewis D. The detection of 1-palmitoyl-2-oleoyl-sn-glycero-3-phosphoethanol in human dried blood spots. Anal Methods. 2011;3(5):1101–6.
Hahn JA, Dobkin LM, Mayanja B, et al. Phosphatidylethanol (PEth) as a biomarker of alcohol consumption in HIV-positive patients in sub‐Saharan Africa. Alcoholism: Clin Experimental Res. 2012;36(5):854–62.
Ulwelling W, Smith K. The PEth blood test in the security environment: what it is; why it is important; and interpretative guidelines. J Forensic Sci. 2018;63(6):1634–40.
Helander A, Hansson T. National harmonization of the alcohol biomarker PEth. Lakartidningen. 2013;110(39–40):1747–8.
Kraemer HC, Mintz J, Noda A, Tinklenberg J, Yesavage JA. Caution regarding the use of pilot studies to guide power calculations for study proposals. Arch Gen Psychiatry. 2006;63(5):484–9.
NIH/NCCIH. Pilot Studies: Common Uses and Misuses. Website: https://nccih.nih.gov/grants/whatnccihfunds/pilot_studies. 2017.
Leon AC, Davis LL, Kraemer HC. The role and interpretation of pilot studies in clinical research. J Psychiatr Res. 2011;45(5):626–9.
Moore CG, Carter RE, Nietert PJ, Stewart PW. Recommendations for planning pilot studies in clinical and translational research. Clin Transl Sci. 2011;4(5):332–7.
Thabane L, Ma J, Chu R, et al. A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol. 2010;10(1):1.
Teresi JA, Yu X, Stewart AL, Hays RD. Guidelines for designing and evaluating feasibility pilot studies. Med Care. 2022;60(1):95–103.
Horton NJ, Kim E, Saitz R. A cautionary note regarding count models of alcohol consumption in randomized controlled trials. BMC Med Res Methodol. 2007;7(1):1–9.
Schramm B, Temfack E, Descamps D, et al. Viral suppression and HIV-1 drug resistance 1 year after pragmatic transitioning to dolutegravir first-line therapy in Malawi: a prospective cohort study. Lancet HIV. 2022;9(8):e544–53.
Hahn JA, Fatch R, Emenyonu NI, et al. Effect of two counseling interventions on self-reported alcohol consumption, alcohol biomarker phosphatidylethanol (PEth), and viral suppression among persons living with HIV (PWH) with unhealthy alcohol use in Uganda: a randomized controlled trial. Drug Alcohol Depend. 2023;244:109783.
Asiimwe C, Fatch R, Cheng DM, et al. Bar Attendance and Alcohol Use before and after COVID-19 related restrictions among HIV-infected adults in South-Western Uganda. AIDS Behav. 2023;27(6):2005–14.
UNAIDS. Understanding Fast-Track: accelerating action to end the AIDS epidemic by 2030. unaids.org/sites/default/files/media_asset/201506_JC2743_Understanding_FastTrack_en.pdf. 2015.
Ruark AT, Darbes S, Neilands L, Hahn T, Mulauzi J, Mkandawire N, Ssewamala J, Conroy F. A. Mlambe economic and relationship-strengthening intervention increases relationship quality and decreases intimate partner violence among couples in Malawi. AIDS Impact Conference; Stockholm, Sweden. June 12-14.2023.
Swann M. Economic strengthening for retention in HIV care and adherence to antiretroviral therapy: a review of the evidence. AIDS Care. 2018;30(sup3):99–125.
Ssewamala FM, Sauceda JA, Brathwaite R, et al. Suubi + Adherence4Youth: a study protocol to optimize the Suubi intervention for adherence to HIV treatment for youth living with HIV in Uganda. BMC Public Health. 2023;23(1):717.
Funding
This study was funded by the National Institutes of Health under grants R34-AA027983 and K24-AA22586.
Author information
Authors and Affiliations
Contributions
AC led the conceptualization and design of this study, led the analysis, and drafted this manuscript. LD, JH, TN, JM, and FS conceptualized the study and edited the manuscript. ST, NM, and JM assisted with data collection and edited the manuscript. All authors contributed to the interpretation of findings and approved this manuscript.
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the UCSF Human Research Protection Program (HRPP) and the National Health Sciences Research Committee (NHSRC) in Malawi.
Consent for Publication
All authors approve the publication of this manuscript.
Informed Consent
Informed consent was obtained from all participants included in the study.
Competing Interests
There are no conflicts of interest for any of the study authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Conroy, A.A., Hahn, J.A., Neilands, T.B. et al. Pilot Trial Results of Mlambe: An Economic and Relationship-Strengthening Intervention to Address Heavy Drinking and Adherence to Antiretroviral Therapy in Malawi. AIDS Behav 28, 2296–2306 (2024). https://doi.org/10.1007/s10461-024-04326-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-024-04326-x