
Abstract
To determine operational and analytical characteristics of respondent-driven sampling (RDS) in international settings and to explore factors that may affect recruitment of most-at-risk populations using RDS, we reviewed HIV biological and behavioral surveillance studies that used this method outside of the United States. We identified 123 eligible studies, 59 from Europe, 40 from Asia and the Pacific, 14 from Latin America, seven from Africa and three from Oceania. Studies collectively recruited 32,298 participants between 2003 and 2007; 53% of studies were conducted among injecting drug users, which generally had faster recruitment compared with studies among sex workers. All but 13 studies reached ≥90% of their intended sample size, and six studies failed to reach equilibrium for key variables. This review has shown that RDS is an effective technique, when designed and implemented appropriately, to sample most-at-risk populations for HIV biological and behavioral surveys.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
With 33.2 million people worldwide currently infected, and with 2.1 million deaths in 2007 alone, the HIV pandemic is one of the most significant public health challenges of the 21st century (UNAIDS 2007). In most countries, the HIV epidemic is driven by sub-populations at highest risk (termed “most-at-risk populations”) for becoming infected with or transmitting HIV (UNAIDS/WHO Working Group on Global HIV/AIDS and STI Surveillance 2000). In two types of epidemic, low-level (prevalence of infection is <5% in most-at-risk populations) and concentrated (prevalence is >5% in most-at-risk populations but is not yet >1% in the general population) these most-at-risk populations include injecting drug users (IDUs), men who have sex with men (MSM), and sex workers (SWs) along with their sexual partners, as well as displaced populations, migrant workers, long-distance truck drivers, and youth (Mills et al. 2004). Even in generalized epidemics, in which prevalence is >1% in pregnant women attending antenatal clinics, there is recognition that risk is not uniformly distributed within populations and is driven, at least initially, by most-at-risk populations that bridge HIV to the lower-risk general population (Chopra et al. 2007; Doherty et al. 2006; Gregson et al. 2002; Halperin and Epstein 2004).
Accurate HIV data on incidence and prevalence and associated behavioral data from most-at-risk populations are essential for designing targeted prevention programs to reduce the further spread of the epidemic (Mills et al. 2004; Pisani et al. 2003; Zaba et al. 2006). In most countries, however, HIV surveillance systems, the primary source of epidemiologic data, do not generate representative samples of most-at-risk populations. Although probability-based sampling methods are the gold standard for collecting unbiased and generalizable biological and behavioral data on HIV, their application is limited when sampling most-at-risk populations such as IDUs, MSM and SWs, especially the hidden subsets of these groups. The methods are limited, first of all, because these populations generally do not have sampling frames from which to draw random samples using conventional probability-based sampling methods. In addition, the groups are too small to be captured in large enough numbers in surveys of the general population. Second, individuals within these populations often practice socially stigmatized or illegal behaviors, resulting in difficulties accessing them. As a result, they are often recruited through institutions (e.g., hospitals, jails, drug-treatment clinics) using convenience techniques, such as quota and snowball sampling, or they are recruited through visible venues (e.g., bars, clubs, street corners, shooting galleries) using targeted sampling (Magnani et al. 2005; Semaan et al. 2002; Watters and Biernacki 1989).
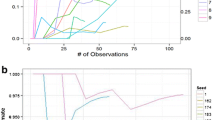
Respondent-driven sampling (RDS) is a relatively new sampling method that has been recognized and adopted by public health researchers as a promising alternative means to sample most-at-risk populations for biological and behavioral HIV surveys. RDS is a chain-referral sampling technique that uses statistical adjustments for network size to produce generalizable samples (Abdul-Quader et al. 2006a; Heckathorn 1997, 2002; Magnani et al. 2005; Salganik and Heckathorn 2004; Semaan et al. 2002). The RDS recruitment process begins with a set number of individuals, or “seeds,” selected purposefully from the target population. Seeds are trained to recruit a set number of individuals (“recruitment quota”) from their social network of peers. The recruits of the seeds who enroll in an RDS study are also trained to recruit a set number of individuals from their social network of peers. Both seeds and recruited participants typically receive incentives, both to be interviewed (referred to as “primary incentives”) and to refer additional recruits (“secondary incentives”). Ideally, this recruitment process continues to produce long recruitment “chains” made up of several “waves” of recruits. As the recruitment chains lengthen, the composition of the sample begins to reach a point of “equilibrium” whereby the composition of certain characteristics (e.g., age group, gender, ethnicity, HIV prevalence) within the sample eventually stabilizes, indicating that the final sample is not biased by the purposeful selection of seeds (Heckathorn 2002). It is generally understood that RDS can be applied only in populations that are socially networked and in which members of the networks are willing to recruit from among their peers.
In addition to the recruitment process, RDS involves a complex analytical component that is crucial to generate representative estimates and confidence intervals. It is done through adjustments that factor in the sizes of participants’ social networks and the sample’s different recruitment patterns. In this paper, we refer to RDS as both the recruitment and analysis components.
Respondent-driven sampling was first used in 1994 to study HIV-related risk behaviors among IDUs in the eastern United States (Heckathorn 1997). Outside the United States, RDS was not used for HIV surveillance until 2003 (Wattana et al. 2007), but since then it has been employed widely by international researchers to gather biological and behavioral data on HIV. To date, there are ongoing discussions about the effectiveness of RDS in different socio-cultural settings and among certain most-at-risk populations (Abdul-Quader et al. 2006b). Additionally, misunderstandings exist about RDS methodology, the importance of statistical adjustment, and the method’s requirements (Heimer 2005; Johnston et al. 2008; Ramirez-Valles et al. 2005; Salganik 2006; Simic et al. 2006). To address these issues, we reviewed biological and/or behavioral HIV surveillance surveys that used RDS and that were conducted outside of the United States to sample HIV most-at-risk populations. In this papar, we summarize operational and analytical characteristics of RDS studies and discuss factors that may affect recruitment. Implementation and theoretical challenges to RDS studies are discussed in a companion paper (Johnston et al. 2008).
Methods
Literature Search
We searched published and unpublished manuscripts, abstracts, reports, protocols and notes from field supervisors related to HIV biological and/or behavioral surveillance (accessible from 2003 through October 1, 2007) that involved RDS in countries other than the United States. We excluded studies based in the United States because those conducted prior to 2006 have already been or are currently being reviewed (Abdul-Quader et al. 2006b; Robinson et al. 2006). We conducted initial searches using MEDLINE (1970–2007), PubMed and Google Scholar (up to the first 50 pages). This search included an iterative process to refine the search strategy by testing several search terms and incorporating new search terms as new relevant citations were identified. Multiple combinations of keywords and phrases were used to assess study eligibility, including: (1) methodology: “chain-referral sampling” or “respondent-driven sampling”; (2) population of interest: “men who have sex with men”, “bisexual”, “sex workers” (male, female, transgender) and their partners, “drug users” (injectors or non-injectors), “homeless”, “run-away youth” or “migrant population”; (3) medical domains: “HIV”, “HCV”, “sexually transmitted infections”, “drug abuse”, “overdose” and “needle sharing”; (4) language: documents in English, Spanish, French, Portuguese, Farsi, or Arabic; (5) location: studies conducted in a country or countries other than the United States. We further conducted a “cited reference search” in Web of Science on the relevant papers and used the “related articles feature” in PubMed.
The majority of data was provided by co-authors and their collaborators directly involved in conducting RDS surveys and through contacts with organizations involved in specific RDS surveys, including Tulane University School of Public Health and Tropical Medicine; University of California, San Francisco Global Health Sciences; the Global AIDS Program, Centers for Disease Control and Prevention; Family Health International; the Federal University of Ceará, Brazil; and national ministries of health.
Eligibility Criteria
We assessed articles identified through our original search and differentiated studies that used the RDS recruitment process and analytical elements from those that did not. First we included studies in our review that (1) initiated recruitment chains with members of the target population, known as seeds; (2) used a recruitment quota; (3) collected data on the size of social network for all participants using a consistent set of parameters; and (4) systematically recorded who recruited whom. To ascertain whether a study was conducted among a population that was socially networked, we included only studies that either reported that one or more seeds could generate a minimum of three referral waves or, in case waves were unreported, that the study attained a minimum of 10% of its desired sample size. Second, we also excluded studies that (1) did not generate weighted estimates of variable frequency and confidence intervals using data on network size or, in the case of studies with only recently completed data collection, did not intend to use weighting in their analysis; (2) combined an RDS sample with other samples generated using other methods; or (3) combined samples from multiple RDS studies with different eligibility criteria or conducted in distinct geographical areas. We considered studies that fulfilled all inclusion criteria as complete RDS studies and included them in our review.
Categorizing Documents and Abstraction
We created a master table in Microsoft Excel, extracted key information from included surveys, and entered data into the table. Once we completed data entry, we divided studies into four sub-tables based on the population of interest: IDU, MSM, SW and high-risk heterosexual (HRH) men. We abstracted (1) the principal investigator or contact person or organization; (2) the year of the study; (3) where the survey was conducted; (4) eligibility criteria; (5) types of biological specimen(s) gathered and laboratory tests performed; (6) whether formative research was conducted prior to the survey; (7) interview method; (8) number of recruitment sites; (9) type of recruitment site; (10) whether mobile recruitment sites were used; (11) whether seeds were diversified, meaning they were selected differently from each other based on key demographic or risk behavior characteristics; (12) total number of seeds used for the study; (13) number of seeds that failed to recruit anyone; (14) whether additional seeds were added after the study began; (15) the maximum number of allowable referrals; (16) whether an expiration period was used, meaning the total number of days between when a participant completes the survey and his or her recruited peer enrolls in the survey; (17) the primary incentive amount, which is the amount given for completing the survey in US dollars calculated on October 15, 2007; (18) the secondary incentive amount, which is the amount given for each participant-referred recruit who enrolls in the survey; (19) other services offered during the survey; (20) design effect used to calculate a sample size; (21) desired sample size; (22) actual sample size; (23) maximum number of waves; (24) sampling duration in weeks; (25) whether equilibrium was reported as being reached; (26) whether survey data were adjusted using respondent-driven sampling analysis tool (RDSAT) (Volz et al. 2007) or a similar software program; and (27) description of any operational limitations.
We assessed the success of each study by the proportion of the pre-designated sample size that was actually recruited and whether the authors reported reaching equilibrium. We compared the number of successful recruits per seed per week using the Mann–Whitney U test with significance at P = 0.05 in STATA version 10 (StataCorp, College Station, Texas).
Results
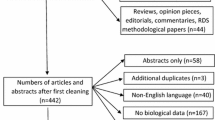
We identified 155 biological and/or behavioral HIV surveys that were conducted among most-at-risk populations outside of the United States. Of these, 32 (21%) studies did not fulfill our RDS criteria and were excluded. Nineteen (59%) of these studies combined RDS samples with samples collected using other sampling techniques; five (16%) failed to generate a minimum of three referral waves, four (13%) either did not report whether they had collected data on size of the social networks or reported them inconsistently; two (6%) did not analyze their data using proper RDS techniques; one (3%) did not provide sufficient information about RDS recruitment requirements: and one (3%) combined samples from two different RDS studies.
One hundred twenty-three studies met all of our eligibility criteria. Of these, one study was completed in 2003, nine studies in 2004, 34 in 2005, 65 in 2006, and 14 in 2007. Studies were conducted in 28 different countries and five continents: Europe (59, 48%), Asia (40, 33%), Latin America (14, 11%), Africa (7, 6%) and Oceania (3, 2%) (Table 1). Sixty-five studies (52%) were among IDUs (Table 2), 39 (32%) among MSM (Table 3), 18 (15%) among SW (Table 4), and one (1%) among HRH men (Table 5). Between 2003 and October 2007, a total of 32,298 participants were surveyed, of whom 17,434 (54.0%) were IDUs, 10,101 (31.0%) were MSM, 4,342 (13.5%) were SWs, and 421 (1.5%) were HRH men.
One hundred six studies (86%) reported collecting both HIV biological and behavioral data concurrently, and the remaining 17 (14%) were solely behavioral surveys. Sixty-four (53%) collected dried blood spots, 44 (36%) venous blood, 6 (5%) oral fluid and 25 (21%) urine or penile or vaginal swabs. Of the 112 studies with available information, 101 (90%) reported conducting some degree of a priori formative research. Although face-to-face methods were the most common means of interviewing (110 studies, 89%), audio computer-assisted structured interviews (ACASI) and self-administered instruments were used in eight (7%) and five (3%) studies, respectively. Participants were enrolled at a variety of sites including governmental hospitals, public health clinics, public health departments, non-governmental organizations providing services for target groups, voluntary counseling and testing clinics, hotel rooms, rented store fronts, and mobile vans. Of the 114 studies that reported the number of recruitment sites, 92 (81%) used a single site, but as many as five sites were used. Only six (5%) studies reported using mobile vans as recruitment sites; and in one study, two vans were used but in stable locations.
One hundred twenty (99%) studies reported that seeds were diversified (i.e., selected differently from each other) based on key demographic or risk behavior characteristics; three studies did not report on diversification. Thirty-one (43%) of 72 studies with available data reported adding seeds beyond the original seeds. All but three studies set the allowable number of recruits per participant at three. Of 103 studies with available data, 59 (57%) did not limit the time during which participants were allowed to refer their recruits. Among 44 studies that did limit time for recruits to respond, the recruitment period ranged from 7 to 60 days.
Studies used a wide range of primary and secondary incentives for recruitment. Of the 107 studies that reported using primary incentives, a majority of 89 (83%) used cash incentives, 11 (10%) gave cash equivalents (e.g., food stamps) or small goods with minimal monetary value and 3 (3%) gave condoms and lubricants; 4 (4%) did not offer any primary incentive. Seventy-eight studies reported data on secondary incentives, and 72 (92%) offered them; these incentives were usually monetary (58 studies, 74%). Seventy-eight studies reported data on both primary and secondary incentives; the value of the primary incentive was higher than that of the secondary incentive in 52 (67%) studies, the same in 14 (18%), lower in seven (13%) and undetermined in four (5%) studies. One (1%) study did not offer any kind of incentive. Of these 78 studies, 55 (71%) gave money as both primary and secondary incentives, 8 (11%) provided money only for one of them, and 15 (19%) did not offer monetary incentives at all. In addition to incentives, studies offered a wide range of additional services, such as free HIV testing and counseling, referral for clinical follow-up, condoms, lubricants and information and educational materials.
We also summarize how successfully studies were able to recruit participants (Table 6). On average, RDS studies used 10 seeds (range, 2–32, median 8.0, intra-quartile range [IQR] 6.0–13.0) and had 1.6 (range 0–19, median 0, IQR 0–2.0) unsuccessful seeds per study. Of 86 studies with available data, 51 (59%) reported having no unsuccessful seeds. The median proportion of unsuccessful seeds per study was lower among studies of IDUs (0%, IQR, 0–5%) than among SWs (20%, IQR 14–30%, z score −3.872, P < 0.0005). There was no significant difference in the median proportion of unsuccessful seeds per study between MSM and IDUs (z score −0.915) or MSM and SWs (z score −1.916). The greatest number of referral waves was among IDUs (34); the average number for all studies was 9.2 waves (median 8.0, IQR 6.0–11.0, range 3–34).
The length of time for recruitment of subjects ranged from 2 to 56 weeks, with an average of 9.2 weeks (median 8.0 weeks, IQR 4.0–10.0). On average, studies recruited 41.0 (median 35.0, IQR 25.0–50.0) subjects per week or 6.4 subjects per seed per week (median 5.2, IQR 2.0–9.1). The recruitment process was relatively more productive in studies of IDUs (median of 7.5 recruits per seed per week), and slower in studies of MSM and SWs (3.6, z score 2.837, P < 0.005) and (3.5, z score 2.727, P < 0.01), respectively (Table 6). There was no significant difference in median recruits per seed per week between MSM and SW studies (z score 0.199).
In 91 studies with available data, design effects varied from 1.0 to 2.5; only 34 (38%) used a design effect of ≥1.5 when calculating sample sizes. One hundred eighteen (83%) studies reported their calculated sample size; the average was 280 and ranged from 100 to 800. One hundred eighteen (83%) studies also reported their final sample size, which ranged from 59 to 963 and averaged 273 (median 247.0, IQR 197–377.0). One hundred thirteen studies reported both calculated (desired) and final (recruited) sample sizes. Studies on average reached 98% of their intended sample size; studies among IDUs reached a greater proportion of their intended sample size (100.0%) than studies of SWs (97.0%) and MSM (94.0%). Thirteen studies (12%) failed to attain at least 90% of their intended sample size; 6 (46%) of these were MSM studies, 4 (31%) SW studies and three (20%) IDU studies. Eleven (85%) of these studies, nonetheless, reached equilibrium on at least one key variable of interest despite shortfalls in recruitment.
Of the 105 studies that reported whether or not they had reached equilibrium, 99 (94%) reached equilibrium and six (6%) had not. These six studies included four studies of IDUs and two studies of SWs. All four IDU studies attained intended sample sizes despite these two SW studies. Of the 18 studies that did not report whether or not they had reached equilibrium, 16 (89%) attained at least 90% of their intended sample size. All but two studies that completed data collection and attained their sample size used RDSAT software to adjust data for different social network sizes and recruitment patterns, and the other two used other methods of adjustment.
Discussion
We were able to identify 123 HIV biological and/or behavioral surveys that used RDS and were conducted outside the United States. The studies were conducted in 28 countries in five continents and had an average sample size of 273 participants. Over 32,000 IDUs, MSM, SWs and HRH men were surveyed in these 123 studies. We are also aware of at least 18 additional HIV biological and/or behavioral studies that, as of October 1, 2007, are being conducted around the world.
We found substantial methodological heterogeneity among the studies. The majority of the studies used formative research, face-to-face interview formats, three referrals per participant, a single interview site for data collection and biological specimens collected from participants, mostly for HIV but also for other sexually and parenterally transmitted infections. Types of sites, number of seeds and types of incentives varied. During data collection, some studies added seeds if recruitment slowed or seeds failed to recruit any peers. The use of some incentive was relatively constant across the studies, consistent with standard RDS methods.
Notably, we found that RDS has been somewhat more successful in IDU studies in terms of recruitment efficiency, as measured by the number of new participants referred per seed for week. Our findings show that RDS studies took 9 weeks to complete on average, but in some cases studies took as long as several months. This variation, however, can be explained; these studies had many differences (e.g., sample sizes, number of seeds, target populations) that would most likely affect the length of the study. Furthermore, investigators can manipulate the process to accelerate or slow recruitment for operational reasons (Johnston et al. 2007).
Our review is subject to several limitations. Like any systematic review, ours is limited by how complete our search was and how complete the reports were once we identified them. Although there may be a few studies that we were unable to find, we believe our search was comprehensive and complete to the greatest extent possible. We also found that many reports were missing key data, which introduced uncertainty into our calculations of average number of initial and added seeds, size of a design effect (if used), desired and recruited sample sizes, number of recruitment waves and sampling duration. Finally, our findings can be affected by multiple RDS studies using the same RDS protocol but conducted in different cities within one country, such as occurred in Ukraine and India (Appendix: references 6, 8).
To assess whether any of these studies generated representative data, detailed information about the implementation and analytical characteristics of each RDS study is needed. In the future it may prove useful to establish certain key data that should be reported for each RDS study, as has been done for randomized controlled trials (Moher et al. 2001) and observational (Von Elm et al. 2007) and qualitative studies (Tong et al. 2007). In general, we suggest that RDS studies should report the following items: (1) whether formative research was conducted, the quality and quantity of such research, and whether the population under study was found to be socially networked; (2) comprehensive description of eligibility criteria; (3) how initial and replacement seeds were selected and how they were found; (4) the maximum number of allowable referrals per participants; (5) whether the recruiter–recruit relationship was tracked; (6) whether a design effect was used during calculation of sample size and the size of the design effect; (7) the sample size calculated versus the sample size attained; (8) the maximum number of recruitment waves attained; (9) length of time needed for data collection; (10) whether equilibrium was reached and for which variables; (11) how the sizes of participants’ social networks were measured; and (12) whether survey data were adjusted using RDSAT or a similar software program.
Our review shows that RDS has been used widely for HIV prevalence and risk behavior surveillance in most-at-risk populations. When designed and conducted correctly, RDS is a valuable method for monitoring trends, better understanding epidemic dynamics and evaluating the effect of public health programs.
References
Abdul-Quader, A. S., Heckathorn, D. D., McKnight, C., Bramson, H., Nemeth, C., Sabin, K., et al. (2006a). Effectiveness of respondent-driven sampling for recruiting drug users in New York City: Findings from a pilot study. Journal of Urban Health, 83, 459–476. doi:10.1007/s11524-006-9052-7.
Abdul-Quader, A. S., Heckathorn, D. D., Sabin, K., & Saidel, T. (2006b). Implementation and analysis of respondent driven sampling: Lessons learned from the field. Journal of Urban Health, 83(Supplement 7), 231–235. doi:10.1007/s11524-006-9029-6.
Bozicevic, I., Rode, O., Zidovec-Lepej, S., Johnston, L. G., Stulhofer, A., Dominkovic, Z., et al. (2008). Prevalence of sexually transmitted infections among men who have sex with men in Zagreb, Croatia. AIDS and Behavior (submitted).
Chopra, M., Johnston, L. G., Townsend, L., Mathews, C., Cloete, N., Shaikh, N., & Qotole, M. (2007). HIV prevalence and associated risk behavioural surveillance among ‘sugar daddies’ in Cape Town. Presented at the South Africa AIDS Conference. 2007. Durban, South Africa, 2007.
Doherty, I. A., Shiboski, S., Ellen, J. M., Adimora, A. A., & Padian, N. S. (2006). Sexual bridging socially and over time: A simulation model exploring the relative effects of mixing and concurrency on viral sexually transmitted infection transmission. Sexually Transmitted Diseases, 33, 368–373. doi:10.1097/01.olq.0000194586.66409.7a.
Frost, S. D., Brouwer, K. C., Firestone Cruz, M. A., Ramos, R., Ramos, M. E., Lozada, R. M., et al. (2006). Respondent-driven sampling of injection drug users in two U.S.-Mexico border cities: Recruitment dynamics and impact on estimates of HIV and syphilis prevalence. Journal of Urban Health, 83(Supplement 7), 83–97. doi:10.1007/s11524-006-9104-z.
Gregson, S., Nyamukapa, C. A., Garnett, G. P., Mason, P. R., Zhuwau, T., Caraël, M., et al. (2002). Sexual mixing patterns and sex-differentials in teenage exposure to HIV infection in rural Zimbabwe. Lancet, 359, 1896–1903. doi:10.1016/S0140-6736(02)08780-9.
Halperin, D. T., & Epstein, H. (2004). Concurrent sexual partnerships help to explain Africa’s high HIV prevalence: Implications for prevention. Lancet, 364, 4–6. doi:10.1016/S0140-6736(04)16606-3.
Heckathorn, D. D. (1997). Respondent driven sampling: A new approach to the study of hidden populations. Social Problems, 44, 174–199. doi:10.1525/sp. 1997.44.2.03x0221m.
Heckathorn, D. D. (2002). Respondent driven sampling II: Deriving valid population estimates from chain-referral samples of hidden populations. Social Problems, 49, 11–34. doi:10.1525/sp. 2002.49.1.11.
Heimer, R. (2005). Critical issues and further questions about respondent-driven sampling: Comment on Ramirez-Valles, et al.. AIDS and Behavior, 9(Supplement 4), 403–408. doi:10.1007/s10461-005-9030-1.
Johnston, L. G., Khanam, R., Reza, M., Khan, S. I., Banu, S., Alam, M. S., et al. (2007). The effectiveness of respondent driven sampling for recruiting males who have sex with males in Dhaka, Bangladesh. AIDS and Behavior [Epub ahead of print].
Johnston, L. G., Malekinejad, M., Rifkin, M. R., Kendall, C., & Rutherford, G. W. (2008). Implementation challenges to using respondent-driven sampling methodology for HIV biological and behavioral surveillance: Field experiences in international settings. AIDS and Behavior (in press).
Johnston, L. G., Sabin, K., Mai, T. H., & Pham, T. H. (2006). Assessment of respondent driven sampling for recruiting female sex workers in two Vietnamese cities: Reaching the unseen sex worker. Journal of Urban Health, 83(Supplement 7), 16–28. doi:10.1007/s11524-006-9099-5.
Kajubi, P., Kamya, M. R., Raymond, H. F., Chen, S., Rutherford, G. W., Mandel, J. S., et al.(2007). Gay and bisexual men in Kampala, Uganda. AIDS and Behavior [Epub ahead of print].
Ma, X., Qiyun, Z., Xiong, H., Zhao, J., Sun, W., Hai, Y., et al. (2007). Trends in prevalence of HIV, syphilis, hepatitis C, hepatitis B, and sexual risk behavior among men who have sex with men. Journal of Acquired Immune Deficiency Syndromes (submitted).
Magnani, R., Sabin, K., Saidel, T., & Heckathorn, D. (2005). Sampling hard to reach and hidden populations for HIV surveillance. AIDS (London, England), 19(Supplement 2), S67–S72. doi:10.1097/01.aids.0000172879.20628.e1.
Mills, S., Saidel, T., Magnani, R., & Brown, T. (2004). Surveillance and modelling of HIV, STI, and risk behaviors in concentrated HIV epidemics. Sexually Transmitted Infections, 80, 57–62. doi:10.1136/sti.2004.011916.
Moher, D., Schulz, K. F., & Altman, D. G. (2001). The CONSORT statement: Revised recommendations for improving the quality of reports of parallel-group randomised trials. Lancet, 357, 1191–1194. doi:10.1016/S0140-6736(00)04337-3.
Pisani, E., Dadun, Sucahya, P. K., Kamil, O., & Jazan, S. (2003). Sexual behavior among injection drug users in three Indonesian cities carries a high potential for HIV spread to noninjectors. Journal of Acquired Immune Deficiency Syndromes, 3, 403–406. doi:10.1097/00126334-200312010-00007.
Platt, L., Wall, M., Rhodes, T., Judd, A., Hickman, M., Johnston, L. G., et al. (2006). Methods to recruit hard-to-reach groups: Comparing two chain referral sampling methods of recruiting injecting drug users across nine studies in Russia and Estonia. Journal of Urban Health, 83(Supplement 7), 39–53. doi:10.1007/s11524-006-9101-2.
Ramirez-Valles, R., Heckathorn, D. D., Vázquez, R., Diaz, R. M., & Campbell, R. T. (2005). The fit between theory and data in respondent-driven sampling: Response to Heimer. AIDS and Behavior, 9, 409–414. doi:10.1007/s10461-005-9031-0.
Robinson, W. T., Risser, J. M., McGoy, S., Becker, A. B., Rehman, H., Jefferson, M., et al. (2006). Recruiting injection drug users: A three-site comparison of results and experiences with respondent-driven and targeted sampling procedures. Journal of Urban Health, 83(Supplement 7), 29–38. doi:10.1007/s11524-006-9100-3.
Salganik, M. J. (2006). Variance estimation, design effects and sample size calculations for respondent driven sampling. Journal of Urban Health, 83(Supplement 7), 98–112. doi:10.1007/s11524-006-9106-x.
Salganik, M. J., & Heckathorn, D. D. (2004). Sampling and estimation in hidden populations using respondent-driven sampling. Sociological Methodology, 34, 193–239. doi:10.1111/j.0081-1750.2004.00152.x.
Semaan, S., Lauby, J., & Liebman, J. (2002). Street and network sampling in evaluation studies of HIV risk-reduction interventions. AIDS Reviews, 4, 213–223.
Simic, M., Johnston, L. G., Platt, L., Baros, S., Andjelkovic, V., Novotny, T., et al. (2006). Exploring barriers to ‘respondent driven sampling’ in sex worker and drug-injecting sex worker populations in Eastern Europe. Journal of Urban Health, 83(Supplement 7), 6–15. doi:10.1007/s11524-006-9098-6.
Stromer, A., Tun, W., Guli, L., Harxhi, A., Bodanovskaia, Z., Yakovleva, A., et al. (2006). An analysis of respondent driven sampling with injection drug users (IDU) in Albania and the Russian Federation. Journal of Urban Health, 83(Supplement 1), 73–82. doi:10.1007/s11524-006-9105-y.
Stulhofer, A., Bacak, V., Bozicevic, I., & Begovac, J.(2007). HIV-related sexual risk taking among HIV-negative men who have sex with men in Zagreb, Croatia. AIDS and Behavior [Epub ahead of print].
Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19, 349–357. doi:10.1093/intqhc/mzm042.
UNAIDS and WHO. (2007). AIDS Epidemic Update: December 2007. Report UNAIDS/07.27E/JC1322E. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS.
UNAIDS/WHO Working Group on Global HIV/AIDS and STI Surveillance. (2000). Guidelines for Second Generation HIV Surveillance. Report UNAIDS/00.03E, WHO/CDS/CSR/EDC/2000.5. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS, World Health Organization.
Volz, E., Wejnert, C., Degani, I., & Heckathorn, D. D. (2007). Respondent-driven sampling analysis tool (RDSAT) version 5.6. Ithaca, NY: Cornell University.
Von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., Vandenbroucke, J. P., et al. (2007). The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet, 370, 1453–1457.
Wattana, W., van Griensven, F., Rhucharoenpornpanich, O., Manopaiboon, C., Thienkrua, W., Bannatham, R., et al. (2007). Respondent-driven sampling to assess characteristics and estimate the number of injection drug users in Bangkok, Thailand. Drug and Alcohol Dependence, 90, 228–233.
Watters, J. K., & Biernacki, P. (1989). Targeted sampling: Options for the study of hidden populations. Social Problems, 36, 416–430.
Yeka, W., Maibani-Michie, G., Prybylski, D., & Colby, D. (2006). Application of respondent driven sampling to collect baseline data on FSWs and MSM for HIV risk reduction interventions in two urban centres in Papua New Guinea. Journal of Urban Health, 83(Supplement 7), 60–72.
Zaba, B., Slaymaker, E., Urassa, M., & Boerma, J. T. (2006). The role of behavioral data in HIV surveillance. AIDS, 19(Supplement 2), S39–S52.
Acknowledgments
Disclaimer
The findings and conclusions in this paper are those of the authors and do not necessarily represent those of donor agencies. We would like to thank the individual investigators and organizations that generously shared their information with us or assisted in locating principal investigators (Appendix). We would like to extend our special gratitude to Family Health International; Centers for Disease Control and Prevention, Global AIDS Program; and the Eastern Mediterranean Regional Office of World Health Organization, which contributed to this project through sharing information from several studies.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Resources used for Tables 2–5
Reference number | Data sources | Principal investigator or contact person | Organization/contact information | Related documents |
|---|---|---|---|---|
1 | Co-author personal involvement, study protocol, personal communication | Valerio Bacak | Knowledge Hub for Capacity Building in HIV/AIDS Surveillance, Andrija Stampar School of Public Health, University of Zagreb, Croatia | Protocol: Procjena prevalence HIV-a, HCV-a, HBV-a, sifilisa i rizičnog ponašanja u populaciji intravenoznih korisnika droga u Sarajevu, Banja Luci i Zenici. (2007). UNICEF BiH |
2 | Personal communication | Anneli Uusküla | Department of Public Health, University of Tartu, Estonia | Uuskula, A., Kals, M., Rajaleid K., Abel K., Talu, A., et al. (2008) High-prevalence and high-estimated incidence of HIV infection among new injecting drug users in Estonia: need for large scale prevention programs. Journal of Public Health. Advance Access published Feb. 28, 2008. pp. 1–7 |
Platt et al. (2006) | ||||
3 | Personal communication, unpublished paper | Guy Morineau | Family Health International, Jakarta, Indonesia | Cambodian studies were reported in: Morineau, G., Pisani, E., Neal, J. J., and Saphonn, V. (2007). Respondent driven sampling of men who have sex with men in Cambodia: is the bang worth the buck? Unpublished paper |
MSM studies in 2007 were conducted under: “Dr. Sigit Priohutomo, Centers for Disease Controland Prevention, Ministry of Health (MOH), Government of Indonesia, # 29, Pecetakan Negara, Jakarta, Indonesia | ||||
4 | Co-author personal involvement, field notes, surveillance report | Mohammed J. Dahoma | Zanzibar AIDS Control Program, Ministry of Health and Social Welfare, Zanzibar, Tanzania | Protocol: Protocol for sampling sex workers, injection drug users and males who have sex with other males using respondent driven sampling in Zanzibar, Tanzania. (2007). Zanzibar, Tanzania: Zanzibar AIDS Control Programme, Ministry of Health and Social Welfare; Atlanta: Centers for Disease Control and Prevention, Global AIDS Program; New Orleans: Tulane University, School of Public Health and Tropical Medicine |
5 | Conference presentation, personal communication | Sherine Shawky | PI: Dr Nasr El Sayed Egyptian Ministry of Health and Population, Cairo, Egypt | Presentation: Behavioral and social sciences research on HIV/AIDS in the Middle East and North Africa. The Biological and Behavioral Surveillance Survey: The first round experience in Egypt (PowerPoint presentation). Tunis, Tunisia, May 1–3, 2007 |
Dr. Sherine Shawky: Social Research Center, American University, Cairo, Egypt | ||||
6 | Co-author personal involvement, personal communication | Ramesh Paranjap | National AIDS Research Institute, Bhosari, Pune, India | Protocol: Mapping, size estimation and integrated behavioral and biological assessment (IBBA) in high HIV prevalence settings in India. (2006) |
7 | Co-author personal involvement, field notes, study protocol | Mohsen Malekinejad | Iranian Research Center for HIV//AIDS (IRCHA), Tehran University of Medical Sciences, Tehran, Iran. Institute for Global Health, University of California, San Francisco, and University of California, Berkeley, School of Public Health, CA, USA | Protocol: HIV Prevalence and Risk Behavior among Injection Drug Users in Tehran, Iran. (2006). Eastern Mediterranean Regional Office of World Health organization. ID number: SGS06/67, EMRO/TDR Web Site: http://www.emro.who.int/tdr |
Malekinejad, M., Mohraz, M., Razai, N., Khairandish, P., McFarland, W., et al. (2008). Enhancing HIV surveillance capacity in Iran: Lessons learned from implementation of respondent-driven sampling (RDS) among injecting drug users. Unite For Sight, Fifth Annual International Health Conference, Building Global Health For Today and Tomorrow. Yale University, New Haven, Connecticut, USA. April 12–13, 2008 | ||||
8 | Personal communication, final report | Olga Balakireva | Ukrainian Institute for Social Research, Kiev, Ukraine | Protocol: Risk and protective factors in the initiation of injecting drug use: report of a respondent driven sampling study and strategy paper on preventing the initiation of injecting drug use among vulnerable adolescents and young people. (2006). Olexander Yaremenko Unkranian Institute for Social Research, Kiev, Ukraine |
9 | Personal communication | Vivian Hope | London School of Hygiene and Tropical Medicine, UK Matthew Hickman, University of Bristol, UK | |
10 | Surveillance report, personal communication | Roland Bani | National AIDS Program, Tirana, Albania | The Implementing AIDS Prevention and Care Project (IMPACT). (2005). 2005 Albania Behavioral and Biological Surveillance Study Report. I. Arlington, VA: Family Health International. Available at: http://www.fhi.org/en/HIVAIDS/pub/survreports/res_BioBSS_Albania2005.htm. Access date: November 29, 2007 |
Stromer et al. (2006) | ||||
11 | Published paper | Simon D. Frost | Department of Pathology and Antiviral Research Center, University of California, San Diego, CA, USA | Frost et al. (2006) |
Pollini, R.A., Brouwer, C.B., Lozada, R.M., Ramos, R., Cruz, M.F. (2008) Syringe possession arrests are associated with receptive syringe sharing in two Mexico–US border cities. Addiction. 103: 101–108 | ||||
12 | Co-author personal involvement, personal communication, published paper, protocol | Lucy Platt, Tim Rhodes | Centre for Research on Drugs and Health Behavior, Department of Public Health and Policy, London School of Hygiene and Tropical Medicine, London, UK | |
Tkatchenko-Schmidt, E. (2006). Knowledge for Action in HIV/AIDS in the Russian Federation. London: Institute for Health and Human Development, University of East London. Available at: http://www.uel.ac.uk/ihhd/programmes/RussiaKP.htm. Access date: November 29, 2007 | ||||
13 | Personal communication, personal notes, brief conference abstract | Laxmi Bilas Acharya | Family Health International, Katmandu, Nepal | Acharya, L.B., Dhungel, N., and Ross, J.L. (2004). Factors associated to HIV prevalence among male IDUs in the Eastern Terai of Nepal? [Abstract C11318]. International AIDS Conference, Bangkok, Thailand, July 11–16, 2004 |
14 | Zinaida Bodanovskaia | St-Petersburg Non-Governmental Organization of Social Projects “Stellit”, St. Petersburg, Russia | Stromer et al. (2006) | |
15 | Surveillance report | Trinh Quan Huan | Ministry of Health. Hanoi, Vietnam | Ministry of Health. (2006). Results from the HIV/STI Integrated Biological and Behavioral Surveillance (IBBS) in Vietnam 2005–2006. Hanoi, Vietnam: National Institute of Hygiene and Epidemiology; Arlington, VA: Family Health International |
16 | Published paper | Wantanee Wattana | Bangkok Metropolitan Administration, Bangkok, Thailand | Wattana et al. (2007) |
17 | Co-author personal involvement, final report | Aire Trummal | National Institute for Health Development, Tallinn, Estonia | Final report: Trummal, A., Johnston, L.G., & Lõhmus L. (2007). Men having sex with men in Tallinn: pilot study using respondent driven sampling. Final study report. National Institute for Health Development. Tallinn, Estonia |
18 | Co-author personal involvement, field notes, published paper | Tasnim Azim | HIV/AIDS Programme, ICDDR,B, Dhaka, Bangladesh | Johnston et al. (2007) |
19 | Personal communication and published paper | Jinkou Zhao | Centers for Disease Control and Prevention Global AIDS Program, Beijing, China. Also, Dr. Willi McFarland at San Francisco Department of Public Health, San Francisco, CA, USA | Ma et al. (2007) |
20 | Co-author personal involvement, personal communication | Ivana Bozicevic | Andrija Stampar School of Public Health, University of Zagreb, Zagreb, Croatia | Bozicevic et al. (2008) |
Stulhofer et al. (2007) | ||||
21 | Co-author personal involvement, personal communication, final report | Morales-Miranda Sonia | Centers for Disease Control and Prevention, Global AIDS Program, Office for Central America and Panama, Guatemala City, Guatemala | Reporte final: Estudio centroamericano de vigilancia de comportamiento sexual y prevalencia de VIH/ITS en poblaciones vulnerables: hombres que tienen sexo con hombres. (2007). Guatemala City, Guatemala: Centers for Disease Control and Prevention, Global AIDS Program, Office for Central America and Panama |
22 | Personal communication | Chinaglia, MLM, Reprolatina Solucoes Inovadoras em Saude | ||
Sexual e Reprodutiva Rua Maria Tereza da Silva, 740, Campinas 13083–820 Brazil | ||||
23 | Personal communication, final report | Edona Deva | Bio-BSS Principal Investigator and Kosovo AIDS Committee, Ministry of Health, Pristina, Kosovo, Serbia | The Implementing AIDS Prevention and Care Project (IMPACT). (2006). Behavioral and Biological Surveillance Study Kosovo, February 2006–July 2006. Arlington, VA: Family Health International. Available at: http://www.fhi.org/en/HIVAIDS/pub/res_IMPACT+Kosovo+Final+Report.htm. Access date: November 29, 2007 |
24 | Personal communication, study protocol (Campinas, Brazil) | Maeve Mello | Oswaldo Cruz Foundation – FIOCRUZ, Rio de Janeiro, Brazil; Programa Nacional de DST/Aids, Brasilia, Brazil; Centers for Disease Control and Prevention, Global AIDS Program, Brasilia, Brazil | Protocol: Risk factors for HIV infection in the MSM and transgender populations in theMetropolitan Area of Campinas city, Brazil, using Respondent-Driven Sampling (Sept 2005–Feb 2007) |
25 | Co-authors personal involvement, field notes, unpublished paper | Ligia Regina Franco Sansigolo Kerr | Federal University of Ceará, Medical School, Fortaleza, Brazil; Programa Nacional de DST/Aids, Brasilia, Brazil; Centers for Disease Control and Prevention, Global AIDS Program, Brasilia, Brazil | Kendall, C., Kerr, L.R.F.S., Gondim, R.C., Werneck, G.L., Hermelinda, R. ., et al. (2007). An empirical comparison of respondent-driven sampling, time location sampling, and snowball sampling for behavioral surveillance in men who have sex with men, Fortaleza, Brazil. Unpublished paper |
26 | Published paper, personal communication | Geraldine Maibani | Papua New Guinea Institute of Medical Research, Goroka, Papua New Guinea | Yeka et al. (2006) |
27 | Co-author personal involvement, published paper | Willi McFarland | San Francisco Department of Public Health, San Francisco, CA, USA | Kajubi et al. (2007) |
28 | Personal communication | Cíntia Germany | Centro de Estudos de Aids/DST do Rio Grande do Sul, Porto Alegre, Brazil; Programa Nacional de DST/Aids, Brasilia, Brazil; Centers for Disease Control and Prevention, Global AIDS Program, Brasilia, Brazil | |
29 | Personal communication | Neide Gravato da Silva | Associação Santista de Pesquisa Prevenção e Educação em DST/Aids, São Paulo, Brazil; Programa Nacional de DST/Aids, Brasilia, Brazil; Centers for Disease Control and Prevention, Global AIDS Program, Brasilia, Brazil | |
30 | Co-author personal involvement, field notes, unpublished and published papers, conference abstract (IDU, 2004) | Luu Thi Minh Chau | Ministry of Health, Hanoi, Vietnam, and Centers for Disease Control and Prevention, Global AIDS Program, Hanoi, Vietnam | Johnston et al. (2006) |
Johnston, L.G., Huong. P.T., Hien M.T., Chau L.M., Hau D.H. HIV prevalence and risk factors among injecting drug users in Ho Chi Minh City, Vietnam. 16th Annual International Conference for the reduction of Harm among Injecting Drug Users. Abstract 910, p. 111 March, 2005. Belfast, Ireland | ||||
31 | Co-author personal involvement, field notes, unpublished paper | Mickey Chopra | Medical Research Council, Cape Town, South Africa | Johnston, L.G., O’Bra, H., Chopra, Mathews, C., Townsend, L., Sabin, K.,Tomlinson M., Kendall, C. (2008). The associations of HIV risk perception and voluntary counseling and testing acceptance to HIV status and risk behaviors among men with multiple sex partners in a South African township. AIDS and Behavior [in press] |
Chopra et al. (2007) |
Rights and permissions
About this article
Cite this article
Malekinejad, M., Johnston, L.G., Kendall, C. et al. Using Respondent-Driven Sampling Methodology for HIV Biological and Behavioral Surveillance in International Settings: A Systematic Review. AIDS Behav 12 (Suppl 1), 105–130 (2008). https://doi.org/10.1007/s10461-008-9421-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-008-9421-1