
Abstract
Historically, the investigations of electromyography (EMG) pattern recognition-based classification of intentional movements for control of multifunctional prostheses have adopted the filter cut-off frequency and sampling rate that are commonly used in EMG research fields. In practical implementation of a multifunctional prosthesis control, it is desired to have a higher high-pass cut-off frequency to reduce more motion artifacts and to use a lower sampling rate to save the data processing time and memory of the prosthesis controller. However, it remains unclear whether a high high-pass cut-off frequency and a low-sampling rate still preserve sufficient neural control information for accurate classification of movements. In this study, we investigated the effects of high-pass cut-off frequency and sampling rate on accuracy in identifying 11 classes of arm and hand movements in both able-bodied subjects and arm amputees. Compared to a 5-Hz high-pass cut-off frequency, excluding the EMG components below 60 Hz decreased the average accuracy of 0.1% in classifying the 11 movements across able-bodied subjects and increased the average accuracy of 0.1 and 0.4% among the transradial (TR) and shoulder disarticulation (SD) amputees, respectively. Using a 500 Hz instead of a 1-kHz sampling rate, the average classification accuracy only dropped about 2.0% in arm amputees. The combination of sampling rate and high-pass cut-off frequency of 500 and 60 Hz only resulted in about 2.3% decrease in average accuracy for TR amputees and 0.4% decrease for SD amputees in comparison to the generally used values of 1 kHz and 5 Hz. These results suggest that the combination of sampling rate of 500 Hz and high-pass cut-off frequency of 60 Hz should be an optimal selection in EMG recordings for recognition of different arm movements without sacrificing too much of classification accuracy which can also remove most of motion artifacts and power-line interferences for improving the performance of myoelectric prosthesis control.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The surface recordings of myoelectric signals, well known as electromyogram (EMG), are effective and important input signals in control of prostheses for people with limb amputations. Most commercially motorized artificial arms are controlled with EMG recordings from the remaining muscles of an amputated arm. Current myoelectric prostheses require a pair of remaining agonist–antagonist muscles for control of one degree of freedom (DOF) and allow only a single motion to be controlled at a time. As a result, given a limited number of residual muscles available after limb amputations, the conventional control method is not well suited for the intuitive control of prosthesis with multiple DOFs.14,20,24 A significant improvement over the conventional method is the use of EMG pattern recognition-based control strategy,1–3,6,7,9,11,14,20 which is grounded on the assumption that EMG patterns contain rich information about the intended movements involved in a residual limb.14 Previous efforts have showed that using a pattern classification technique, an intentional movement can be predicted with the distinguishable characteristics of EMG patterns1,2,10,20,22; this new method may allow users to operate a multifunctional prosthesis intuitively and easily. Some important issues related to this new control strategy, such as performance of various pattern recognition algorithms,1–3,6 EMG analysis window length,6 and EMG electrode displacement,10 have been well investigated. However, two other important issues, EMG signal conditioning and sampling rate, still remain uninvestigated.
EMG signals are commonly filtered by a band-pass filter to eliminate the interferences and noise. Properly choosing the frequency band for the band-pass filter would be of importance for improving the control performance of a myoelectric prosthesis. At the higher frequency side of signal spectrum, a low-pass filter is used to attenuate the unwanted high-frequency components in EMG signals and avoid aliasing signal distortion. Generally, the cut-off frequency of a low-pass filter is determined by the requirement of the Nyquist sampling theory, which should be equal or less than half of signal sampling rate. At the lower frequency side of signal spectrum, the cut-off frequency is determined by the need to remove slow variations in the signals caused by the motion artifacts such as electrode shift and cable movement. Almost all the previous studies of EMG pattern recognition-based prosthesis controls adopted a high-pass cut-off frequency ranging from 5 Hz to 20 Hz.4,5,8,23 The lower frequency components of EMG spectrum mainly contain the information on the firing rates of active motor units, which may be important for some EMG studies. However, these components may not make a significant contribution to the movement classification in EMG-based movement analysis.25 It is known that the cable motion artifacts typically have a frequency range of 1–50 Hz, and the power density of electrode motion artifacts is up to 20 Hz.5 Thus, a high-pass filter of 5–20 Hz could not effectively attenuate the motion artifacts, which may impair control accuracy and stability of a myoelectric prosthesis. Therefore, a higher high-pass cut-off frequency will be expected to significantly reduce more motion artifacts in the captured EMG signals; this may enhance the control accuracy and stability of a myoelectric prosthesis.
The Nyquist sampling theory states that the sampling rate must be at least twice the highest frequency of interest in a signal. It is well known that the major power (about 95%) of surface EMG signals is accounted for by harmonics up to 400–500 Hz5,26 and most of the EMG components with a frequency of more than 500 Hz are contributed by electrode and equipment noise or environmental interference. Thus, the widely used sampling rate in surface EMG studies is around 1,000 Hz.4,5,8,15 This sampling rate was also adopted in most studies of EMG pattern recognition prosthesis control.1–3,6,7,9,14,26 It is obvious that using a high-sampling rate may involve more high-frequency contents in myoelectric signals captured with surface electrodes, but it simultaneously adds more processing and computational complexity to the controller of a prosthesis. With the limited computation capability of a microprocessor-based prosthetic controller embedded into socket of a prosthesis, it would be desirable in EMG signal acquisition to use a low-sampling rate without compromising much of control performance of a prosthesis.
For the specific application of EMG signals in the movement analysis for control of multifunctional prostheses, it is unknown whether using a lower sampling rate in EMG acquisition and a higher cut-off frequency in EMG high-pass filtering still preserve sufficient neural control information for accurate classification of movement intents. In this study, we investigated the effects of EMG conditioning and sampling rate on the performance of EMG pattern recognition in identifying different classes of arm and hand motion. The outcomes of this study would aid the proper choice of EMG signal sampling rate and cut-off frequencies of band-pass filtering for the development of practical multifunctional myoelectric prostheses for limb amputees.
Methods
Subject Information
Eight patients with upper-limb amputations participated in the study. Five of the eight amputees had unilateral transradial (TR) amputation and the other three had shoulder disarticulation (SD). The five TR subjects (males) aged from 28 to 77 years and their post-amputation times ranged from 4 months to 21 years. The three SD amputees were a 54-year-old man with bilateral SD, a 24-year-old woman with a left SD, and a 37-year-old man with a right SD, who had targeted muscle reinnervation (TMR) to improve control of myoelectric prostheses.13,16–19 With TMR surgery, remaining arm nerves are transferred to residual chest or upper-arm muscles that are no longer biomechanically functional due to arm amputation. Once reinnervated, these muscles could provide physiologically appropriate myoelectric signals for control of hand, wrist, and elbow functions. For comparison, five able-bodied subjects (three males and two females) ranging from 22 to 46 years of age were also included in the study. The protocol of this study was approved by the Shenzhen Institutes of Advanced Technology Institutional Review Board, Chinese Academy of Sciences, China, and the Northwestern University Institutional Review Board, USA. All subjects gave written informed consent and provided permission for publication of photographs for scientific and educational purposes.
Experiment and EMG Data Acquisition
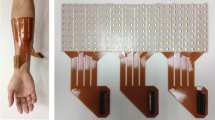
For each subject, 12 self-adhesive bipolar electrodes (Noraxon USA, Inc.) with a circular contact surface diameter of 1.25 cm and a center-to-center distance of 2 cm were used for EMG data acquisition. For able-bodied subjects, the 12 electrodes were placed on the biceps and triceps (CH1–CH2), the proximal forearm (6 electrodes around the apex of the muscle bulge, 2–3 cm distal to the elbow crease, CH3–CH8), the wrist (1 electrode, dorsal, 2–3 cm proximal to the wrist crease, CH9), and the hand (3 electrodes, medial and lateral thenar eminence and hypothenar eminence, CH10–CH12) on their dominated arms, respectively, as illustrated in Fig. 1a. These electrodes recorded EMG signals from muscles physiologically related to arm and hand movements. For TR amputees, the 12 electrodes were divided into two electrode rings, as shown in Fig. 1b. The first ring had eight electrodes (CH1–CH8) that were uniformly placed around the proximal portion of the forearm over the apex of the muscle bulge (about 2–3 cm to the elbow crease), and the second ring had four electrodes that were uniformly positioned on the distal end (CH9–CH12). The distance between two electrode rings varied with the length of residual limb. A large circular electrode was placed on the bony portion of the elbow of the tested arm for a ground. For each patient who underwent TMR surgery (Fig. 1c), the 12 electrodes were placed on the skin over the reinnervated muscles (Fig. 1c). Four electrodes were placed at the sites of their direct-control prosthesis17,18 and the eight additional sites were determined by an electrode optimization algorithm12 that enabled the highest classification accuracy for different movements. The EMG signals were amplified and filtered with a band-pass filter of 5–500 Hz and sampled at a rate of 1 kHz by an analog-to-digital converter (USB-1616FS; Measurement Computing Corp, Norton, Massachusetts) and acquired with a Matlab-based custom data acquisition and processing system.19,20

Placement of 12 bipolar electrodes for EMG recordings. (a) The electrodes were placed on the intact arm of an able-bodied subject; (b) the electrodes were placed on the residual arm of a transradial subject; and (c) right panel shows the electrodes placed on the chest of a shoulder disarticulation subject with TMR surgery and left panel demonstrates the scheme diagram of TMR surgery in the SD subject
Ten classes of arm and hand movements plus a “no movement” class were included in the study. For able-bodied subjects and SD amputees, the 10 motion classes were elbow flexion and extension, wrist flexion and extension, wrist rotation (pronation and supination), hand open and three hand-grasp patterns (power grip, fine pinch grip, and tool grip) (Fig. 2). The elbow flexion and extension were excluded in TR amputees since their elbow function was intact. Instead, two more hand-grasp patterns, key grip and chuck grip, were added. Subjects were instructed to follow demonstrations of each motion class displayed in random order on a big TV screen and performed target movements with a comfortable and consistent level of force effort. EMG data were collected in eight consecutive trials. In each trial, all the 11 motion classes were repeated twice and held for 4 s, producing 8 s EMG recordings per motion class. There was a 3-s interval between consecutive movements in the four even-numbered trials and a variable time interval (3, 2, 0, and 1 s, in turn) in the four odd-numbered trials in order to enhance the classifier’s robustness. To avoid muscle and mental fatigue, subjects were allowed to rest for 1–5 min between trials.

Motion classes involved in the study
EMG Analysis and Movement Classification
For each motion class, the EMG data from the four odd-numbered trials were concatenated, producing 32 s of EMG recordings, and used as a training set to build a classifier; the EMG data from the four even-numbered trials were also combined together, producing 32 s of EMG recordings per movement, and used as a test set to evaluate the classification accuracy of the movement classifier. EMG pattern recognition was performed on windowed EMG data. EMG recordings from all 12 electrodes were segmented into a series of 150 ms analysis windows with a time overlap of 50 ms (the time increment was 100 ms), resulting in a new classification every 100 ms. For each movement, 32-s EMG recordings were divided into 320 analysis windows. Four generally used time-domain (T-D) features (mean absolute value, number of zero crossings, waveform length, and number of slope sign changes)14 were extracted from each analysis window as a representation of EMG signal patterns.19,20 For each analysis window, a feature set was extracted on each of the 12 channels, producing a four-dimensional feature vector (corresponding to the four T-D features). After concatenating the feature sets of all 12 channels, the entire EMG feature matrix (4 × 12 × 320) from the training set was provided to a classifier for training and the feature matrix from the test set for testing. A simple linear discriminant analysis (LDA)19,20,26,27 classifier was applied in the study for the classification of 11 motion classes. For each subject, a specific LDA classifier was built using the training data set. The performance of a trained classifier in identifying a movement was evaluated using the testing data set and measured by the classification accuracy, which is defined as:
For a subject, the classification accuracies in identifying all 11 classes of movements were averaged to calculate the overall classification accuracy.
EMG Data Re-filtering and Re-sampling
All EMG recordings were analyzed offline with Matlab (the Mathworks, Natick, MA, version 7.3). For each subject, the original EMG data that were filtered by an analog high-pass filter with a cut-off frequency of 5 Hz and acquired with a sampling rate of 1 kHz were used to evaluate classification accuracy for the 11 classes of arm and hand movements. In order to assess the influence of cut-off frequencies of a high-pass filter on the performance in classifying different movements, the original EMG data were digitally re-filtered by a high-pass filter with a gradually increasing cut-off frequency from 5 to 100 Hz with a 5-Hz increment, and then the classification accuracy was re-calculated for each new cut-off frequency. The high-pass filters were 6th order digital Butterworth filters. In addition, to evaluate the effect of a low-sampling rate on accuracy in identifying different movements, the original EMG data were re-sampled with a down sampling rate from 1000 to 100 Hz with a 20-Hz decrement, and then the accuracy for classification of different movements was estimated for each new sampling rate. In signal re-sampling process, Matlab used a proper anti-aliasing (low-pass) finite-impulse-response (FIR) filter with a cut-off frequency of the half of corresponding re-sampling rate to the original EMG data. The t test was used to assess the statistical difference between the means of compared classification accuracies, and the level of statistical significance was set to p < 0.05.
Results
Effect of High-Pass Cut-off Frequency on Classification Accuracy
The influence of different EMG high-pass cut-off frequencies on classification performance in identifying different motion classes was evaluated on able-bodied subjects and upper-limb amputees. For different cut-off frequencies, the sampling rate of EMG signals remained the same of 1 kHz. Overall classification accuracy across the 11 arm motion classes was calculated with every cut-off frequency for each subject. Figure 3 illustrates the relationship of average classification accuracy vs. high-pass cut-off frequency across five able-bodied subjects (Fig. 3a), five TR amputees (Fig. 3b), and three SD amputees (Fig. 3c), respectively. When the high-pass cut-off frequency increased from 5 to 100 Hz, the classification accuracy gradually decreased for both able-bodied subjects and TR amputees, but the reduction of classification accuracy was slight. Using a cut-off frequency of 100 Hz, the average classification accuracy was only about 0.3 and 1.4% lower in comparison with using a cut-off frequency of 5 Hz for able-bodied subjects and TR amputees. For SD amputees, it seemed that using a cut-off frequency in the range of 25–65 Hz could achieve the better performance in classifying different arm movements, but the maximum accuracy difference was only less than 0.7% when the cut-off frequency ran from 5 to 100 Hz. Compared to a 5-Hz high-pass cut-off frequency, excluding the EMG components below 60 Hz decreased the average accuracy of 0.1% (p = 0.2) in classifying the 11 movements across able-bodied subjects and increased the average accuracy of 0.1% (p = 0.5) and 0.4% (p = 0.4) among the TR and SD amputees, respectively.

Effect of EMG high-pass cut-off frequency on average classification accuracy across subjects. The values shown in the right upper corner of each figure are the range of the standard deviation (SD) of average classification accuracy from subjects. (a) Able-bodied subjects; (b) TR amputees; and (c) SD amputees with TMR surgery
Effect of Sampling Rate on Classification Accuracy
In EMG down-sampling, the high-pass cut-off frequency of EMG signals remained the same of 5 Hz. For each subject, the overall classification accuracy over all 11 arm motion classes was calculated with every sampling rate. The averaged overall accuracy was computed across each of three groups of subjects (able-bodied, TR, and SD), respectively, and is shown in Fig. 4. Although amputees achieved a lower accuracy than able-bodied subjects, all three groups of subjects had a similar trend of accuracy changing along with EMG down-sampling. It can be seen from Fig. 4 that the average classification accuracy was slowly decreasing when the sampling rate went down from 1 kHz to 400 Hz, and then was quickly going down when the sampling rate was less than 400 Hz. Down-sampling the EMG signals from 1 kHz to 400 Hz only decreased the average accuracy of about 1.2, 2.6, and 3.1% among the five able-bodied subjects, the five TR amputees and three SD amputees, respectively. Using a 500-Hz sampling rate, the average classification accuracy for the three groups of subjects only dropped around 0.7% (p = 0.2), 1.9% (p = 0.2), and 1.9% (p = 0.9), respectively, in comparison of a 1-kHz sampling rate.

Effect of EMG sampling rate on average classification accuracy across subjects. The values shown in the right upper corner of each figure are the range of the standard deviation (SD) of average classification accuracy from subjects. (a) Able-bodied subjects; (b) TR amputees; and (c) SD amputees with TMR surgery
Co-effect of Cut-off Frequency and Sampling Rate on Classification Accuracy
The simultaneous influence of high-pass cut-off frequency and sampling rate on the accuracy in classifying the 11 classes of arm movements were also investigated in the three groups of subjects. The average overall classification accuracies with six different high-pass cut-off frequencies and six sampling rates are shown in Fig. 5a for able-bodied subjects, in Fig. 5b for TR amputees, and in Fig. 5c for SD amputees. With different high-pass cut-off frequencies, the accuracy in identifying different arm movements decreased along with down-sampling of EMG signals in all three groups of subjects. For every sampling rate, different high-pass cut-off frequencies slightly affected the classification accuracy with a maximum difference of less than 2.0%. With a sampling rate of greater than 500 Hz, the similar classification accuracy could be achieved by a high-pass filter with a cut-off frequency ranging between 5 and 80 Hz in TR amputees with a maximal accuracy difference of about 1.0% and between 40 and 80 Hz in SD amputees with a maximal accuracy difference of about 0.7%. Table 1 shows the average classification accuracy for three combinations of sampling rate (f s) and high-pass cut-off frequency (f c) in three groups of subjects. Compared to (f s, f c) = (1000 Hz, 5 Hz), (f s, f c) = (500 Hz, 40 Hz), or (f s, f c) = (500 Hz, 60 Hz) decreased accuracy by 2.1 or 2.3% for TR amputees and by 1.1 or 0.4% for SD amputees. The accuracy difference between (f s, f c) = (500 Hz, 40 Hz) and (f s, f c) = (500 Hz, 60 Hz) was 0.2% for TR amputees and 0.7% for SD amputees.

Co-effect of EMG high-pass cut-off frequency and sampling rate on average classification accuracy across subjects. Every color curve corresponds to one high-pass cut-off frequency as designated by the color labels on the right side of each figure. (a) Able-bodied subjects; (b) TR amputees; and (c) SD amputees with TMR surgery
Discussion
Surface EMG is a commonly used non-invasive mean to investigate muscle electrophysiological characteristics in a large number of relevant application studies such as kinesiology, disorders of motor control, musculoskeletal rehabilitation, identifying neuromuscular diseases, and assessing low-back pain. EMG signals are also used as control signals for prosthetic devices such as prosthetic hands, arms, and lower limbs. For different studies based on EMG recordings, the frequency band of interest in EMG signals may be different. For example, some applications of EMG signals need a precise waveform analysis to get the waveform property like turns and spike amplitudes, which requires a high-sampling rate reducing the distortion of EMG waveform. In control of a multifunctional myoelectric prosthesis, we hope the EMG signal recordings to be able to provide accurate and stable motor command information for classification of intended movements. Using a higher sampling rate can acquire more myoelectric information that may increase the motion classification accuracy, but it simultaneously adds more computational and analysis complexity as well as more memory requirements to the controller of a prosthesis. In addition, while a lower high-pass cut-off frequency can retain more low-frequency components of EMG signals, it will capture more motion artifacts in EMG recordings from cable motion (1–50 Hz in frequency) or electrode motion (up to 20 Hz in frequency) that may decay the control stability of a myoelectric prosthesis in practical applications.5 In this study, we investigated the possibility and feasibility of using a low-sampling rate and a high high-pass cut-off frequency in comparison of the generally used values in EMG recordings for intentional motion recognition in control of multifunctional myoelectric prostheses.
Results from this study show that the accuracy in identifying multiple classes of arm movements could not benefit much from acquiring more low frequency components of EMG signals. The 20–100 Hz frequency-band components of EMG signals only slightly increased the classification accuracy for able-bodied subjects (about 0.25%) and TR amputees (about 1.6%). For SD amputees, the accuracy did not benefit from the EMG information below 25 Hz. This indicates that the low-frequency components in EMG recordings may provide limited useful information for the classification of different arm movements. With a widely applied high-pass cut-off frequency of 5–20 Hz in EMG recordings, this finding suggests that we can use a higher high-pass cut-off frequency to remove or reduce more low-frequency motion artefacts from EMG recordings for improving the control stability of a multifunctional myoelectric prosthesis. It is noteworthy that EMG signal recordings are always interrupted with power-line interference with a 50 Hz (or 60 Hz). Specifically, since signal-to-noise ratio (SNR) of EMG recordings in the practical application of a myoelectric prosthesis will be low, the power-line interference may overwhelm myoelectric source signals. This would greatly decrease the accuracy for classification of arm movements, which will decay myoelectric prosthetic control performance or even make the prosthesis lose control completely. The current study demonstrated that using a 50-Hz (or 60 Hz) high-pass cut-off frequency only decreased the accuracy slightly (Fig. 3b) (below 0.2%) for TR amputees and even got a high accuracy (Fig. 3c) for SD amputees in comparison of using a 20-Hz frequency. And the statistical test did not show significant difference between the classification accuracies for all three groups of subjects. The standard deviations of classification accuracy from the arm amputated subjects seemed large, but the classification accuracy in each subject had similar change trend along with the increase of high-pass filter frequency as the average accuracy shown in Fig. 3. With these results, it is feasible in EMG signal conditioning to use a 50-Hz (or 60 Hz) cut-off frequency to remove the effect of power-line interference on control performance of a multifunctional myoelectric prosthesis.
It is desired to use a low-sampling rate to save the data processing time and memory in a microprocessor-based prosthesis controller. With a generally used 1-kHz sampling frequency in EMG recordings, this study found that it is possible to use a lower sampling rate for the recognition of multiple classes of arm movements with little compromising with classification accuracy. Compared to a 1-kHz sampling rate, using a 500-Hz sampling rate can save about 50% storing memory and reduce 50% data processing time with a slight accuracy sacrifice (around 2% decrease for amputees) (Fig. 4), and the statistical test did not show significant difference between the classification accuracies for all three groups of subjects; this will greatly simplify the design and implementation of a microprocessor-based prosthetic controller. In addition, fast data processing speed may allow us to use more sophisticated pattern recognition algorithms and additional control strategies such as prosthetic adaptive control and majority vote in decision making7 to further improve the control performance of multifunctional myoelectric prostheses. Note that the classification accuracy had a big inter-subject variation among arm amputees. However, when down-sampling EMG signals from 1000 to 100 Hz, the classification accuracy in each subject had similar change trend as the average accuracy shown in Fig. 4.
Selection of high-pass cut-off frequency and sampling rate in EMG signal recordings would be the two important issues for ensuring high accuracy and stability of a multifunctional myoelectric prosthesis control as well as its implementation in practice. The results from the co-effect of both issues on the classification accuracy in this study suggested that a band-pass filter with the passband range of 60–250 Hz (corresponding to sampling rate = 500 Hz) seems to be a proper selection for conditioning of EMG signals in classifying multiple classes of arm movements. Using the combination of sampling rate and high-pass cut-off frequency of 500 and 60 Hz only resulted in about 2.3% decrease in average accuracy for TR amputees and 0.4% decrease for SD amputees in comparison of the generally used values of 1 kHz and 5 Hz. Thus, this combination does not sacrifice too much of classification accuracy which can also remove most of motion artifacts and power-line interferences for improving the performance of myoelectric prosthesis control.
Note that the classification accuracy was calculated by post-processing EMG recordings (offline) and was not a direct measure of real-time performance in clinic. Generally speaking, the low offline classification accuracy may decay the accuracy and reliability of a multifunctional prosthesis control in real time application. However, a pilot study revealed that some decrease (less than 5%) in classification accuracy could not significantly affect the real-time performance of myoelectric prosthesis control.21 This may be because the users have a visual feedback on their prosthetic manipulation and thus can voluntarily adjust their control when the prosthetic manipulation becomes a little cumbered. In addition, our previous studies on real-time prosthesis control19,20 also showed that with various offline classification accuracies (averaged 87 ± 7% for wrist movements20) among several arm amputees, they could achieve similar real-time performance in operating a virtual prosthetic wrist (for example, their motion completion rates for wrist movements were near 100%20).
It is very interesting to know that the accuracy in classifying the different arm and hand movements did not change much when the cut-off frequency of EMG high-pass filter increased from 5 to 60 Hz and the sampling rate decreased from 1000 to 500 Hz. The possible reasons underlying this funding may be that the low-frequency components of EMG signals do not provide much discriminant information for the recognition of different movements. It is well known that the lower frequency components of EMG spectrum mainly contain the information on the firing rates of active motor units, which may not be of great interest in the case of movement analysis.25 Another reason may be that the EMG T-D features used in the study may not be significantly sensitive to the low-frequency components. We are very interested in further exploring the reasons of this funding in future studies. In addition, using relatively narrow frequency-band EMG information may be able to achieve a high accuracy in classifying different arm movement in an offline case, as shown in this study, but it is unknown whether this can provide high and stable performance of multifunctional prosthesis control in practical application. This study only used the offline pattern recognition classification accuracy to evaluate the effect of EMG conditioning and sampling rate on the control performance of multifunctional prosthesis. We have developed three real-time performance measures to assess important control parameters and gain insight into the feasibility of clinically implementing EMG pattern recognition-based controllers for arm amputees.19,20 Using these real-time performance metrics, future investigations will be conducted in a real-time setting to further validate the feasibility and performance of the combination of sampling rate and cut-off frequency of 500 and 60 Hz in EMG pattern recognition-based control of a multifunctional prosthesis. It is noteworthy that traditionally, most of investigators have used able-bodied subjects to quantify EMG pattern recognition performance.1,2,6,7 This may be appropriate for a simple goal of comparing classification accuracy of different pattern recognition algorithms. The results from the present study showed again that arm amputees had very low classification accuracy in comparison to able-bodied subjects (Table 1). This requires that future investigations of real-time control performance of a multifunctional myoelectric prosthesis should use amputees as subjects who are the final users of a prosthesis.
References
Ajiboye, A. B., and R. B. Weir. A heuristic fuzzy logic approach to EMG pattern recognition for multifunctional prosthesis control. IEEE Trans. Neural Syst. Rehabil. Eng. 13(3):280–291, 2005.
Chan, A. D., and K. B. Englehart. Continuous myoelectric control for powered prostheses using hidden Markov models. IEEE Trans. Biomed. Eng. 52:121–124, 2005.
Chu, J. U., I. Moon, and M. S. Mun. A real-time EMG pattern recognition system based on linear-nonlinear feature projection for a multifunction myoelectric hand. IEEE Trans. Biomed. Eng. 53:2232–2239, 2006.
Clancy, E. A., S. Bouchard, and D. Rancourt. Estimation and application of EMG amplitude during dynamic contractions. IEEE Eng. Med. Biol. Mag. 20(6):47–54, 2001.
Clancy, E. A., E. L. Morin, and R. Merletti. Sampling, noise-reduction and amplitude estimation issues in surface electromyography. J. Electromyogr. Kinesiol. 12:1–16, 2002.
Englehart, K., and B. Hudgins. A robust, real-time control scheme for multifunction myoelectric control. IEEE Trans. Biomed. Eng. 50(7):848–854, 2003.
Englehart, K., B. Hudgins, and A. D. Chan. Continuous multifunction myoelectric control using pattern recognition. Tech. Disabil. 15(2):95–103, 2003.
Farina, D., R. Merletti, and R. M. Enoka. The extraction of neural strategies from the surface EMG. J. Appl. Physiol. 96:1486–1495, 2004.
Gallant, P. J., E. L. Morin, and L. E. Peppard. Feature-based classification of myoelectric signals using artificial neural networks. Med. Biol. Eng. Comput. 36:4485–4489, 1998.
Hargrove, L., K. Englehart, and B. Hudgins. A comparison of surface and intramuscular myoelectric signal classification. IEEE Trans. Biomed. Eng. 54:847–853, 2007.
Huang, Y. G., K. B. Englehart, B. Hudgins, and A. D. Chan. A Gaussian mixture model based classification scheme for myoelectric control of powered upper limb prostheses. IEEE Trans. Biomed. Eng. 52(11):1801–1811, 2005.
Huang, H., P. Zhou, G. Li, and T. A. Kuiken. An analysis of EMG electrode configuration for targeted muscle reinnervation based neural machine interface. IEEE Trans. Neural Syst. Rehabil. Eng. 16(1):37–45, 2008.
Huang, H., P. Zhou, G. Li, and T. A. Kuiken. Spatial filtering improves EMG classification accuracy following targeted muscle reinnervation. Ann. Biomed. Eng. 37:1849–1857, 2009.
Hudgins, B. S., P. A. Parker, and R. N. Scott. A new strategy for multi-functional myoelectric control. IEEE Trans. Biomed. Eng. 40(1):82–94, 1993.
Ives, J. C., and J. K. Wigglesworth. Sampling rate effects on surface EMG timing and amplitude measures. Clin. Biomech. 18:543–552, 2003.
Kuiken, T. A. Consideration of nerve-muscle grafts to improve the control of artificial arms. J. Technol. Disabil. 15(2):105–111, 2003.
Kuiken, T. A. Targeted reinnervation for improved prosthetic function. Phys. Med. Rehabil. Clin. N. Am. 17(1):1–13, 2006.
Kuiken, T. A., G. A. Dumanian, R. D. Lipschutz, L. A. Miller, and K. A. Stubblefield. The use of targeted muscle reinnervation for improved myoelectric prosthesis control in a bilateral shoulder disarticulation amputee. Prosthet. Orthot. Int. 28(3):245–253, 2004.
Kuiken, T. A., G. Li, B. A. Lock, R. D. Lipschutz, L. A. Miller, K. A. Stubblefield, and K. B. Englehart. Targeted muscle reinnervation for real-time myoelectric control of multifunction artificial arms. JAMA 301:619–628, 2009.
Li, G., A. E. Schultz, and T. A. Kuiken. Quantifying pattern recognition based myoelectric control of multifunctional transradial prostheses. IEEE Trans. Neural Syst. Rehabil. Eng. 18:185–192, 2010.
Lock, B. A., K. Englehart, and B. Hudgins. Real-time myoelectric control in a virtual environment to relate usability vs. accuracy. In: MyoElectric Controls Symposium, New Brunswick, Fredericton, pp. 122–127, 2005.
Parker, P. A., and R. N. Scott. Myoelectric control of prostheses. Crit. Rev. Biomed. Eng. 13(4):283–310, 1986.
Reaz, M. B. I., M. S. Hussain, and F. Mohd-Yasin. Techniques of EMG signal analysis: detection, processing, classification and applications. Biol. Proced. Online 8:11–35, 2006.
Sears, H. H. Trends in upper-extremity prosthetic development. In: Atlas of Limb Prosthetics, edited by J. H. Bowker, and J. W. Michael. St. Louis: Mosby, 1992.
Stegeman, D. F. and H. J. Hermens. Standards for surface electromyography: the European project “Surface EMG for non-invasive assessment of muscles (SENIAM),” http://www.med.uni-jena.de/motorik/pdf/stegeman.pdf, 2007.
Winter, D. A. Biomechanics and Motor Control of Human Movement. New York: Wiley Interscience, 1990.
Zhou, P., M. M. Lowery, K. B. Englehart, H. Huang, G. Li, L. Hargrove, J. P. A. Dewald, and T. A. Kuiken. Decoding a new neural machine interface for control of artificial limbs. J. Neurophysiol. 98(5):2974–2982, 2007.
Acknowledgments
The authors would like to thank Dr. Todd Kuiken at Neural Engineering Center for Artificial Limbs, Rehabilitation Institute of Chicago, USA, for supplying the raw EMG data from SD amputees for this study. This work was supported in part by the National Natural Science Foundation of China under Grant #60971076, Hong Kong Innovation and Technology Fund (ITF) #GHP/031/08, the Shenzhen Governmental Basic Research Grand #JC200903160393A, and grants from Guangdong Key Laboratory of Robotics and Intelligent System, Guangdong Province #2009A060800016 and Shenzhen Key Laboratory of Neuropsychiatric Modulation. We also thank the industrial sponsors Standard Telecommunication Ltd., Jetfly Technology Ltd., Golden Meditech Company Ltd., Bird International Ltd., Bright Steps Corporation and PCCW for their supports to the ITF project.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Thurmon E. Lockhart oversaw the review of this article.
Rights and permissions
About this article
Cite this article
Li, G., Li, Y., Yu, L. et al. Conditioning and Sampling Issues of EMG Signals in Motion Recognition of Multifunctional Myoelectric Prostheses. Ann Biomed Eng 39, 1779–1787 (2011). https://doi.org/10.1007/s10439-011-0265-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-011-0265-x