
Abstract
Goal This study tests the hypothesis of loading-dependence on the temporomandibular joint during clenching on the particular of experimentally partial edentate conditions. Methodology A complete and detailed finite element model of the temporomandibular joint (TMJ) was used. The closing movement of the mouth was reproduced by contracting the closing muscles of the masticatory system. Electromyography (EMG) data were taken from 10 healthy, dentulate volunteers, both with and without intraoral appliances. The intraoral appliances served to mimic nine partially edentulate (PE) conditions for each volunteer. The EMG data were fed into the finite element model (FEM) for each condition and the loading of the joint was analyzed. Results The results obtained show that muscular activity decreases when the contact between teeth disappears. In particular, the numerical results showed that when there is no contact between the posterior teeth an overload of the joints appeared. Moreover, the existence of a unilateral unique molar induced asymmetric overloading in the TMJ disc without posterior contact. Conclusions During clenching, a uniform distribution of the dental contact along the maxillar arches prevents the TMJ from overloading. In contrast, severe partial edentation seems to induce overloading of the TMJ with severity depending on the type of contact.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The term temporomandibular disorders (TMDs) embraces a number of analogous clinical problems, which involve pain and dysfunction of the masticatory system, the temporomandibular joint and of associated structures.25 However, controversy exists regarding the prevalence of TMD; these disorders can occur in dentates and also in edentates and partially edentates, and it has been reported that 50–70% of the population have signs of this kind of disorder at some stage during their life.4 The cause of most TMD has not yet been established,13 however, it has been reported that the likelihood of degenerative joint disease increases with higher temporomandibular joint (TMJ)-loads.18,29 Moreover, a positive association between missing mandibular posterior teeth and the presence of disk displacement was found.45 In the same line, Al-Jabrah and Al-Shumanilan1 showed that edentulous patients exhibited more TMD signs when compared with complete dentate patients.
Muscle forces may generate excessive loading on the tooth row and/or TMJs during static biting23 depending on the individual and biting location.28 Teeth contacting habit is a contributing factor to chronic pain in patients with TMD39 and is performed four times more in patients with masticatory myalgia than in controls.6 Structural changes can occur as a response to joint loads.5,48 Consequently, it is reasonable to assume that TMJ-loads are a possible etiologic cofactor of TMD and it seems interesting to evaluate TMJ-stresses from both physiology and physiopathology point of view.
Loads in the human TMJ are transferred between the articular surfaces by the TMJ disc which allows absorbing and distributing joint stresses.29 TMJ loads cannot be measured experimentally. Several FE studies have shown disc-stresses under different scenarios. For instance, large stresses appeared in the central and lateral parts of the articular discs during clenching,2,16 while the retrodiscal tissue was subjected to excessive stress in a symptomatic joint (anterior disc displacement).16 Koosltra and van Eijden20 demonstrated that joint loads increased with muscle activation. Tanne et al.44 analyzed the effect of vertical discrepancies of the craniofacial skeleton and found that the nature of stress distributions in the TMJ was substantially affected. Regarding the effect of bite point, the biomechanical reaction of the TMJ during clenching seems to be greater when the lower central incisor is restrained and the stresses and displacement of the discs were higher.27 FE studies of shortened dental arch, i.e., a dental arch with missing second molars, provided no evidence of overloading of the joint and the teeth.14 Although these authors analyzed the TMJ-loads in different occlusal conditions, there is no information about the stresses undergone by the joint discs in partial edentate (PE) patients, no withstanding the fact, that this situation is very common. The goal of this work is therefore to determine the influence on the joint-loads of different types of PE.
Materials and Methods
The following procedure was followed: a finite element model of the TMJ was obtained from one individual in a previous study32–34 from CT and MR images. Electromyography (EMG) data were taken from 10 healthy dentulate volunteers, both with and without intaoral appliances. The intraoral appliances served to mimic partially edentulate (PE) conditions for each volunteer. The EMG data were fed into a FEM for each condition. Each of these steps is described above.
Finite Element Model
A finite element model (FEM) of a healthy patient developed in previous studies was used34 (Fig. 1). The contours of the cranium (temporal bone) and the mandible were obtained from CT images and the soft tissues contours were constructed from MR images. Bones were considered to be rigid, since they are much stiffer than the relevant soft tissues. The deformable parts of the joint (the articular disc and the ligaments) were manually created from the set of images of a healthy joint. The disc and the temporomandibular ligaments were manually refined to discriminate them from the adjacent soft tissues. However, since the geometry of the collateral ligaments was difficult to identify, it was determined from the articular disc position and the shape of the bony components. The FE meshes of the disc and ligaments were constructed in I-Deas v.9 (Master Series I-Deas SDRC) using eight-node brick elements. Finally, the retrodiscal tissue was not meshed. The reconstruction of an accurate geometry for this tissue able to reproduce its main characteristics is very difficult. Thus, it was replaced by a set of springs with a similar orientation and an equivalent stiffness of 6.5 N/mm.32–34

(Left) FE model of the temporomandibular joint with details of both sides; (right) connector elements used to describe the masticatory muscles (jaw closing muscles: anterior and posterior portion of the temporal muscle, deep and superficial portions of the masseter muscle, and medial pterygoid; jaw opening muscles: lateral pterygoid and digastric)
The assumptions for the constitutive models for the soft tissues were the same as in previous works.32–35 A fiber-reinforced porohyperelastic model was used for the disc with a transversely isotropic behavior for the solid phase. Collagen fibers were oriented in the mediolateral direction in the bands and along the anteroposterior direction in the intermediate zone.3,8,35,40,43 The following strain energy function17 used in many other applications for soft tissues was considered
where c 1 characterizes the assumed Neohookean behavior of the isotropic matrix, k 1 and k 2 are related to the anisotropy introduced by the collagen fibers and D weights the tissue incompressibility. The procedure of data acquisition and model fitting were reported in Pérez del Palomar and Doblaré.32 To take into account the fact that, as the tissue compacts, its porosity and consequently its permeability decrease, a nonlinear strain dependent permeability function was also included with parameters obtained from literature.41
The disc was considered to be stress free in the initial configuration that was identified with the state without contraction of the masticatory muscles. This constitutive model for the disc was implemented as a user routine in the general-purpose finite element code ABAQUS v.6.5 (HKS inc. Pawtucket, RI, USA, 2003). This implementation is extensively discussed from a numerical point of view in Pérez del Palomar and Doblaré.35 For the ligaments, a Neo-Hookean strain energy function defined as \( \Uppsi = c_{1} (I_{1} - 3) \) was considered, motivated by the lack of data on these. The different material constants have been summarized in Table 1.32–34
Action of the Masticatory Muscles
To simulate both active and passive responses of the muscles, connector elements (Fig. 1) were used in ABAQUS. These elements allowed including a nonlinear stiffness depending on their stretching taking into account their passive resistance. In addition, these elements can exert a follower force that can reproduce the active response of the muscle. These connector elements were defined between their insertion.11,21,30 As the closing movement of the mouth was analyzed for different restraint conditions (see section “Restrictions”), the active response of the closers (from data obtained from EMG, see section “EMG activity analysis”) and the passive resistance of the openers had to be included for each case.
Passive muscle behavior was modeled by a nonlinear stress–strain relation in which the stress is related to the strain (defined as the elongation relative to the optimum length of the muscle) by the strain-dependent passive muscle stiffness. When the length of the muscle is at or below its optimum length, its passive resistance is negligible, but it increases if it is stretched beyond this length. Knowing the passive muscle stress for any length of muscle, the force due to the passive components can be computed by means of the physiological cross-sectional area (PCSA) of the muscle.31
This behavior is defined in the following way:
where ε is defined as the elongation relative to the length of the muscle at rest when it is removed from the body, l ref is its optimum length,46 S ref is the optimum length of the sarcomere (2.73 mm),47 and l free and S free are the lengths of the muscle and of the sarcomere in a free state. The values of PCSA, l free and S free which depend on the type of muscle, were obtained from Van Eijden et al.46 The remaining factors were considered constants, being k the estimated force length stiffness (k = 3.34 N/cm2) and a the passive force length asymptote (a = 0.7). Thus, passive forces were defined to be dependent on their length47 taking into account their estimated fiber and sarcomere lengths and cross-sectional area as a measure of their force capabilities.
Muscular forces were estimated by surface EMG to investigate the functional adaptation of the masticatory system of PE subjects, and were fed into a FE model.
Restrictions
There are over 65,000 possible combinations of teeth and edentulous spaces in opposing arches.24 Thus, different edentulous patterns with similar mechanical behavior were grouped in several sets. These were symmetric (0–4) and non symmetric (5–9) groups. These groups are described in Table 2. Note that group 1 corresponds to a situation in which there are not incisors and canines, this situation corresponds to the so-called mutually protected articulation.45
EMG Activity Analysis
It is widely known that jaw elevator muscle activity can be influenced by orofacial pain,10,13,15 gender,19,38 age,10 occlusion,9,26,37 and hemispheric dominance.36 Thus, full-dentate (except for the third molars), normo-occlusion, right-handed and similarly aged (18–22 years) female subjects (inclusion criteria) were the only case analyzed in this study and all of them were fitted with intraoral appliances to simulate the partial edentulous cases. Exclusion criteria included gingivitis, periodontitis, dental decay, fixed restorations that affected occlusal surfaces, clinically visible malocclusions, orthodontic therapy in the last 2 years (except passive retention), bruxism, neuropathic conditions, systemic diseases, localized maxillofacial diseases, psychological disorders, and pregnancy. According to the aforementioned criteria, 10 subjects were randomly selected from students of the Faculty of Medicine and Odontology. Informed consent was obtained from the subjects according to the guidelines of the Ethics Committee, University of Santiago de Compostela, Spain.
Bone marks were drawn on to the subjects to locate the bipolar electrodes. For the masseter muscles the electrodes were located on both sides of a line joining the tragus and the labial commisure, with the active electrode placed on the mandibular angle, over the third inferior portion of the muscle. The reference electrode was 2 cm above, just below the zygomatic process of the temporal bone. For the temporalis muscle, the reference electrode was placed over the third superior portion of the muscle belly, on a vertical passing through the tragus, while the active one was set 2 cm below, on a line joining the tragus to the active electrode. The ground surface electrode was taped below the subject’s left earlobe. After the skin was degreased (Nuprep™, D.O. Weaver and Co., Nucla Way, Au, CO, USA) and rubbed with grinding paper to reduce impedance, surface EMG signals were obtained using 10-mm bipolar gold surface electrodes (Nicolet Biomedical, Madison, WI, USA) with a 2-cm electrode distance.12 Conductive paste (Ten20™, D.O. Weaver and Co.) was applied and the electrodes were attached and secured by adhesive pads (Omnifix®, Unitex-Hartmann S.A., Mataró, Barcelona, Spain). Pairs of electrodes were connected to the Nicolet Viking IV™ electrodiagnostic system (Nicolet Biomedical) at a 200 ms time base with 200 μV to 1 mV of amplitude. Calibrated surface impedance was lower than 5 kΩ. The raw EMG signal was filtered and amplified (band pass 20–1 kHz, sampling frequency 2 kHz). The EMG recordings evaluated the muscle output during sustained maximum voluntary clenching (MVC) for 1–3 s, and were undertaken in a quiet environment at 21 °C with only the explored subject, sat on a raised comfortable position on an examination chair. Surrounding noises were controlled. One experimentally blind operator, moving as little as possible during the experiment, performed EMG recordings. Subjects were instructed to maintain a sustained maximum voluntary clenching avoiding any facial or orbicular expression.
All ten subjects received a resin intraoral appliance (splint) of the superior arch, adjusted in centric relation (CR2) in the closest position to reproduce the different partial edentulate conditions.
Firstly, EMG data were recorded for a full contact between arches, in the maximal intercuspal articulation, and the subject was invited to develop a maximum bite-force (group 0). Three EMG records of maximum voluntary clenching were obtained in each of two sessions performed in every subject to evaluate intra- and inter-sessions reproducibility.
After this, the intraoral appliance was placed in the mouth. Then, these devices were fragmented in order to modify the points of contact and to simulate different situations of partial edentulous patients (see Table 2). The EMG-activity was recorded for different experimental occlusal condition, interrupted by 4-min rest periods to avoid muscle fatigue.
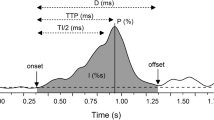
As described above, the EMG recordings evaluated the muscle output during sustained maximum voluntary clenching (MVC) for 1–3 s, and were undertaken in a quiet environment at 21 °C with only the explored subject, sat on a raised comfortable position on an examination chair. Surrounding noises were controlled. One experimentally blind operator, moving as little as possible during the experiment, performed EMG recordings. The magnitude (area, in μV × ms) of the EMG-activity was calculated after manual positioning of the cursors7 for 1 s, in the central part of 1–3-s clench; the computer use the following algorithm:
Data measurements and analysis were performed in blind conditions. General linear models for a two-way analysis of variances (ANOVA) were used when multiple comparisons were intended. Comparisons between dependent factor (EMG values) and independent ones (six for muscle locations and nine for different PE conditions) were made. When ANOVA indicated a significant difference, a Student–Newman–Keuls was carried out as post-hoc test. Statistical analysis was carried out using SPSS software. The cut-off level for significance was set at α = 0.
Results
EMG-Activity
The validity of the measurements was evaluated by computing the coefficient of variation (CV) of the EMG recordings. CVs of 0.17 and 0.21 showed an acceptable individual intra- and inter-session reproducibility.
The muscle activity for subjects during clenching in maximal natural intercuspidal position (group 0) and with the intraoral splint (group 1) was obtained. The mean clenching-EMG activity of the four jaw elevators was 522.04 ± 131.07 mV × ms. The analysis of variance for the repeated-measures showed no significant differences between all elevator jaw muscles (p = 0.38). The lower activity was recorded for both digastric muscles 107.24 ± 28.15 mV × ms, with not significant differences between both sides (p = 0.47). Electromyographic values of six locations during maximum voluntary clenching were used a reference (100%).
Different levels of EMG-activity were obtained for different partial edentulous (PE) conditions. These values are shown in percentage in Fig. 2.

(Left) Electrodes location on a control patient. Golden surface electrodes of 10 mm were used. (Right) Histogram showing the percentage of EMG-activity for the different groups. The 100% reference corresponds to the mean value of the EMG-activity during clenching in fully dentate patients with intraoral appliance placed in the mouth (groups 0 and 1, respectively). R, right; L, left; M, masseter, T, temporalis; D, digastric muscles. Asterisks indicate those variables in which a significative difference of EMG activity was found with respect to the obtained value in maximum voluntary clench in maximal intercuspidal position and/or with intraoral appliance, i.e., 0 and 1 groups (confidence label 95%)
When a symmetric contact at the anterior part was introduced, the EMG activity of the elevator muscles decreased significantly. The masseters showed a lower activity (30%) while the temporalis exhibited a lower reduction (60%) when the contact was only between the central incisors (group 2). Contact between canine teeth caused a reduction of the elevators activity that was higher in the anterior temporalis (59%) than in the masseters (80%).
Besides, the presence of some posterior teeth at both sides or a complete posterior side (premolars and molars) seemed to be enough to hold the muscle activity up to 80% of the muscle activity recorded during clenching (groups 4–7). Contact restricted to only one tooth (canine or molar) provoked a reduction of the activity of the elevators of 50%.
The activity of the digastric muscles was 20% of the one produced during clenching. In addition, their activity did not change when the number of contacts during clenching was limited; however, the contact of only one molar provoked a significant reduction of the electromyographic activity (10%, group 9).
Finite Element Results
In Figs. 3 and 4 the maximum and minimum principal stresses that appeared in both articular discs during clenching incorporating the previously described restrictions are shown. It can be seen how clenching with total dentition provoked minimal loads to the TMJ (groups 0 and 1). In contrast, the most unfavorable situation for the joint seemed to be the absence of all the teeth except from the incisors. It can be seen how in group 2 the stresses are ten times higher than those for fully dentate. Besides, it was obtained that a bilateral contact between canine teeth (group 3) doubled the TMJ stresses. Furthermore, the limitation of the contact to the first molar bilaterally (group 4) also increased the loads in the TMJ.

Comparison of the maximum principal stresses in compression in both articular discs for the different situations analyzed

Comparison of the maximum principal stresses in tension in both articular discs for the different situations analyzed
The lack of only one side of the posterior section caused an increase in the stresses in the contralateral disc and also, but in a lower intensity, in the ipsilateral (groups 5 and 6). It was also obtained that when one lateral section remained (group 7), the loads increased in the contralateral disc protecting the ipsilateral one. Regarding group 8, the contact between only one canine caused overloading at both joints, but significantly higher at the contralateral disc. Finally, when only one molar contact was present, both discs were subjected to overloading, being higher at the opposite side of the teeth.
These results can also be seen in Fig. 5 where the stress distributions in the discs for the nine cases have been plotted.

Distribution of maximum and minimum principal stresses in both discs (coronal view) for the different cases analyzed. The numbers indicate the group. A, anterior part; P, posterior; M, medial; and L, lateral
In general, the distribution and the intensity of the stresses at the discs exhibited an almost symmetric behavior in the symmetric dentate situations and an unequal response in asymmetric conditions. As the posterior contacts reduced, higher overloads were obtained in the articular disc at the contralateral side of the contact.
Discussion
Aims and Justification
The interest for this work comes from previous works18,29 reporting that overloading of the TMJs increases the risk of TMDs. Consequently, it is reasonable to assume that TMJ-loads are a possible etiologic cofactor of TMD. In this study, the influence of edentulous situations on the joint-loading was analyzed.
It is known that body tries to prevent the tissues from damage. This is the case of patients who have lost some teeth, in those cases, the elevator muscles seem to activate in a different way to avoid damage. By means of surface EMG the muscle behavior under different conditions can be analyzed. In fact, the muscle activity obeys the principle of protection of the structures, reducing its activity and therefore the load. In this way, we have performed an electromyographic study of muscle adaptation to different restraints using a finite element model to compare the load absorbed by the articular discs in each case.
EMG-Activity
One of the most important results of this work was that a limited contact between incisors gave rise to a significant reduction of the EMG activity, which was higher for the masseters. This effect can be related to the protection of these teeth and/or the TMJs. These teeth, far from the mandibular insertion of the masseters, present a large fulcrum and therefore it seems reasonable to obtain a reduction of their forces, leading to a smaller fulcrum for the TMJ which should absorb more loads when contracting the masseters. This is the behavior that seems to obey fulcrum laws of type III: support points at the incisors, force at the goniac angle and mandibular body, and stiffness of both joints. The same behavior occurred when the contact was established between the canine teeth although the arm of the fulcrum of the tooth to the force application point was in this case shorter. Remember that normally, the muscular forces are directed to tooth row and forces are not expected through the TMJs.
However, when the contact was established between both sides, the activity was similar to the one in called mutually protected articulation.45 Amazingly, this behavior persisted when the occlusion appeared unilaterally in a posterior section (group 7) in which it seems reasonable to obtain a reduction of the activity of the elevator muscles in the side where there was no contact, since the lack of them suggests the redistribution of the loads in the edentulous side joint. Finally, the contact of only one canine tooth, provoked a significant reduction of the muscle activity, approximately of 50% reduction comparing to the mutually protected articulation, suggesting a protecting mechanism which also occurred when the contact was located only in one molar.
Finite Element Study
Clenching with contacts in mutually protected articulation caused minimal loads at the TMJs. Due to the maximum muscle activity during this task, it seems reasonable to obtain the highest force to the tooth row. It was obtained that the situation in which the highest overloads occurred corresponded to the restriction of the incisors. Although the effect of fulcrum of Type III should be minimized due to the high reduction of EMG activity, both TMJ were overloaded. The proximity of the TMJs to the masseter, as well as the direction of these muscles with respect to the distance to the incisors could explain this behavior.
Although, for group 3 (in which the canine teeth are restrained) the same behavior would be reasonable, it was obtained that the stresses at both discs increased only slightly. This fact could be explained not only by the nature of these teeth since the adaptation of the muscle activity is similar to the previous case, but due to the proximity to the masseters insertion. This fact suggests higher loads in these teeth than in the incisors. This group (3) is especially interesting because it represents the most common partial edentulous situation.22
The bilateral restriction between molars (group 4) caused a significant increase of the stresses. It is possible that the lack of equilibrium of one tooth in each side, does not allow guiding properly the force vectors.
Groups 5 and 6 showed an increase of the stresses in the side where there is not posterior contact, as it could be expected. However, the presence of a premolar in that side seems to reduce the stresses significantly, in contrast to what happened in Case 7 as we will see later.
Group 7 which corresponds to the situation where only the posterior teeth of one side were present, provoked overloading in the contralateral TMJ. This behavior shows the inability of the neuromuscular system to achieve a reduction of the muscular activity in the edentulous side. This fact seems to reinforce the clinical evidence of partial edentulous patients that suffer from a TMD, to whom a reposition of the lost teeth is usually suggested.
Contact between only one canine (group 8) produced higher loads at the contralateral side. This seems to be related with the developing of unilateral disorders. The restriction of only one molar provoked an overload in both joints, but higher in the contralateral side.
Thus, it has been shown that edentulous situations or a sudden restoration of teeth, as well as, parafunctionals habit of biting with specific teeth, could contribute to develop pathologies of the TMJ at the contralateral side of the contact.
Limitations of the Study
In this study, the pterygoid muscles which are more inaccessible were not explored. Nevertheless, only the medial pterygoid muscle acts as elevator and it behaves similarly to the masseter muscle, so a similar response for these muscles was assumed.
Another limitation of this study corresponds to the noninclusion of the adaptation system when a patient looses a portion of his/her teeth. However, it is known that recent exodontias or orthodontic procedures can lead to pain in the TMJ in a really short period of time.
Furthermore, every partial edentulous situation in a real patient was not evaluated, but the selection of the nine groups presented here was based on Kennedy concepts about PE.24
Another limitation of the study is that it has been performed under CR occlusion conditions. In this scenario the splints were fitted and the finite element simulations were made. In fact, clenching in human is more complex since several adjustments and jaw movements are also performed. The study assumes that muscular activity was similar in experimentally partial edentates than in real partial edentates; however, some functional adaptation of the muscular activity can appear in a chronic partially edentulate.
Some assumptions were also made for the FE modeling regarding the geometry and the material properties of the tissues involved. The ligaments were considered to be isotropic hyperelastic, although they should have been considered as prestressed transversely isotropic materials since they are composed of fibers oriented along their longitudinal direction. As far as the authors know there are no experimental measurements of the strain distributions in these elements. Moreover, the mechanical properties of these ligaments are not available. Therefore, average values for their stiffness were considered and a simplification of their behavior was used.35 With respect to the modeling of the retrodiscal tissue a somewhat rough approximation was used. This tissue was replaced by an equivalent set of springs, since the goal of this study was to analyze the response of the disc and not of the retrodiscal tissue itself.
The present model enables the analysis of the stresses in the articular discs controlled by muscle tensions. It is clear that a more accurate description of the elements of the joint would probably modify the magnitude of the stresses obtained, but we consider that the present work is a good qualitative tool to predict the response of the soft tissues in the joint under different loading conditions, taking into account different restrictions of the movement of the mandible, and could be used to analyze muscle activity adaptation to mastication restrictions, occlusal defects or diseased discs.
Conclusion
In conclusion, during clenching, the physiologic dental contacts distributed along the arches protect the TMJs from loading. It was obtained that punctual contacts in specific teeth or the lack of posterior teeth both unilateral and bilaterally caused loading of the joints. In addition, under asymmetric occlusal conditions, the loads increased more significantly in the side where the posterior teeth were lost.
References
Al-Jabrah O., Al-Shumailan Y. R. 2006. Prevalence of themporomandibular disorder signs in patines with complete versus partial dentures. Clinical Oral Investigations 10(3):167–173
Beek M., Koolstra J. H., van Ruijven L. J., van Eijden T. M. 2000. Three-dimensional finite element análisis of the human temporomandibular joint disc. J Biomech 33(3):307–16
Berkovitz B. K. B. 2000. Collagen crimping in the intra-articular disc and articular surfaces of the human temporomandibular joint. Arch Oral Biol 45:749–756
Carlsson G. E. 1999. Epidemiology and treatment need for temporomandibular disorders. J Orofac Pain 13(4):232–7
Carvalho R. S., Yen E. H., Suga D. M. 1995. Glycosaminoglycan synthesis in the rat articular disk in response to mechanical stress. Am J Orthod Dentofacial Orthop 107(4):401–10
Chen C.-Y., Palla S., Erni S., Sieber M., Gallo L. M. 2007 Nonfunctinal toot contact in healthy controls and patients with myogenous facial pain. J Orofac Pain 21:185–193
Chung J. W., Kim C., McCall Jr W. D. 2002. Effect of sustained contraction on motor unit action potentials and EMG power spectrum of human masticatory muscles. J Dent Res 81(9):646–649
Detamore M. S., Athanasiou K. A. 2003 Tensile properties of the porcine temporomandibular joint disc. J Biomech Eng 125(4): 558–65
Ferrario V. F., Tartaglia G. M., Galletta A., Grassi G. P., Sforza C. 2006. The influence of occlusion on jaw and neck muscle activity: a surface EMG study in healthy young adults. J Oral Rehabil 33(5):341–348
Fogle L. L., Glaros A. G. 1995. Contributions of facial morphology, age, and gender to EMG activity under biting and resting conditions: a canonical correlation analysis. J Dent Res 74:1496–1500
Gal J. A., Gallo L. M., Palla S., Murray G., Klineberg I. 2004. Analysis of human mandibular mechanics based on screw theory, in vivo data. J Biomech 37:1405–1412
Gallo L. L., Gross S. S., Palla S. 1999. Nocturnal masseter EMG activity of healthy subjects in a natural environment. J Dent Res 78(8):1436–1444
Greene, C. S. Concepts of TMD etiology: effects on diagnosis and treatment. In: TMDs An Evidence-Based Approach to Diagnosis and Treatment, edited by D. M. Laskin, C. S. Greene, and W. L. Hylander. Quintessence Publishing Co, Inc., 2006.
Hattori Y., Satoh C., Seki S., Watanabe Y., Ogino Y., Watanabe W. 2003. Occlusal and TMJ loads in subjects with experimentally shortened arches. J Dent Res 82(7):532–536
Helkimo N., Ingervall B., Carlsson G. E. 1975. Comparison of different methods in active and passive recording of the retruded position of the mandible, Scand J Dent Res 81:265–271
Hirose M., Tanaka E., Tanaka M., Fujita R., Kuroda Y., Yamano E., van Eijden T. M., Tanne K. 2006. Three-dimensional finite-element model of the human temporomandibular joint disc during prolonged clenching. Eur J Oral Sci 114(5):441–8
Holzapfel G. A. 1998. Nonlinear Solid Mechanics. Wiley, New York
Iwasaki L. R., Nickel J. C., McLachlan K. R. 1997. Relationship between growth, function, and stress in the temporomandibular joint. In: McNeill C (eds) Science and practice of occlusion. Quintessence, Chicago, pp. 125–136
Johansson A., Unell L., Carlsson G. E., Söderfelt B., Halling A. 2003. Gender difference in symptoms related to temporomandibular disorders in a population of 50-year-old subjects. J Orofac Pain 17(1):29–35
Koolstra J., Van Eijden T. M. G. J. 2005. Combined finite element and rigid body analysis of human jaw joint dynamics. J Biomech 38(2): 2431–9
Langenbach G. E. J., Hannam A. G. 1999. The role of passive muscle tensions in a three-dimensional dynamic model of the human joint. Arch Oral Biol 44:557–573
Marcus, S. E., T. F. Drury, L. J. Brown, and G. R. Zion. Tooth retention and tooth loss in the permanent dentition of adults: United Status, 1988–1991. J. Dent. Res. Feb; 75 Spec No:684–695, 1996.
May B. M., Garabadian C. 2000. Reducing condylar compression in clenching patients. Crit. Rev. Biomed. Eng, 28(3–4):389–94
McGivnet G. P., Castleberry D. J. 1995. McCracken’s Removable Partial Prosthodontics, 9th edition. Mosby-Year Book, Inc.St.Louis, MI. pp 17–23
McNeill C., Mohl N. D., RTanatan T. T. 1990. Temporomandibular disorders: diagnosis, management, education and research. J Am Dent Assoc 120:252–263
Møller E, Bakke M. 1988. Occlusal harmony and disharmony: frauds in clinical dentistry? Int Dent J. 38(1):7–18
Nagahara K, Murata S, Nakamura S, Tsuchiya T. 1999. Displacement and stress distribution in the temporomandibular joint during clenching. Angle Orthod 69(4):372–9
Nickel J. C., McLachlan K. R. 1994. In vitro measurement of the stressdistribution properties of the pig temporomandibular joint disc. Arch Oral Biol 39:439–448
Nitzan D. W. 2001. The process of lubrication impairment and its involvement in temporomandibular joint disc displacement: a theoretical concept. J Oral Maxillofac Surg 59:36–45
Peck C., Langenbach G., Hannam A. 2000. Dynamic simulation of muscle and articular properties during human wide jaw opening. Arch Oral Biol 45:963–982
Peck C., Murray G., Johnson C., Klineberg I. 1999. Trajectories of condylar points during nonworking side and protrusive movements of the mandible. J Prosthet Dent 82:322–331
Pérez del Palomar A., Doblaré M. 2006. The effect of collagen reinforcement in the behaviour of the temporomandibular joint. J Biomech 39(6): 1075–1085
Pérez del Palomar A., Doblaré M. 2006. Finite element analysis of the temporomandibular joint during lateral excursions of the mandible. J Biomech 39(12): 2153–2163
Pérez del Palomar A., Doblaré M. 2006. 3D finite element simulation of the opening movement of the mandible in healthy and pathologic situations. J Biomech Eng. ASME; 128(2): 242–249
Pérez del Palomar A., Doblaré M. 2006. On the numerical simulation of the behaviour of articular cartilage. Int J Num Meth Eng 67(9): 1244–271
Pirttiniemi P. 1998. Normal and increased functional asymmetries in the craniofacial area. Acta Odontol Scand 56(6):342–345
Racich M. J. 2005. Orofacial pain and occlusion: Is there a link? An overview of current concepts and the clinical implications. J Prosthet Dent 93:189–96
Sarlani E., Greenspan J. D. 2005. Why look in the brain for answers to temporomandibular pain? Cells, Tissues, Organs, 180:69–75
Sato F., Kino K, Sugisaki M., et al. 2006. Teeth contacting habit as a contributing factor to chronic pain in patients with temporomandibular disorders. J Med Dent Sci, 53:103–109
Scapino R. P., Obrez A., Gresing D. 2006. Organization and function of the collagen fiber system in the human temporomandibular joint disk and its attachments. Cells Tissues Organs 182(34): 202–225
Shengyi T., Yinghua X. 1991. Biomechanical Properties and Collagen Fiber Orientation of TMJ Discs in Dogs: Part I. Gross Anatomy and collagen fiber orientation of the Discs. J Craniomand Disord, 5:28–34
Svensson P., Wang K., Sessle B. J., Arendt-Nielsen L. 2004. Associations between pain and neuromuscular activity in the human jaw and neck muscles. Pain 109:225–232
Tallents Tallents R. H., Macher D. J., Kyrkanides S., Katzberg R. W., Moss M. E. 2002. Prevalence of missing posterior teeth and intraarticular temporomandibular disorders. J Prosthet Dent 87(1):45–50
Tanne K., Tanaka E., Sakuda M. 1995. Stress distribution in the TMJ during clenching in patients with vertical discrepancies of the craniofacial complex. J Orof Pain 9(2): 153–160
The Academy of Prosthodontics. 2005. The Glossary of Prosthodontic Terms. J Prosthet Dent 94(1):10–92
van Eijden T. M. G. J., Korfage J. A. M., Brugman P. 1997. Architecture of the Human Jaw-closing and Jaw-opening muscles. Anat Rec, 248:464–474
van Ruijven L. J., Weijs W. A. 1990. A new model for calculating muscle forces from electromyograms. Eur J Appl Physiol, 61:479–485
Wong M., Carter D. R. 2003. Articular cartilage functional histomorphology and mechanobiology: a research perspective. Bone 33:1–13
Acknowledgments
The authors thanks to Prof. Otero Cepeda from the Statistics Department of Santiago de Compostela University for his support in the statistical part. The authors gratefully acknowledge the support of the Spanish Ministry of Education and Research through the research project DPI2006-14669.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pérez del Palomar, A., Santana-Penín, U., Mora-Bermúdez, M.J. et al. Clenching TMJs-Loads Increases in Partial Edentates: A 3D Finite Element Study. Ann Biomed Eng 36, 1014–1023 (2008). https://doi.org/10.1007/s10439-008-9487-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-008-9487-y