
Abstract
People living with HIV (PLHIV) have higher rates of suicidal behavior than the general population. This study assessed suicidal behavior (ideation and/or attempts, ever and in the past 12 months) among PLHIV receiving outpatient HIV medical care in Estonia and associations between suicidal behavior and psychological treatment. The cross-sectional study collected data from January to November 2013 using a self-report questionnaire. Eight hundred PLHIV participated, 39 % (n = 306) of whom had been suicidal. Lifetime prevalence was 36 % for suicidal ideation and 20 % for attempts. Younger age, incarceration, having ever abused alcohol and also injected drugs, having lived with HIV for more than 10 years, and being depressed were associated with lifetime suicidal behavior. Suicidal behavior within the past 12 months was reported by 20 % (n = 156) of respondents. Of these, 27 % received psychological treatment (counseling and/or psychotherapy), 20 % had taken antidepressants, and 49 % sedatives. Individuals perceiving a need for treatment were significantly more likely to receive psychological treatment when experiencing suicidal behavior (OR 25.65, 95 % CI 2.92–225.47). In conclusion, suicidal behavior is frequent among PLHIV but psychological treatment is not often received. One of the barriers to treatment is patients’ lack of perceived need for help.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Every year, more than 800,000 people die by committing suicide globally [1]. Suicide rates among people living with HIV (PLHIV) seem to be higher than those observed in the general population. For example, in the early 2000s, the mortality ratio for suicide in Spain was 9.6 times higher among PLHIV than in the general population [2]. In the last decade, suicide was recorded as the cause of death for 4 % of a Cologne–Bonn HIV cohort, 6.3 % of the Swiss HIV cohort, and 3.4 % in San Francisco [3–5].
Not everyone with suicidal behavior, defined as ideation, planning of, and/or attempted suicide, goes on to complete suicide. An epidemiological study of suicidal behavior among general populations in 17 countries found the lifetime prevalence of suicidal ideation to be 9.2 %, planning a suicide 3.1 %, and non-lethal attempts 2.7 % but figures varied widely by country [6]. In Estonia in 2014, lifetime prevalence was 16.1 % for suicidal ideation and 4.0 % for attempts [7]. A 17-country study among the general populations demonstrated that 29.0 % of ideators ever go on to make an attempt [6]. Further, data from the 1973–2003 cohort from Sweden found that 11.8 % of non-lethal suicide attempts are followed by a lethal one, depending on the type of attempt [8]. The situation seems to be graver among PLHIV. According to a systematic review, 26.9 % of PLHIV have reported suicidal ideation, 22.2 % have had a suicide plan, and 20.0 % have deliberately harmed themselves (the majority of studies focused on men and westerners who do not inject drugs) [9]. Between 1996 and 2008 in Switzerland, 35.1 % of lethal suicides occurred among PLHIV with a history of a previous suicide attempt [10]. However, there is no consensus on whether suicidal behavior is more frequent among PLHIV than in the general population because of considerable heterogeneity between methods used which limit direct comparisons. A study from the Netherlands in the late 2000s found that a larger proportion of HIV infected people reported suicidal ideation than people who were not HIV infected, but there was no difference between the groups in the rates of attempted suicides [11].
Personality and individual differences, cognitive factors, social aspects, and negative life events are key contributors to suicidal behavior; the single most significant risk factor for death by suicide is a previous suicide attempt [12]. Overall, the risk for nonfatal suicidal behavior is higher among young people, women, the unmarried, and socially disadvantaged people (i.e., those with low income and education, or unemployed) [12]. Similar risk factors have emerged among PLHIV: female gender, being young or middle-aged, unemployment, anxiety, depression, and abuse/addiction to psychoactive substances as was found in a recent study in Brazil [13]. Studies carried out in Switzerland and Denmark showed that PLHIV who die by suicide are more likely to have received inpatient treatment for AIDS, to have had their HIV diagnosis for less than two years, and/or have a history of a psychiatric disorder that commonly developed after being diagnosed with HIV [10, 14]. HIV infection does not appear to provide an additional contribution to increasing suicidal behavior among key populations at risk for HIV, including men who have sex with men (MSM) and people who inject drugs (PWID). A study among PWID in China between 2006 and 2010 found that being infected with HIV does not seem to contribute to thinking more about suicide (37.1 % of HIV+ PWID vs. 43.2 % HIV− PWID) but drug use itself does (43.2 % HIV− PWID vs. 8.5 % HIV− non-PWID) [15]. In Australia, HIV-positive MSM were no more likely than other gay or bisexual men to report feeling suicidal yet sexual identity as MSM itself was associated with elevated suicidal behavior compared with heterosexual men [16].
The management of people at risk of suicide is challenging because of the diverse causes of suicidal behavior and lack of evidence of efficacy for interventions aimed at reducing it [12, 17]. A systematic review concluded that improving recognition of depression by general practitioners, limiting access to lethal means, offering psychopharmacological treatment (e.g. selective serotonin reuptake inhibitors, high-potency anxiolytics), and cognitive behavioral therapy seem to be the best practices for suicide prevention by healthcare professionals [18]. Suicidal behavior has been associated with psychiatric disorders (e.g. depression) but proneness to certain mental processes (e.g. hopelessness, burdensomeness, agitation, rumination) are of greater importance in predicting suicidal behavior than being diagnosed with a psychiatric disorder [12, 17]. Synthesis of the research literature has underlined the need for effective interventions that specifically address suicidal thinking (e.g. hopelessness), and that the therapy for depression alone is not sufficient [19]. Most evidence-based psychotherapy interventions for prevention of suicide can be considered broadly as treatment designed to influence dysfunctional cognitions, emotions, and behaviors through a goal-oriented, systematic procedure in order to teach the patient that death is not the only option [20]. Psychopharmacological therapy is recommended for specific psychiatric disorders which have been identified [20].
A study from 21 countries among general populations found that only 34.8 % of people who had engaged in any sort of suicidal behavior in the past year had some form of contact with healthcare, and the low perception of need for help was consistently the most common barrier reported (57.8 % of respondents with any suicidal outcome did not perceive that psychological help was needed) [21]. Therefore healthcare professionals need to notice suicidal behavior and offer the best possible treatment to their patients. There is scarce information about barriers to treatment and interventions aimed at PLHIV with suicidal behavior [9].
Although the spread of HIV is stabilizing and declining globally, the epidemic in certain parts of Europe continues to grow at an alarming and accelerating pace [22]. An estimated 1.1 million people in Eastern Europe and Central Asia are infected with HIV [23]. There is limited information about suicidal behavior among PLHIV from the region and none from Estonia. The aim of this study was (i) to describe the prevalence and factors associated with suicidal behavior among PLHIV receiving medical care in Estonia, and (ii) to describe the uptake of mental health care (psychological and psychopharmacological treatment) among PLHIV experiencing suicidal behavior in the previous 12 months and factors associated with receiving psychological treatment.
Methods
Participants and Study Design
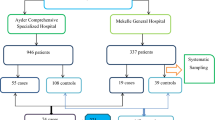
This was a cross-sectional study in three infectious disease outpatient clinics that provide 90 % of HIV outpatient care in Estonia [24]. We used convenience sampling in which participants were recruited by their infectious disease physician during their regular visits to the clinic. Patients were eligible for participation if they were HIV-infected, at least 18 years of age, spoke Estonian or Russian, had been aware of their HIV status for at least 3 months, were not pregnant, and were not under the influence of drugs or alcohol. A physician obtained informed consent and a nurse provided instructions for the questionnaire that was completed by the participant in a separate room and then placed in a sealed envelope. Respondents received a €10 supermarket voucher for study participation. Data collection took place between January 2013 and November 2013.
Measures
The questionnaire elicited information on participants’ socio-demographic characteristics (gender, age, ethnicity, incarceration, education, employment), sexual and substance use behavior, health information (including mental health care received) and date of first positive HIV test result.
Suicidality
Suicidal ideation was measured with a single item: “Have you ever thought about suicide?”, as was suicide attempt: “Have you ever tried to take your life?”, with response options of “in the last 12 months”, “more than a year ago”, and “no”. The term “suicidal behavior” includes both suicidal ideation and/or suicide attempts and is commonly used in suicide research [12].
Depression
The Emotional State Questionnaire (EST-Q2) is a screening instrument for mental health validated for use in Estonia [25]. EST-Q2 is recommended for screening for depression in primary care in Estonia and is widely used [26]. Its depression scale does not include questions about anxiety, fatigue or insomnia, which have a subscale of their own. When studying PLHIV it is advised to measure nonspecific symptoms of depression such as fatigue separately when screening for depression as the medical sequelae of HIV infection, associated opportunistic infections, and side effects of antiretroviral therapy can mimic them and overestimate the actual prevalence of depression [27, 28]. Using EST-Q2, patients were asked about the extent to which various problems had troubled them in the previous 4 weeks using a five-level scale with response options, “not at all = 0” to “all of the time = 4”. The maximum possible score for depression was 32. For maximum specificity and lowest false positive rate a cut-off point of ≥12 was used [29]. The instrument showed high internal consistency in both languages (in Estonian Cronbach’s α = 0.93, in Russian Cronbach’s α = 0.92).
Substance Abuse
Injection drug use (IDU) was determined from self-reported history of having injected drugs during the patient’s lifetime. The CAGE questionnaire was used for problematic alcohol use with a score of ≥2 taken to indicate alcohol abuse [30, 31]. This instrument showed high internal consistency in both languages (in Estonian Cronbach’s α = 0.80, in Russian Cronbach’s α = 0.77).
Mental Health Care
Patients were asked whether they had felt the need for psychological counseling and/or psychotherapy within the past 12 months and whether they had used these services within the past 12 months. As no definition was provided for the terms “psychotherapy” and “counseling”, answers for the two were combined into “psychological treatment” to limit bias due to confusion of the two by the participants. Mentioning of at least one (psychotherapy or counseling) categorized the participant as having received or needed psychological treatment. Psychopharmacological treatment was measured by patient self-report of antidepressant and/or sedative use within the past 12 months. The term “mental health care” as used in this study includes psychological as well as psychopharmacological treatment.
Statistical Analysis
Descriptive statistics were used to characterize the study sample. Pearson’s Chi squared test was used to compare the suicidal and non-suicidal groups for demographic variables, also to test the relationship between suicidal behavior and having received/needed psychological treatment within the past 12 months. Multivariable logistic regression was used to identify factors associated with suicidal behavior (ideation and/or attempt; ever in lifetime) and for receiving psychological treatment among those reporting suicidal behavior within the last 12 months. In dummy coding, the biggest subgroup was chosen as a reference for socio-demographic characteristics, and for substance abuse and depression the reference group was the one with no problems. Factors that were statistically significant at the 5 % significance level in univariable analyses were included into the regression models. To measure the logistic regression model’s goodness of fit, comparison of percents classified as correct in the null model was compared with the developed model. Statistical analyses were performed using SPSS 21.
Ethics
The study was approved by the Tallinn Medical Research Ethics Committee. Participation was anonymous and all participants gave written informed consent.
Results
Sample Characteristics
Out of 924 patients invited to participate, 86.6 % agreed to take part in the study (n = 805). Eight hundred PLHIV were included in the analyses (Table 1). At the time of the study, there were 4162 patients registered in the clinics, therefore the study captured 19.2 %. The mean age of participants was 33.9 years (SD = 7.6; range 21–67 years). Of men, 4.1 % (n = 18) identified themselves as bi- or homosexual (seven as gay). Of women, 4.8 % (n = 15) identified themselves as bisexual (none as lesbian). Two-thirds of participants had injected drugs (n = 541; 67.7 %), and half reported problematic alcohol use (n = 400; 53.3 %).
Prevalence of Suicidal Behavior
Most participants (61.4 %; n = 487) had never been suicidal. However, 306 participants (38.6 %) reported suicidal behavior at some point in their life with 51.0 % (n = 156) of them reporting an episode within the past year (19.5 % of the total sample). Suicidal ideation was reported by 36.3 % (n = 288) of the total sample and 54.2 % of them (n = 156) had thought about suicide within the past 12 months. One hundred sixty-two people (20.4 % of the total sample) had attempted suicide and, of them, 24.7 % (n = 40) had made a suicide attempt within the previous year. Twenty people reported having attempted suicide more than a year ago but did not report ever having suicidal thoughts and three people reported a suicide attempt within the past 12 months but recorded that they last thought about suicide more than a year ago.
Factors Associated with Suicidal Behavior
Factors such as age, incarceration, employment, substance abuse (IDU and/or problematic alcohol use), current depression, years since first positive HIV test result (shown in Table 1) were included in multivariable logistic regression to estimate odds of ever engaging in suicidal behavior. The model included answers from 674 people. Null model classified correctly 60.8 % of cases and the developed model 72.4 % of cases.
Depressed people showed higher odds of lifetime suicidal behavior than their non-depressed peers (adjusted OR 6.4; 95 % CI 4.3–9.4; P < 0.001). PLHIV aged 20–24 had higher odds than PLHIV aged 30–34 of having been suicidal at some point in their life (adjusted OR 4.0; 95 % CI 1.5–10.2; P = 0.006). Those reporting both having injected drugs and abused alcohol had higher odds of lifetime suicidal behavior than PLHIV with no substance use problems (adjusted OR 2.7; 95 % CI 1.5–4.8; P < 0.001). People who had been in prison had higher odds than those who had not been in prison of having ever been engaged in suicidal behavior (adjusted OR 1.5; 95 % CI 1.0–2.3; P = 0.043). Those reporting having had the first positive HIV test 5–10 years ago had lower odds of having experienced suicidal behavior than their counterpart with the first HIV + test for more than 10 years ago (adjusted OR 0.61; 95 % CI 0.40–0.94; P = 0.023).
Mental Health Care and Factors Associated with Not Receiving it When Experiencing Suicidal Behavior in the Last 12 Months
Across all the study participants, 9.7, 33.7, and 19.6 % reported using antidepressants, sedatives or psychological treatment, respectively. Just under half of the HIV patients (41 %) perceived the need for psychological treatment. Table 2 presents data and comparison of the use of antidepressants, sedatives and psychological treatment between respondents with (n = 156) and without (n = 637) suicidal behaviour in the last 12 months (recent suicidal behavior). The prevalence of depression (based on measuring symptomatology of previous 4 weeks) was 87.1 % (n = 121) among PLHIV with recent suicidal behavior and 45.1 % (n = 264) among those with no recent suicidal behavior (P < 0.001). People with recent suicidal behavior report receiving significantly more mental health care than their non-suicidal peers (Table 2).
To identify the factors associated with receiving psychological treatment among those with recent suicidal behavior, additional multivariable analysis was executed. Factors significantly associated with past year suicidal behavior in univariable analyses (employment, incarceration, substance abuse, current depression, perceiving a need for psychological treatment, taking antidepressants, and sedatives) were included in this analysis. The model included data from 113 study subjects. Null model classified correctly 69.9 % of cases and the developed model 77.9 % of cases.
Among people who reported recent suicidal behavior, those who perceived a need for psychological treatment had higher odds of receiving it compared to those who perceived no need (adjusted OR = 25.65; 95 % CI 2.92–225.47; P = 0.003). Indeed, when looking at proportions of PLHIV receiving psychological treatment when recently suicidal, only 4.3 % (2/47) of those who did not feel a need for counseling and/or psychotherapy received it compared to 42.0 % (37/88) of those perceiving a need for it. Factors of being depressed (adjusted OR 0.21; 95 % CI 0.03–1.25; P = 0.085) and having received antidepressants (adjusted OR 3.74; 95 % CI 0.95–14.63; P = 0.058) approached significance.
Discussion
This study investigated the prevalence of suicidal behavior (ideation and attempts, during participants’ lifetime and in the past year), factors associated with lifetime suicidal behavior and having received psychological treatment in the previous year among suicidal individuals in HIV outpatient care in Estonia.
We found that 39 % of the surveyed PLHIV reported suicidal behavior at some point in their life. Suicidal ideation (36 %) was the most prevalent form of suicidal behavior. However, suicide attempts were quite common too (20 %). The results are similar to the suicidal behavior prevalence estimates among PLHIV from other countries but are higher than those observed in the general population in Estonia (suicide ideation 16 %, attempts 4 %) [7, 9]. Based on this indirect comparison one might speculate that suicidal behavior is more frequent among PLHIV than in the general population (in Estonia). Some HIV risk behaviors such as substance abuse and high risk sexual behavior have been associated with increased suicidal behavior and contribute to suicidal behavior regardless of HIV serostatus [15, 16, 32–34]. In our sample, two thirds of respondents had a history of injecting drugs and half had a history of alcohol abuse, both behaviors associated with increased suicidal behavior [33]. It is plausible that higher prevalence of suicidal behavior among HIV infected in care captured in this study in comparison to the study among general population can partially be explained by over representation of people already at increased risk for suicidal behavior among PLHIV.
In our study current depression, younger age, having been incarcerated, having injected drugs as well as abused alcohol, and having lived with HIV for over 10 years were associated with the high occurrence of lifetime suicidal behaviour. These results are in agreement with previous studies among PLHIV as well as in general populations [12, 13]. In addition, reporting more suicidal behaviour among those living with HIV for more than a decade is similar to the pattern found in other chronic diseases—which is how HIV is often regarded nowadays [35, 36]. We did not find an association with gender which is in disagreement with previous research [12, 13]. However, the identified factors of suicidal behavior in our study such as drug/alcohol use and incarceration were overrepresented among male respondents. It is plausible that in our sample behavioural and health related factors had a stonger effect on suicidal behavior than gender.
In our study, PLHIV with recent suicidal behavior were more likely than their counterparts to report uptake of mental health care (use of antidepressants, sedatives, and receiving psychological treatment). This can be seen as a positive finding, given that individuals with higher risk for fatal suicide (suicidal behavior) are receiving the care they need.
Psychological treatment is a cornerstone of managing a suicidal patient in outpatient care [20]. Not perceiving a need for psychological treatment was the single most important association we found with not receiving such treatment. To our knowledge this is the first time this phenomenon has been observed among PLHIV although it has been shown in the general population [21]. Still, less than half of those in need (40 % of those who perceived a need) and less than third (27 %) of all recently suicidal PLHIV actually received psychological treatment. There is a clear gap between the need for and actual use of mental health care. The gap can be potentially attributed to both patient and health care related factors. In Estonia, mental health care is not integrated with HIV medical care (except opioid substitution therapy for HIV infected PWID). PLHIV can access mental health care outside HIV care/clinics (however, psychiatric care is expensive in the private sector and has a long waiting list in the public sector). Our results indicate that there is a clear need for additional mental health services for PLHIV. For better access, mental health care should be integrated with HIV medical care (psychiatrists, clinical psychologists) [37]. Based on our results assessing psychological morbidity at each HIV care visit as suggested by the European Guidelines for treatment of HIV-positive adults in Europe is well justified [38]. HIV care providers could consider following treatment guidelines for depression used in primary care in Estonia [26].
This study has some limitations. First of all, we are describing factors associated with suicidal ideation and/or attempts; these might differ from factors that increase the likelihood of lethal suicides. The cross-sectional study design does not allow us to establish the direction of the associations described (e.g. for the association of suicidal behavior with substance abuse or depression). Third, the external validity of the study results cannot be ensured (non-probability sampling; exclusion of PLHIV not in HIV care). However, we note the high response rate within the study participation. Characteristics and treatment experiences of those who completed suicide prior to the study remain unknown. Survey studies are prone to several measurement biases. We used several measures to reduce social desirability bias such as anonymous study design, carefully selected questionnaire design (ordering, wording) and survey strategy (self administered in a private room). We assumed that patients were aware of the psychological treatment they received and why they received it. While these limitations are important, we feel it is unlikely that they created the patterns that we observed in the data. Rather, we believe that these patterns were sufficiently strong that they reflect the actual situation despite the study’s limitations.
Conclusions
In conclusion, a large proportion of PLHIV in Estonia has been suicidal and does not perceive a need for counseling and/or psychotherapy. Factors associated with suicidal behavior among PLHIV are similar to those found among general or key populations at risk for HIV.
References
WHO. Preventing suicide: a global imperative. Geneva: WHO; 2014.
Aldaz P, Moreno-Iribas C, Egues N, et al. Mortality by causes in HIV-infected adults: comparison with the general population. BMC Public Health. 2011;11:300.
Ehren K, Hertenstein C, Kummerle T, et al. Causes of death in HIV-infected patients from the Cologne–Bonn cohort. Infection. 2014;42(1):135–40.
Weber R, Ruppik M, Rickenbach M, et al. Decreasing mortality and changing patterns of causes of death in the Swiss HIV Cohort Study. HIV Med. 2013;14(4):195–207.
Schwarcz SK, Vu A, Hsu LC, Hessol NA. Changes in causes of death among persons with AIDS: San Francisco, California, 1996–2011. AIDS Patient Care STDS. 2014;28(10):517–23.
Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry. 2008;192(2):98–105.
Tekkel M, Veideman T. Health behavior among Estonian adult population, 2014. Tallinn: National Institute for Health Development; 2015.
Runeson B, Tidemalm D, Dahlin M, Lichtenstein P, Långström N. Method of attempted suicide as predictor of subsequent successful suicide: national long term cohort study. BMJ. 2010;341:c3222.
Catalan J, Harding R, Sibley E, Clucas C, Croome N, Sherr L. HIV infection and mental health: suicidal behavior: systematic review. Psychol Health Med. 2011;16(5):588–611.
Keiser O, Spoerri A, Brinkhof MWG, Hasse B, Gayet-Ageron A, Tissot F, et al. Suicide in HIV-infected individuals and the general population in Switzerland, 1988–2008. Am J Psychiatry. 2010;167(2):143–50.
Schadé A, van Grootheest G, Smit JH. HIV-infected mental health patients: characteristics and comparison with HIV-infected patients from the general population and non-infected mental health patients. BMC Psychiatry. 2013;13:35.
O’Connor RC, Nock MK. The psychology of suicidal behaviour. Lancet Psychiatry. 2014;1(1):73–85.
Passos SM, Souza LD, Spessato BC. High prevalence of suicide risk in people living with HIV: who is at higher risk? AIDS Care. 2014;26(11):1379–82.
Jia CX, Mehlum L, Qin P. AIDS/HIV infection, comorbid psychiatric illness, and risk for subsequent suicide: a nationwide register linkage study. J Clin Psychiatry. 2012;73(10):1315–21.
Jin H, Atkinson H, Duarte NA, et al. Risks and predictors of current suicidality in HIV-infected heroin users in treatment in Yunnan, China: a controlled study. J Acquir Immune Defic Syndr. 2013;62(3):311–6.
Abelson J, Lambevski S, Crawford J, Bartos M, Kippax S. Factors associated with ‘feeling suicidal’: the role of sexual identity. J Homosex. 2006;51(1):59–80.
Hawton K, van Heeringen K. Suicide. Lancet. 2009;373(9672):1372–81.
van der Feltz-Cornelis CM, Sarchiapone M, Postuvan V, et al. Best practice elements of multilevel suicide prevention strategies: a review of systematic reviews. Crisis. 2011;32(6):319–33.
Cuijpers P, de Beurs DP, van Spijker BA, Berking M, Andersson G, Kerkhof AJ. The effects of psychotherapy for adult depression on suicidality and hopelessness: a systematic review and meta-analysis. J Affect Disord. 2013;144(3):183–90.
The US Department of Veterans Affairs. The US Department of Defense. Assessment and management of patients at risk for suicide: VA/DoD clinical practice guideline. 2013.
Bruffaerts R, Demyttenaere K, Hwang I, Chiu WT, Sampson N, Kessler RC, et al. Treatment of suicidal people around the world. Br J Psychiatry. 2011;199(1):64–70.
UNAIDS. Global AIDS update 2016. 2016.
UNAIDS. The gap report. Geneva: UNAIDS; 2014.
Estonian Health Board. 2015. aastal Eestis diagnoositud HIV-positiivsed (People newly diagnosed with HIV in Estonia in 2015). Tallinn, 2016.
Aluoja A, Shlik J, Vasar V, Luuk K, Leinsalu M. Development and psychometric properties of the Emotional State Questionnaire, a self-report questionnaire for depression and anxiety. Nord J Psychiatry. 1999;53(6):443–9.
Kleinberg A, Jaanson P, Lehtmets A, et al. Depressiooni ravijuhend perearstidele (Guidelines for managing depression in primary care). Eesti Arst. 2011;90(9):431–46.
Kalichman SC, Heckman T, Kochman A, Sikkema K, Bergholte J. Depression and thoughts of suicide among middle-aged and older persons living with HIV-AIDS. Psychiatr Serv. 2000;51(7):903–7.
Simoni JM, Safren SA, Manhart LE, et al. Challenges in addressing depression in HIV research: assessment, cultural context, and methods. AIDS Behav. 2011;15(2):376–88.
Oopik P, Aluoja A, Kalda R, Maaroos HI. Screening for depression in primary care. Fam Pract. 2006;23(6):693–8.
Skogen JC, Overland S, Knudsen AK, Mykletun A. Concurrent validity of the CAGE questionnaire. The Nord-Trondelag health study. Addict Behav. 2011;36(4):302–7.
Ewing JA. Detecting alcoholism: the CAGE questionnaire. JAMA. 1984;252(14):1905–7.
Blosnich JR, Nasuti LJ, Mays VM, Cochran SD. Suicidality and sexual orientation: characteristics of symptom severity, disclosure, and timing across the life course. Am J Orthopsychiatr. 2016;86(1):69–78.
Yuodelis-Flores C, Ries RK. Addiction and suicide: a review. Am J Addict. 2015;24(2):98–104.
Houck CD, Hadley W, Lescano CM, Pugatch D, Brown LK. Suicide attempt and sexual risk behavior: relationship among adolescents. Arch Suicide Res. 2008;12(1):39–49.
Bisschop MI, Kriegsman DM, Deeg DJ, Beekman AT, van Tilburg W. The longitudinal relation between chronic diseases and depression in older persons in the community: the Longitudinal Aging Study Amsterdam. J Clin Epidemiol. 2004;57(2):187–94.
Deeks SG, Lewin SR, Havlir DV. The end of AIDS: HIV infection as a chronic disease. Lancet. 2013;382(9903):1525–33.
WHO. HIV/AIDS treatment and care in Estonia. Estonia: WHO; 2014.
European AIDS Clinical Society. European guidelines for treatment of HIV-positive adults in Europe. Barcelona: European AIDS Clinical Society; 2015.
Acknowledgments
We would like to thank all members of the HIV-BRIDGE Study Group: (in alphabetical order) Tiiu Aug, Tatiana Fishkova, Marjana Golubnitšija, Anne Junolainen, Kerstin Kase, Kersti Kink, Juta Kogan, Olev Lumiste, Merike Meindok, Irina Milaševitš, Helen Mülle, Liudmila Ponomarenko, Natalia Nikitina, Svetlana Semjonova, Irina Sorokina, Jelena Šmidt, and Kai Zilmer, as well as Lilia Novikova for their valuable contribution.
Funding
The study was funded by the European Union through the European Regional Development Fund within the research project “Bridging the gap in knowledge and practice of prevention and care for HIV in Estonia (HIV-BRIDGE)”, the Estonian Ministry of Education and Research (Grant #IUT34-17), and National Institute for Health Development, Estonia, through National Health Plan 2009–2020.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of Interest
Liis Lemsalu declares that she has no conflict of interest. Kristi Rüütel declares that she has no conflict of interest. Kaja-Triin Laisaar declares that she has no conflict of interest. Liilia Lõhmus declares that she has no conflict of interest. Aire Raidvee declares that she has no conflict of interest. Anneli Uusküla declares that she has no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Lemsalu, L., Rüütel, K., Laisaar, KT. et al. Suicidal Behavior Among People Living with HIV (PLHIV) in Medical Care in Estonia and Factors Associated with Receiving Psychological Treatment. AIDS Behav 21, 1709–1716 (2017). https://doi.org/10.1007/s10461-016-1561-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-016-1561-0