
Abstract
Muscle structure is an essential component in typical computational models of the musculoskeletal system. Almost all musculoskeletal models represent muscle geometry using a set of line segments. The straight-line approach limits models’ ability to accurately predict the paths of muscles with complex geometry. This approach needs knowledge of how the muscle changes shape and interacts with fundamental structures like muscles, bones, and joints that move. Moreover, the moment arms are supposed to be equivalent to all the fibers in the muscle. This study aims to create a shoulder musculoskeletal model that includes complex muscle geometries. We reconstructed the shape of fibers in the entire volume of six muscles adjacent to the shoulder using an automated technique. This method generates many fibers from the surface geometry of the skeletal muscle and its attachment areas. Highly discretized muscle representations for all muscles were created and used to simulate different shoulder movements. The moment arms of each muscle were calculated and validated against cadaveric measurements and models of the same muscles from the literature. We found that simulations using the developed musculoskeletal models generated more realistic geometries, which expands the physical representation of muscles compared to line segments. The shoulder musculoskeletal model with complex muscle geometry is created to increase the anatomical reality of models and the lines action of muscle fibers, and to be used for finite element investigations.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Computational models of the musculoskeletal (MSK) system provide a framework for integrating anatomic and physiological data, allowing many applications in neuromuscular control. A variety of MSK models of the shoulder [3, 6, 12, 19, 29, 30] have been developed and used for differing studies in recent years. These models typically represent muscles with a set of lines. The straight-lines approach has the primary advantage of being simple to simulate and computationally efficient. However, limitations of straight-line models have been frequently reported due to the fiber arrangements of muscles [9, 10], the volumetric penetrations [11] with bones and other muscles, and their inability to correctly capture the moment arms [26, 39]. The last one is an important determinant of the muscle’s functioning during skeletal motion, because it determines the leverage that a muscle has on a joint, and this in turn affects the muscle’s ability to produce joint torque [20]. The two most important design considerations when modeling muscles using a series of line segments in multibody models are (1) the geometrical complexity which is determined by the number of straight-line segments constituting the line of action and the wrapping surfaces [4], that define the geometrical constraint of the path from penetrating underlying bones and muscles, and (2) the level of muscle discretization of each of these fiber paths [24], which means the number of fibers included in the muscle representation.
According to previous studies, a single line of action is generally insufficient to represent the geometry of muscles that have broad attachments and complex fiber arrangements, such as the shoulder muscles [37]. Multiple lines of action are recommended. However, this approximation makes model creation difficult because one must decide how many lines of action to use, and where to place the insertion, origin, and path (geometrical constraints) of each line of action [37]. In addition, specifying these constraints is difficult because it requires the knowledge of how muscles deform in three dimensions and the muscle moment arms can be highly sensitive to how the constraints are defined [4]. The high muscle discretization level is required to accurately estimate muscle moment arms [4, 24, 37], muscle forces [41], and joint contact [23, 38] forces.
Several methods have been developed in the literature to provide a realistic anatomical representation of skeletal muscles. Blemker and Delp [4] created a finite element model of the hip muscles using surface meshes to map templates of fiber architectures. The muscle geometries were segmented using magnetic resonance imaging (MRI) scans, and the shape deformations predicted by their model were validated against additional segmentation of MRI scans for multiple hip joint positions. In their investigation, lengths and moment arms for fiber paths could be determined, but the results were not applied in a multibody MSK model. Webb et al. [37] used this technique to create 3D finite element models of the deltoid and rotator cuff muscles and tendons to study how moment arms varied across the fibers within each muscle and compared the 3D models with line-segment representations. Kohout et al. [14,15,16] developed a method of muscle decomposition into an arbitrary number of fibers and employed it to create a walking simulation proposed as a visual help for clinicians, but did not provide any quantity of biomechanical interest. Modenese and Kohout [24] proposed an automated technique that, based on the surface geometry of a skeletal muscle and its attachment areas, can construct multiple lines of action (fibers) composed of several straight-line segments. They applied this methodology to the surfaces of four muscles that support the hip joint, which were segmented using magnetic resonance imaging scans from a cadaveric dataset and for which highly discretized muscle representations were constructed and used for simulating functional tasks.
Based on the technique presented in the works of Kohout and Cholt [14] and Modenese and Kohout [24], and the scapular kinematics described by Seth et al. [33], the purpose of this paper is to create a MSK model of the shoulder with a scapulothoracic joint that represents complex muscle geometry. The first step is to develop a biomechanical model of the shoulder with a scapulothoracic joint using NMSBuilder software [35] and the plugin of the scapulothoracic joint in OpenSim software [7, 32]. This model was used to evaluate the accuracy of the shoulder kinematics from the model against bone-pin data measured during the shoulder abduction task in the scapular plane (Scaption) and the flexion task in the sagittal plane. The second step is to generate muscle fibers based on surface meshes. For each surface mesh, the principal inputs like the attachment areas of the muscle with bones (origin & insertion) and the artificial fibers were prepared first. This method can generate an arbitrary number of fibers comprised of a specified number of straight-line segments that can be used as musculotendon actuators in MSK models and biomechanical analyses. The last step is to develop a MSK model with the fibrous muscle created in the second step using the application programming interface (API) of OpenSim from MATLAB after solving the kinematics of the produced fibers. The moment arms produced by the model developed in this study are compared with prior investigations: the in-vitro studies [1, 17, 18], the straight-lines model of Holzbaur et al. [12], and the validated finite element models [28, 37].
Materials and Methods
Shoulder Skeletal Model
To create our shoulder model, we used the dataset BodyParts3D (The Database Center for Life Science, Japan). This dataset contains surface meshes representing muscles, bones, and other structures. The surface meshes of bones and muscles were performed in MeshLab using smoothing and decimation processes to improve the mesh’s poor quality (e.g., non-manifold edges, duplicated vertices, and degenerate triangles).
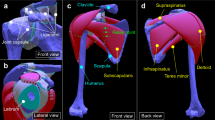
The skeletal model of the shoulder was created using NMSBuilder [35], specifically designed to support the rapid development of computer-aided medical applications integrated with dedicated simulation (OpenSim). The geometries of the upper extremity were used to construct the skeletal model, which includes (1) Four rigid bodies: the thorax, clavicle, scapula, and humerus. The inertial properties were calculated for each body segment using NMSBuilder [35], assigning different densities to bones (1.42 g/cm3) and soft tissue (1.03 g/cm3). (2) The anatomical landmarks and joint reference systems were created following the International Society of Biomechanics (ISB) recommendations [40] (Fig. 1). (3) Four joints: The defined sets of landmark clouds were used to generate the joint reference systems as anatomical reference systems. According to the ISB recommendations [40], two reference systems were automatically produced per joint, whose location and orientation were determined for the reference systems of the parent body and the child body, respectively [35]. The sternoclavicular joint was defined as a ball joint type, which enables protraction–retraction, and elevation–depression of the clavicle since axial rotation cannot be accurately measured because of the conoid ligament that limits this movement. The glenohumeral joint was defined as a custom gimbal joint, which was specified by the following coordinates: elevation plane angle, elevation, and internal rotation. The acromioclavicular joint was modeled as a ball joint by the constraint point AC (Acromioclavicular Joint) [40]. Finally, the scapulothoracic joint was defined by the translation and rotation of the scapula on the thoracic surface, which was modeled as an ellipsoid [34] (Fig. 1). This joint was specified by four coordinates: abduction–adduction, elevation–depression, upward rotation, and internal rotation or “winging” [34]. The origin of the joint frame on the thorax was defined by the center of the ellipsoid, and the origin of the joint frame on the scapula was specified as the centroid of the Angulus Acromialis (AA), Trigonum Spinae (TS), and Angulus Inferior (AI) markers. These anatomical landmarks and the joint frame orientation were recommended by the ISB [40]. However, the scapulothoracic joint frame was rotated -90° about the scapular Y-axis to define upward rotation as a positive rotation about the scapulothoracic joint frame’s Z-axis. The scapulothoracic joint was defined using the available plugin of the scapulothoracic joint in OpenSim software [7, 32] developed by Seth et al. [33]

a Thorax, clavicle, scapula, and humerus joint reference systems. b Scapulothoracic joint definition
Evaluation of Shoulder Kinematics
The purpose of inverse kinematics is to compute the coordinates (joint angles) of the scaled model that best reproduces the experimental kinematics. The inverse kinematics tool in OpenSim goes through each captured motion and quantifies the set of joint angles that place the model in a configuration that “best matches” the experimental kinematics. Bones and related joint locations were scaled linearly based on the distance between the subject and the generic model. The ellipsoid surface of the thorax in the scapulothoracic joint was scaled by optimizing the geometric parameters of the ellipsoid to reduce marker-tracking errors [31]. Comparing the model’s marker placements to measured marker data from bone-pin motion-capture experiments of Ludewig et al. [22] allowed us to assess the kinematic accuracy of the model’s joints. We calculated the root-mean-squared (RMS) errors for each marker across each trial. They measured marker locations with magnetic sensors mounted to different parts of the upper limb for different tasks: arm flexion, arm abduction, and arm rotation.
Shoulder Musculoskeletal Model with Straight-Lines Muscle Representations
The MSK model with straight-line muscles was created using the skeletal model representing the scapulothoracic joint. The muscle paths and architecture, including wrapping surfaces, were defined using the straight-line muscle representation of the model created by Seth et al. [31] as a reference.
Shoulder Musculoskeletal Model with Complex Muscle Geometries
The MSK model with highly discretized muscles was created by passing through three stages: (1) Muscle geometry decomposition was the first stage for generating a set of muscle fibers using the method described by Kohout and Cholt [14] and Modenese and Kohout [24]; (2) a fiber kinematics stage for solving the kinematics of the produced fibers; (3) the last stage was to define the force set to the skeletal model using OpenSim’s application programming interface (API) from MATLAB.
Muscle Geometry Decomposition
We applied the described automatic algorithm for the muscle geometry decomposition presented in the works of Kohout and Cholt [14] and Modenese and Kohout [24]. The essential inputs of this method (Fig. 2) are (1) a triangular surface mesh representing the muscle geometry; (2) the attachment areas of the muscle (insertion and origin), defined as a triangular surface mesh and a set of landmarks fixed on the bone; and (3) an artificial fiber giving geometrical information about the internal fiber arrangement of the muscle. The triangular surfaces of muscles were performed in MeshLab because the bad quality of the mesh affected the decomposition results, and the attachment areas were created in MeshLab by selecting faces from bones. Then, the sets of landmarks were created by selecting points from the outline of the attachment areas. Lastly, the artificial fibers were constructed in NMSBuilder [35] by creating a set of landmarks according to illustrations in anatomical atlases.

The required inputs of the automated muscle decomposition method
All inputs were transformed into Visualization Toolkit (VTK) files. The method started with a cubic spline interpolating of the artificial fibers to create the fibers on the muscle surface. Muscle thickness was determined, and the fibers in deep layers were reconstructed by linear extrapolating of those on the surface. All the fibers were linked to muscle attachment areas and refined to get the final smooth fibers. The user can customize the muscle geometry decomposition from this workflow by choosing the number of fibers between the artificial fibers, the number of fibers in deep layers, and straight-line segments per fiber. The surface meshes of muscles were decomposed into highly discretized models using a C++ implementation of the automatic algorithm for muscle decomposition [14]. The artificial fibers were specified according to illustrations in anatomical atlases. The inputs for specifying the number of created fibers were determined by trial and error, aiming to make a realistic shape with an optimal number of fibers. However, the shape of the realistic fibers needs an important number of line segments and fibers. A visualization of created muscles and an atlas of human anatomy were compared to see how good an estimation of real muscle architecture was.
Fiber Kinematics
The kinematics of the produced fibers was solved by using an algorithm based on binding the points of the fibers to the bones. Every fiber point i was related to its two adjacent bones, and the transformed positions were blended to give the new position of the point. The new position V’i could be computed as a linear combination of the transformations of its rest pose position Vi concerning these bones [25]:
where n is the number of points in the fibers, wij is the blending weights for determining the bone influence, Mj denotes the transformation matrix associated with the jth nearest bone-in, and Mj−1 is the inverse of the transformation matrix associated with the jth influencing bone. The weights wij in this study were computed from the relative position t = (i − 1)/(n − 1) of the ith fiber point Vi on the fiber (measured from the fiber origin V1) using a quadratic function f(t) [24]:
where a, b, and c are muscle-specific parameters that determine how quickly the influence of an attachment bone diminishes along the fiber length [24]. The first and the last fiber point positions were ruled by bones only, i.e., f(0) = 1 and f(1) = 0, indicating that c = 1 and b = −a − 1, thus leading to a formula with just one muscle-specific parameter a to specify. The value of parameter a was determined by experimenting with different values for each muscle, to minimize the muscle–bone penetrations [24].
Creation of the Force Set of the Shoulder Musculoskeletal Model
The MSK model with highly discretized muscles was created by adding the ForceSet to the skeletal model using the API of OpenSim from MATLAB. The type of muscle path actuator used is Thelen2003Muscle [13], with the GeometryPath as MovingPathPoints. The element of this latter contains the path points that move within a body’s reference frame as a function of a generalized coordinate. The MovingPathPoint’s x_location, y_location, and z_location were defined as LinearFunction which maps the value of the generalized coordinate to the XYZ value of the path point’s location in its owner’s body. The shoulder MSK model developed is shown in Fig. 3.

Shoulder musculoskeletal model with high discretization muscles. a Anterior view, b lateral view, and c posterior view
Computing and Validation of Muscle Moment Arms
Simulations of different shoulder tasks were generated using both models. We simulated the same two motion patterns, abduction, and internal-to-external rotation, as reported in the research of Webb et al. [37] The abduction was simulated in the frontal plane by imposing the kinematics on the glenohumeral joint for angles ranging from 0° to 60°, which is equivalent to a thoracohumeral abduction of 0° to 90°: the resulting moment arms were scaled by 2/3 to transform them from a glenohumeral angle to a thoracohumeral using the ratio reported in Inman et al. [36]. The rotation was simulated from –45°(internal) to 45°(external). In addition, the abduction and flexion were simulated in the scapular and sagittal planes, respectively, by imposing the kinematics result presented in “Shoulder Musculoskeletal Model with Straight-Lines Muscle Representations” section on the glenohumeral joint, for angles ranging from 0° to 80°, which is equivalent to a thoracohumeral abduction of 0° to 120°.
The moment arms of both models were calculated. For the model with straight-lines muscles, we used Muscle Analysis (MA) tool in OpenSim 4.1 to compute the moment arms for all shoulder tasks previously presented. The tendon excursion method [2] was used to calculate the moment arms of the model with highly discretized muscles as expressed in Eq. (3).
where li is the length of the ith fiber for the jth coordinate θj. Then, the length l of each fiber was calculated using the same API, interpolated with a 4th-order polynomial function, and used to determine the moment arm MAij.
In designing and validating computational models, it is very important to compare the results of the developed models with experimental measurements. Indeed, we compared our obtained moment arms at each shoulder joint motion with the cadaveric measurements that Ackland et al. [1] determined and the in-vitro study presented by Kuechle et al. [17, 18] Additionally, we compared the moment arms calculated using the developed model with results of the validated finite element (FE) models [28, 37]. The first one presents the FE shoulder model of Webb et al. [37], which itself was compared with a numerical model [12] as well as in-vitro measurements of Otis et al. [27], and Liu et al. [21]. The second one represents the volumetric and extensive finite element model of Péan et al. [28] Our results were also compared with the developed model with straight-lines muscles and data available from the previous literature [12].
The obtained results from the preceding literature were digitized from published graphs using Graph Grabber v2.0 (https://www.quintessa.org). For each shoulder task, we calculated the percentage of poses for which previously reported moment arm values were within the range of moment arm values estimated by our model. This percentage was computed for each previous study. For the model of Webb et al. [37], the percentage of poses were defined by the intersection between the area outlined by results from Webb et al. [37] (AB) and the area outlined by the highly discretized moment arms results (AA), as expressed in Eq. (4).
Concerning the other models and cadaveric measurements, we calculated the percentage of poses using the following equation:
For each previous study, we interpolated the digitized graphs using a 4th-order polynomial function, and then discretized the range of motion into NT frames using a multiplicator of 5. Additionally, the number Nt is not fixed value but changes depending on the simulated motions being studied. NP_Out represents the number of the points that are not within the range estimated by our model. Regarding muscles that present multiple lines of action, the percentage of poses was averaged across the number of fibers k that represent the muscle (see Appendix 3—Supplementary Materials).
The criteria used for comparing the moment arms estimated by our model with those reported in the other investigations included the computed percentages of poses, the muscle roles in joint actuation determined by the sign of the moment arms, and the magnitude of the moment arms representing the muscle leverage about a joint. The comparison was considered excellent if the percentage of poses was greater than 80%, good if the percentage of poses was between 50% and 80% with similarity in trend and actions, and poor if the percentage of poses was less than 50% with differences in trend and actions.
Peaks (minimum and maximum) and mean values with standard deviations of moment arms obtained across the entire range of motion from our model, together with those from the straight-line muscles and estimation from the results available from previous literature, were reported for each shoulder task. The mean value of each muscle was defined as the mean of values that represented the mean of the moment arms for each frame. However, the mean values for Webb et al. [37] were computed using the digitized upper and lower boundaries of the results.
Results
The results obtainable from the preceding simulations were performed in a Lenovo Workstation (RAM: 64 GB, CPU: 2 Intel Xeon E5-2660 v4 2.00 GHz).
The evaluation of the shoulder kinematics with the developed model is presented in Appendix 2 in Supplementary materials.
Overall, the geometry of the deltoid muscles (anterior deltoid, middle deltoid, posterior deltoid) was visually accurate. The simulations of the rotator cuff muscle (supraspinatus, infraspinatus, teres minor, and subscapularis) and the teres major also generated visually satisfactory geometries, except for the scaption angles, for which some fibers, especially of the subscapularis, were penetrating the humeral ridge geometry.
Comparison to Cadaveric Measurements
The comparison shows an excellent agreement between the moment arms of the deltoid muscles in our model and those in the in-vitro studies [1] during shoulder movements (Figs. 4, 5, 6, 7).

Results of the simulations of the shoulder abduction in the frontal plane. The moment arms calculated (colored lines) are compared to the moment arms obtained from the model with straight-line muscles and other research from the literature (see legend)

Results of the simulations of the shoulder rotation in the natural position. The moment arms calculated (colored lines) are compared to the moment arms obtained from the model with straight-line muscles and other research from the literature (see legend)

Results of the simulations of the shoulder abduction in the scapular plane. The moment arms calculated (colored lines) are compared to the moment arms obtained from the model with straight-line muscles and other research from the literature (see legend)

Results of the simulations of the shoulder flexion in the sagittal plane. The moment arms calculated (colored lines) are compared to the moment arms obtained from the model with straight-line muscles and other research from the literature (see legend)
On average, deltoid scaption and flexion moment arms estimated by our model were within the moment arms reported in the in-vitro study of Ackland et al. [1] in 87% of the shoulder joint poses for the anterior deltoid, 98% for the middle deltoid, and 100% for the posterior deltoid. The action of the deltoid muscles is similar all over the shoulder scaption and flexion. For the rotator muscles and the teres major, scaption and flexion moment arms of the highly discretized model were consistent with those from Ackland et al. [1] study as presented in Figs. 6 and 7. There is a similarity in amplitude and magnitude between the moment arms of these muscles.
The comparison with the in-vitro studies of Kuechle et al. [17, 18] suggested a remarkable similarity of the estimated moment arms (A-Deltoid: 73%, M-Deltoid: 96%, P-Deltoid: 72%, T-Maj: 85%). Except for the rotator muscles, some differences were shown in the moment arms magnitudes, leading to a lower level of agreement (Infra: 33%, Supra: 32%, Subsc: 35%, T-Min: 36%) (Table 1). However, we observed a similarity in trend and actions which are represented by the sign of the moment arms, all these remain in agreement with models and the in-vitro studies of Kuechle et al. [17, 18].
Comparison to Validated Finite Element Models
Moment arms of the developed model were in good agreement with those from the FE model of Webb et al. [37], especially for the deltoid muscles when simulating abduction in the frontal plane (Fig. 4). During this movement, the mean percentage of pose for the deltoid muscles is 70%. Some differences in trends were observed for rotation angles in the natural position for the deltoid muscles (Fig. 5). The mean percentages of the area outlined by the results from Webb et al. [37] that is overlapping with the area outlined by the highly discretized moment arms results are 58% for the anterior deltoid, 46% for the middle deltoid, and 54% for the posterior deltoid. For the rotator muscles, the moment arms of the supraspinatus, infraspinatus, and subscapularis all follow the trend of the moment arms from the FE model of Webb et al. [37] with some differences in values (Supra: 39%, Infra: 43%, Subsc: 22%). However, the teres minor moment arms had a good agreement with on average in 64% of the considered poses (Table 1).
Compared to Péan et al. [28], the moment arms of the deltoid muscles for different shoulder movements agreed well with the range estimated by our developed model (A-Deltoid: 68%, M-Deltoid: 66%, P-Deltoid: 91%). However, it is clear from Fig. 6 that the middle deltoid moment arms revealed a difference in trend for scaption angles characterized by 4% of pose agreement. Concerning the rotator muscles, the moment arms of the supraspinatus, infraspinatus, and teres minor all follow the trend of the moment arms from the FE model of Péan et al. [28] for scaption angles (Fig. 6). However, the subscapularis showed more fluctuations. Some differences in trends and values were observed for abduction and rotation angles. But, their actions, represented by the sign of the moment arms, remain in agreement with the FE model.
Comparison to Straight-Lines Models
Through shoulder abduction in the frontal plane, moment arms of the highly discretized muscles were in strong agreement with those from the line-segment model of Holzbaur et al. [12] All moment arms were similar in trend and values, except, the subscapularis and the supraspinatus which had some differences in amplitude as presented in Fig. 4. During shoulder rotation, our results revealed less agreement with those of the line-segment model of Holzbaur et al. [12] Except, the anterior deltoid and the teres minor were within the range estimated by our model. The other muscles showed differences in trends and values.
On average, the comparison with the moment arms from the straight-lines muscles model indicates that these latter were within the range estimated by the highly discretized muscles in 65% of the shoulder joint poses for the anterior deltoid, 54% for the middle deltoid, and 81% for the posterior deltoid. Concerning the rotator muscles, the moment arms are different in values and trends (Supra: 27%, Infra: 25%, Subsc: 14%, T-Min: 70%) (Table 1). However, there was an excellent agreement between the results of the teres major with 91% of the considered poses.
The peaks and mean values with standard deviations of moment arms calculated throughout the shoulder tasks for our models, the straight-lines muscles model, and the results obtained from previous studies are reported in Tables 2 and 3.
Discussion
The objective of the present study was to create a shoulder MSK model representing complex three-dimensional skeletal muscles. The developed model eliminates the usual duality of the straight-lines model which has some difficulty for more geometrically complex muscle representations. This is difficult due to many parameters such as the number of the line of the action to use, the placement of the origin, the insertion, and the path of via points. To evaluate the developed model, we generated simulations of different shoulder tasks and compared the computed moment arms for shoulder muscles against cadaveric measurements, validated finite element models, and models that used the straight-lines approach for muscle modeling. We found good agreement, especially for the deltoid muscles, teres minor, and teres major. We obtained poor agreement for supraspinatus, infraspinatus, and subscapularis; however, their actions were in line with the other investigations.
Our comparisons to the 3D finite element models of Webb et al. [37] and Péan et al. [28] confirmed the main finding of these investigations that a single muscle has many actions across a motion, which is particularly evident in the anterior deltoid and posterior deltoid, and the muscle deformations influence the results. Our model reinforces both these findings: The moment arms obtained with the straight-lines models changed more with joint rotation than moment arms determined with the 3D models, which are very clear in the case of the shoulder rotation in the natural position. Our results show that the action of the infraspinatus, supraspinatus, subscapularis, and teres minor are in line with the 3D finite element models.
Compared to the experimental measurements, our findings are of the same order of magnitude and amplitude as those of Ackland et al. [1]. However, compared to Kuechle et al. [17, 18], there are similarities in magnitude with some differences in the amplitude, particularly for infraspinatus, subscapularis, and the posterior deltoid in the shoulder rotation task and supraspinatus and subscapularis for the shoulder abduction in the frontal plane. This is explained by the fact that moment arm computations are affected by the subject size and the location of tendon attachment sites.
We used the dataset BodyParts3D, which presents image data from a healthy adult human male, to develop a representative model of a normal and healthy shoulder. Previous shoulder models have been developed from either cadaveric information [12], the visible human project [5, 8], or from healthy subject [28, 37]. The referenced investigations are very different in terms of mean age and average size. In addition, cadaveric specimens frequently have atrophied. Therefore, we might assume that some of the differences between our results and the other studies would be because of those different subject populations.
The shoulder three-dimensional MSK model ignores features such as the presence of fascia or inter-muscle collisions that might increase the accuracy of the moment arms prediction. Overall, the moments arms produced by the models developed in this study were within the range of the values in literature. There were differences between the output of our new model and the literature values, both in terms of magnitude and trends of moment arms for some muscles. We believe that the presented deviation may be explained by the use of different subject populations, as we discussed earlier.
This study has several modeling limitations. First of all, the muscle decomposition stage presents a visualized comparison of created muscles and an atlas of human anatomy to see how good the estimation of real muscle architecture was. Secondly, the prepared inputs like the attachment areas used for generating highly discretization muscles have created the intersection between the bone and muscle of the dataset BodyParts3D, however, they can be estimated using statistical shape approaches or mapped from existing atlases datasets.
Future investigations will integrate the other muscles which contribute to shoulder movement, then will investigate the evaluation of the muscular forces. The latter will be used in finite element studies.
Conclusion
We have presented a MSK model of the shoulder that represents three-dimensional muscle geometries. The model includes the skeletal system of the upper limb with the deltoid muscles and the rotator cuff muscles with complex geometry. The developed model expands the physical representation of muscles compared to line segments by simulating the volumetric structures for many shoulder tasks. We believe that the developed model could benefit various applications in biomechanics, especially for finite element investigations.
References
Ackland, D. C., P. Pak, M. Richardson, and M. G. Pandy. Moment arms of the muscles crossing the anatomical shoulder. J. Anat. 213(4):383–390, 2008.
An, K. N., K. Takahashi, T. P. Harrigan, and E. Y. Chao. Determination of muscle orientations and moment arms. J. Biomech. Eng. 106:280–282, 1984.
Assila, N., S. Duprey, and M. Begon. Glenohumeral joint and muscles functions during a lifting task. J. Biomech. 126:110641, 2021.
Blemker, S. S., and S. L. Delp. Three-dimensional representation of complex muscle architectures and geometries. Ann. Biomed. Eng. 33:661–673, 2005.
Charlton, I. W., and G. R. Johnson. A model for the prediction of the forces at the glenohumeral joint. Inst. Mech. Eng. H. 220:801–812, 2015.
Damsgaard, M., J. Rasmussen, S. T. Christensen, E. Surma, and M. de Zee. Analysis of musculoskeletal systems in the AnyBody Modeling System. Simul. Model. Pract. Theory. 14:1100–1111, 2006.
Delp, S. L., F. C. Anderson, A. S. Arnold, P. Loan, A. Habib, C. T. John, E. Guendelman, and D. G. Thelen. OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 54:1940–1950, 2007.
Garner, B. A., and M. G. Pandy. A kinematic model of the upper limb based on the visible human project (VHP) image dataset. Comput. Methods Biomech. Biomed. Eng. 2:107–124, 1999.
Garner, B. A., and M. G. Pandy. The obstacle-set method for representing muscle paths in musculoskeletal models. Comput. Methods Biomech. Biomed. Eng. 3:1–30, 2000.
Hawkins, D., and A. Barr. A computational approach for simulating muscle morphologic changes in musculoskeletal modeling. Comput. Methods Biomech. Biomed. Eng. 4:399–411, 2001.
Hoffmann, M., D. Haering, and M. Begon. Comparison between line and surface mesh models to represent the rotator cuff muscle geometry in musculoskeletal models. Comput. Methods Biomech. Biomed. Eng. 20:1175–1181, 2017.
Holzbaur, K. R. S., W. M. Murray, and S. L. Delp. A model of the upper extremity for simulating musculoskeletal surgery and analyzing neuromuscular control. Ann. Biomed Eng. 33:829–840, 2005.
John, C. T. Complete Description of the Thelen2003Muscle Model. Stanford: OpenSim, 2011.
Kohout, J., and D. Cholt. Computer Methods and Programs in Biomedicine Automatic reconstruction of the muscle architecture from the superficial layer fibres data. Comput. Methods Programs Biomed. 150:85–95, 2017.
Kohout, J., G. J. Clapworthy, Y. Zhao, Y. Tao, F. Dong, H. Wei, and E. Kohoutova. Patient-specific fibre-based models of muscle wrapping. Interface Focus. 3:20120062, 2013.
Kohout, J., and M. Kukačka. Real-time modelling of fibrous muscle. Comput. Graph. Forum. 33:1–15, 2014.
Kuechle, D. K., S. R. Newman, E. Itoi, B. F. Morrey, and K. N. An. Shoulder muscle moment arms during horizontal flexion and elevation. J. Shoulder Elbow Surg. 6(5):429–439, 1997.
Kuechle, D. K., S. R. Newman, E. Itoi, G. L. Niebur, B. F. Morrey, and K. N. An. The relevance of the moment arm of shoulder muscles with respect to axial rotation of the glenohumeral joint in four positions. Clin. Biomech. 15:322–329, 2000.
Lang, A. E., J. H. Lin, and C. R. Dickerson. Activation patterns of shoulder internal and external rotators during pure axial moment generation across a postural range. J. Biomech.123:110503, 2021.
Lieber, R. L., and J. Fridén. Clinical significance of skeletal muscle architecture. Clin. Orthopaed. Relat. Res. 383:140–151, 2001.
Liu, J., R. E. Hughes, W. P. Smutz, G. Niebur, and K. Nan-An. Roles of deltoid and rotator cuff muscles in shoulder elevation. Clin. Biomech. 12:32–38, 1997.
Ludewig, P. M., V. Phadke, J. P. Braman, D. R. Hassett, C. J. Cieminski, and R. F. Laprade. Motion of the shoulder complex during multiplanar humeral elevation. J. Bone Jt. Surg. Ser. A. 91:378–389, 2009.
Mathai, B., and S. Gupta. Numerical predictions of hip joint and muscle forces during daily activities: A comparison of musculoskeletal models. Proc. Inst. Mech. Eng. 233:636–647, 2019.
Modenese, L., and J. Kohout. Automatic generation of personalised skeletal models of the lower limb from three-dimensional bone geometries. Ann. Biomed. Eng. 116:110186, 2020.
Mohr, A., and M. Gleicher. Building efficient, accurate character skins from examples. ACM Trans. Graph. 22(3):562–568, 2003.
Mulla, D. M., J. N. Hodder, M. R. Maly, J. L. Lyons, and P. J. Keir. Modeling the effects of musculoskeletal geometry on scapulohumeral muscle moment arms and lines of action. Comput. Methods Biomech. Biomed. Eng. 22:1311–1322, 2019.
Otis, J. C., C. C. Jiang, T. L. Wickiewicz, M. G. E. Peterson, R. F. Warren, and T. J. Santner. Changes in the moment arms of the rotator cuff and deltoid muscles with abduction and rotation. J. Bone Jt. Surg. 76:667–676, 1994.
Péan, F., C. Tanner, C. Gerber, and P. Fürnstahl. A comprehensive and volumetric musculoskeletal model for the dynamic simulation of the shoulder function. Comput. Methods Biomech. Biomed. Eng. 22:740–751, 2019.
Reilly, M., and K. Kontson. Computational musculoskeletal modeling of compensatory movements in the upper limb. J. Biomech.108:109843, 2020.
Saul, K. R., X. Hu, C. M. Goehler, M. E. Vidt, M. Daly, A. Velisar, and W. M. Murray. Benchmarking of dynamic simulation predictions in two software platforms using an upper limb musculoskeletal model. Comput. Methods Biomech. Biomed. Eng. 18:1445–1458, 2014.
Seth, A., M. Dong, R. Matias, and S. Delp. Muscle contributions to upper-extremity movement and work from a musculoskeletal model of the human shoulder. Front. Neurorobot. 13:90, 2019.
Seth, A., J. L. Hicks, T. K. Uchida, A. Habib, L. Dembia, J. J. Dunne, C. F. Ong, M. S. Demers, A. Rajagopal, M. Millard, S. R. Hamner, E. M. Arnold, R. Yong, S. K. Lakshmikanth, M. A. Sherman, J. P. Ku, and S. L. Delp. OpenSim: Simulating musculoskeletal dynamics and neuromuscular control to study human and animal movement. PLoS Comput. Biol. 14(7):e1006223–e1006224, 2018.
Seth, A., R. Matias, A. P. Veloso, and S. L. Delp. A biomechanical model of the scapulothoracic joint to accurately capture scapular kinematics during shoulder movements. PLoS ONE. 11:1–18, 2016.
Seth, A., M. Sherman, P. Eastman, and S. Delp. Minimal formulation of joint motion for biomechanisms. Nonlinear Dyn. 62:291–303, 2010. https://doi.org/10.1007/s11071-010-9717-3.
Valente, G., G. Crimi, N. Vanella, E. Schileo, and F. Taddei. NMSBUILDER: freeware to create subject-specific musculoskeletal models for OpenSim. Comput. Methods Prog. Biomed. 152:85–92, 2017.
Inman, V. T., J. D. M. Saunders, and L. C. Abbott. Observations of the function of the shoulder joint. J. Bone Jt. Surg. 26(1):1–30, 1944.
Webb, J. D., P. Taylor, S. S. Blemker, and S. L. Delp. 3D finite element models of shoulder muscles for computing lines of actions and moment arms. Comput. Methods Biomech. Biomed. Eng. 17(8):829–837, 2014.
Weinhandl, J. T., and H. J. Bennett. Musculoskeletal model choice influences hip joint load estimations during gait. J. Biomech. 91:124–132, 2019.
de Wilde, L., E. Audenaert, E. Barbaix, A. Audenaert, and K. Soudan. Consequences of deltoid muscle elongation on deltoid muscle performance: a computerised study. Clin. Biomech. 17:499–505, 2002.
Wu, G., F. C. T. van der Helm, H. E. J. Veeger, M. Makhsous, P. van Roy, C. Anglin, J. Nagels, A. R. Karduna, K. McQuade, X. Wang, F. W. Werner, and B. Buchholz. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: shoulder, elbow, wrist and hand. J. Biomech. 38:981–992, 2005.
Xiao, M., and J. Higginson. Sensitivity of estimated muscle force in forward simulation of normal walking. J. Appl. Biomech. 26(2):142–149, 2010.
Acknowledgments
The authors wish to thank the staff of the Mechanical System Design Laboratory-EMP.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Associate Editor Jillian Urban oversaw the review of this article.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kedadria, A., Benabid, Y., Remil, O. et al. A Shoulder Musculoskeletal Model with Three-Dimensional Complex Muscle Geometries. Ann Biomed Eng 51, 1079–1093 (2023). https://doi.org/10.1007/s10439-023-03189-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-023-03189-y