
Abstract
In adults living with HIV, pharmacy refill data are good predictors of virologic failure (VF). The utility of pharmacy refill data for predicting VF in adolescents has not been reported. We evaluated data from 291 adolescents on antiretroviral therapy. The main outcome measure was VF, defined as two consecutive HIV viral load measurements ≥ 400 copies/mL during 24-months of follow-up. Pharmacy refill non-adherence was defined as two consecutive refill adherence measurements < 95% during the same period. Fifty-three (18%) adolescents experienced VF. One hundred twenty-eight (44%) adolescents had refill non-adherence. Refill non-adherence had poor discriminative ability for indicating VF (receiver operating characteristic AUC = 0.60). Sensitivity and specificity for predicting VF was poor (60% (95% CI 46–74%) and 60% (95% CI 53–66%), respectively). The lack of a viable surrogate for VF in adolescents highlights the urgent need for more access to virologic testing and novel methods of monitoring adolescent treatment adherence.
Resumen
En los adultos que viven con el VIH, los datos en la farmacia sobre la renovación de recetas médicas son buenos predictores del fracaso virológico. La utilidad de los datos en la farmacia sobre la renovación de recetas médicas para predecir fracaso virológico en adolescentes no ha sido reportada. Se evaluaron los datos de 291 adolescentes en terapia antirretroviral. La principal medida de resultado fue el fracaso virológico, definida como dos medidas consecutivas de carga viral del VIH ≥ 400 copias/ml durante 24 meses de seguimiento. La no adherencia a la renovación de recetas médicas en la farmacia se definió como dos medidas consecutivas de adherencia a la renovación de recetas médicas < 95% durante el mismo período. Cincuenta y tres (18%) adolescentes tuvieron fracaso virológico. Ciento veintiocho (44%) adolescentes tuvieron no adherencia a la renovación de recetas médicas. El no-adherencia a la renovación de recetas médicas tuvo poca capacidad para indicar fracaso virológico (característica de funcionamiento del receptor AUC = 0.60). La sensibilidad y especificidad para predecir fracaso virológico fue deficiente (60% (95%: 46–74%) y 60% (95% CI 53–66%), respectivamente). La falta de un sustituto viable para el fracaso virológico en los adolescentes resalta la necesidad urgente para más acceso a las pruebas virológicas y métodos novedosos para monitorear la adherencia del tratamiento en los adolescentes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Worldwide, adolescent HIV-related deaths have more than tripled since 2000, making it the second most common cause of adolescent mortality globally and the leading cause in Africa [1]. Adolescents are the only age group around the world for which AIDS deaths rose between 2001 and 2012 [2, 3]. Infants perinatally infected with HIV during the time of peak incidence in high-prevalence settings, are now reaching adolescence [4]. Many have been taking antiretroviral therapy (ART) for more than 10 years. Compared with younger children and adults, adolescents are more likely to exhibit variability in their daily activities and to experiment with risk-taking behaviors [5, 6]. Adolescents who achieved virologic suppression on antiretroviral therapy have been shown to have a more rapid time to virologic failure (VF) compared to adults [7].
Adherence is strongly associated with virologic response in a dose-dependent manner [8]. Viral load monitoring can improve counselling and clinical decision-making, but is frequently unavailable in low-resource settings [9]. Immunologic criteria are often used in lieu of viral load testing but CD4 + T lymphocyte cell count (CD4 count) criteria have been shown in adults to miss nearly half of all VF cases due to the fact that immunologic decline tends to follow, instead of precede, viral load increases [10]. Substantial misclassification of ART success and failure with immunologic monitoring can happen in both directions. Because of natural variability in CD4 counts, using immunologic criteria as a sole indicator of VF can also lead to premature switches to second-line regimens [11, 12]. Multiple studies have shown that immunologic criteria have poor sensitivity and specificity in identifying VF in both adults and children [13, 14].
Researchers have increasingly turned to pharmacy refill monitoring as a low-cost, simple method of tracking adherence. Pharmacy records have been found to be more strongly associated with virologic outcomes than self-reported adherence data in adults [15]. In addition, Bisson et al. reported that pharmacy refill data were more accurate predictors of VF than CD4 count changes among adults newly starting antiretroviral treatment in Botswana [16]. This association has yet to be studied in a treatment-experienced population or among adolescents. We hypothesized that pharmacy refill would be less predictive in adolescents due to the fact that adolescents frequently have autonomy over medication-taking even when they do not obtain their own refills. This difference in control over medication taking versus obtaining refills potentially delinks the expected association between obtaining refills regularly and taking medications regularly. Given low access to viral load monitoring and the potential for available metrics to predict VF, we sought to determine and compare the discriminative abilities of pharmacy refill measured adherence and immunological criteria for VF in adolescents.
Methods
Participants and Procedures
Three hundred primarily perinatally HIV-infected adolescents (aged 10– < 20 years) were enrolled in an observational study at the Botswana-Baylor Children’s Clinical Centre of Excellence in Gaborone, Botswana beginning in October 2012. This is a large pediatric HIV treatment and referral center in the capital city, which opened in 2003. Participants had a minimum of 6 months of antiretroviral treatment experience at the time of study enrollment. Study participants obtained standard-of-care monitoring and treatment per the Botswana National HIV Treatment Guidelines, including HIV viral load testing and CD4 + T-lymphocyte counts every 3 months [17]. Refill adherence measurements were obtained with every medication refill with refill frequency being determined by the treatment team. In addition, adherence to treatment was monitored using microelectronic medication (MEMS) [18] caps on the adolescents’ medication bottles. The adolescents and staff at the treatment site were blinded to the MEMS data to help minimize incentives to open the medication bottles when doses were not taken. Data from the first 24 months of follow-up were included in this analysis.
Definitions
Virologic Treatment Failure (VF)
VF was defined as at least two consecutive viral loads > 400 copies/mL during the 24-month follow-up period or a single viral load > 400 copies/mL if it was the last viral load obtained before an adolescent failed to follow-up for scheduled monitoring.
Refill Non-adherence
Refill non-adherence was evaluated as both a continuous variable and a dichotomous variable. The dichotomous refill non-adherence variable allows for direct comparison to the dichotomous immunologic failure variable and classifies refill non-adherence as at least two consecutive refill adherence measurements < 95% during the 24-month follow-up period. The continuous variable was calculated as the number of visits at which adherence was < 95% divided by the total number of visits, reported as a percentage.
Immunologic Failure
Immunologic failure was defined as worsening WHO immune status classification (e.g. from mild to advanced or from advanced to severe CD4 levels) at any point during 24-month follow-up [19].
Adolescent Autonomy
Adolescents’ autonomy over obtaining their medications was assessed using a 3-point scale. (1 = adolescent went to the clinic and picked up medicines alone; 2 = adolescent went to the clinic and picked up medications accompanied by someone else; 3 = someone else went to the clinic and picked up the adolescent’s medicines for him or her.) Adolescents’ autonomy over taking their medicines was assessed using a 4-point scale. (1 = “On most days, I took my medicines by myself with nobody reminding me or watching me;” 2 = “On most days, I took my medicine by myself, but somebody reminded me to take them;” 3 = “On most days, somebody gave me my medicines when it was time for me to take them but I took them by myself;” 4 = “On most days, somebody gave me my medicines and watched me take them.”) Autonomy scores at each study visit were averaged over the 24-month study follow-up period.
MEMS Adherence
Electronic medication event monitoring systems (MEMS) [18] caps were utilized with blinding of Botswana-based members of the study team to the MEMS data to minimize social desirability bias. MEMS adherence was calculated based on the number of medication cap openings divided by the number of doses prescribed, and were truncated at 100% per day (with days beginning and ending at 3AM to minimize dosing errors).
Data Analysis
Data were collected and stored using Research Electronic Data Capture (REDCap) Software [20]. Logistic regression and receiver operating characteristic (ROC) analysis assessed the associations of the two-comparator measures of refill non-adherence and immunologic failure with the outcome of VF. ROC analysis also was applied to the comparison between MEMS adherence and VF. Test characteristics were calculated to measure sensitivity and specificity of both refill non-adherence and immunologic failure as diagnostic tests for VF. The ROC curves were compared through non-parametric comparison of areas under the curve (AUC). To further characterize differences between age and medication-taking autonomy among adolescents with and without VF, Wilcoxon rank-sum tests were performed. Pearson’s correlation was used to describe the correlation between age and autonomy. All analyses were completed using STATA 14 software [21].
Results
291 adolescents were included in the analyses. Potential study participants were excluded if they left the study before completing 24 months of follow-up (N = 7) or because genotypic resistance testing indicated that they had moderate or severe resistance to their antiretroviral regimen (N = 2) that might have compromised their ability to achieve and sustain virologic suppression even with perfect adherence to their medications. Subject characteristics are summarized in Table 1. The range of ages was 10.1–19.9 years at study entry with ages skewed toward younger adolescents. Time on treatment at study entry ranged from 6 months to 11.5 years.
53 adolescents (18%) met the pre-defined criteria for VF. With the expectation that each adolescent would have a viral load result at least every 3 months, 84% of expected viral load values (n = 1957) were available for the 24 month follow-up interval. The median number of viral loads per adolescent was 7 (IQR 6–7). Those with VF were older (median age 16.1 years (IQR 14.2–17.7) versus 12.9 years (IQR 11.5–14.7) at study entry, p < 0.01) and had higher levels of autonomy over obtaining their pharmacy refills (median refill score 1.49 (IQR 1.37–1.61) versus 1.78 (IQR 1.74–1.83), p < 0.01). Older adolescents were more likely than younger adolescents to have increased autonomy over obtaining their refills (Pearson’s correlation coefficient − 0.74, p < 0.01) and over taking their medicines daily (Pearson’s correlation coefficient − 0.66, p < 0.01). However, there was only a moderate correlation between refill autonomy and medication-taking autonomy (Pearson’s correlation coefficient 0.58, p < 0.01). Median time on treatment at entry into the study was ~ 7.5 years for both those with and without VF (p > 0.5).
128 adolescents met our definition of refill non-adherent during the 24-month study period and 32 (25.0%) of these individuals experienced VF during the same time period. Of 163 adolescents who did not meet the definition of refill non-adherence, 21 (12.9%) also experienced VF. The odds of having VF was 2.3 times higher among individuals with refill non-adherence than among those who are refill adherent (95% CI 1.2–4.1; p < 0.01).
109 adolescents had immunologic failure during the 24-month study period and 34 (31.2%) of these individuals also experienced VF during the same time period. 182 adolescents maintained or improved their CD4 + T-lymphocyte count and 19 (10.4%) of these individuals also experienced VF. The odds of having VF was 5.6 times higher among individuals with immunologic failure than those who did not have immunologic failure (95% CI 3.0–10.6; p < 0.001) (Fig. 1).

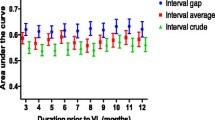
ROC curve for refill non-adherence and immunologic failure when used to identify patients with virologic failure. Blue and green lines are observed dichotomous and continuous refill non-adherence values, respectively, and the red line demonstrates observed immunologic failure values. The graphs therefore represent the sensitivity graphed against the 1-specificity that would result if each observed refill non-adherence or immunologic failure were used as a diagnostic test for virologic failure. The AUC was 0.58 (95% CI 0.50–0.66) for dichotomous refill non-adherence, 0.69 (95% CI 0.61–0.76) for continuous refill non-adherence and 0.66 (95% CI 0.58–0.73) for immunologic failure. The reference line represents an AUC of 0.50, what would be expected with a measure based on flipping a coin
Test characteristics for refill non-adherence and immunologic failure compared to the outcome of VF are outlined in Table 2. ROC analysis resulted in an area under the curve (AUC) of 0.69 (95% CI 0.61–0.76) for the continuous refill measure and 0.58 (95% CI 0.50–0.66) for the dichotomous refill measure. The AUC for the dichotomous immunologic failure measure was 0.66 (95% CI 0.58–0.73) and did not differ significantly from that of the dichotomous refill measure (difference = 0.08; χ2 = 2.71; p = 0.10) or from that of the continuous refill measure (difference = 0.03; χ2 = 0.38; p = 0.54) (Fig. 2).

Distribution of Autonomy Scores. Average autonomy of adolescents during the 24-month study follow-up period. Adolescents with an average autonomy of “1” always picked up their medications alone. Those with an average of “3” always had another person pick up the medicines for them. For the subgroup analyses described in the text, adolescents with higher averaged levels of autonomy were classified as “Group 1” and adolescents with lower averaged levels of autonomy as “Group 2”
The refill adherence and VF relationship was the weakest among adolescents with the lowest average levels of autonomy (“Group 2”) throughout the study period (AUC = 0.49; 95% CI 0.32–0.65). In comparison, adolescents with the highest average levels of autonomy (“Group 1”) had an AUC of 0.63 (95% CI 0.50–0.76). Thus, while the relationship of refill to viral load was weak in both groups, it was particularly unhelpful among those with little autonomy over picking up their own refills.
In contrast to the low AUC’s observed for the comparisons between refill adherence/virologic failure and immunologic failure/VF, the AUC for the comparison between adherence as measured by electronic monitors and VF was 0.91 (95% CI 0.86–0.96). The high AUC for the comparison between adherence as measured by electronic monitoring caps and VF demonstrates that non-adherence was responsible for most of the VF seen in these adolescents.
Discussion
These results demonstrate that both refill non-adherence and immunologic failure have low sensitivity and specificity for identifying VF in treatment-experienced adolescents. The two-comparator measures were similarly suboptimal for indicating VF in our cohort. Bisson et al. reported that pharmacy refill data reflected virologic treatment outcomes better than immunologic response to treatment and both measures were stronger in identifying VF in treatment-naïve adults than in our treatment-experienced adolescent cohort [16]. In a cohort of treatment-experienced South African adults, pharmacy refill data predicted virologic outcomes nearly as well as electronic monitoring [22]. Pharmacy refill measures have also been shown to be strongly associated with adults’ virologic treatment outcomes in Brazil [23]. In some populations, pharmacy refill measures have been found to be sensitive, but not specific for detecting antiretroviral therapy non-adherence [24,25,26,27]. However, in our adolescents, sensitivity of the pharmacy refill measure was also poor.
There are several possible reasons for the difference in the strength of pharmacy refill records to predict virologic treatment outcomes in adolescents compared with adults. Perinatally HIV-infected adolescents might be more likely than adults to share pills with others in the household due to increased rates of within-family disclosure of their HIV status [28]. Adolescents may have autonomy over taking their medications, but not over obtaining their own pharmacy refills. Discordance between responsibility over medication-taking and responsibility over obtaining refills may lead to increased misclassification of good refill adherence as indicative of good medication adherence. Pharmacy refill records may be more predictive of treatment failure in an adult population because adults typically maintain autonomy over every step of the medication-acquisition and medication-taking processes. In addition, adolescents may receive a “secondary gain” from coming to the clinic for refills, not because they want their medications but because they receive emotional support or comfort from the clinic staff. Finally, during late adolescence, the majority of adolescents have yet to transition from concrete to abstract thinking [29]. This may lead them to come to the clinic simply because they are scheduled for a refill, despite not having completed their medications.
Our results therefore may not be generalizable to clinics that do not provide patients with a scheduled refill date. It is common in public clinics in Africa for pharmacy refill visits to be scheduled, however [24]. Similarly, clinics with high staff turnover and/or particularly busy staff who have little time to engage with individual patients might have fewer adolescents who come for refills when they have not completed their medications. The strength of relationships with clinic staff (or the likelihood of being scolded for not obtaining refills on the prescribed date) likely impacts behavior. Although most adolescents had viral loads drawn as scheduled every 3 months, misclassification of treatment outcomes may also have occurred for adolescents who did not get their viral loads drawn as scheduled.
Despite these limitations, this study has several major strengths. First, the Botswana-Baylor Children’s Clinical Centre of Excellence is adjacent to the clinic where the Bisson, et al. study was conducted, serving similar catchment areas, and thus allowing for a more direct comparison between the adult and adolescent populations than would have been possible with two disparate settings. Frequent and consistent viral load monitoring was available throughout the 2-year follow-up. The strong association between MEMS data and viral load values demonstrated that most VF can be directly attributed to poor adherence in our cohort.
Conclusion
Since both pharmacy refill data and CD4 counts are poor identifiers of treatment failure for treatment-experienced adolescents, there is a strong need for alternative monitoring methods or increased access to viral load tests for this vulnerable group.
Abbreviations
- ART:
-
Anti-retroviral therapy
- AUC:
-
Area under the curve
- HIV:
-
Human immunodeficiency virus
- MEMS:
-
Medical event monitoring system
- ROC:
-
Receiver operating characteristic
- VF:
-
Virologic failure
References
WHO. Health for the World’s adolescents, A second chance in the second decade. 2017; http://apps.who.int/adolescent/second-decade/section3. Accessed 31 Aug 2017.
UNAIDS. Global report: UNAIDS report on the global AIDS epidemic 2013. Geneva2013.
Kasedde S, Luo C, McClure C, Chandan U. Reducing HIV and AIDS in adolescents: opportunities and challenges. Curr HIV/AIDS Rep. 2013;10(2):159–68.
Lowenthal ED, Bakeera-Kitaka S, Marukutira T, Chapman J, Goldrath K, Ferrand RA. Perinatally acquired HIV infection in adolescents from sub-Saharan Africa: a review of emerging challenges. Lancet Infect Dis. 2014;14(7):627–39.
Biglan A, Metzler CW, Wirt R, et al. Social and behavioral factors associated with high-risk sexual behavior among adolescents. J Behav Med. 1990;13(3):245–61.
Guiella G, Madise NJ. HIV/AIDS and sexual-risk behaviors among adolescents: factors influencing the use of condoms in Burkina Faso. Afr J Reprod Health. 2007;11(3):182–96.
Nachega JB, Hislop M, Nguyen H, et al. Antiretroviral therapy adherence, virologic and immunologic outcomes in adolescents compared with adults in southern Africa. J Acquir Immune Defic Syndr. 2009;51(1):65–71.
Gross R, Bilker WB, Friedman HM, Strom BL. Effect of adherence to newly initiated antiretroviral therapy on plasma viral load. AIDS. 2001;15(16):2109–17.
Rutstein SE, Golin CE, Wheeler SB, et al. On the front line of HIV virological monitoring: barriers and facilitators from a provider perspective in resource-limited settings. AIDS Care. 2016;28(1):1–10.
Rawizza HE, Chaplin B, Meloni ST, et al. Immunologic criteria are poor predictors of virologic outcome: implications for HIV treatment monitoring in resource-limited settings. Clin Infect Dis. 2011;53(12):1283–90.
Kantor R, Diero L, Delong A, et al. Misclassification of first-line antiretroviral treatment failure based on immunological monitoring of HIV infection in resource-limited settings. Clin Infect Dis. 2009;49(3):454–62.
Moore DM, Awor A, Downing R, et al. CD4 + T-cell count monitoring does not accurately identify HIV-infected adults with virologic failure receiving antiretroviral therapy. J Acquir Immune Defic Syndr. 2008;49(5):477–84.
van Oosterhout JJ, Brown L, Weigel R, et al. Diagnosis of antiretroviral therapy failure in Malawi: poor performance of clinical and immunological WHO criteria. Trop Med Int Health. 2009;14(8):856–61.
Davies MA, Boulle A, Eley B, et al. Accuracy of immunological criteria for identifying virological failure in children on antiretroviral therapy—the IeDEA Southern Africa Collaboration. Trop Med Int Health. 2011;16(11):1367–71.
Grossberg R, Gross R. Use of pharmacy refill data as a measure of antiretroviral adherence. Curr HIV/AIDS Rep. 2007;4(4):187–91.
Bisson GP, Gross R, Bellamy S, et al. Pharmacy refill adherence compared with CD4 count changes for monitoring HIV-infected adults on antiretroviral therapy. PLoS Med. 2008;5(5):e109.
Ministry of Health of Botswana. 2012 botswana national HIV & AIDS treatment guidelines. Gaborone: Government of Botswana; 2012.
Cramer JA. Microelectronic systems for monitoring and enhancing patient compliance with medication regimens. Drugs. 1995;49(3):321–7.
WHO. WHO case definitions of HIV for surveillance and revised clinical staging and immunologic classification of HIV-related disease in adults and children. 2007. http://www.who.int/hiv/pub/guidelines/HIVstaging150307.pdf. Accessed 10 June 2016.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
Stata Statistical Software. Release 14 [computer program]. College Station: StataCorp LP; 2015.
Orrell C, Cohen K, Leisegang R, Bangsberg DR, Wood R, Maartens G. Comparison of six methods to estimate adherence in an ART-naive cohort in a resource-poor setting: which best predicts virological and resistance outcomes? AIDS Res Ther. 2017;14(1):20.
Martin D, Luz PM, Lake JE, et al. Pharmacy refill data can be used to predict virologic failure for patients on antiretroviral therapy in Brazil. J Int AIDS Soc. 2017;20(1):1–5.
Henegar CE, Westreich D, Maskew M, et al. Comparison of pharmacy-based measures of adherence to antiretroviral therapy as predictors of virological failure. AIDS Behav. 2015;19(4):612–8.
Sangeda RZ, Mosha F, Prosperi M, et al. Pharmacy refill adherence outperforms self-reported methods in predicting HIV therapy outcome in resource-limited settings. BMC Public Health. 2014;14:1035.
Abah IO, Ojeh VB, Musa J, et al. Clinical utility of pharmacy-based adherence measurement in predicting virologic outcomes in an adult HIV-infected cohort in Jos, North Central Nigeria. J Int Assoc Provid AIDS Care. 2016;15(1):77–83.
Vinikoor MJ, Schuttner L, Moyo C, et al. Short communication: late refills during the first year of antiretroviral therapy predict mortality and program failure among HIV-infected adults in urban Zambia. AIDS Res Hum Retroviruses. 2014;30(1):74–7.
Galano E, Turato ER, Succi RC, et al. Costs and benefits of secrecy: the dilemma experienced by adolescents seropositive for HIV. AIDS Care. 2017;29(3):394–8.
Hosek SG, Harper GW, Domanico R. Predictors of medication adherence among HIV-infected youth. Psychol Health Med. 2005;10(2):166–79.
Acknowledgements
The study team would like to thank the adolescent study participants and the staff at the Botswana- Baylor Children’s Clinical Centre of Excellence. We would also like to thank Alexandra Montesinos for translating the abstract into Spanish. This work was presented in part by Leah Genn at the Children’s Hospital of Philadelphia Research Institute Summer Scholar Program (CRISSP) 2015 Poster Session.
Funding
The first author’s work on this project was funded through the Children’s Hospital of Philadelphia Research Institute Summer Scholar Program (1R25HD082842-01). Study funding to establish this cohort was obtained from a CDC PEPFAR Public Health Effectiveness grant to the senior author. This work was supported by NIH K23 MH095669 to the senior author. Dr. Gross received support from the Penn Center for AIDS Research (P30 AI 045008). The funders did not play a role in study design, analysis, or the decision to publish this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict interest
None of the authors have conflicts of interest related to this manuscript.
Ethical Approval
All procedures were in accordance with the ethical standards of the institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments and comparable ethical standards. The study was approved by the Botswana Health Research Development Committee and Institutional Review Boards at the University of Pennsylvania and Baylor College of Medicine. Written informed consent was obtained from a parent or guardian of each adolescent study participant and assent was obtained for each adolescent participant.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Genn, L., Chapman, J., Okatch, H. et al. Pharmacy Refill Data are Poor Predictors of Virologic Treatment Outcomes in Adolescents with HIV in Botswana. AIDS Behav 23, 2130–2137 (2019). https://doi.org/10.1007/s10461-018-2325-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-018-2325-9