
Abstract
Burning landscapes under controlled conditions to reduce the risk of wildfires is a controversial land management practice. The health risks of smoke generated from controlled burning relative to wildfire remain uncertain. Recent work in the Australian monsoon tropics provided a unique opportunity to study the health effects of smoke pollution at and well below national air quality standards. It found that for each increase in the atmospheric mass of particles 10 μg or less in aerodynamic diameter (PM10) per cubic meter of air per 24-hour period, there was a 26% increase in daily asthma presentations to the emergency department of the Royal Darwin Hospital, with an apparent threshold at 40 μg/m3 PM10 (lower than the Australian PM10 air quality standard of 50 μg/m3). This finding was unaffected by adjusting for weekly rates of influenza, weekday vs. weekends, and school holiday periods. Although further research is being undertaken to substantiate these findings, the upshot of the study suggests that for airsheds containing large human populations, fire managers should strive to keep smoke pollution less than 40 μg/m3 PM10.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Wildfire management involves many ecologic and social trade-offs (Gonzalez-Caban, 1997). Burning landscapes under controlled conditions to reduce fuel loads and, thereby, to minimize the frequency and severity of wildfires is a controversial type of landscape management. A particularly problematic aspect of this land management intervention concerns the health effects of smoke pollution from frequent, controlled landscape fires vs. severe smoke pollution from infrequent, uncontrolled wildfires (Schwela, 2001; Lewis and Corbett, 2002; Sim, 2002). It has been recently suggested that particulates derived from wood smoke might be more injurious to human health (Boman et al., 2003) than particulates derived from other sources that are also known to cause ill health (Vedal and McClellan, 2002; Katsouyanni, 2003). Despite this knowledge base, there is a rudimentary understanding of the health effects of wildfire smoke on human health (Table 1). Consequently, land managers and health professionals are operating in a policy vacuum with little to guide them beyond existing national air quality standards. For example, the U.S. Environmental Protection Agency (1998) produced an interim policy for the management of wildfire management that promoted the “thoughtful use of fire by all wildland owners and managers while mitigating the impacts of emissions on air quality and visibility.” In this context, the work of Johnston et al. (2002a) is very significant to the ongoing policy debate concerning fire management and air quality because, unlike all previous studies, they were able to study the effect of a wide range of smoke pollution levels at and well below national air quality standards.
TEMPORAL PATTERNS IN ASTHMAAND WILDFIRE SMOKE
Johnston et al. (2002a) undertook a correlative analysis of atmospheric pollution and asthma in the isolated coastal tropical city of Darwin, situated in the vast savannas of the Australian monsoon tropics (Fig. 1). The study was conducted during the 7-month rain-free dry season in 2000. There are a number of advantages for the study of human health effects of wildfire smoke in Darwin: 1) there is no significant source of atmospheric air pollution other than particulates derived from wildfires (CSIRO Atmospheric Research, 2001); 2) during the dry season, the lower atmosphere is stable, with little convective mixing and a persistent inversion at approximately 3000 m (Kondo et al., 2003), allowing reliability of exposure measurement within the geographic area (CSIRO Atmospheric Research, 2001); 3) there is a small population of approximately 115,000 and a single major hospital that has systematic data collection systems in place; and 4) wildfires occur in the Darwin region throughout every dry season (e.g., Edwards et al., 2001), thereby providing a continuous background of smoke pollution with peaks and troughs over several months.

The location of the Australian city of Darwin and other regional population centers. Also shown is the extent of the urban area within Darwin and the location of the university and the meteorology station where PM10 (atmospheric mass of particles 10 μg or less in aerodynamic diameter per cubic meter of air) levels were measured. PM10 loadings were continuously measured by using a tapered element oscillating mass balance at the university, and gravimetric mass loadings were measured at the meteorology station. Determinations from the two sites were highly correlated (r = 0.89; CSIRO Atmospheric Research, 2001).
Smoke pollution was measured as PM10 (atmospheric mass of particles 10 μg or less in aerodynamic diameter per cubic meter of air) averaged over a 24-hour period at two locations within the city of Darwin; this provided a reliable measure of exposure of the city’s population (Fig. 1). For each day of the study, the number of asthma presentations to the emergency department of the Royal Darwin Hospital was determined by interrogating the electronic emergency department register, which was coded according to a subset of the International Classification of Diseases, version 9, codebook. The two codes used for asthma presentations were 493.00 (childhood asthma) and 493.9 (asthma not elsewhere classified), which was used to code all types of adult asthma.
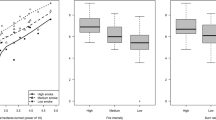
Johnston et al. (2002a, b) demonstrated a significant relationship of asthma presentations with increasing PM10 concentrations by using negative binomial regression and controlling for potential confounders known to be coincident with fire activity and potentially influencing asthma presentations to hospital, including weekend and holiday periods and the incidence of influenza-like illness, a well-known precipitant of asthma (Cohen and Castro, 2003). They showed that when the PM10 data were analyzed as a continuous variable, there was a significant increase in asthma presentations with each 10 μg/m3 increase in PM10. However, when the PM10 data were aggregated into 10 μg/m3 PM10 classes, the modeling revealed a threshold at 40 μg/m3, where the risk of asthma increased 2.6 times relative to the baseline category of less than 10 μg/m3 (Table 2).
Time series has been the predominant and orthodox approach for longitudinal studies of air pollution at a number of urban loci and is used to overcome the effects of autocorrelation due to seasonality, weather fluctuations, and long-term trends or cycles (Jalaludin et al., 2002). Reanalysis of Johnston and associates’ original data to test for temporal autocorrelation (by using autoregressive integrated moving average autoregressive integrated moving average (ARIMA) modeling) indicated that their original analysis was robust: there was no evidence of temporal autocorrelation in asthma presentations or any obvious trend or cycle in the data (Fig. 2).

Daily asthma presentations to the emergency department of the Royal Darwin Hospital and 24-hour mean concentration of atmospheric particles (PM10) measured at two locations in the city of Darwin from April 1 to October 31, 2000. With autoregressive integrated moving average (ARIMA) analysis, the highest partial autocorrelation coefficient for asthma presentations was 0.13 at 1 day, with no trends or cycles in the data. The mean daily PM10 for the entire study period was 20.84 μg/m3, and it ranged from 2.0 to 70.0 μg/m3. The observed PM10 levels are representative of the regional setting, because Vanderzalm et al. (2003) found similar levels of carbon particles at Jabiru (Fig. 1) in the dry season of 1996.
THE NEXUS BETWEEN HUMAN ANDL ANDSCAPE HEALTH
A manifestation of global environmental change is the worldwide increase in the severity and frequency of wildfires (Schwela, 2001). Because of the effects of wildfires on human populations, there is an increasing need to consider this problem in a holistic manner, including understanding the effect of both wildfires and prescribed fires on human health and landscape ecology. Demonstrating a health effect of wildfires presents numerous practical and technical challenges because of the infrequency of fire events and the large number of potential confounders that make it difficult to distinguish the epidemiologic “signal” from the background “noise.”
The Johnston et al. (2002a) study represents an advance in this field because it examined temporal variation in smoke pollution over 7 months of continuous exposure rather than using a more usual retrospective design comparing an unexpected fire event with an “equivalent” period without wildfire (Table 1). The finding that asthma hospital presentation more than doubled at more than 40 μg/m3 PM10 is potentially of great significance for fire management, because this is below currently accepted Australian air quality standards (i.e., <50 μg/m3 PM10). Furthermore, this threshold was rarely exceeded by fires in the early and mid dry season, most of which were deliberately lit to reduce fuel loads. This observation lends support to the idea that well-managed controlled burning programs may, for asthma, have negligible public health effects relative to uncontrolled fires that cause severe pollution (Table 1).
It must be stressed that the 40 μg/m3 PM10 threshold detected by Johnston et al. (2002a) may be a statistical anomaly, given that it is inconsistent with previous studies of health effects of particulates. To resolve this question, we are exploiting the unique opportunity presented by Darwin to undertake a more comprehensive epidemiologic study of the associations between wildfire smoke and health. This study includes measures of particulate pollution measured as PM10 and PM2.5, spores and pollens, meteorologic conditions, day of the week, and school holiday time periods. In contrast to previous study designs, we are examining multiple health outcomes, including tracking the response of a cohort of patients with asthma to varying levels of wildfire smoke exposure by recording their daily symptoms, medication use, and health service attendances for asthma. Additionally, for the city of Darwin, we are tracking hospital attendances for heart and lung diseases (including asthma, chronic obstructive pulmonary disease, and ischemic heart disease) and family physician presentations for rhinitis and flu-like illness. To understand the interactive effect of meteorologic conditions and the geographic location of fires on smoke pollution levels in Darwin, we are undertaking landscape ecology studies by using moderate resolution imaging spectroradiometer satellite imagery to locate active wildfires and by using a geographic information system and dynamic atmospheric modeling to map smoke dispersion from them (Draxler and Hess, 1998). Such ambitious joint landscape ecology and epidemiologic perspectives are crucial in the quest for sustainable fire management practices for a variety of reasons, including building a bridge between the presently segregated professions of fire management and public health; providing urban dwellers with a direct stake in fire management; and providing specific, evidence-based, and measurable air quality targets for fire managers.
References
BC Boman AB Forsberg BG Jarvholm (2003) ArticleTitleAdverse health effects from ambient air pollution in relation to residential wood combustion in modern society Scandinavian Journal of Work, Environment and Health 29 251–260 Occurrence Handle1:CAS:528:DC%2BD3sXnt1GitLs%3D
InstitutionalAuthorNameCenters for Disease Control and Prevention (1999) ArticleTitleSurveillance of morbidity during wildfires—Central Florida, 1998 Morbidity and Mortality Weekly. Review 48 78–79
T Churches S Corbett (1991) ArticleTitleAsthma and air pollution in Sydney NSW Public Health Bulletin 8 72–73
L Cohen M Castro (2003) ArticleTitleThe role of viral respiratory infections in the pathogenesis and exacerbation of asthma Seminars in Respiratory Infection 1 3–8
C Cooper M Mira M Danforth K Abraham B Fasher P Bolton (1994) ArticleTitleAcute exacerbations of asthma and bushfires Lancet 343 1509 Occurrence Handle1:STN:280:DyaK2c3mtVyhsw%3D%3D
CSIRO Atmospheric Research (2001) A Pilot Study of Air Quality in Darwin NT, Darwin, Australia: Northern Territory Government Department of Lands Planning and Environment. Available: http://www.lpe.nt.gov.au/enviro/wmpcreg/AirQ/AQStudy/AQStudy.pdf [accessed 2 August 2004]
RR Draxler GD Hess (1998) ArticleTitleAn overview of the Hysplit_4 modeling system for trajectories, dispersion, and deposition Australian Meteorological Magazine 47 295–308
P Duclos LM Sanderson M Lipsett (1990) ArticleTitleThe 1987 forest fire disaster in California: assessment of emergency room visits Archives of Environmental Health 45 53–58 Occurrence Handle1:STN:280:DyaK3c7pslaqsg%3D%3D Occurrence Handle2180383 Occurrence Handle10.1080/00039896.1990.9935925
A Edwards P Hauser M Anderson J McCartney M Armstrong R Thackway et al. (2001) ArticleTitleA tale of two parks: contemporary fire regimes of Litchfield and Nitmiluk National Parks, monsoonal northern Australia International Journal of Wildland Fire 10 79–89
SC Emmanuel (2000) ArticleTitleImpact to lung health of haze from forest fires: the Singapore experience Respirology 5 175–182 Occurrence Handle10.1046/j.1440-1843.2000.00247.x Occurrence Handle1:STN:280:DC%2BD3M3pvFOmtQ%3D%3D Occurrence Handle10894108
InstitutionalAuthorNameEnvironmental Protection Agency (1998) USEPA Interim Air Quality Policy on Wildland and Prescribed Fires U.S. Environmental Protection Agency Washington, DC
A Gonzalez-Caban (1997) ArticleTitleManagerial and institutional factors affect prescribed burning costs Forest Science 43 535–543
B Jalaludin GB Marks GG Morgan (2002) ArticleTitleSerial correlation and confounders in time-series air pollution studies Medical Journal of Australia 177 397
B Jalaludin M Smith B O’Toole S Leeder (2000) ArticleTitleAcute effects of bushfires on peak expiratory flow rates in children with wheeze: a time series analysis Australian and New Zealand Journal of Public Health 42 174–177
F Johnston A Kavanagh D Bowman R Scott (2002a) ArticleTitleBushfire smoke and asthma: an ecological study Medical Journal of Australia 176 535–538
F Johnston A Kavanagh D Bowman R Scott (2002b) ArticleTitleSerial correlation and confounders in time-series in air pollution studies Medical Journal of Australia 177 397–398
K Katsouyanni (2003) ArticleTitleAmbient air pollution and health British Medical Bulletin 8 143–156
Y Kondo N Takegawa Y Miyazaki M Ko M Koike K Kita et al. (2003) ArticleTitleEffects of biomass burning and lightning on atmospheric chemistry over Australia and South-east Asia International Journal of Wildland Fire 12 271–281
P Lewis S Corbett (2002) ArticleTitleBushfires, air pollution and asthma Medical Journal of Australia 176 517
JA Mott CJ Alverson DM Mannino A Kiyu J Hashim K Falter et al. (2003) ArticleTitleThe 1997 Malaysian forest fires: respiratory hospitalizations in persons with a history of chronic obstructive pulmonary disease American Journal of Respiratory and Critical Care Medicine 167 A498
JA Mott P Meyer D Mannino SC Redd EM Smith C Gotway-Crawford et al. (2002) ArticleTitleWildland forest fire smoke: health effects and intervention evaluation, Hoopa, California, 1999 Western Journal of Medicine 176 162–163
N Sastry (2002) ArticleTitleForest fires, air pollution, and mortality in Southeast Asia Demography 39 1–23
D Schusterman ZZ Kaplan C Canabarro (1993) ArticleTitleImmediate health effects of an urban wildfire Western Journal of Medicine 158 133–138
D Schwela (2001) ArticleTitleFire disasters: the WHO-UNEP-WMO health guidelines for vegetation fire events Annals of Burns and Fire Disasters 13 178–179
M Sim (2002) ArticleTitleBushfires: are we doing enough to reduce the human impact? Occupational and Environmental Medicine 59 215–216 Occurrence Handle1:STN:280:DC%2BD383gt1alsg%3D%3D
MA Smith B Jalaludin JE Byles L Lim SR Leeder (1996) ArticleTitleAsthma presentations to emergency departments in western Sydney during the January 1994 bushfires International Journal of Epidemiology 25 1227–1236 Occurrence Handle1:STN:280:DyaK2s7nvFansQ%3D%3D
JL Vanderzalm M Hooper B Ryan W Maenhaut P Martin PR Rayment et al. (2003) ArticleTitleImpact of seasonal biomass burning on air quality in the ‘top end’ of regional Northern Australia Clean Air and Environmental Quality 37 28–33
S Vedal RO McClellan (2002) ArticleTitleUpdate on the health effects of outdoor air pollution—setting ambient air quality standards for particulate matter Clinical Chest Medicine 23 763–775
Acknowledgments
We are grateful to Barry Brook, who ran and interpreted the time series analyses. We acknowledge support for our current study of the epidemiology of wildfire smoke pollution from the Bureau of Meteorology, the Northern Government Department of Health and Community Services, the Department of Infrastructure, Planning and Environment, the Department of Business and Resource Development, and the Australian Research Council.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bowman, D.M., Johnston, F.H. Wildfire Smoke, Fire Management, and Human Health. EcoHealth 2, 76–80 (2005). https://doi.org/10.1007/s10393-004-0149-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10393-004-0149-8