
Abstract
Patient navigation is a promising strategy for improving health among persons with multiple barriers to HIV care, yet little is known about navigation’s core components. From 24 systematically identified navigation studies, we abstracted navigators’ activities, grouped activities into 20 thematic activity categories, and ordered them by frequency. Subsequently, Principal Components Analysis of activity categories was used identify independent clusters. Accompaniment characterized 71% of navigation programs; ≥ half included health education (58%), collaboration/coordination (58%), linkage-to-care (54%), transportation support (54%), service referrals (50%) and instrumental support (50%). Five unique components (comprising 13 activity categories) were identified: (1) services beyond office, (2) health education and relationship building, (3) accompaniment and instrumental support, (4) locating patients and tracking information, and (5) beyond HIV care. Navigators who located patients or tracked information were less likely to provide accompaniment or instrumental support (r = − 0.60, p = 0.002). Findings can enhance precision in developing, describing, evaluating and improving navigation programs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the United States, HIV disproportionately impacts sexual, racial and ethnic minorities [1], is concentrated among the poor and socially disadvantaged [2, 3] and demonstrates high comorbidity with mental and substance use disorders [4, 5]. Owing to the advent of powerful antiretroviral medications that control viral replication, HIV-related mortality has decreased markedly since peaking in 1995 [6] and continues to decrease [7] as an increasing proportion of people with HIV (PWH) are achieving the viral suppression that maximizes health and prevents transmission. Yet these outcomes vary by age, race, and ethnicity with young people more likely than adults to have undiagnosed infection and to not be virally suppressed [8, 9], and Hispanics/Latinos or Blacks less likely than Whites to have their infection diagnosed [8], to be linked to care in a timely manner or to be virally suppressed [10]. Similar disparities are found for the use of pre-exposure prophylaxis (PrEP), medications that prevent HIV acquisition for those who are HIV-negative. That is, although PrEP has become more accessible and utilized by individuals at risk [11], uptake is much lower among those who are young, of minority race or ethnicity and without private insurance [10, 12, 13].
Many in need of HIV treatment or prevention services do not access them due to a myriad of social, cultural or other barriers that affect healthcare utilization. This is due, in part, to the complex and fragmented nature of HIV services (e.g., varying locations for receiving HIV testing, HIV treatment, other HIV prevention services) and other health-related needs (e.g., behavioral or reproductive health care, social services) relevant for PWH in the United States. Patient navigation is a support service specifically designed to help individuals find their way through complex and often fragmented medical or health-relevant systems. Originally developed to address disparities in cancer mortality [14], patient navigation is increasingly being incorporated in HIV care [15,16,17]. By helping disadvantaged persons address the barriers that undermine timely linkage to and engagement in care and treatment, HIV patient navigation addresses health disparities in viral suppression [15, 18].
Although navigation programming is increasing, the research literature on HIV patient navigation is still relatively limited. However, a recent systematic review suggested preliminary evidence in support of its effectiveness for linkage to HIV care, retention in care, and viral suppression [18]. At the same time, this review made clear several limitations of the current evidence base. On the one hand, two-thirds of the supportive studies were of low methodological quality, and the reporting of navigator characteristics (e.g., level of training, paid vs volunteer, demographic or community matching) and navigator contact with clients or patients (e.g., number of hours, sessions or length of program) was incomplete or inconsistent, limiting ability to examine moderators of program outcomes. Moreover, the authors reported that it was challenging to specify which studies should be included in the review—that is, to determine which interventions were truly ‘navigation’—due to the lack of a clear definition of what constitutes HIV patient navigation.
To address this last concern, our team conducted an analysis of the content of published HIV patient navigation programs to better define HIV patient navigation as implemented in the field. Utilizing the unique opportunity provided by the Mizuno et al. [18] systematic review, we conducted a secondary analysis of these systematically identified studies. Although navigation services are used to support PrEP use, this review is limited to those programs supporting HIV care and treatment. Our aims were to identify and characterize the activities of navigators; to determine which were most common; whether there were essential or defining features; and whether distinct elements of navigator interventions could be distinguished. Our goal was to better define HIV patient navigation as an intervention or strategy—regardless of who was practicing it, what population was receiving it, or in what setting it was implemented—in order to assist in future navigation program development, program evaluation, and program outcome research.
Methods
Database and Search Strategy
As part of a broader literature review on HIV patient navigation, our team conducted a secondary analysis based on the systematic review conducted for Mizuno et al. [18]. We followed the same search strategy. Specifically, a librarian performed a systematic search of the literature utilizing indexing terms and keywords to restrict citations to the following areas: (1) HIV infections, HIV seropositivity, or AIDS serodiagnosis, AND (2) patient navigation or care coordination (see appendix in Mizuno et al. [18] for complete information on search strategies). The automated search was performed in MEDLINE (OVID), EMBASE (OVID), PsycINFO (OVID), and CINAHL (EBSCOhost) online databases for citations published and indexed by January 1, 1996 through April 23, 2018. In addition, supplementary searches were performed in (1) PubMed, Scopus, and the New York Academy of Medicine literature database (http://www.greylit.org), (2) hand searches of key HIV journals in the HIV prevention literature, and (3) reference checks of included studies and reviews identified by the search. Two coders independently screened for relevant titles and abstracts of all citations identified using DistillerSR (Evidence Partners, Ottawa, Canada), and then two coders independently reviewed full reports to determine eligibility, with discrepancies resolved through discussion.
Eligibility
Selected studies reported the use of HIV patient navigation services or navigation-like services. Navigation-like services were not labelled as navigation but described activities broadly consistent with descriptions of patient navigation (e.g., assist PWH to find their way to obtain HIV care and support services, help PWH address barriers so they could utilize HIV care). Studies also needed to be conducted in the United States, be published in English in a peer-reviewed journal and report primary data. Reviews, commentaries, protocols and intervention descriptions without study sample information, guidelines, unpublished materials and conference abstracts were excluded. We followed the Mizuno et al [18] selection strategy, with two differences in our inclusion criteria. First, we included (that is, we did not eliminate) primary data papers that did not report association (i.e., outcome) data, as intervention outcome was not part of this analysis. Second, studies needed to provide descriptions of the navigation intervention and navigator activities with sufficient detail to allow for abstraction.
Data abstraction and coding
Data abstraction of navigator activities occurred in two stages. First, for each relevant citation, all navigator activities mentioned in the papers were abstracted by the first author. These activities were included only if they were identified as being a responsibility of the navigator. For example, case management was sometimes identified as an activity of the navigator (sole duty or shared with a case manager). It was only abstracted when specifically noted to be part of the navigator’s duties.
Activities were then organized into categories, first by reducing redundancies (that is, identical and highly similar activity descriptions), and subsequently by grouping these activities into thematic activity categories. These activity categories were atheoretical and primarily relied on shared words or concepts. For example, activities described as educating or providing information or clarification about a health topic were categorized as ‘health education’, regardless of its format (e.g., classes; one-on-one meetings) or target (e.g., patients, staff). These activity categories were created by two co-authors (LK, CL) and then revised with feedback from the coding team. In this stage, some categories were broken apart further (e.g., transportation was pulled out into its own category due to the high frequency with which it was included relative to a range of other less frequently noted instrumental support activities, so that any distinct role would not be hidden) while others were combined (e.g., various adjunct therapies/interventions combined into an “other interventions” category). Using these categories, pairs of coders independently reviewed each article for described navigator activities and identified which of the activity categories were part of the intervention for that study. When multiple papers described the same navigation intervention (that is, linked studies), the primary study was identified. Papers linked to the primary study or directed to for intervention description by the primary study were reviewed/abstracted to identify navigator activities, but they were not considered primary studies. Discrepancies were resolved through discussion and further review. Frequencies were calculated to identify the most commonly occurring navigator activity categories.
Analyses
Based on abstraction of navigator activities, we identified the frequency of different categories of navigator activities. Principal Components Analysis, a multivariate analysis to reduce data for exploratory purposes [19], was then used to identify whether the navigator activity categories grouped together into meaningful distinct strategies. Specifically, to better understand the underlying structure of navigators’ functions, we conducted a Principal Components Analysis (using varimax rotation to maximize component orthogonality) with the navigator activity categories using IBM SPSS for Windows, Version 21 [20]. Starting with components with an eigenvalue > 1, the number of components was reduced sequentially, examining component stability and item-total correlations, removing items that decreased internal consistency (as measured by Cronbach’s alpha). Component reduction concluded when further reduction forced previously stable components to break apart or internal consistency was reduced below α = 0.60. Pearson product-moment correlations were calculated to examine associations among components.
Results
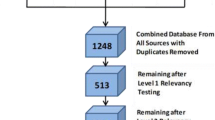
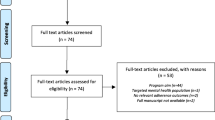
Searches yielded 789 unique citations, with 88 potentially relevant studies. After review, 64 were excluded for the following reasons: qualitative [n = 23], commentaries [n = 12], reviews/guidelines [n = 12], insufficient intervention description [n = 8], protocols [n = 5], and linked studies (same navigation intervention described in multiple citations) [n = 4]. Five papers [21,22,23,24,25] that were linked or directed to for intervention description by a primary paper were reviewed/abstracted for navigator content, but not included as primary studies. This included 24 independent HIV patient navigation studies [15, 26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48] (Fig. 1).

Study flow diagram
HIV Navigator Activities
Navigator intervention activities reported in these studies were grouped into 20 categories. Table 1 provides a list of navigation activity categories ordered according to frequency, examples of specific activities under each activity category, and the intervention studies that included that activity category. The HIV patient navigation activity category most reported was Accompany Patient, which was included in 71% of the studies. Of these, navigators in 76% of studies accompanied to medical or HIV care appointments, and 41% accompanied to behavioral health and social or other (e.g., financial) service appointments. (One study navigator accompanied to only social services whereas other navigators accompanied to both medical and social/behavioral appointments.) Three studies did not describe the type of appointments to which navigators accompanied patients. Navigation activity categories mentioned by at least half of the intervention studies included Educate About Health (58%), Collaborate/Coordinate Care (58%), Link Patients to Care (54%), Arrange/Support Transportation (54%), Refer to Services (50%) and Provide Instrumental Support (50%). One third to just under half of the interventions included: Assess/Address Needs or Barriers (46%), Build a Relationship to Guide Patient (46%), Make Appointments (46%), Make Home/Jail/Other Location Visits (42%), Locate Patient (37%) and Remind Patient (37%). Support Expectations/Future Goals, and Support ART Adherence were each mentioned by one-quarter of the studies, and the following navigation activity categories were infrequently mentioned (that is, by less than one-quarter of the studies): Use/Track Information in a Database (21%), Develop/Teach Skills (17%), Provide Case Management (17%), Serve as a Role Model (12%), and Deliver Adjunct Interventions (12%).
Structure of Navigator Activities Principal Components Analysis of the 20 navigator activity categories revealed eight initial components with an eigenvalue > 1. Following procedures previously described, these were reduced to five with α ≥ 0.60, which can be found in Table 2. Thirteen navigator activity categories characterized the five components, with item-total component correlations ranging from r = 0.42 to r = 0.60. Component 1 (α = 0.76), which was characterized by two types of categories—providing or arranging for transportation for the patient, and making visits to either the patient’s home or another external setting (e.g., a jail)—appeared to capture the distinct role that navigators play in providing services beyond the confines of the clinic or office. Five activities characterized Component 2 (α = 0.74) including: being a role model (e.g., sharing personal experiences that can help the patient), building a relationship with the patient (e.g., serving as a coach or mentor), helping to build patients’ skills (either HIV specific, such as serostatus disclosure, or general, such as job seeking skills), providing the patient with reminders (e.g., of upcoming appointments, drug refills), and providing health education. This component appeared to capture the importance of the relationship between patients and navigators that is often the conduit to health education, mentoring and skill-building. The third component (α = 0.63) comprised two items: accompanying the patient to appointments or other visits, and providing instrumental support (i.e., tangible things such as arranging for childcare or assistance with medical benefits) that sets the stage for utilization of health services by removing barriers. The fourth component (α = 0.61) comprised two items: using a database (e.g., to track information about a patient’s location/contact information, or update regarding appointments and other relevant data) and locating patients (e.g., for outreach or finding patients lost to care). Finally, the two items that made up the fifth component (α = 0.60)—helping the patient to set goals or expectations for the future (e.g., making a plan for the future) and making referrals to other services (e.g., social services, other health care [e.g., reproductive health or mental health], or supportive social networks)—may not seem related on the surface but together point to the important role of addressing the patient holistically and thinking beyond HIV care alone.
Table 3 presents the inter-correlations among these components. A statistically significant negative association between Component 4 (“Locating and Tracking”) and Component 3 (“Escort and Support”) (r = –0.60, p = 0.002) indicates that navigators whose duties involve outreach, locating or tracking of patients are less likely to accompany or provide additional support. There is a tendency for navigators who do engage in accompaniment and support (Component 3) to also be involved in activities that are focused ‘beyond the office’ (Component 1) (r = 0.36, p < 0.09).
Discussion
As a strategy designed to enhance the delivery of medical care to disadvantaged persons, patient navigation is increasingly being employed by health care providers addressing illnesses for which there are health disparities and a high burden of disease for vulnerable populations. In HIV, it is increasingly being used to support linkage to and engagement in HIV care, HIV care retention and viral suppression, and access to and utilization of PrEP for HIV prevention. Often combined with other services (e.g., case management, social work, housing or financial services), performed by a variety of actors (e.g., care coordinators, nurses, social workers, community health workers, peers or lay workers) or designed to meet distinct needs of different populations (e.g., youth, individuals with mental illness or substance use disorders, persons leaving correctional facilities, individuals with minority cultural or linguistic backgrounds), HIV patient navigation takes many forms and is rarely evaluated apart from other program components with which it is combined. Toward the objective of determining whether there are universal or shared features of HIV patient navigation as it is currently being practiced, we delved deeply into the actions and roles of navigators described in systematically identified and published navigation intervention studies. We identified five distinct domains of navigation, along with seven activity categories that characterized at least half of the interventions. Although we did not identify a universal activity that characterized all navigation interventions, one activity—accompaniment—came close.
Accompaniment was the most universally described navigator activity, characterizing nearly three-quarters of all interventions. As a concept related to health, the term “accompaniment” has a range of meanings, emerging from liberation theology of Latin America and evolving to reflect the psychosocial act of travelling along with and alongside of individuals who are marginalized, often those with a history of various traumas including poverty [49]. In this way, accompaniment reflects the acts of listening, of witnessing, and of offering flexible and strategic support [49]. Farmer [50, 51] incorporates this notion of accompaniment—to go with someone on their journey and experience the journey as they do—as a cornerstone of his model of social medicine for the poor, with para-professional community health workers commonly serving as the accompagnateurs for those in need of medical care. Although accompaniment in the navigation interventions we examined typically involved escorting individuals to their medical or adjunct appointments to ensure that they arrived, received services and understood the provider information and instructions, it is possible that this act conveyed something more to individuals receiving navigation services. That is, as taking the time to travel with the individual to appointments conveys an interest and investment in their health and well-being, the awareness of that investment may play an important role in establishing or enhancing the relationship, which according to both navigators and patients is an essential mechanism by which clients are connected to care [52, 53]. To the extent that accompaniment places the navigator on a path with the patient, it may provide the conduit to education, and the motivation to make the changes patients need in order to improve their health, allowing navigators to model behaviors and skills, build client independence and self-efficacy [52] and reinforce trust [53].
At the same time, not all interventions included accompaniment. Results of the components analysis revealed that accompaniment and instrumental support are less likely to be parts of navigation programs when locating individuals or tracking their information within a database are included. Indeed, although database tracking/updating was not a common navigator activity, a scan of the five interventions that did include this activity [28, 29, 35, 40, 45] revealed that none of them included accompaniment. It’s possible that navigation programs for which an important aspect includes using data systems (e.g., HIV surveillance data, clinic data) to locate individuals who’ve not linked to or remained in HIV care in order to re-link and engage them back into care are not able to provide the more intensive support that accompaniment requires. Public health ‘Data-to-Care’ strategies have been successful at using surveillance-based laboratory data (i.e., CD4 and VL test results) to identify patients who’ve fallen out of HIV care, and sharing their names with health departments so that outreach workers can locate them and help them return to care [54, 55]. These outreach programs are themselves labor intensive with a necessary focus on initial stages of engagement. Should locating and tracking activities be part of data-to-care programs, this would explain why other resource-intense services such as accompaniment are typically not also provided. Alternatively, these two types of activities might be provided to patients as part of a broader support program but delivered by staff with different roles (that is, roles not specifically assigned to navigators).
On the surface, it may seem that the five components or domains of navigation are inconsistent with the results of the frequency analysis. That is, not all frequently occurring activities are included in the five domains, and some activities of the five domains do not occur frequently. However, it is important to note that these findings tell us about different ways of thinking about navigation. On the one hand, the components analysis maps out higher-level domains defining the construct of navigation. From these five domains, we can say that key defining features involve: going beyond office-based care (and meeting the patient where they are at); building a relationship through which individuals receiving navigation services pick up information and skills; accompanying individuals on their journey to wellness and providing strategic support that makes this journey feasible; being aware and not losing sight of individuals by locating them or tracking them so that they don’t miss out on care; and focusing more holistically on their goals and non-HIV care needs. The marginally significant positive association of “Beyond the Office” (home visits and transportation support) and “Escort and Support” (accompaniment and instrumental support) may reflect the fact that both address practical barriers to service utilization that patients experience. On the other hand, the frequency analysis tells how each domain is being enacted. For example, if we look at the navigator activity categories that are commonly included (by at least half of the programs), we can see that the “Escort and Support” domain is almost always enacted through both accompaniment (72%) and instrumental support (50%). “Relate and Educate” is typically enacted through health education (56%) and not infrequently with a specific goal to build a relationship with the patient (46%). “Beyond the Office” is typically enacted with providing or arranging for transportation support (54%) but not infrequently with home or other location visits by the navigator (42%). A focus “Beyond HIV Care” is often enacted via referral to services (50%) but also sometimes enacted by focusing on broad goals or expectations for the future (25%). As previously noted, “Locate and Track” may be a domain included in only certain types of navigation programs, with activities of locating patients and tracking information utilizing a database not frequently enacted by programs (37% and 21%, respectively).
Several high frequency items did not map directly onto a specific domain, which may reflect the lack of specificity of those activities. For example, collaboration/coordination is a role as well as an activity, and it may have co-occurred with so many of the other activities across the domains that it could not be unique to any single domain. Other less frequently mentioned activities may have suffered from lack of distinction as navigators’ activities. For example, assessing needs and addressing barriers can be functions of case managers, care coordinators and patient navigators, or may even reflect shared duties. Indeed, case management itself was a navigator activity sometimes mentioned, and it was included in our analysis only when it was specifically noted as being something the navigator did. Thus, our analysis reflects navigators’ roles and activities and not necessarily navigation-type programs overall. These issues highlight the need for increased clarity regarding navigator roles and duties, as well as increased clarity of published descriptions of navigator interventions. Although in theory case management, care coordination and patient navigation are sometimes said to be distinguished by characteristics such as whether they are time-limited, for newly-diagnosed vs established patients, for comorbid conditions vs economic and sociocultural challenges, or even by whether they are provided by peers or professionals, in practice, these distinctions appear to be blurred. Clear and consistent definitions will be helpful as we better understand and replicate effective navigator interventions and to determine which elements are most likely to lead to improved outcomes [18, 56].
Finally, less common activities might have reflected unique ways that navigator programs are tailored to the populations they serve. Often, navigation is one element of a multi-component intervention which may be tailored to, or uniquely combined with other services specific for an intended population. For example, programs for those being released from corrections facilities might require the navigator to engage in discharge planning or liaise with courts [32, 42] whereas navigation services for marginally housed or homeless individuals might require specialized knowledge about and outreach to housing agencies and the provision of rental assistance [57, 58]. Still other navigation programs might be combined with the delivery of other evidence-based HIV interventions, or occupational or mental health interventions, depending on the skill set or training of the navigator. This reflects less of a problem for understanding the core aspects of navigation and more of a need to clearly identify auxiliary activities of a navigator.
This study is not without limitations. Navigation programs that were not evaluated or published would have been missed. Yet, the use of a systematic approach to the literature search and program identification does decrease study selection bias. However, as the use of the terms ‘navigation’ and patient navigation interventions were introduced to HIV care fairly recently, we chose to include ‘navigation-like’ interventions so as not to miss relevant programs. To do so we identified interventions that included persons directly helping patients address barriers and find their way to obtain HIV care and other needed services. On closer inspection, these ‘navigation-like’ interventions often described case management or care coordination programs that were multi-faceted or were described as ‘enhanced’ or ‘intensified’ beyond usual services. Nevertheless, inclusion of several studies needed to rely on pre-determined expectation of what constitutes patient navigation, and this may have added bias to the results.
Due to limited space, published reports are not always written to fully describe all of a navigation program’s activities. Where there were linked program descriptions, we reviewed them. However, not all studies had linked papers and omissions due to these limited descriptions may be reflected in the analysis. Further, abstraction processes can be imprecise and even with the use of multiple coders, interpretation differences could have affected activity delineation. Similarly, decisions about ‘lumping’ or ‘splitting’ activities into meaningful navigator categories necessarily reflects some subjectivity. Future research will want to continue to examine the clustering of navigators’ activities as their use and their roles expand. Finally, internal reliability was in the borderline range (that is, alpha ≥ 0.60 to < 0.70) for several of the navigation domains identified through Principal Components Analysis. We set a cut-off at alpha = 0.6, which is not uncommon in exploratory investigations such as this one. The small number of items within each of these components also likely contributed to the lower internal reliability. Further work is needed to determine if these are stable components or whether they fluctuate as new and/or more precisely described navigation programs are implemented.
To our knowledge, this represents the first attempt to use empirical data to examine and refine the construct of healthcare navigation as it applies to HIV care. We identified seven activity categories common to most HIV patient navigator programs (accompaniment, education, collaboration/coordination, linkage services, transportation support, referrals, and instrumental support), and five overarching navigator domains. These domains—providing services outside of the confines of the office, educating about health and building a relationship through which guidance is provided, accompanying the patient and providing direct instrumental support to address barriers to care, locating patients and tracking information about location or care in a database, and addressing needs indirectly related to HIV care—capture the unique approach that HIV patient navigation can add to current healthcare services. Further, this information about navigator roles and activities can be useful not only to further research on the effectiveness of patient navigation for improving key HIV care continuum outcomes, but also as a guide for clinics or community organizations that are developing or enhancing their own patient navigation services.
Code availability
Standard SPSS software.
References
Centers for Disease Control and Prevention. HIV Surveillance Report, 2018 (updated). 2020. http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. Accessed 4 Sept 2020.
Centers for Disease Control and Prevention. Characteristics associated with HIV infection among heterosexuals in urban areas with high AIDS prevalence—24 cities, United States, 2006–2007. MMWR Morb Mortal Wkly Rep. 2011;60(31):1045–9.
Pellowski JA, Kalichman SC, Matthews KA, Adler N. A pandemic of the poor: social disadvantage and the U.S. HIV epidemic. Am Psychol. 2013;68(4):197–209.
Cook JA, Burke-Miller JK, Steigman PJ, et al. Prevalence, comorbidity, and correlates of psychiatric and substance use disorders and associations with HIV risk behaviors in a multisite cohort of women living with HIV. AIDS Behav. 2018;22(10):3141–54.
Gaynes BN, Pence BW, Eron JJ Jr, Miller WC. Prevalence and comorbidity of psychiatric diagnoses based on reference standard in an HIV+ patient population. Psychosom Med. 2008;70(4):505–11.
Centers for Disease Control and Prevention. HIV Mortality—2018. 2018. https://www.cdc.gov/hiv/pdf/library/slidesets/cdc-hiv-surveillance-mortality-2018.pdf. Accessed 6 Nov 2020.
Bosh KA, Johnson AS, Hernandez AL, et al. Vital signs: deaths among persons with diagnosed HIV infection, United States, 2010–2018. MMWR Morb Mortal Wkly Rep. 2020;69(46):1717–24.
Centers for Disease Control and Prevention. Estimated HIV incidence and prevalence in the United States, 2014–2018. 2020. https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-supplemental-report-vol-25-1.pdf. Accessed 4 Sept 2020.
Koenig LJ, Hoyer D, Purcell DW, Zaza S, Mermin J. Young people and HIV: A call to action. Am J Public Health. 2016;106(3):402–5.
Centers for Disease Control and Prevention. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 dependent areas, 2018. 2020. https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-supplemental-report-vol-25-2.pdf. Accessed 4 Sept 2020.
Kamitani E, Wichser ME, Adegbite AH, et al. Increasing prevalence of self-reported HIV preexposure prophylaxis use in published surveys: a systematic review and meta-analysis. AIDS (London, England). 2018;32(17):2633–5.
Marcus JL, Hurley LB, Hare CB, Silverberg MJ, Volk JE. Disparities in uptake of HIV preexposure prophylaxis in a large integrated health care system. Am J Public Health. 2016;106(10):e2–3.
Serota DP, Rosenberg ES, Thorne AL, Sullivan PS, Kelley CF. Lack of health insurance is associated with delays in PrEP initiation among young black men who have sex with men in Atlanta, US: a longitudinal cohort study. J Int AIDS Soc. 2019;22(10):e25399.
Freeman HP, Rodriguez RL. History and principles of patient navigation. Cancer. 2011;117(15 Suppl.):3539–42.
Bradford JB, Coleman S, Cunningham W. HIV system navigation: an emerging model to improve HIV care access. AIDS Patient Care STDS. 2007;21(Suppl. 1):S49–58.
Farrisi D, Dietz N. Patient navigation is a client-centered approach that helps to engage people in HIV care. HIV Clin. 2013;25(1):1–3.
Thompson MA, Mugavero MJ, Amico KR, et al. Guidelines for improving entry into and retention in care and antiretroviral adherence for persons with HIV: evidence-based recommendations from an International Association of Physicians in AIDS Care panel. Ann Intern Med. 2012;156(11):817–33.
Mizuno Y, Higa DH, Leighton CA, Roland KB, Deluca JB, Koenig LJ. Is HIV patient navigation associated with HIV care continuum outcomes? AIDS (London, England). 2018;32(17):2557–71.
Bryant FB, Yarnold PR. Principal-components analysis and exploratory and confirmatory factor analysis. In: Grimm LG, Yarnold PR, editors. Reading and understanding multivariate statistics. Washington, DC: American Psychological Association; 1995. p. 99–136.
SPSS for Windows [computer program]. 2020. Version 21. Amonk, NY.
Irvine MK, Chamberlin SA, Robbins RS, et al. Improvements in HIV care engagement and viral load suppression following enrollment in a comprehensive HIV care coordination program. Clin Infect Dis. 2015;60(2):298–310.
Jordan AO, Cohen LR, Harriman G, Teixeira PA, Cruzado-Quinones J, Venters H. Transitional care coordination in New York City jails: facilitating linkages to care for people with HIV returning home from Rikers Island. AIDS Behav. 2013;17(Suppl. 2):S212-219.
Koester KA, Morewitz M, Pearson C, et al. Patient navigation facilitates medical and social services engagement among HIV-infected individuals leaving jail and returning to the community. AIDS Patient Care STDS. 2014;28(2):82–90.
Myers JJ, Koester KA, Kang Dufour MS, Jordan AO, Cruzado-Quinone J, Riker A. Patient navigators effectively support HIV-infected individuals returning to the community from jail settings. Int J Prison Health. 2017;13(3–4):213–8.
Stitzer M, Matheson T, Cunningham C, et al. Enhancing patient navigation to improve intervention session attendance and viral load suppression of persons with HIV and substance use: a secondary post hoc analysis of the Project HOPE study. Addict Sci Clin Pract. 2017;12(1):16.
Andersen M, Hockman E, Smereck G, et al. Retaining women in HIV medical care. JANAC J Assoc Nurses AIDS Care. 2007;18(3):33–41.
Andersen M, Paliwoda J, Kaczynski R, et al. Integrating medical and substance abuse treatment for addicts living with HIV/AIDS: evidence-based nursing practice model. Am J Drug Alcohol Abuse. 2003;29(4):847–59.
Asamsama OH, Squires L, Tessema A, et al. HIV nurse navigation: charting the course to improve engagement in care and HIV virologic suppression. J Int Assoc Provid AIDS Care. 2017;16(6):603–7.
Bove JM, Golden MR, Dhanireddy S, Harrington RD, Dombrowski JC. Outcomes of a clinic-based surveillance-informed intervention to relink patients to HIV care. JAIDS J Acquir Immune Defic Syndr. 2015;70(3):262–8.
Cabral HJ, Davis-Plourde K, Sarango M, Fox J, Palmisano J, Rajabiun S. Peer support and the HIV continuum of care: results from a multi-site randomized clinical trial in three urban clinics in the United States. AIDS Behav. 2018;22(8):2627–39.
Cabral HJ, Tobias C, Rajabiun S, et al. Outreach program contacts: do they increase the likelihood of engagement and retention in HIV primary care for hard-to-reach patients? AIDS Patient Care STDS. 2007;21(Suppl. 1):S59–67.
Cunningham WE, Weiss RE, Nakazono T, et al. Effectiveness of a peer navigation intervention to sustain viral suppression among HIV-positive men and transgender women released from jail: the LINK LA randomized clinical trial. JAMA Intern Med. 2018;178(4):542–53.
Gardner LI, Metsch LR, Anderson-Mahoney P, et al. Efficacy of a brief case management intervention to link recently diagnosed HIV-infected persons to care. AIDS (London, England). 2005;19(4):423–31.
Irvine MK, Chamberlin SA, Robbins RS, Kulkarni SG, Robertson MM, Nash D. Come as you are: improving care engagement and viral load suppression among HIV care coordination clients with lower mental health functioning, unstable housing, and hard drug use. AIDS Behav. 2017;21(6):1572–9.
Keller J, Heine A, LeViere AF, et al. HIV patient retention: the implementation of a North Carolina clinic-based protocol. AIDS Care. 2017;29(5):627–31.
Kral AH, Lambdin BH, Comfort M, et al. A strengths-based case management intervention to reduce HIV viral load among people who use drugs. AIDS Behav. 2018;22(1):146–53.
Leider J, Fettig J, Calderon Y. Engaging HIV-positive individuals in specialized care from an urban emergency department. AIDS Patient Care STDS. 2011;25(2):89–93.
Maulsby C, Charles V, Kinsky S, Riordan M, Jain K, Holtgrave D. Positive charge: filling the gaps in the U.S. HIV continuum of care. AIDS Behav. 2015;19(11):2097–107.
Metsch LR, Feaster DJ, Gooden L, et al. Effect of patient navigation with or without financial incentives on viral suppression among hospitalized patients with HIV infection and substance use: a randomized clinical trial. JAMA J Am Med Assoc. 2016;316(2):156–70.
Mignano JL, Miner L, Siedl K, et al. Results and implications of routine HIV testing in the inpatient setting: a descriptive analysis. Popul Health Manag. 2018;21(1):40–5.
Molitor F, Waltermeyer J, Mendoza M, et al. Locating and linking to medical care HIV-positive persons without a history of care: findings from the California Bridge Project. AIDS Care. 2006;18(5):456–9.
Myers JJ, Kang Dufour MS, Koester KA, et al. The effect of patient navigation on the likelihood of engagement in clinical care for HIV-infected individuals leaving jail. Am J Public Health. 2018;108(3):385–92.
Rich JD, Holmes L, Salas C, et al. Successful linkage of medical care and community services for HIV-positive offenders being released from prison. J Urban Health. 2001;78(2):279–89.
Shacham E, López JD, Brown TM, Tippit K, Ritz A. Enhancing adherence to care in the HIV care continuum: the barrier elimination and care navigation (BEACON) project evaluation. AIDS Behav. 2018;22(1):258–64.
Sitapati AM, Limneos J, Bonet-Vázquez M, Mar-Tang M, Qin H, Mathews WC. Retention: building a patient-centered medical home in HIV primary care through PUFF (Patients Unable to Follow-up Found). J Health Care Poor Underserved. 2012;23(3 Suppl.):81–95.
Teixeira PA, Jordan AO, Zaller N, Shah D, Venters H. Health outcomes for HIV-infected persons released from the New York City jail system with a transitional care-coordination plan. Am J Public Health. 2015;105(2):351–7.
Wohl AR, Dierst-Davies R, Victoroff A, et al. Implementation and operational research: the navigation program: an intervention to reengage lost patients at 7 HIV clinics in Los Angeles County, 2012–2014. JAIDS J Acquir Immune Defic Syndr. 2016;71(2):e44–50.
Wohl AR, Ludwig-Barron N, Dierst-Davies R, et al. Project engage: snowball sampling and direct recruitment to identify and link hard-to-reach HIV-infected persons who are out of care. JAIDS J Acquir Immune Defic Syndr. 2017;75(2):190–7.
Watkins M. Psychosocial accompaniment. J Soc Polit Psychol. 2015;3(1):324–41.
Farmer P. Accompaniment as policy [transcript of speech]. 2011. https://www.lessonsfromhaiti.org/press-and-media/transcripts/accompaniment-as-policy/. Accessed 22 May 2020.
Farmer P. To repair the world: Paul Farmer speaks to the next generation. Oakland: University of California Press; 2013.
Roland KB, Higa DH, Leighton CA, Mizuno Y, DeLuca JB, Koenig LJ. Client perspectives and experiences with HIV patient navigation in the united states: a qualitative meta-synthesis. Health Promot Pract. 2020;21(1):25–36.
Roland KB, Higa DH, Leighton CA, Mizuno Y, DeLuca JB, Koenig LJ. HIV patient navigation in the United States: a qualitative meta-synthesis of navigators’ experiences. Health Promot Pract. 2020. https://doi.org/10.1177/1524839920982603
Fanfair RN, Khalil G, Camp N, et al. Health department randomized trial to re-engage out-of-care HIV infected persons—The Cooperative Re-engagement Controlled Trial. 2019. Conference on Retroviruses and Opportunistic Infections. Seattle, Washington
Sweeney P, DiNenno EA, Flores SA, et al. HIV data to care-using public health data to improve HIV care and prevention. JAIDS J Acquir Immune Defic Syndr. 2019;82(Suppl. 1):S1–5.
Giacamazzo A, Challacombe L. Health navigation in HIV services: A review of the evidence. CATIE: Canadian AIDS Treatment and Information Exchange. 2018. https://www.catie.ca/en/pif/fall-2018/health-navigation-hiv-services-review-evidence. Accessed 26 May 2020.
Bowen EA, Canfield J, Moore S, Hines M, Hartke B, Rademacher C. Predictors of CD4 health and viral suppression outcomes for formerly homeless people living with HIV/AIDS in scattered site supportive housing. AIDS Care. 2017;29(11):1458–62.
Maskay MH, Cabral HJ, Davila JA, et al. Longitudinal stigma reduction in people living with HIV experiencing homelessness or unstable housing diagnosed with mental health or substance use disorders: an intervention study. Am J Public Health. 2018;108(Suppl. 7):S546–51.
Funding
NA.
Author information
Authors and Affiliations
Contributions
LJK: conceptualized the review, oversaw the intervention abstraction and prepared the original draft; DHH: conducted the statistical analyses; JBD: conducted the literature review; LJK, DHH, CAL, KBR and YM: coded studies; all authors edited the paper and revised it critically for important intellectual contributions.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare they have no financial or competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Koenig, L.J., Higa, D.H., Leighton, C.A. et al. Toward An Enhanced Understanding of HIV Patient Navigation as a Health Care Intervention: An Analysis of Navigation in Practice. AIDS Behav 25, 4044–4054 (2021). https://doi.org/10.1007/s10461-021-03244-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-021-03244-6