
Abstract
The aim of this study was to develop a methodology based on muscle synergies to investigate whether rectilinear and curvilinear walking shared the same neuro-motor organization, and how this organization was fine-tuned by the walking condition. Thirteen healthy subjects walked on rectilinear and curvilinear paths. Electromyographic data from thirteen back and lower-limb muscles were acquired, together with kinematic data using inertial sensors. Four macroscopically invariant muscle synergies, extracted through non-negative matrix factorization, proved a shared modular organization across conditions. The fine-tuning of muscle synergies was studied through non-negative matrix reconstruction, applied by fixing muscle weights or activation profiles to those of the rectilinear condition. The activation profiles tended to be recruited for a longer period and with a larger amplitude during curvilinear walking. The muscles of the posterior side of the lower limb were those mainly influenced by the fine-tuning, with the muscles inside the rotation path being more active than the outer muscles. This study shows that rectilinear and curvilinear walking share a unique motor command. However, a fine-tuning in muscle synergies is introduced during curvilinear conditions, adapting the kinematic strategy to the new biomechanical needs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Human bipedal locomotion is an inherently unstable task that requires accurate control of body progression and balance in the mediolateral plane.38 The central nervous system (CNS) allows humans to face various walking paths during daily life, of which only 55% are fully straight,21 and to accomplish them efficiently through the coordinated activation of muscles. The analysis of muscle coordination during various types of walking paths, especially those where mediolateral balance is challenged, can provide insight on the way the CNS adapts to these different conditions. Examples of daily-life walking paths are curvilinear trajectories,15,16 which represent a challenge for the elderly and neurologically-impaired subjects,22,24,32 as they require more cognitive flexibility32 and may heighten the risk of falling. The strategies that healthy subjects use to cope with such challenge have been studied in terms of muscle activation,14,18 kinematics,16,18 and kinetics.18,23,44 These studies have shown small modifications in muscle activation, speed or kinematics during curvilinear trajectories that contribute to a slightly different biomechanical strategy that tends to include the inclination of the trunk towards the centre of the curve.22,44
The study of muscle activations has been enriched with the formalization of muscle synergies.3 Muscle synergies are neural structures that are hypothesized to simplify the control of movement and posture3 through the activation of groups of muscles with the same neural command, fine-tuned to deal with the need of a given motor task. Thus, muscle synergies allow the extraction of repeatable patterns of synchronous muscle activations, making intuitive their association with a specific biomechanical function. For this reason, they have been used to give new insight into the traditional upper35 and lower-limb2,12,13 movement analysis, by finding the motor primitives that were combined to generate those movements.
Several studies have analysed gait in terms of muscle synergies, during treadmill walking at different speeds,13,30 rectilinear overground walking,29 running,7 walking with altered mechanical demands,30,33 perturbed standing or walking balance,12 and walking with changes in speed, cadence, step length and step height.39 However, curvilinear trajectories have not received much attention, despite their frequent occurrence in daily-life walking and their implications in terms of balance control.
The aim of the present study was to analyse the muscle synergies of healthy subjects during rectilinear and curvilinear walking. Our hypothesis was that rectilinear and curvilinear walking share a common modular organization.14 We did expect minor behavioural adjustments of the CNS to the curvilinear trajectory, reflected in the tuning of the muscle synergies activation and recruitment. The second objective of the study was the definition of a methodology to quantitatively assess the fine-tuning of muscle synergies activation and recruitment across walking conditions. Such a methodology could be used in further studies to highlight not only significant differences across walking conditions, but also the changes in muscle synergy tuning occurring in patients with motor impairments.
Materials and Methods
Experimental Protocol
Thirteen healthy young subjects (7 men, age: 24.8 ± 1.3 years, height: 1.73 ± 0.11 m, weight: 60.8 ± 11.4 kg) walked at their self-selected speed on a rectilinear and a curvilinear path. The latter was performed by turning both clockwise and counterclockwise. The three walking conditions will be referred as rectilinear, internal and external, where the last two correspond to the curvilinear trajectory performed with the dominant leg on the internal or external side of the curve, respectively. The dominance of the leg was established by asking the subjects which leg they would use to kick a ball.18 The rectilinear walking was performed on a 10-m path and was repeated 10 times. The curvilinear path was drawn with a tape stuck on the floor with a radius of 1.2 m,16,23,24,44 and was travelled 10 times for each turning direction.
Surface electromyography (EMG) was used to record the activity of the main muscles of the dominant leg and of the ipsilateral side of the back, for a total of 15 muscles: Erector Spinae (ES), External Oblique (EO), Adductor Magnus (AM), Gluteus Maximus (GM), Tensor Fasciae Latae (TFL), Rectus Femoris (RF), Vastus Lateralis (VL), Vastus Medialis (VM), Medial Hamstrings (MH), Biceps Femoris (in the following referred to as Lateral Hamstrings, LH), Medial Gastrocnemius (MG), Lateral Gastrocnemius (LG), Soleus (SO), Peroneus Longus (PL), and Tibialis Anterior (TA). The EMG data were acquired at 1024 Hz using a multi-channel signal amplifier system (Porti™, Twente Medical System International, The Netherlands). Self-adhesive Ag/AgCl electrodes (Kendall™, COVIDIEN, USA) were applied to shaved skin.
The kinematic data were acquired at 50 Hz by means of 3 inertial and magnetic sensors (MTx, Xsens Technologies B.V., The Netherlands) positioned on the chest and the external part of both shanks.
The Internal Advisory Board of the Institute of Veruno, Fondazione Salvatore Maugeri (IRCCS), approved the protocol, and informed consent was obtained from all patients.
Kinematics Analysis
The gyroscope signal from both shank sensors was used to extract the phases of stationary walking and divide gait into cycles. The initiation and termination phases of each walking repetition were removed, selecting only the cycles where the peak-to-peak amplitude of the sagittal-plane shank angular speed remained within a stable range. Then, gait cycles were delimited using the initial contact with the ground of the dominant leg,11 and they were further split into six gait sub-phases (left and right double supports, initial swings, and terminal swings), using an algorithm developed and validated by the authors.11
For each gait cycle, the following gait parameters were computed: cadence, duration of the dominant-leg stance and swing sub-phases (as percentage of the gait cycle), sum of the duration of the double support sub-phases (as percentage of the gait cycle), and mediolateral inclination of the trunk. This angle was estimated from the accelerometer signal of the chest sensor after low-pass filtering the signal and applying a trigonometric transformation.5
Additionally, the walking speed of each repetition was obtained by measuring the duration of the trials with a stopwatch. The mean walking speed was computed separately for each subject and condition, and it was correlated with the duration of the gait sub-phases, to test whether the adaptations of the gait sub-phases to the curvilinear walking could have been caused by changes in walking speed.13
EMG Processing
EMG Pre-Processing
The EMG envelopes were obtained from the raw EMG data by applying a band-pass filter (3rd-order Butterworth filter, passband: 40–400 Hz), a rectifier, and a low-pass filter (3rd-order Butterworth filter, cut-off frequency of 5 Hz, chosen to keep 95% of the total power of the signal).41 The EMG signals were split into gait cycles using the initial contact of the dominant leg, extracted from the shank sagittal-plane angular velocity. Each cycle was interpolated into a 100-point vector. Outliers and motion artefacts were removed by visual inspection, keeping on average twenty representative strides per-subject and condition to guarantee a proper muscle-synergies reconstruction.36 Afterwards, the EMG envelopes of each muscle were normalized for all conditions to the median peak value calculated across the strides of the rectilinear walking condition.
The quality of the EMG envelopes was evaluated through their intra-individual variability, using the Variance Ratio (VR).4,26 The values of VR were calculated separately for each muscle, condition, and subject. Then, the VR values were averaged across subjects. VR was calculated as indicated in Eq. (1) where i and j represent the samples within each gait cycle and the number of gait cycles, respectively, whereas n is the number of strides over which the VR was calculated. \(X_{ij}\) is the value of the EMG envelope at the i-th sample of the j-th cycle, \(\bar{X}_{j}\) is the mean value of the EMG envelope obtained for the i-th sample calculated across the strides, and \(\bar{X}\) is the grand mean of the EMG envelope.
Extraction of Individual Muscle Synergies
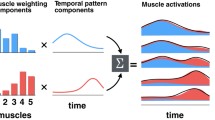
The non-negative matrix factorization (NMF) algorithm was applied, separately for each subject and condition, to the EMG matrix, M, with size m·n (where m is the number of muscles, and n is equal to the number of strides multiplied by 100 samples/stride).31 This factorization technique decomposes the EMG matrix M into a linear combination of k muscle synergies, allowing a certain level of reconstruction error, ε (2). Mathematically, the muscle synergies are the factorization of the EMG signals into two matrices: the muscle weights matrix, W, containing the relative level of contribution of each muscle to the muscle synergy, and the activation profile matrix, H, containing the temporal profile of activation of the muscle synergy throughout the gait cycle.
To use this technique, the number of muscle synergies must be specified a priori, as the quality of the reconstruction depends on it. This quality was measured by comparing the original data (M) with the reconstruction (R = W·H), using the Variability Accounted For (VAF) as a figure of merit. The VAF is defined by Eq. (3), where i and j are two indexes representing the different muscles and samples, respectively. The repeatability of the algorithm was assessed by studying the variability of the total VAF obtained in ten separate factorizations of the M matrix for each subject and condition, initializing each time the matrices W and H to random values.
The number of muscle synergies was chosen independently for each subject and condition, as the smallest number that allowed the reconstruction with a total VAF higher than 90%, or the number that did not improve the single-muscles VAF more than 5% when adding a new muscle synergy.13 Then, the modal value of muscle synergies was used to extract them from all subjects and conditions.13
Comparison of Muscle Synergies Across Walking Conditions
When extracting muscle synergies, the variability of the EMGs is divided into two factors: muscle weights and activation profiles. This implies that to compare two sets of muscle synergies (i.e., those from two walking conditions), the variations in both factors would have to be considered. An alternative way is comparing conditions through non-negative matrix reconstruction (NMR),35 which fixes one of the two factors (muscle weights or activation profiles) letting the remaining factor update at each NMR iteration. This way, the variability of the EMG is always forced to be represented only by the varying factor, and the parameters estimated from that factor already contain meaningful information of the differences between conditions. We performed two separate NMR through the procedure detailed below, by fixing the muscle weights or the activation timing profiles to the mean physiological muscle synergies extracted from the rectilinear condition.
Computation of the Mean Muscle Synergies
All muscle-weight vectors from the individual muscle synergies were normalized to have unit module, and all activation timing profiles were forced to have maximum amplitude equal to one. A mean set of weights (W mean) and activation profiles (H mean) was computed for each condition by averaging across subjects. To establish whether the average muscle synergies were representative of the group of subjects, for each walking condition, the mean muscle synergies were compared to the individual muscle synergies. The metrics used as figures of merit were the similarity9 (normalized scalar product) for the muscle weights, and the circular cross-correlation28 and time lag28 for the activation timing profiles. The muscle synergies were considered representative when their average values were above 0.75 for the similarity,10 above 0.75 for the cross-correlation,20 and lower than 5% of gait cycle for the time lag.
Non-Negative Reconstruction with the Mean Rectilinear Muscle Synergies
In the first reconstruction analysis, the vector of muscle weights was fixed to the W mean of the rectilinear condition, and the reconstructed H (H rec) was updated at every NMR algorithm iteration. For each subject, the H rec from each pair of conditions were compared using the circular cross-correlation and the time lag. Then, the H rec were normalized to have a maximum value of one. The metrics used to assess the fine-tuning of the reconstructed activation timing profiles were the onset, offset, and area under the curve.25,40 These values were computed for each gait cycle and each muscle synergy. The onset and offset were identified as the percentage of the gait cycle where the signal ascended and descended, respectively, above or below a threshold defined as the minimum of each cycle plus 20% of the cycle peak-to-peak amplitude. Additionally, a battery of correlations was performed to understand whether differences in onset and offset across walking conditions were dependent on the transition between gait sub-phases that occurred shortly before or after them.
The second reconstruction analysis was performed by fixing the activation timing profiles to the average of the rectilinear condition, and letting the reconstructed muscle weights variate across algorithm iterations (W rec). These reconstructed muscle weights were compared for each subject across walking conditions using the similarity9 (normalized scalar product). To identify the relevant muscles within each muscle synergy, we reconstructed the muscle synergies with ten bootstrapped versions of the dataset.8,25 Each new dataset was created with replacement, starting from the original EMG dataset, by maintaining the total number of EMG cycles included in the analysis.8 The confidence intervals of the muscle contribution to each synergy (muscle weight) were computed separately for each condition.25 Each muscle was defined as significantly active within each muscle synergy when the confidence interval of its weights did not include zero (i.e., when its weights were significantly greater than zero)25 for at least one of the walking conditions. The muscles identified as active within a muscle synergy were further compared across walking conditions to assess the fine-tuning of the reconstructed muscle weights.
The VAF was used to assess the reliability of both reconstruction analyses, which were considered acceptable if their total VAF was greater than 0.75.
Statistical Analysis
The inter-cycle repeatability of all the kinematics and EMG parameters obtained from H rec was tested by computing their standard deviation. Then, each parameter was averaged across gait cycles to convey the results with one value per-subject and condition.
After verifying the normality with the Shapiro–Wilk test of the walking speed, we computed the mean kinematic parameters (cadence, trunk inclination, stance phase, double-support phase) and EMG parameters extracted from H rec (onset, offset, area) and W rec (muscle weights of the muscles identified as active within a muscle synergy). Then, the walking conditions were compared using a 1-way repeated-measures ANOVA (p = 0.05) separately applied to each parameter. The Mauchly’s test was used to verify the sphericity of the data, applying the Greenhouse–Geisser correction when the sphericity assumption was violated. The Bonferroni post hoc test was used to analyse which pairs of conditions were statistically different.
Results
The median [interquartile range] number of strides used for the processing of each subject and walking condition was 20.0 [1.5] strides.
Kinematics
All kinematic parameters showed very high inter-cycle reliability. Their standard deviation across gait cycles was 0.02 strides/s for the cadence, 0.7° for the mediolateral inclination angle of the trunk, and 3.0 and 2.3% of the Gait Cycle (%GC) for the duration of the double support and the stance gait sub-phases, respectively. The statistical analysis (Fig. 1; Table 1) showed that cadence was significantly higher in rectilinear than in curvilinear gait. The inclination of the trunk showed significant variations across all conditions, being inclined towards the centre of the curve during curvilinear walking and almost straight during rectilinear walking. The duration of the stance gait sub-phase was significantly higher for the internal condition than for the others, whereas the double support was significantly shorter for the rectilinear walking with respect to the other two conditions.

Results of the kinematics analysis. For each condition, the mean and standard deviation values for cadence, trunk inclination, stance and double support phases are reported. Asterisks represent significant differences between conditions: * p < 0.05, ** p < 0.01, *** p < 0.001.
The mean ± standard deviation value of the walking speed for the rectilinear condition was 1.14 ± 0.12 m/s, which was higher than for the other conditions, with 1.04 ± 0.20 m/s for internal trajectory and 1.05 ± 0.16 m/s for external trajectory. These differences were not statistically significant. There was no correlation between the duration of the stance and double-support phases with the walking speed (r 2 = 0.35, and 0.39, respectively).
EMG Processing
EMG Pre-Processing
The mean Variance Ratio (VR) of most muscles was very low, proving a high quality and repeatability of the EMG signals. However, there were two muscles that had to be excluded from the analysis. The first was the AM, with a VR of 0.35, which was repeatedly affected by motion artefacts due to the crossing of the legs, especially during the condition of internal walking. Additionally, the electrodes to acquire the EO were poorly positioned in some subjects, since the signal showed a low signal-to-noise ratio that was translated into a VR of 0.56. Thus, both muscles had to be excluded from further analysis. The mean VR of the remaining muscles ranged from 0.09 (SO) to 0.25 (PL).
Extraction of Individual Muscle Synergies
The extraction of muscle synergies was repeatable across different factorizations. The algorithm converged to total VAF values whose mean within-subject and within-condition standard deviation was 0.001. Among all the 39 individual muscle synergy extractions (13 subjects, 3 walking conditions), 21 required 4 muscle synergies, and 18 required 5. The number of muscle synergies was not dependent of the walking condition. Indeed, 3 subjects required 4 muscle synergies for all conditions, other 3 subjects always required 5 muscle synergies, and the rest did not have a specific trend. Out of the 18 extractions that required 5 muscle synergies, 7 had reached a VAF higher than 0.89 with four muscle synergies. The fifth muscle synergy was usually needed only to gather the variability of the original EMG signals, as it was often not repeatable across cycles (measured through a high VR of the muscle synergy activation profile) and did not have a clear activation phase. Therefore, 4 muscle synergies were extracted for all subjects and conditions, obtaining mean ± standard deviation VAF values of 0.89 ± 0.03, 0.89 ± 0.02, and 0.89 ± 0.02 for the rectilinear, internal, and external walking conditions, respectively.
The four extracted muscle synergies are shown in Fig. 2. Each muscle synergy was associated with a biomechanical gait subtask, which depended on the muscles recruited and its main phase of activation:

Mean and standard deviation of the muscle weights and activation timing profiles of the individual muscle synergies, for the three conditions (identifying colours are in the bottom left box). The six gait sub-phases identified by the inertial-sensor based algorithm11 are included and represented in the activation timing profiles through vertical dashed lines.
- Weight acceptance :
-
Recruiting mainly the GM, TFL, RF, VL, VM, and TA, this muscle synergy was active during early stance to provide body support and acceptance of the weight transfer.
- Push-off :
-
This muscle synergy grouped the MG, LG, SO, and PL during late stance to provide forward propulsion and actively restrain the forward rotation of the tibia, controlling the gap between the centre of mass and the centre of pressure.27
- Trunk balance :
-
This muscle synergy was mainly characterized by the activation of the ES and the RF, and to a much lesser extent, SO, PL, and TA. The muscle synergy was active during the two double support phases, and can be associated with the support of the trunk during mediolateral transfers of body weight.
- Leg deceleration :
-
The last muscle synergy grouped the two hamstring muscles (MH, LH) with a smaller contribution of TA. The activation of the muscle synergy was predominant in early stance and late swing, acting to give propulsion to the body in the first case, and decelerate the leg in the latter.1
Comparison Across Walking Conditions
The comparison between the mean set of muscle synergies and the individually-extracted muscle synergies is reported in Table 2. The similarity and correlation were above their predefined threshold, whereas the time lag was below its threshold. Therefore, the mean muscle synergies were representative of the group under study.
High VAF values were obtained when the activation timing profiles were reconstructed using the mean weights of the rectilinear conditions (Fig. 3). Indeed, the mean ± standard deviation VAF values were 0.85 ± 0.03, 0.79 ± 0.04, and 0.82 ± 0.03 for the rectilinear, internal and external conditions, respectively.

Reconstructed muscle synergies using fixed rectilinear mean muscle weights. The mean and standard deviation of the reconstructed activation profiles are shown on the right side. The six gait sub-phases are represented in the activation timing profiles through vertical dashed lines. Identifying colours at the bottom.
Table 3 reports the comparison across walking conditions of the reconstructed activation timing profiles computed individually. The shape of the muscle synergies had a good agreement between conditions, with a median circular cross-correlation higher than 0.94 and a median time lag shorter than 3%GC.
The parameters extracted from the reconstructed profiles showed a high inter-cycle repeatability. Their mean standard deviation across gait cycles was 4.5%GC for the onset, 4.9%GC for the offset, and 5.5 for the area under the curve. The results of the one-way repeated-measures ANOVA are reported in Table 4 and shown in Fig. 4. In all muscle synergies, the curvilinear conditions showed more extended activation profiles than the rectilinear. Specifically, in the Weight-Acceptance muscle synergy, the offset of the external walking condition was significantly delayed with respect to the rectilinear walking; the external walking condition was also characterized by an augmented activation with respect to the other two conditions. In the Push-Off muscle synergy, both curvilinear conditions showed a profile that was activated significantly earlier than in the rectilinear walking, whereas in the Trunk-balance muscle synergy the internal walking condition had the longest activation. In the leg-deceleration muscle synergy, the external walking profile was anticipated with respect to the rectilinear walking, but it was also activated with lower amplitude.

Left panel: mean and standard deviation values of the intervals of onset and offset of the reconstructed activation timing profiles. The white crosses inside the bars represent the position of the maximum peak of activation. Right panel: area under the reconstructed activation timing profiles. For the trunk-balance synergy, the area corresponds to the sum of the two activation phases. The six gait sub-phases are represented in the activation timing profiles through vertical dashed lines. In both panels, the asterisks show significant differences: * p < 0.05, ** p < 0.01, *** p < 0.001.
Two of the correlations performed between the onset and offset of the reconstructed activation profiles and the gait sub-phases were significant for most subjects. The first was the onset of the second peak of the Trunk-balance muscle synergy and the start of the swing phase, which was significant for 8 subjects (r 2 = 0.50 ± 0.10), with the muscle synergy activated on average 12.1%GC before the start of the swing phase. The correlation between the muscle contributing the most to this muscle synergy, the ES, and the beginning of the swing phase had already been reported in a previous study.16 The second significant correlation occurred between the onset of the leg-deceleration muscle synergy and the start of the ipsilateral terminal swing. This correlation was significant for 9 subjects (r 2 = 0.44 ± 0.11), seven of which overlapped with the previous subset of eight subjects. The onset of the muscle synergy occurred, on average, 6.9%GC before the beginning of the final gait sub-phase.
The VAF values obtained by reconstructing the muscle weights using the mean rectilinear activation timing profiles were always above the reliability threshold. The mean ± standard deviation values obtained across subjects were 0.87 ± 0.02, 0.84 ± 0.03, and 0.86 ± 0.02 for the rectilinear, internal, and external walking conditions, respectively.
As reported in Table 5, the median and interquartile ranges of the similarity computed between pairs of walking conditions were always very high and well above the 0.75 threshold.10
Figure 5 shows the reconstructed weights for each muscle synergy averaged across subjects. The one-way ANOVA performed on the muscle weights revealed a significant effect of walking conditions on most muscles considered significantly relevant for each muscle synergy (Table 6). In the Weight-Acceptance muscle synergy, both monoarticular muscles acting on the hip (GM and TFL) had a significantly greater weight in the external condition. Instead, the vasti group (VM, VL) had significantly lower weights in both curvilinear conditions than in the rectilinear walking condition. In the Push-Off muscle synergy, the activity of the LG was significantly augmented in the internal with respect to the external walking condition and the opposite modulation was found in the MG muscle. A similar behaviour was found in the leg-deceleration muscle synergy where the LH was significantly more active in the internal and MH in the external condition. The contribution of the RF to the Trunk-balance muscle synergy was significantly different across all walking conditions, being significantly higher for the rectilinear condition, and significantly lower for the external condition.

Reconstructed muscle weights using fixed rectilinear mean activation timing profiles. The mean and standard deviation of the contribution of each muscle to the synergies are shown in the left panel. The six gait sub-phases are represented in the activation timing profiles through vertical dashed lines. Statistical differences are shown only for the muscles whose contribution to the muscle synergy was considered relevant. Asterisks represent significant differences: * p < 0.05, ** p < 0.01, *** p < 0.001.
Discussion
Our results support the hypothesis that walking along rectilinear and curvilinear trajectories share the same number of muscle synergies and associated biomechanical functions. Four muscle synergies were extracted for all conditions, each related to a different biomechanical function: weight acceptance, push off, trunk balance, and leg deceleration. The muscle synergies obtained for the rectilinear trajectory were able to reconstruct reliably the muscle activity during the curvilinear trajectories, as the mean reconstruction VAF values were always greater than 0.8 for all conditions. These results support the hypothesis that the kinematic changes characterizing the curvilinear walking22,44 could be ascribed to a fine-tuning of both temporal recruitment and spatial composition of the single muscle synergies,14 but not to the creation of new muscle synergies to cope with the different complexity of the movement. It was shown earlier16 that curved walking introduces kinematic changes and a fine-tuning in amplitude and timing of the EMG bursts. Our findings are compatible with the view that, for curved walking, a descending command modulates the spinal oscillators that control both straight-ahead and curved walking.14
Fine Tuning of Muscle Synergies Across Conditions
The proposed methodology allowed further comparison across walking conditions by reconstructing the muscle synergies using the rectilinear muscle synergies as reference. This analysis confirmed that during curvilinear walking, the motor command was slightly modified by a fine-tuning that introduced variations mainly on recruitment timing and on the activation amplitude of posterior muscles. In fact, during curvilinear walking, the activation of some muscle synergies was longer and often larger (Fig. 4), likely to cope with a more challenging walking modality.22,32,44 These changes in activation were not only due to changes in the duration of gait sub-phases, since the transitions between gait phases were not strongly correlated to the onset and offset of the muscles synergies. The Weight-Acceptance muscle synergy had delayed offset and augmented amplitude when the leg was at the external part of the curve, which is the condition where during stance the body weight moves away from the stance leg in the mediolateral direction. Under this condition, the gluteus maximus and tensor fasciae latae were more active than during rectilinear and internal conditions. The Push-Off muscle synergy anticipated its activation in both curvilinear conditions with respect to the rectilinear, giving stability to the ankle and the knee during the stance phase. Looking at single-muscle involvement in the Push-Off muscle synergy (Fig. 5), soleus and medial gastrocnemius reduced their activity in the internal condition, whereas lateral gastrocnemius reduced its activity for the external. Both behaviours are consistent with previous studies.14,18 In the trunk-balance muscle synergy, the offset of the second peak was significantly delayed in the internal condition, suggesting that it might take longer to transfer the weight to the contralateral leg when the centre of mass is slightly shifted towards the ipsilateral leg.42 Finally, the onset of the leg-deceleration muscle synergy was significantly anticipated in the external condition, maybe due to a larger excursion of the leg during the swing phase. This longer activation was somewhat compensated by a significant decrease in the activation amplitude.
The results uncovered the modulation of the posteromedial and posterolateral muscles during curvilinear walking. For both gastrocnemii and hamstrings, the muscles that remained internal to the rotation path were always more active than the outer muscles. Thus, during the internal condition, the lateral gastrocnemius was more active than the medial gastrocnemius, and the opposite happened during the external condition. This modulation had already been identified by two single-muscle studies of curvilinear walking.16,18 The same modulation was also found for the hamstrings muscles, confirming what was already found in a previous study.18 This modulation could be due to a strategy to allow the body to rotate while the centre of mass shifts towards the inside of the curvilinear path.18
Methodological Considerations
Three of the muscle synergies presented in this study (weight acceptance, push off, leg deceleration) agreed with the results obtained in other studies, in terms of composition and associated biomechanical functions.1,13,30 The only muscle synergy that is somewhat different here from most studies in the literature is the trunk-balance muscle synergy, identified in other studies30,40 as a factor with a large contribution of the erector spinae. This muscle synergy is usually substituted with the Foot-Clearance muscle synergy, which couples the rectus femoris and tibialis anterior in a double-peak muscle synergy.1,13
Regarding the number of muscle synergies, other studies have restricted the study to eight muscles and obtained four muscle synergies,13 whereas others augmented to a range of 12–16 muscles and extracted five30 or more40 muscle synergies. Since the selection of muscles has been proven to influence not only the number of muscle synergies, but also their composition,37 we analysed the effect that our set of muscles had on the resultant number of muscle synergies and their structure. We restricted our set of muscles to those acquired by Clark et al.13 (GM, RF, VM, MH, LH, MG, SO and TA), to test whether the extraction of muscle synergies for the rectilinear condition would provide analogous results. The resultant four muscle synergies (Fig. 6) were extracted with mean ± standard deviation VAF values of 0.90 ± 0.03. The weight acceptance, push off, and leg deceleration muscle synergies were analogous to those previously found,13 and those extracted for the rectilinear condition with the full dataset of thirteen muscles. However, the third muscle synergy was substituted by the Foot Clearance, which is equivalent to the muscle synergy found in other gait studies with a restricted set of muscles.1,13 From the present analysis, it can be inferred that the trunk-balance muscle synergy is influenced by the inclusion of the erector spinae into the dataset. There was also a secondary effect of increasing the dataset of muscles to thirteen, which is the redistribution of the tibialis anterior within the remaining muscle synergies, especially to the leg-deceleration muscle synergy.

Muscle synergies extracted during the rectilinear condition using the restricted set of muscles of Clark et al.13
A third methodological aspect to be considered is whether differences in walking speed could have influenced the results.13 The walking speed obtained in this study was similar,14 or slightly lower44 than in other studies of curvilinear walking. The values did not vary significantly across walking conditions, and were not correlated to the temporal duration of the gait sub-phases. Thus, the significant differences found in the muscle synergies across conditions throughout this study were not related to variations in walking speed.
In surface EMG measurements, crosstalk between muscles can affect the results. The crosstalk can be difficult to avoid especially between the peroneus longus and the tibialis anterior or lateral gastrocnemius.6 The effects of crosstalk on muscle synergies are particularly critical, since this factorization technique would highlight a common activation pattern across muscles. However, the separated recruitment of the peroneus longus with the tibialis anterior and with the lateral gastrocnemius in the muscle synergies (see Figs. 2 and 5) suggests that our data did not critically suffer from crosstalk.
The results presented in the present study could have been limited by the selection of the muscles that were included in the study. Additional muscles could have provided more insight on the CNS mechanisms steering the body during curvilinear walking. Even if the number of muscles acquired was high compared to other studies, some muscles with a putative role during curvilinear walking had to be excluded. This was due to a deliberate simplification of the experimental protocol, and to an impossible accurate acquisition of the activity of certain muscles with superficial EMG electrodes.
Another potential limitation of this study was that simultaneous bilateral EMG measures were not available to evaluate any inter-limb coordination. However, we preferred to increase the number of muscles acquired in the same side, given that literature supports that EMG signals acquired from legs and trunk of healthy subjects are invariant between sides.13,17 An additional limitation is that no metrics of stability were measured on the same subjects, preventing a more complete data interpretation.
The experimental protocol was restricted to the stationary state of curvilinear walking, by removing the initial and final parts of acceleration and deceleration. An analysis of the transitions between different walking conditions could be interesting since it could give valuable insight on the CNS mechanisms to adapt to new conditions. However, this would be somewhat difficult to analyse with muscle synergies, as reiterated muscle activations are required. Nevertheless, further studies should consider including transient states in the experimental protocol, since they can contain significant information on adaptation and coordination.
Only young healthy subjects were recruited in this study. This choice could reduce the generalization of the obtained results to older adult populations or to neurological patients normally having a higher average age. Nevertheless, during walking physiological muscle synergies have been proved to be invariant with aging.34
Clinical Impact
The analysis of muscle synergies during rectilinear and curvilinear walking can be integrated into the rehabilitation of neurological patients in several ways. First, it can be used to assess quantitatively motor control in patients, using walking trajectories closer to daily life. More specifically, the inclusion of curvilinear paths can provide information under a condition that particularly requires cognitive flexibility and balance control.32 In this scope, this analysis can be used both as a sole assessment of the patient’s coordination and as a measure of the effect of treatment on neural control.43 Second, the method of non-negative reconstruction can also be applied to factorize the pathological muscle activations using the physiological muscle weights or the activation timing profiles. This would allow a deeper understanding of the patient’s motor coordination, using the physiological muscle synergies as a gold standard of locomotion complexity. This approach has already been implemented by Ambrosini et al.,2 where the locomotor impairment of stroke patients was assessed during cycling. A further step would be to apply this assessment in a longitudinal study, as a way to understand the evolution in motor coordination or its eventual changes that might derive from a treatment. Eventually, this information can be exploited into the personalization of a neurorehabilitation treatment that might target the patient’s specific needs. As a matter of fact, an example of the non-negative reconstruction potential to help customizing a gait neuroprosthesis was demonstrated by the authors in a recent study.19
Conclusions
This study has presented evidence that supports that rectilinear and curvilinear walking share a unique motor command. However, during the curvilinear conditions, a fine-tuning in the muscle synergies was introduced, adapting the kinematic strategy to the new biomechanical needs. The methodology that was defined throughout the study uncovered that the muscle contributions to the muscle synergies were modulated by the walking condition, which was in agreement with previous studies that analysed EMG activity at the single-muscle level.14,18 The advantage of investigating the tuning in timing and amplitude in terms of muscle synergies lied in the possibility to understand how these muscles work together to create such uncovered adaptations.
References
Allen, J. L., and R. R. Neptune. Three-dimensional modular control of human walking. J. Biomech. 45:2157–2163, 2012.
Ambrosini, E., C. De Marchis, A. Pedrocchi, G. Ferrigno, M. Monticone, M. Schmid, T. D’Alessio, S. Conforto, and S. Ferrante. Neuro-Mechanics of Recumbent Leg Cycling in Post-Acute Stroke Patients. Ann. Biomed. Eng. 44:3238–3251, 2016.
Bizzi, E., and V. C. K. Cheung. The neural origin of muscle synergies. Front. Comput. Neurosci. 7:51, 2013.
Burden, A., M. Trew, and V. Baltzopoulos. Normalisation of gait EMGs: A re-examination. J. Electromyogr. Kinesiol. 13:519–532, 2003.
Bussmann, J. B., W. L. Martens, J. H. Tulen, F. C. Schasfoort, H. J. van den Berg-Emons, and H. J. Stam. Measuring daily behavior using ambulatory accelerometry: the Activity Monitor. Behav. Res. Methods. Instrum. Comput. 33:349–356, 2001.
Campanini, I., A. Merlo, P. Degola, R. Merletti, G. Vezzosi, and D. Farina. Effect of electrode location on EMG signal envelope in leg muscles during gait. J. Electromyogr. Kinesiol. 17:515–526, 2007.
Cappellini, G., Y. P. Ivanenko, R. E. Poppele, and F. Lacquaniti. Motor patterns in human walking and running. J. Neurophysiol. 95:3426–3437, 2006.
Cheung, V. C. K., A. d’Avella, and E. Bizzi. Adjustments of motor pattern for load compensation via modulated activations of muscle synergies during natural behaviors. J. Neurophysiol. 101:1235–1257, 2008.
Cheung, V. C. K., A. d’Avella, M. C. Tresch, and E. Bizzi. Central and sensory contributions to the activation and organization of muscle synergies during natural motor behaviors. J. Neurosci. 25:6419–6434, 2005.
Cheung, V. C. K., A. Turolla, M. Agostini, S. Silvoni, C. Bennis, P. Kasi, S. Paganoni, P. Bonato, and E. Bizzi. Muscle synergy patterns as physiological markers of motor cortical damage. Proc. Natl. Acad. Sci. 109:14652–14656, 2012.
Chia Bejarano, N. E. Ambrosini, A. Pedrocchi, G. Ferrigno, M. Monticone, and S. Ferrante. A Novel Adaptive, Real-Time Algorithm to Detect Gait Events From Wearable Sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 23:413–422, 2015.
Chvatal, S. A., and L. H. Ting. Common muscle synergies for balance and walking. Front. Comput. Neurosci. 7:48, 2013.
Clark, D. J., L. H. Ting, F. E. Zajac, R. R. Neptune, and S. A. Kautz. Merging of healthy motor modules predicts reduced locomotor performance and muscle coordination complexity post-stroke. J. Neurophysiol. 103:844–857, 2010.
Courtine, G., C. Papaxanthis, and M. Schieppati. Coordinated modulation of locomotor muscle synergies constructs straight-ahead and curvilinear walking in humans. Exp. Brain Res. 170:320–335, 2006.
Courtine, G., and M. Schieppati. Human walking along a curved path. II. Gait features and EMG patterns. Eur. J. Neurosci. 18:191–205, 2003.
Courtine, G., and M. Schieppati. Tuning of a Basic Coordination Pattern Constructs Straight-Ahead and Curved Walking in Humans. J. Neurophysiol. 91:1524–1535, 2004.
Dominici, N., Y. P. Ivanenko, G. Cappellini, A. D’Avella, V. Mondì, M. Cicchese, A. Fabiano, T. Silei, A. Di Paolo, C. Giannini, R. E. Poppele, and F. Lacquaniti. Locomotor primitives in newborn babies and their development. Science 334:997–999, 2011.
Duval, K., K. Luttin, and T. Lam. Neuromuscular strategies in the paretic leg during curved walking in individuals post-stroke. J. Neurophysiol. 106:280–290, 2011.
Ferrante, S., and N. Chia. Bejarano, E. Ambrosini, A. Nardone, A. M. Turcato, M. Monticone, G. Ferrigno, and A. Pedrocchi. A Personalized Multi-Channel FES Controller Based on Muscle Synergies to Support Gait Rehabilitation after Stroke. Front. Neurosci. 10:425, 2016.
Gizzi, L., J. F. Nielsen, F. Felici, Y. P. Ivanenko, and D. Farina. Impulses of activation but not motor modules are preserved in the locomotion of subacute stroke patients. J. Neurophysiol. 106:202–210, 2011.
Glaister, B. C., G. C. Bernatz, G. K. Klute, and M. S. Orendurff. Video task analysis of turning during activities of daily living. Gait Posture 25:289–294, 2007.
Godi, M., A. Nardone, and M. Schieppati. Curved walking in hemiparetic patients. J. Rehabil. Med. 42:858–865, 2010.
Godi, M., A. M. Turcato, M. Schieppati, and A. Nardone. Test-retest reliability of an insole plantar pressure system to assess gait along linear and curved trajectories. J. Neuroengineering Rehabil. 11:95, 2014.
Guglielmetti, S., A. Nardone, A. M. De Nunzio, M. Godi, and M. Schieppati. Walking along circular trajectories in Parkinson’s disease. Mov. Disord. 24:598–604, 2009.
Hayes, H. B., S. A. Chvatal, M. A. French, L. H. Ting, and R. D. Trumbower. Neuromuscular constraints on muscle coordination during overground walking in persons with chronic incomplete spinal cord injury. Clin. Neurophysiol. 125:2024–2035, 2014.
Hershler, C., and M. Milner. An Optimality Criterion for Processing Electromyographic (EMG) Signals Relating to Human Locomotion. IEEE Trans. Biomed. Eng. 25:413–420, 1978.
Honeine, J.-L., M. Schieppati, O. Gagey, and M.-C. Do. By counteracting gravity, triceps surae sets both kinematics and kinetics of gait. Physiol. Rep. 2:e00229, 2014.
Hug, F., N. A. Turpin, A. Couturier, and S. Dorel. Consistency of muscle synergies during pedaling across different mechanical constraints. J. Neurophysiol. 106:91–103, 2011.
Ivanenko, Y. P., G. Cappellini, N. Dominici, R. E. Poppele, and F. Lacquaniti. Coordination of locomotion with voluntary movements in humans. J. Neurosci. 25:7238–7253, 2005.
Ivanenko, Y. P., R. E. Poppele, and F. Lacquaniti. Five basic muscle activation patterns account for muscle activity during human locomotion. J. Physiol. 556:267–282, 2004.
Lee, D. D., and H. S. Seung. Learning the parts of objects by non-negative matrix factorization. Nature 401:788–791, 1999.
Lowry, K. A., J. S. Brach, R. D. Nebes, S. A. Studenski, and J. M. VanSwearingen. Contributions of Cognitive Function to Straight- and Curved-Path Walking in Older Adults. Arch. Phys. Med. Rehabil. 93:802–807, 2012.
McGowan, C. P., R. R. Neptune, D. J. Clark, and S. A. Kautz. Modular control of human walking: Adaptations to altered mechanical demands. J. Biomech. 43:412–419, 2010.
Monaco, V., A. Ghionzoli, and S. Micera. Age-related modifications of muscle synergies and spinal cord activity during locomotion. J. Neurophysiol. 104:2092–2102, 2010.
Muceli, S., A. T. Boye, A. D’Avella, and D. Farina. Identifying representative synergy matrices for describing muscular activation patterns during multidirectional reaching in the horizontal plane. J. Neurophysiol. 103:1532–1542, 2010.
Oliveira, A. S., L. Gizzi, D. Farina, and U. G. Kersting. Motor modules of human locomotion: influence of EMG averaging, concatenation, and number of step cycles. Front. Hum. Neurosci. 8:335, 2014.
Pirondini, E., M. Coscia, A. Crema, M. Mancuso, and S. Micera. How the selection of muscles influences their synergies? A preliminary study using real data. In: 6th International IEEE/EMBS Conference on Neural Engineering (NER) (IEEE), 2013, pp. 581–584.
Rosenblatt, N. J., and M. D. Grabiner. Measures of frontal plane stability during treadmill and overground walking. Gait Posture 31:380–384, 2010.
Routson, R. L., S. A. Kautz, and R. R. Neptune. Modular organization across changing task demands in healthy and poststroke gait. Physiol. Rep. 2:e12055, 2014.
Sawers, A., J. L. Allen, and L. H. Ting. Long-term training modifies the modular structure and organization of walking balance control. J. Neurophysiol. 114:3359–3373, 2015.
Shiavi, R., C. Frigo, and A. Pedotti. Electromyographic signals during gait: Criteria for envelope filtering and number of strides. Med. Biol. Eng. Comput. 36:171–178, 1998.
Sozzi, S., J.-L. Honeine, M.-C. Do, and M. Schieppati. Leg muscle activity during tandem stance and the control of body balance in the frontal plane. Clin. Neurophysiol. 124:1175–1186, 2013.
Ting, L. H., H. J. Chiel, R. D. Trumbower, J. L. Allen, J. L. McKay, M. E. Hackney, and T. M. Kesar. Neuromechanical principles underlying movement modularity and their implications for rehabilitation. Neuron 86:38–54, 2015.
Turcato, A., M. Godi, A. Giordano, M. Schieppati, and A. Nardone. The generation of centripetal force when walking in a circle: insight from the distribution of ground reaction forces recorded by plantar insoles. J. Neuroeng. Rehabil. 12:4, 2015.
Acknowledgements
This research was supported by the Italian Ministry of Education, University and Research (Grant No. 2010R277FT) and the Italian Ministry of Health (Grant No. GR-2010-2312228).
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Thurmon E. Lockhart oversaw the review of this article.
Rights and permissions
About this article

Cite this article
Chia Bejarano, N., Pedrocchi, A., Nardone, A. et al. Tuning of Muscle Synergies During Walking Along Rectilinear and Curvilinear Trajectories in Humans. Ann Biomed Eng 45, 1204–1218 (2017). https://doi.org/10.1007/s10439-017-1802-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-017-1802-z