
Abstract
Substance use disorders (SUDs) are thought to predict care discontinuity, though magnitude and substance-specific variance of effects are unclear. This report of analytic work undertaken with a multi-regional American cohort of 9153 care enrollees addresses these gaps. Care retention was computed from 24-month post-linkage clinic visit documentation, with SUD cases identified from patient-report screening instruments. Two generalized estimating equations tested binary and hierarchial SUD predictors of retention, and potential effect modification by patient age-group, sex, and care site. Findings demonstrate: (1) detrimental SUD effect, equivalent to a nine percentage-point decrease in retention, with independent effects of age-group and care site; (2) substance-specific effect of marijuana UD associated with lower retention; and (3) age-modification of each effect on care discontinuity, with SUDs serving as a risk factor among 18–29 year-olds and protective factor among 60+ year-olds. Collective findings document patient attributes as influences that place particular subgroups at-risk to discontinue care.
Resumen
Los trastornos de uso de sustancias (TUS) se cree que predicen la discontinuidad del cuidado, aunque la magnitud y la varianza de los efectos de sustancias específicos no son claros. Este informe de trabajo analítico realizado con una multi-regional americano cohorte de 9153 inscritos de cuidado aborda estos brechas. La retención en la atención se calculó utilizando la documentación de la visita clínica registrada 24 meses después de la conexión a la atención, con casos de TUS identificados a partir de las medidas de detección realizadas por los pacientes. Dos ecuaciones de estimacion generalizadas probaron predictores binarios y jeraquicos del efecto de trastornos de uso de sustancias en la retencion, y la modificación del efecto potencial por edad del paciente, sexo y ubicación del cuidado. El análisis demuestra: (1) TUS tuvieron un efecto perjudicial equivalente a una disminución del 9 por ciento en la retención, con efectos independientes de la edad y ubicación del cuidado; (2) El TUS de marihuana tuvo un efecto de la sustancia específico asociado con menor retención; y (3) La edad tuvo un efecto modificador en la discontinuidad del cuidado; TUS fueron un factor de riesgo para los jóvenes de 18 a 29 años y un factor de protección para los mayores de 60 años. Los resultados colectivos documentan los atributos del paciente que influyen en el riesgo de interrupción de la atención para subgrupos particulares.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Substance use disorders (SUDs), defined by recurrent use of alcohol, tobacco, or illicit drugs causing clinically and functionally significant impairment [1], pose challenges along the HIV Care Continuum [2]. In diagnosis and care linkage phases, SUDs diminish the effectiveness of universal test-and-treat approaches and hamper care continuity [3,4,5]. Whereas Gardner and colleagues’ [6] seminal HIV Care Continuum data suggested 19% of HIV+ Americans linked to care are not subsequently retained, a recent Center for Disease Control (CDC) estimate [7] places the figure at 71% and highlights this as a prime target for quality improvement. Multisite studies document inverse association of HIV+ Americans’ substance use and retention [8, 9]. Beyond its doubling of mortality rates for HIV+ Americans [9], unsuccessful care retention—reflected by lack of recurrent care visits at which virologic monitoring occurs—unduly burdens health system resources via “churn” processes where patients cycle in and out services [10]. If global health goals for antiretroviral medication access and viral suppression are to be attained in the U.S. [11, 12], impediments that SUDs appear to pose to HIV+ Americans’ care retention merit attention.
Care retention is variously conceptualized by the HIV community, mostly as post-linkage indices marked by patterns of care visit attendance in one or more 12-month periods. Mugavero and colleagues [13] note among relevant indices: visit constancy, reflecting semi-annual intervals during which a visit is attended; gaps in care, or 6-month intervals in which no visits occur; and visit adherence, computed as percentage of visits attended [e.g., attended visits/(attended visits + ‘no-shows’)]. A widely-recognized retention index is that formulated by the Health Resources and Services Administration HIV/AIDS Bureau (HRSA/HAB), since adopted by the Institute of Medicine as a core clinical indicator [14]. This HRSA/HAB index defines care retention as two attended visits, separated by at least 90 days, in a 12-month period. While other retention indices have been linked to clinical care milestones like initiation of antiretroviral medications or viral suppression, this HRSA/HAB retention index most robustly and reliably predicts these milestone achievements in initial years of HIV care [13, 15]. To what extent the presence of SUDs among HIV+ Americans may influence their retention, and if patient attributes—age, sex, or location of care received—that are robust predictors of the presence of SUDs in this population [16] may modify hypothesized SUD effects on retention, remain unanswered questions. Likewise, to what extent retention may vary among substance-specific SUD patient groups, and potential influence of these other patient attributes on variance in their HIV care retention, remains unsettled.
In the current work, the aforementioned patient attributes were examined as influences of HRSA/HAB-defined 2-year retention among a multisite Center for AIDS Research Network of Integrated Clinical Systems [CNICS; [17] ] cohort of HIV+ Americans linked to care. The primary patient attribute was SUDs, conceptualized in models as a: (1) bivariate predictor (any SUD, no SUD), or (2) categorical predictor, defined hierarchically to form substance-specific SUD subgroups that vary in antiretroviral medication initiation [18]. In each model, patient age, sex, and care site were explored as potential modifiers of the proposed SUD effects on retention. Enhanced understanding of patient attributes serving as risk factors for care discontinuance may inform health service dissemination to address unmet needs among HIV+ Americans.
Methods
Data Sources
This work utilized CNICS [19], a network initiated in 1995 for longitudinal observation of HIV+ adults linked to care at its affiliated sites. Continual integration of data from these sites afforded opportunity to address care retention absent sampling biases and surrogate endpoints of clinical trials [20]. Available CNICS data include care visit information documented by site staff, standardized HIV risk factor information obtained at enrollment, medication/laboratory information from electronic medical records, and patient-reported outcomes collected by personal computer or touch-screen tablet [19]. Approval of university-based institutional review boards (IRBs) for CNICS sites govern data collection, and the University of Washington IRB approved analyses of de-identified data provided to the principal investigator by the CNICS Data Management Core. Current work is restricted to data on patient demography, substance-focused patient-reporting on the Alcohol Use Disorders Identification Test-Version C [AUDIT-C [21]] and the Alcohol, Smoking, and Substance Involvement Test [ASSIST [22]], and care visit information for the 2-year period following each patient’s earliest recorded visit date.
Patient Attributes
Focal attributes explored as potential effect modifiers for expected SUD influences on care retention were those previously found to be robust predictors of care retention [15, 23] and SUD prevalence [16] in CNICS cohorts. These attributes were patients’: (1) care site (affiliated universities later noted), (2) age-group (18–29, 30–39, 40–49, 50–59, 60+ year-olds), and (3) sex (female, male). Other demographic characteristics that furthered initial sample description were race (non-hispanic white, non-hispanic black, hispanic, other), gender (cis, trans) and male patients’ history of sex with male partners (yes, no).
SUD Identification
Governed by a ‘past 12 months’ reporting interval, the AUDIT-C is well-established as a screening instrument with strong sensitivity and specificity for diagnoses of alcohol use disorder [21], hereafter referred to as alcohol UD. In the current work, AUDIT-C summary scores were compared against this diagnostic threshold to identify cases of alcohol UD. Regarding other substances, CNICS assessment abbreviates ASSIST measurement to cocaine, marijuana, methamphetamine, and non-prescription opioids. Governed by a ‘past 3 months’ reporting interval and resulting in substance-specific ‘involvement scores,’ the ASSIST is also well-established as a screening instrument for SUD diagnoses [22] with its involvement scores demonstrating strong diagnostic sensitivity and specificity for cocaine use disorder, marijuana use disorder, methamphetamine use disorder, and opioid use disorder (hereafter referred to as cocaine UD, marijuana UD, methamphetamine UD, and opioid UD). Substance-specific ASSIST involvement scores were compared against these diagnostic thresholds to identify cases of cocaine UD, marijuana UD, methamphetamine UD, and opioid UD. Cases for which neither AUDIT-C nor ASSIST diagnostic thresholds were reached comprised a no SUD group.
2-Year Care Retention
The dependent variable was a binary HRSA/HAB index (0 = not retained, 1 = retained), computed from clinic documentation for the 2-year period that followed patients’ initial visit date. For descriptive purposes, additional indices outlined by Mugavero and colleagues [13] were similarly calculated from this 24-month visit documentation. These were: 1) visit-constancy, or number of 4-month intervals wherein a scheduled visit was attended (range of 0–6), 2) care gaps, or number of 6-month periods without an attended visit (range of 0–4), 3) number of attended visits (range of 0–67), 4) number of ‘no-shows’, or visits scheduled but not kept by the patient (range of 0–36), and 5) visit adherence, or rate at which scheduled visits were attended [attended visits/(attended visits + ‘no-shows’), range .01–1.00].
Participants
The sample (N = 9153) were HIV+ adults linked to care at seven sites, who voluntarily completed a patient-report assessment between 01/01/2007 and 12/31/2014 and for whom available visit data encompassed the 1st 2 years of care. Sites were located at Harvard University, Johns Hopkins University, University of Alabama-Birmingham, University of California-San Diego, University of California-San Francisco, University of North Carolina-Chapel Hill, and the University of Washington. Demography was reported upon enrollment, and the patient-report assessment was completed prior to a routine clinic visit. Per CNICS policy, otherwise willing patients deemed medically unstable, appearing intoxicated, evidencing significant cognitive impairment, or unable to speak English or Spanish did not complete patient-report assessments.
Analytic Strategy
Generalized estimating equations (GEEs) tested two population-average models [24] that each described variance in HRSA/HAB-defined 2-year retention attributable to a hypothesized predictor (SUD) while accounting for nonindependent observations at CNICS sites. To examine a binary logistic outcome, the 1st model included a binary predictor (any SUD, no SUD) with dummy-coded care site (#1–7), categorical age-group (18–29, 30–39, 40–49, 50–59, 60+ year-olds), and binary sex (male, female) indices as potential effect modifiers and robust covariance structure due to the aggregate sample size. The 2nd model retained the noted specifications, but reconceptualized SUD as a six-level hierarchial index—informed by Tegger’s [18] identification of opioid UD, methamphetamine UD, and alcohol UD as specific SUDs that impede initiation of antiretroviral medications and by mixed evidence regarding marijuana use in HIV care [25,26,27,28,29]. Thus, the hierarchial SUD index was defined as: (1) opiod UD with or without other SUDs, (2) methamphetamine UD with or without other SUDs, (3) alcohol UD with or without other SUDs, 94) cocaine UD with or without other SUDs, (5) marijuana UD only, and (6) no SUD. For the SUD effect identified in each model, supplemental post hoc examination focused on corresponding annual patterns of retention during the 2-year care period (i.e., initial year, subsequent year). For further descriptive purposes, other aforementioned care retention indices outlined by Mugavero and colleagues [13] were computed and presented from available 24-month clinic visit documentation for each of the six groups defined in the hierarchial SUD index.
Results
In the aggregate sample of 9153 CNICS patients, age ranged from 19 to 84 years [mean (M) = 44.1, standard deviation (S.D.) = 10.4)]. Distribution of race was 51% non-Hispanic White, 33% non-Hispanic Black, 12% Hispanic, and 4% ‘Other.’ The sample was 84% male, among whom 79% had a history of sex with male partners. Transgender status was affirmed for less than 1% of the sample. Table 1 lists 2-year HRSA-HAB-defined care retention by patient demography, and at de-identified CNICS care sites (per IRB stipulations at one or more sites).
Influence of SUD on 2-Year HRSA/HAB-Defined Care Retention
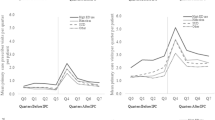
Table 2 lists full reporting of model statistics, as GEE identified SUD, age-group, and care site as predictors of retention. Retention was lower in SUD (67%) than non-SUD patients (76%). As earlier noted in Table 1, retention in 18–29 year-olds was quite low and progressively higher in older age-groups, and between-site variance in retention was extensive. As for SUD effect modifiers, only the SUD × age-group interaction was significant (see Table 2). Retention was lower in SUD than non-SUD patients among 18–29 year-olds (56 vs. 67%), 30–39 year-olds (64 vs. 71%), 40–49 year-olds (70 vs. 73%), and 50-59 year-olds (73 vs. 79%), whereas this pattern reversed in 60+ year-olds (86 vs. 78%). Post-hoc temporal exploration of retention rates underlying the SUD effect revealed a modest initial-year gap (SUD = 89%, non-SUD = 92%) that subsequently doubled among remaining patients (SUD = 76%, non-SUD = 83%).
Influence of Substance-Specific SUDs on 2-Year HRSA/HAB-Defined Care Retention
Table 3 lists full reporting of model statistics, as in addition to age-group and care site GEE identified marijuana UD as a substance-specific predictor of retention. Retention varied minimally among the five substance-specific SUD groups (67–70%), and was lower in all than in the no SUD group (76%). As for marijuana UD effect modifiers, only its interaction with age-group was significant (see Table 3). Relative to overall retention of 67% marijuana UD patients, the rate was lowest in 18–29 year-olds (52%) and progressively higher in the older age-groups (30–39 year-olds, 63%; 40–49 year-olds, 69%, 50–59 year-olds, 71%; 60+ year-olds, 85%). Post-hoc temporal exploration of retention rates for the marijuana UD effect revealed in the initial year retention was slightly lower in the marijuana UD group (87%) than other substance-specific SUD groups (88–90%) and no SUD group (92%). Among remaining patients in the subsequent year, retention was again slightly lower in the marijuana UD group (69%) than other substance-specific SUD groups (70–72%) and the no SUD group (76%).
Additional 2-Year Care Retention Indices by Substance-Specific SUDs
Table 4 lists descriptive statistics, by substance-specific SUD group, for other retention indices noted by Mugavero and colleagues [13]. For visit-constancy, the cohort’s mean number of 4-month intervals with an attended visit was 4.56 (SD = 1.60), with more such intervals for no SUD patients (4.68) than each substance-specific SUD subgroup (range 4.05–4.43). For care gaps, the cohort’s mean of 6-month intervals without an attended visit was .61 (SD = .68), with fewer gaps for no SUD patients (.58) than all substance-specific SUD subgroups (range: .62–.68). Respective mean frequencies for attended visits and ‘no-shows’ were 11.06 (SD = 6.72) and 1.76 (SD = 2.64), eventuating in mean visit adherence rate of 86% for the cohort. Consistent with the pattern of these two other retention indices, the visit adherence rate was higher among no SUD patients (88%) than all other substance-specific SUD subgroups (range of 80–86%).
Discussion
Utilizing a large, multiregional CNICS cohort to examine influence of SUDs on 2-year care retention at seven HIV care sites, the current work advances understanding of the HIV-SUD syndemic specific to post-linkage care continuity of HIV+ individuals. Findings include: (1) a detrimental influence of SUD on HRSA/HAB-defined care retention; (2) independent effects of patient age-group and care site on this outcome, evidencing both progressively higher retention rates for older patient age-groups as well as geographic variance in retention; (3) modification of the SUD effect on retention by patient age-group, with SUD serving as a risk factor for care discontinuance among young adults (aged 18–29) and as a protective factor for retention among older patients (aged 60+); and (4) a substance-specific effect of marijuana UD associated with lower retention, similarly modified by patient age-group such that young adult marijuana UD patients evidenced a particularly low retention rate. Collective findings document these patient attributes as influences that place particular patient subgroups at-risk for care discontinuity.
The 71% 2-year retention rate observed in this multiregional cohort is an encouraging figure, given a much lower rate reported in the aforementioned CDC report [7]. This suggests, perhaps unsurprisingly, that a high quality of care is provided at CNICS-affiliate sites that other HIV care settings in the community struggle to replicate. Given elevated care retention rates in these well-resourced CNICS clinical environments, it may be unsurprising that a hypothesized risk factor like SUD was associated with no more than a nine percentage-point decrease in HRSA/HAB-defined retention and that patient gender—previously linked to differential HIV care retention [8]—failed to emerge as a predictor in any of the analyses of this CNICS cohort. Nevertheless, current findings are broadly consistent with multisite reports of substance misuse as a frequent precursor of care discontinuity [8, 9]. Notably, the lone demographic modifier of this SUD effect was patient age-group, such that the presence of an SUD placed young adult patients at-risk to discontinue care yet was associated with higher care retention rates among 60+ year-old patients. Taken together, current findings underscore the importance of identifying SUDs among HIV care patients and monitoring of patient substance use, particularly among young adults, as critical tasks for the workforce that provides services in HIV care settings.
Modest variability in retention rates among the hierarchically-defined substance-specific SUD groupings was somewhat surprising, given Tegger and colleagues’ [18] reporting of the differential prediction of a related HIV care outcome (i.e., antiretroviral medication initiation) by opiate, amphetamine, alcohol, and cocaine groups. Notably, marijuana UD—the lone substance-specific SUD to emerge as a predictor of care discontinuity in the current CNICS cohort—was omitted in this prior work of Tegger et al. [18]. These discrepant sets of findings underscore an importance of comprehensive, substance-specific SUD measurement when examining influences on HIV care processes. Further, the collective findings point to a varied topography of HIV care adherence wherein substance-specific SUDS may uniquely influence indices of care adherence that encompass attendance of clinic visits, access and adherence to antiretroviral medications, and other relevant clinical targets. While a comparatively large marijuana UD subsample in this CNICS cohort [16] may contribute to findings reported herein, it nevertheless suggests HIV care patients whose use of marijuana results in clinically and functionally significant impairments are specifically at elevated risk for care discontinuity in the initial years following treatment linkage.
In the current findings, age-related influences were salient. This is evident both in direct influences of patient age-group on care retention, and in the modification of SUD effects on care retention by patient age-group. Young adulthood, defined in the current work as 18–29 years of age, was reliably linked in current analyses to the poorest rates of care continuity and magnified the detrimental influence of SUDs on this clinical care index. Notably, young adulthood and substance misuse have been previously identified among a constellation of risk factors for poor HIV care retention [9, 30,31,32]. Clearly, there is need to more effectively engage substance-using young adults in care, as their elevated transmission risks may be exacerbated when disengaged from the health system. A surprising age-related finding—that SUDs were associated with greater continuity of care among 60+ year-olds—also has public health implications. As public access to effective antiretroviral therapy has increased, the HIV care population has matured. Accordingly, it is increasingly important for the HIV workforce to monitor among its elder patients medical marijuana authorizations and other potentially problematic prescriptions (i.e., opioids) to identify and intervene around possible substance misuse. Influence of care site was far less robust as an independent predictor of retention and did not modify SUD effects, but this findings does suggest some variance in care continuity even among these seven CNICS sites.
Strengths and caveats of the work bear mention. Strengths include a multiregional cohort of HIV care enrollees; use of established SUD screening instruments with validated diagnostic thresholds; and 24-month clinic documentation from which to compute an empirically-supported HRSA-HAB index and other care retention variables. An earlier-noted caveat is CNICS setting representativeness, and suggests replication of these findings in other community care settings is warranted. Potential selection bias at a patient-level is also acknowledged, as the cohort included 29% of 32,727 CNICS enrollees to date [17]. It is conceivable that the willingness of this cohort to voluntarily complete a patient-reported outcome assessment prior to a routine clinic visit may in some manner distinguish them from other patients. Unfortunately, the CNICS data access agreement limits the local investigative team to analysis of only this cohort, and thus broader comparisons of its demography, background, or treatment participation vs. that of other CNICS enrollees were not possible. Another study caveat concerns SUD measurement, as the CNICS patient-reported outcome battery includes an abbreviated version of the ASSIST that omits some licit (i.e., tobacco) and illicit (i.e., sedatives/tranquilizers, solvents/inhalants, hallucinogens, club drugs) substance categories that are otherwise included in current national and international diagnostic systems. Further, we recognize potential influence of unassessed 3rd-variables—such as mental illness, trauma/victimization, employment, income, or education—that have been shown in prior research to influence the course and outcome of HIV infection [33,34,35].
Conclusions
Caveats notwithstanding, findings advance understanding of the scope of the American SUD-HIV syndemic as relates to post-linkage care continuity. Even at model HIV care facilities where high rate of 2-year care retention was observed, SUD was a risk factor for discontinuity in the initial years following care linkage. Among substance-specific SUDs, relative risk is greatest among patients with marijuana UD, with broader SUD and specific marijuana UD effects both age-modified with risk concentrated among young adults. Effective clinical efforts to counteract such risks may occur by increasing capacity for addiction-focused services in HIV care settings. In addition to established pharmacotherapies for particular substances of abuse (i.e., acamprosate, disulfirambuprenorphine, methadone, extended release naltrexone), a shortlist of behavior therapies (i.e., cognitive-behavioral therapy, contingency management, motivation interviewing) are documented in multiple randomized controlled trials to increase HIV care adherence among SUD patients [36,37,38,39,40,41]. Each is firmly established in the addictions field, with broad application recommended for its use across adult patient groups and substances of abuse [42]. Expanded therapy application in HIV settings to promote greater care continuity among SUD patients appears entirely appropriate. Case management is an additional form of health service intervention, one for which ubiquity and demonstrated efficacy to improve SUD patient retention in addiction care and linkage to other services [43] may facilitate compliance with HIV treatment tasks (i.e., consistent clinic attendance, antiretroviral medication adherence, use of strategies to reduce transmission risk) that promote care continuity. Current study findings suggest that, even in well-resourced HIV care settings, there remains room to improve care continuity—particularly among young adults with an SUD. This may occur via implementation of empirically-supported behavior therapies, case management, or a blending of the two.
References
APA. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013.
Hall HI, Holtgrave DR, Tang T, Rhodes P. HIV transmission in the United States: considerations of viral load, risk behavior, and health disparities. AIDS Behav. 2013;17:1632–6.
Dieffenbach WW, Fauci AS. Universal voluntary testing and treatment for prevention of HIV transmission. JAMA. 2009;301:2380–2.
Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet. 2009;373:48–57.
Giordano TP, Visnegarwala F, White ACJ, Troisi CL, Frankowski RF, Hartman CM, et al. Patients referred to an urban HIV clinic frequently fail to establish care: factors predicting failure. AIDS Care. 2005;17(6):773–83.
Gardner EM, McLees MP, Steiner JF, del Rio C, Burman WJ. The spectrum of engagement in HIV care and its relevance to test-and-treat strategies for prevention of HIV infection. Clin Infect Dis. 2011;52(6):793–800.
Centers for Disease Control and Prevention. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 dependent areas, 2014 2016. http://www.cdc.gov/hiv/library/reports/surveillance.
Hall HI, Gray KM, Tang T, Li J, Shouse L, Mermin J. Retention in care of adults and adolescents living with HIV in 13 U.S. areas. J Acquir Immune Def Syndr. 2012;60:77–82.
Mugavero MJ, Lin HY, Willig JH, Westfall AO, Ulett KB, Routman JS, et al. Missed visits and mortality among patients establishing initial outpatient HIV treatment. Clin Infect Dis. 2009;48:248–56.
Rebeiro P, Althoff KN, Buchacz K, Gill J, Horberg M, Krentz H, et al. Retention among North American HIV-infected persons in clinical care, 2000-20008. J Acquir Immune Def Syndr. 2013;62(3):356–62.
UNAIDS. 90-90-90: An ambitious treatment target to help end the AIDS epidemic. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS, 2014 October. Report No.: Contract No.: UNAIDS/JC2684.
Office of National AIDS Policy. The National HIV/AIDS Strategy: Updated to 2020 2015. https://www.aids.gov/federal-resources/national-hiv-iad-strategy/nhas-update.pdf.
Mugavero MJ, Westfall AO, Zinski A, Davila J, Drainoni ML, Gardner LI, et al. Measuring retention in HIV care: the elusive gold standard. JAIDS. 2012;61(5):574–80.
IOM. Monitoring HIV care in the United States: indicators and data systems. Washington, D.C.; 2012.
Dombrowski JC, Kitahata MM, Von Rompaey SE, Crane HM, Mugavero MJ, Eron JJ Jr, et al. High levels of antiretroviral use and viral suppression among persons in HIV care in the United States, 2010. JAIDS. 2013;63(3):299–306.
Hartzler B, Dombrowski JC, Crane HM, Eron JJ Jr, Geng EH, Mathews WC, et al. Prevalence and predictors of substance use disorders among HIV care enrollees in the United States. AIDS Behav. 2017;21(4):1138–48.
CNICS. CFAR Network of Integrated Clinical Systems: University of Alabama-Birmingham; 2017. www.uab.edu/cnics. Accessed 3 May 2017.
Tegger MK, Crane HM, Tapia KA, Uldall KK, Holte SE, Kitahata MM. The effect of mental illness, substance use, and treatment for depression on the initiation of highly active antiretroviral therapy among HIV-infected individuals. AIDS Patient Care STDs. 2008;22(3):233–43.
Kitahata MM, Rodriquez B, Haubrick R, Boswell S, Mathews WC, Lederman MM, et al. Cohort profile: the centers for AIDS research network of integrated clinical systems. Int J Epidemiol. 2008;37:948–55.
Hughes MD. Initial treatment of HIV infection: randomized trials with clinical endpoints are still needed. J Infect Dis. 2006;194:542–4.
Dawson DA, Smith SM, Saha TD, Rubinsky AD, Grant BF. Comparative performance of the AUDIT-C in screening for DSM-IV and DSM-5 alcohol use disorders. Drug Alcohol Depend. 2012;126:384–8.
Humeniuk R, Ali R, Babor TF, Farrell M, Formigoni ML, Jittiwuikarn J, et al. Validation of the alcohol, smoking, and substance involvement screening test (ASSIST). Addiction. 2008;103(6):1039–47.
Mugavero MJ, Amico KR, Westfall AO, Crane HM, Zinski A, Willig JH, et al. Early retention in HIV care and viral load suppression: implications for a test and treat approach to HIV prevention. J Acquir Immune Def Syndr. 2012;59(1):86–93.
Hubbard AE, Ahern J, Fleischer NL, Van der Laan M, Lippman SA, Jewell N, et al. To GEE or not to GEE: comparing population average and mixed models for estimating the associations between neighborhood risk factors and health. Epidemiology. 2010;21:467–74.
de Jong BC, Prentiss D, McFarland W, Machekano R, Israelski DM. Marijuana use and its association with adherence to antiretroviral therapy among HIV-infected persons with moderate to severe nausea. JAIDS. 2005;38(1):43–6.
Fogarty A, Rowstorne P, Prestage G, Crawford J, Grierson J, Kippax S. Marijuana as therapy for people living with HIV/AIDS: social and health aspects. AIDS Care. 2007;19:295–307.
Lutge EE, Gray A, Siegfried N. The medical use of cannabis for reducing morbidity and mortality in patients with HIV/AIDS Cochrane Database Systematic Review. 2013;4(CD00517):5.
Bonn-Miller MO, Oser ML, Bucossi MM, Trafton JA. Cannabis use and HIV antiretroviral therapy adherence and HIV-related symptoms. J Behav Med. 2014;37:1–10.
Abrams DI, Jay CA, Shade SB, Vizoso H, Reda H, Press S, et al. Cannabis in painful HIV-associated sensory neuropathy: a randomized placebo-controlled trial. Neurology. 2007;68:515–21.
Mugavero MJ, Lin HY, Allison JJ, Willig JH, Chang PW, Marler M, et al. Failure to establish HIV care: characterizing the ‘no show’ phenomenon. Clin Infect Dis. 2007;45(1):127–30.
Catz SL, McClure JB, Jones GN, Brantley PJ. Predictors of outpatient medical appointment attendance among persons with HIV. AIDS Care. 1999;11:361–73.
Israelski D, Gore-Felton C, Power R, Wood MJ, Koopman C. Sociodemographic characteristics associated with medical appointment adherence among HIV-seropositive patients seeking treatment in a county outpatient facility. Prev Med. 2001;33:470–5.
Oldenburg CE, Perez-Brumer AG, Reisner SL. Poverty matters: contextualizing the syndemic condition of psychological factors and newly diagnosed HIV infection in the United States. AIDS. 2014;28(18):2763–9.
Pence BW, Miller WC, Gaynes BN, Eron JJ Jr. Psychiatric illness and virologic response in patients initiating highly active antiretroviral therapy. J Acquir Immune Def Syndr. 2007;44(2):159–66.
Kalichman SC, Sikkema KJ, DiFonzo K, Luke W, Austin J. Emotional adjustment in survivors of sexual assault living with HIV-AIDS. J Trauma Stress. 2002;15(4):286–96.
Parsons JT, Rosof E, Punzalan JC, Di Maria L. Integration of Motivational Interviewing and Cognitive Behavioral Therapy to Improve HIV medication adherence and reduce substance use among HIV-positive men and women: results of a pilot project. AIDS Patient Care STDs. 2005;19(1):31–9.
Safren SA, O’Cleirigh CM, Bullis JR, Otto MW, Stein MD, Pollack MH. Cognitive behavioral therapy for adherence and depression (CBT-AD) in HIV-infected injection drug users: a randomized controlled trial. J Consult Clin Psychol. 2012;80(3):404–15.
Petry NM, Weinstock J, Alessi SM, Lewis MW, Dieckhaus K. Group-based randomized trial of contingencies for health and abstinence in HIV patients. J Consult Clin Psychol. 2010;78(1):89–97.
Rosen MI, Dieckhaus K, McMahon TJ, Valdes B, Petry N, Cramer JA, et al. Improved adherence with contingency management. AIDS Patient Care STDs. 2007;21(1):30–40.
Diiorio C, McCarty F, Resnicow K, McDonnell-Holstad M, Soet J, Yeager K, et al. Using motivational interviewing to promote adherence to antiretroviral medications: a randomized controlled study. AIDS Care. 2008;20(3):273–83.
Golin CE, Earp J, Tien HC, Stewart P, Porter C, Howie L. A 2-arm, randomized, controlled trial of a motivational interviewing-based intervention to improve adherence to antiretroviral therapy (ART) among patients failing or initiating ART. J Acquir Immune Defic Syndr. 2006;42(1):42–51.
NIDA. Principles of drug addiction treatment: a research-based guide (3rd ed.). Services USDoHaH, editor2012.
Rapp RC, Van Den Noortgate W, Broekaert E, Vanderplasschen W. The efficacy of case management with persons who have substance abuse problems: a three-level met-analysis of outcomes. J Consult Clin Psychol. 2014;82(4):605–18.
Acknowledgements
The funding source for this analytic work was National Institute on Drug Abuse R03DA039719 (Informing Dissemination of Behavior Therapies to Enhance HIV Care Among Substance Abusers, Hartzler PI). The authors thank the CNICS sites for contributing data to this endeavor. CNICS is funded by R24 AI067039 with sites at University of Alabama at Birmingham, University of Washington, University of California San Diego, University of California San Francisco, Case Western Reserve University, John Hopkins University, Fenway Health/Harvard, and University of North Carolina Chapel Hill.
Disclaimer
The content of this report is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Julia C. Dombrowski has conducted STD clinical research unrelated to this work supported by grants to the University of Washington from Genentech, ELITech, Melinta Therapeutics, Curatek Pharmaceuticals, Quidel, and Hologic. Among the authorship group, no other conflicts of interest were declared.
Ethical Approval
All procedures involving human participants were in accordance with institutional review boards at the CNICS-affiliate universities, and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individuals during their initial enrollment in CNICS.
Rights and permissions
About this article

Cite this article
Hartzler, B., Dombrowski, J.C., Williams, J.R. et al. Influence of Substance Use Disorders on 2-Year HIV Care Retention in the United States. AIDS Behav 22, 742–751 (2018). https://doi.org/10.1007/s10461-017-1826-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-017-1826-2