
Abstract
Background
The incidence rates of cutaneous melanoma have been increasing in Canada over the past decades. This study aimed to quantify and assess trends in education- and income-related inequalities in the incidence of cutaneous melanoma in Canada (excluding territories) from 1992 to 2010.
Methods
Data for the analyses were obtained from the Canadian Cancer Registry (CCR), the Canadian Census of Population (CCP), and the National Household Survey (NHS). The concentration index (C) approach was used to quantify income- and education-related inequalities in the incidence rates of cutaneous melanoma. Trend analyses were performed to evaluate changes in inequalities over the study period.
Results
Incidence rates of cutaneous melanoma increased across Canada from 1992 to 2010. The age-adjusted value of C showed a greater concentration of cutaneous melanoma amongst Canadians with higher incomes. Although the age-adjusted value of C did not suggest a significant education-related inequality in the incidence rates, the trend analyses indicate that, with time, incidence rates are becoming more concentrated amongst both males and females with lower levels of education.
Conclusions
Incidence rates of melanoma are rising across Canada and are higher amongst individuals with higher income. Our analyses suggest that incidence rates of melanoma are becoming more concentrated amongst Canadians with lower levels of education. Consequently, campaigns and public policies related to the prevention of melanoma in Canada should focus on Canadians with higher income and lower levels of education.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It is estimated that one in two Canadians will develop cancer in their lifetime, with skin cancers being the most common (Canadian Cancer Society’s Advisory Committee on Cancer Statistics 2017). Although not the most common skin malignancy, cutaneous melanoma, commonly referred to as melanoma, is the most aggressive and lethal form, and arises from pigment-producing cells, melanocytes, in the basal layer of the skin (Chin 2003; Volkovova et al. 2012; Rastrelli et al. 2014). Melanocytes synthesize and deliver the pigment melanin to neighboring keratinocytes. Within the keratinocytes, melanin protects the cell’s DNA by absorbing and deflecting radiation (Chin 2003).
There are four main types of cutaneous melanoma: superficial spreading, nodular, lentigo maligna, and acral lentiginous. Superficial spreading melanoma is the most common, accounting for approximately 70% of all melanoma (Rastrelli et al. 2014). It typically occurs in adults and can develop anywhere on the body, but principally appears on the head and trunk in men, and on the lower extremities in women (Gruber and Armstrong 2006; Ghazawi et al. 2019). These tumors usually begin with a horizontal proliferation of melanocytes, followed by a vertical growth phase. If left untreated, melanoma can invade the basement membrane, reach the blood or the lymphatic systems, and spread to other organs, most commonly the liver, brain, and lung (Rodolfo et al. 2004). Tumors detected at early stages have a five-year survival rate of 85% in men and 92% in women; nonetheless, since melanomas are resistant to most forms of chemotherapy, advanced disease carries an inferior prognosis (Miller and Mihm 2006). While the incidence and mortality rates are decreasing for many types of cancer, melanoma rates have been increasing in Canada (Ortiz et al. 2005; Ghazawi et al. 2019). Additionally, melanoma incidence and mortality rates are greater in older compared to younger Canadians, which is of concern as the population ages (Canadian Cancer Society’s Advisory Committee on Cancer Statistics 2014).
The etiology of cutaneous melanoma is complex and appears to result from the interaction of genetic, host, and environmental influences. The known genetic features associated with increased melanoma susceptibility include germline mutations of the CDKN2A and CDK4 genes and polymorphisms in the MC1R gene associated with the red-hair phenotype (Palmer et al. 2002; Goldstein and Tucker 2013; Azoury and Lange 2014). Somatic mutations in the BRAF gene are the most common in sporadic cases of the disease (Davies et al. 2002; Burotto et al. 2014). The presence of a large number of melanocytic nevi, or moles, is also a significant risk factor, and the presence of dysplastic, or atypical, nevi act as an additional risk (Swedlow et al. 1986; Holly et al. 1987). Other host factors implicated in the development of this cancer include light hair color, light eye color, increased freckling, inability to tan, and immunosuppression (Smith et al. 1993; Tucker and Goldstein 2003; Brewer et al. 2011). Although genetic phenotypes, genotypes, and increasing age contribute to the risk of this disease, exposure to ultraviolet (UV) radiation is the most significant factor for the development of melanoma (Miller and Mihm 2006; Volkovova et al. 2012). UVB radiation is responsible for the formation of the principal DNA lesions, whereas UVA radiation causes oxidative damage (Ichihashi et al. 2003; Situm et al. 2007). This DNA damage typically leads to programmed cell death; however, in melanocytes, which are resistant to apoptosis, a high dose of UV radiation will cause genetic damage, but does not ultimately lead to cell death (Gilchrest et al. 1999). For this reason, unlike basal cell and squamous cell carcinomas, skin cancers associated with total cumulative exposure to sunlight, melanomas are associated with intermittent sun exposure and a history of sunburns (Elwood and Jopson 1997).
Socioeconomic status (SES) may influence the risk of cancer in many ways, including exposure, behavior, and access to care (Krieger et al. 1999; Hiatt 2004). Studies have shown lower SES to be associated with an increased risk of colorectal, lung, and cervical cancer, while higher SES is found to be associated with increased risk of breast cancer and prostate cancer (Krieger et al. 1999; Clegg et al. 2009; Sidorchuk et al. 2009). Previous studies have assessed socioeconomic gradients in melanoma incidence and concluded that, in Canada and worldwide, cutaneous melanoma is more common in those with higher SES (Gallagher et al. 1987; Hwang et al. 2013; Haider et al. 2007). However, to our knowledge, no study has used a summary measure of socioeconomic inequality, one that takes into account the distribution of melanoma incidence in all SES groups, to quantify socioeconomic inequality in the incidence of cutaneous melanoma in Canada. By linking data from the Canadian Cancer Registry (CCR), Canadian Census of Population (CCP), and National Household Survey (NHS), and by applying a widely used summary measure of socioeconomic inequality, the concentration index (C), we quantified income- and education-related inequalities in the incidence of cutaneous melanoma in Canada, excluding territories (Northwest Territories, Nunavut, and Yukon) accounting for 0.03% of the total population (Statistics Canada 2020). We examined trends in income- and education-related inequalities in the incidence of cutaneous melanoma in Canada for the period between 1992 and 2010. This is the period in which the CCR data are available for all Canadian provinces in Statistics Canada’s Research Data Centres (RDCs). The main goal is to understand the difference in melanoma incidence rates amongst individuals of differing SES, in order to provide insight into target populations for intervention and management in Canada.
Materials and methods
Data sources and variables
The data used for this study were sourced from the CCR data file, the CCP (1991, 1996, 2001, 2006), and the NHS (2011). The CCR collects information about cancer cases diagnosed in Canada, including patient demographics and tumor-specific data, but does not collect SES-related information (e.g., education and income). Primary tumors are recorded in this dataset based on their International Classification of Diseases for Oncology (ICD-O) topographical and morphological codes. The third edition of the ICD-O (ICD-O-3) code number C44 (8720–8790) was used to identify individual incidences of cutaneous melanoma within the CCR data. We then obtained the individual’s sex and six-digit postal code from the CCR data. We used the Postal Code Conversion File Plus (PCCF+) Version D software to identify the Census Division (CD) coordinates for each patient based on their postal code. The CDs are groups of municipalities such as cities, districts, and counties defined by Statistics Canada to conduct the CCP. The number of CDs in Canada was in the range of 276–283 from 1992 to 2010. This information was then used to calculate the number of new cases of melanoma in each CD.
The CCP collects demographic and socioeconomic information for the total Canadian population every five years. We used SES variables obtained from the 1991, 1996, 2001, and 2006 CCP and the 2011 NHS to create a dataset that contained measures of SES (average and median equivalized household income and proportion of individuals with a bachelor’s degree or above), as well as population characteristics for each of Canada’s CDs. Since the 2011 CCP did not collect socioeconomic information, the 2011 NHS was used to obtain socioeconomic information about the Canadian population for the more recent years included in our study. Household income was equivalized by dividing the household income by the square root of household size, as per the Organisation for Economic Co-operation and Development (OECD) publications (OECD 2011).
Socioeconomic and demographic information obtained from the CCP and NHS datasets was linked to CCR based on CD coordinates. Since census data are only collected every five years, cases diagnosed in 1992 and 1993 were linked with data from the 1991 census year; cases diagnosed in the 1994–1998 period, the 1996 census year; cases diagnosed in the 1999–2003 period, the 2001 census year; and cases diagnosed in the 2004–2008 period, the 2006 census year. Cases diagnosed from 2009 and 2010 were linked with 2011 NHS data. This linking allowed us to measure the incidence rates of melanoma and to estimate income- and education-related inequalities in the incidence of melanoma from 1992 to 2010.
Statistical analysis
Trends in the incidence of cutaneous melanoma
Trend analyses were performed by plotting time (19 points corresponding to the years 1992–2010) versus the incidence of melanoma. The slope value of the regression line (trend coefficient) was used to determine linear trends in melanoma incidence over time.
Socioeconomic inequalities in melanoma incidence
The concentration index (C) approach (Wagstaff et al. 1991; World Bank 2019) was used to quantify income- and education-related inequalities in the incidence of cutaneous melanoma in Canada from 1992 to 2010. The C is a summary measure of socioeconomic inequality used in health economics and public health literature. It is preferred over other measures of inequality, such as the rate difference and rate ratio, as it reflects the distribution of health outcome across all socioeconomic groups (Wagstaff et al. 1991). The C is defined based on the concentration curve (CC). The CC is a plot of the cumulative share of individuals (CDs) ordered by their SES variable (e.g., income or level of education) on the horizontal axis against the cumulative share of health outcome (incidence of melanoma) on the vertical axis (Fig. 1). If the incidence is the same for all individuals, the CC will be a linear line at 45° to the horizontal axis. This line is termed the “line of perfect equality”. If the CC is above (below) the line of perfect equality, it indicates that health outcome is concentrated among higher (lower) SES individuals. The C is calculated as twice the area between the CC and the line of perfect equality. The index can ranges between −1 to +1, with zero indicating perfect equality. A negative value suggests that the health outcome (melanoma incidence) is higher among individuals with lower SES and a positive value indicates that the health outcome is higher among individuals with higher SES. The crude C can be estimated using the following “convenient regression” formula (Kakwani et al. 1997):
where Mi shows CDi’s melanoma incidence rate, μ is the mean incidence rate of cutaneous melanoma for all CDs, α is the intercept, and Ri is the CDi’s fractional rank in the distribution (i = 1 and n for the lowest SES and highest SES CDs, respectively). The Ri for each CD is calculated as Ri = i/n. The \( {\sigma}_R^2 \)denotes the variance of fractional rank. The ordinary least squares (OLS) estimate of δ in Eq. (1) and its standard error demonstrate the value and the standard error for the crude C, correspondingly.

Concentration curve for cutaneous melanoma incidence (an example)
Age-standardized income- and education-related inequality in the incidence rate of cutaneous melanoma can be calculated using an indirectly standardized C by including the standardizing variable age in the convenient regression as follows (O’Donnell et al. 2008):
where AvAgei denotes the average age of each CDi and βi are the coefficients for AvAge. The OLS estimate of δ in Eq. (2) is the age-standardized C.
Trends in socioeconomic inequalities in melanoma incidence
A trend analysis was performed by plotting time (19 points corresponding to the years 1992–2010) against the age-standardized C of each inequality measure. The slope value of the regression line (trend coefficient) was used to determine the linear trend of the age-standardized C index over time, at a p-value < 0.05.
Results
Trends in melanoma incidence
Table 1 shows the crude incidence of cutaneous melanoma in Canada by sex and province from 1992 to 2010. During this period, the linear regression analysis of the crude incidence rate revealed an increasing trend with a slope of 0.35 cases/100,000 person-years. This increase, although significant for both males and females, was slightly higher for males (p < 0.01). The linear regression analysis of the crude incidence rates from 1992 to 2010 revealed an increasing trend (p < 0.05) in all provinces, except Manitoba. The highest increases were seen in the Atlantic Provinces, with Nova Scotia experiencing the most considerable increase.
Socioeconomic inequalities in melanoma incidence
Income-related inequalities
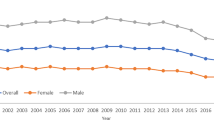
Income-related inequalities (using average and median household equivalized income) in the incidence rates of cutaneous melanoma in Canada from 1992 to 2010 are reported in Table 2 and displayed in Fig. 2a and b. As reported, the values of all the age-standardized C (using average household equivalized income in the calculation) are positive; however, the majority of the 95% confidence intervals (CIs) contain zero values. Years where the CI intervals of the age-standardized C do not include the zero value are 1995, 1997, and 2004 for both sexes, 1995, 1997, 1998, 2002, 2005, and 2008–2010 for males, and 1995 and 2007 for females, suggesting that income-related inequalities in cutaneous melanoma incidence are concentrated among individuals with higher average household equivalized income in these years (see Table 2 and Fig. 2a). Linear regression analysis of the age-standardized C calculated using average household equivalized income did not reveal any significant trends from 1992 to 2010.

Socioeconomic inequalities in the age-adjusted incidence of cutaneous melanoma in Canada (excluding territories): 1992 to 2010. a Average household equivalized income. b Median household equivalized income. c Bachelor’s degree or higher
The values of all age-standardized median household equivalized income C indexes are positive. The majority of the 95% CIs do not span zero; this is especially true for the later years of the study, 2001 to 2009. Years where the CIs do not span zero include 1995–1998 and 2001–2010 for both sexes, 1995–1998, 2000, and 2001–2010 for males, and 1995–1997 and 2001–2009 for females, suggesting that, for most years included, income-related inequalities in cutaneous melanoma incidence are concentrated among individuals with higher income level. Linear trend analysis of the age-standardized C calculated using median household equivalized income revealed an increasing trend from 1992 to 2010 for both males and females (see Table 2 and Fig. 2b). This suggests that income-related inequalities in cutaneous melanoma incidence are becoming more concentrated among individuals with higher incomes (p < 0.05) over time.
Education-related inequalities
Education-related inequalities in the incidence rate of cutaneous melanoma in Canada from 1992 to 2010 are reported in Table 3. Most values of the age-standardized C are negative, suggesting that cutaneous melanoma cases are concentrated among individuals with lower levels of education; however, these findings were not found to be significant for men, and 2010 is the only year where there was statistical significance for women. Linear trend analysis of the age-standardized C, reported in Table 3 and displayed in Fig. 2c, revealed a decreasing trend in the value of C from 1992 to 2010 for both males and females, suggesting that, with time, incidence rates are becoming more concentrated among individuals with lower levels of education (p < 0.01).
Discussion
This study aimed to measure the incidence rates of cutaneous melanoma in Canada from 1992 to 2010 and to quantify and assess trends in income- and education-related inequalities in these rates over time. The results showed an increase in the incidence of melanoma across Canada during the study period. These results are consistent with current literature proposing increasing melanoma incidence in Canada and worldwide (de Vries and Coebergh 2004; Erdmann et al. 2013; Ghazawi et al. 2019). Epidemiologic studies of melanoma have shown that the primary environmental risk factor is UV radiation. It has been suggested that these increases in melanoma rates reflect increased sunlight exposure due to ozone depletion and human behavior, such as increased use of tanning beds, rather than being associated with improvements in diagnostic efforts (Jemal et al. 2001; Boniol et al. 2012; Volkovova et al. 2012). Consequently, primary prevention strategies focus on avoidance of sunburns and decreased exposure to UV radiation (Schottenfeld and Fraumeni 2006), while secondary prevention approaches include enhancing early recognition of melanoma-like lesions, physician screening practices, and patient skin self-examination (Koh and Geller 1995; Rigel and Carucci 2000; Abbasi et al. 2004; de Vries and Coebergh 2004).
Our analysis revealed evidence of increased melanoma incidence rates amongst men and women, with higher median household incomes and increasing C values from 1992 to 2010. These trends were not observed when average household incomes were investigated; however, the median income is a more accurate measure of income, as outliers do not affect it. Lifestyle behaviors commonly associated with higher income, such as outdoors leisure or travel to lesser latitudes where levels of UV radiation are elevated, may increase susceptibility for melanoma development in these individuals (Gallagher et al. 1987). Additionally, individuals with lower SES may have decreased access to screening and examination (Koh et al. 1991). These results are in agreement with the current literature which indicate higher SES being associated with higher incidence of melanoma in Canada (Gallagher et al. 1987; Gorey et al. 1998; Ortiz et al. 2005; Haider et al. 2015; Johnson-Obaseki et al. 2015; Langley et al. 2018), in Scotland (Doherty et al. 2010; MacKie and Hole 1996), and in the United States (Lee et al. 1992; White et al. 1994; Goodman et al. 1995; Harrison et al. 1998); however, these studies do not consider income and education separately in their definitions of SES.
Our analysis showed no statistically significant association between level of education and melanoma incidence in men, and none in women until 2010. In 2010, incidence rates were higher amongst women with lower levels of education. Furthermore, our trend analyses suggest that higher levels of education are becoming increasingly protective against the incidence rates of cutaneous melanoma. An explanation for this finding may be associated with an increasing amount of education related to sun safety. These results contradict studies that report the greatest incidence rates amongst individuals with higher levels of education (Lee et al. 1992; White et al. 1994; Goodman et al. 1995; Harrison et al. 1998). However, such studies were published before the year 2000 and did not focus on the Canadian population.
This study is subject to some limitations. First, although studies have found area-based SES measures, such as CDs, to be comparable to individual-based measures, neighborhood characteristics do not always reflect individual characteristics (Mustard et al. 1999; Krieger et al. 2002). Second, the development of cutaneous melanoma is associated with factors such as family history, skin color, and genetics; we could not control for these factors. Finally, as the census is not conducted every year, to obtain relevant socioeconomic data, we had to use the closest census years to our CCR year of interest.
In conclusion, Canadians with higher incomes have higher incidence rates of melanoma, and trends suggest that incidence is becoming more concentrated amongst Canadians with lower levels of education. Consequently, education and income should be considered separately when discussing the impact of SES on melanoma incidence. Canadian guidelines, campaigns, and public policies should focus on individuals with higher median income and those with lower levels of education.
References
Abbasi NR, Shaw HM, Rigel DS et al (2004) Early diagnosis of cutaneous melanoma: revisiting the ABCD criteria. JAMA 292:2771–2776
Azoury SC, Lange JR (2014) Epidemiology, risk factors, prevention, and early detection of melanoma. Surg Clin North Am 94:945–962. https://doi.org/10.1016/j.suc.2014.07.013
Boniol M, Autier P, Boyle P, Gandini S (2012) Cutaneous melanoma attributable to sunbed use: systematic review and meta-analysis. BMJ 345:e4757. https://doi.org/10.1136/bmj.e4757
Brewer JD, Christenson LJ, Weaver AL et al (2011) Malignant melanoma in solid transplant recipients: collection of database cases and comparison with surveillance, epidemiology, and end results data for outcome analysis. Arch Dermatol 147:790–796. https://doi.org/10.1001/archdermatol.2011.159
Burotto M, Chiou VL, Lee J-M, Kohn EC (2014) The MAPK pathway across different malignancies: a new perspective. Cancer 120:3446–3456. https://doi.org/10.1002/cncr.28864
Canadian Cancer Society’s Advisory Committee on Cancer Statistics (2014) Canadian cancer statistics 2014: special topic: skin cancers. Canadian Cancer Society, Toronto, ON
Canadian Cancer Society’s Advisory Committee on Cancer Statistics (2017) Canadian cancer statistics 2017: special topic: pancreatic cancer. Canadian Cancer Society, Toronto, ON
Chin L (2003) The genetics of malignant melanoma: lessons from mouse and man. Nat Rev Cancer 3:559–570. https://doi.org/10.1038/nrc1145
Clegg LX, Reichman ME, Miller BA et al (2009) Impact of socioeconomic status on cancer incidence and stage at diagnosis: selected findings from the surveillance, epidemiology, and end results: National Longitudinal Mortality Study. Cancer Causes Control 20:417–435. https://doi.org/10.1007/s10552-008-9256-0
Davies H, Bignell GR, Cox C et al (2002) Mutations of the BRAF gene in human cancer. Nature 417:949–954. https://doi.org/10.1038/nature00766
de Vries E, Coebergh JW (2004) Cutaneous malignant melanoma in Europe. Eur J Cancer 40:2355–2366. https://doi.org/10.1016/j.ejca.2004.06.003
Doherty VR, Brewster DH, Jensen S, Gorman D (2010) Trends in skin cancer incidence by socioeconomic position in Scotland, 1978–2004. Br J Cancer 102:1661–1664. https://doi.org/10.1038/sj.bjc.6605678
Elwood JM, Jopson J (1997) Melanoma and sun exposure: an overview of published studies. Int J Cancer 73:198–203. https://doi.org/10.1002/(SICI)1097-0215(19971009)73:2<198::AID-IJC6>3.0.CO;2-R
Erdmann F, Lortet-Tieulent J, Schüz J et al (2013) International trends in the incidence of malignant melanoma 1953–2008—are recent generations at higher or lower risk? Int J Cancer 132:385–400. https://doi.org/10.1002/ijc.27616
Gallagher RP, Elwood JM, Threlfall WJ, Spinelli JJ, Fincham S, Hill GB (1987) Socioeconomic status, sunlight exposure, and risk of malignant melanoma: the Western Canada Melanoma Study. J Natl Cancer Inst 79:647–652
Ghazawi FM, Cyr J, Darwich R et al (2019) Cutaneous malignant melanoma incidence and mortality trends in Canada: a comprehensive population-based study. J Am Acad Dermatol 80:448–459. https://doi.org/10.1016/j.jaad.2018.07.041
Gilchrest BA, Eller MS, Geller AC, Yaar M (1999) The pathogenesis of melanoma induced by ultraviolet radiation. N Engl J Med 340:1341–1348
Goldstein AM, Tucker MA (2013) Genetic epidemiology of cutaneous melanoma: a global perspective. Arch Dermatol 137:1493–1496. https://doi.org/10.1001/archderm.137.11.1493
Goodman KJ, Bible ML, London S, Mack TM (1995) Proportional melanoma incidence and occupation among white males in Los Angeles County (California, United States). Cancer Causes Control 6:451–459. https://doi.org/10.1007/BF00052186
Gorey KM, Holowaty EJ, Laukkanen E, Fehringer G, Richter NL (1998) Association between socioeconomic status and cancer incidence in Toronto, Ontario: possible confounding of cancer mortality by incidence and survival. Cancer Prev Control 2:236–241
Gruber SB, Armstrong BK (2006) Cutaneous and ocular melanoma. Cancer Epidemiol Prev:1196–1229. https://doi.org/10.1093/acprof:oso/9780195149616.003.0063
Haider A, Mamdani M, Shear NH (2007) Socioeconomic status and the prevalence of melanoma in Ontario, Canada. J Cutan Med Surg 11:1–3. https://doi.org/10.2310/7750.2007.00001
Harrison RA, Haque AU, Roseman JM, Soong SJ (1998) Socioeconomic characteristics and melanoma incidence. Ann Epidemiol 8:327–333. https://doi.org/10.1016/S1047-2797(97)00231-7
Hiatt RA (2004) The social determinants of cancer. Eur J Epidemiol 19:821–822
Holly EA, Kelly JW, Shpall SN (1987) Number of melanocytic nevi as a major risk factor for malignant melanoma. J Am Acad Dermatol 17:459–468. https://doi.org/10.1016/S0190-9622(87)70230-8
Hwang E, Johnson-Obaseki S, McDonald JT, Connell C, Corsten M (2013) Incidence of head and neck cancer and socioeconomic status in Canada from 1992 to 2007. Oral Oncol 49:1072–1076. https://doi.org/10.1016/j.oraloncology.2013.08.002
Ichihashi M, Ueda M, Budiyanto A et al (2003) UV-induced skin damage. Toxicology 189:21–39. https://doi.org/10.1016/S0300-483X(03)00150-1
Jemal A, Devesa SS, Hartge P, Tucker MA (2001) Recent trends in cutaneous melanoma incidence among whites in the United States. J Natl Cancer Inst 93:678–683
Johnson-Obaseki SE, Labajian V, Corsten MJ, McDonald JT (2015) Incidence of cutaneous malignant melanoma by socioeconomic status in Canada: 1992–2006. J Otolaryngol Head Neck Surg 44:53. https://doi.org/10.1186/s40463-015-0107-1
Kakwani N, Wagstaff A, van Doorslaer E (1997) Socioeconomic inequalities in health: measurement, computation, and statistical inference. J Econ 77:87–103
Koh HK, Geller AC (1995) Melanoma and skin cancer control: an international perspective. Cancer Control 2:385–391. https://doi.org/10.1177/107327489500200501
Koh HK, Geller AC, Miller DR, Caruso A, Gage I, Lew RA (1991) Who is being screened for melanoma/skin cancer? Characteristics of persons screened in Massachusetts. J Am Acad Dermatol 24:271–277
Krieger N, Quesenberry C Jr, Peng T et al (1999) Social class, race/ethnicity, and incidence of breast, cervix, colon, lung, and prostate cancer among Asian, black, Hispanic, and White residents of the San Francisco Bay Area, 1988–92 (United States). Cancer Causes Control 10:525–537
Krieger N, Chen JT, Waterman PD et al (2002) Geocoding and monitoring of US socioeconomic inequalities in mortality and cancer incidence: does the choice of area-based measure and geographic level matter? The Public Health Disparities Geocoding Project. Am J Epidemiol 156:471–482. https://doi.org/10.1093/aje/kwf068
Langley A, Levesque L, Baetz T, Asai Y (2018) Brief report: increase in melanoma incidence in Ontario. J Cutan Med Surg 22:476–478. https://doi.org/10.1177/1203475418773360
Lee PY, Silverman MK, Rigel DS et al (1992) Level of education and the risk of malignant melanoma. J Am Acad Dermatol 26:59–63
MacKie RM, Hole DJ (1996) Incidence and thickness of primary tumours and survival of patients with cutaneous malignant melanoma in relation to socioeconomic status. BMJ 312:1125–1128. https://doi.org/10.1136/bmj.312.7039.1125
Miller AJ, Mihm MC Jr (2006) Melanoma. N Engl J Med 355:51–65. https://doi.org/10.1056/NEJMra052166
Mustard CA, Derksen S, Berthelot J-M, Wolfson M (1999) Assessing ecologic proxies for household income: a comparison of household and neighbourhood level income measures in the study of population health status. Health Place 5:157–171. https://doi.org/10.1016/S1353-8292(99)00008-8
O’Donnell O, van Doorslaer E, Wagstaff A, Lindelow M (2008) Analyzing health equity using household survey data. The World Bank
OECD (2011) What are equivalence scales? OECD project on income distribution and poverty. http://www.oecd.org/els/soc/OECD-Note-EquivalenceScales.pdf.
Ortiz CA, Goodwin JS, Freeman JL (2005) The effect of socioeconomic factors on incidence, stage at diagnosis and survival of cutaneous melanoma. Med Sci Monit 11:RA163–RA172
Palmer JS, Duffy DL, Box NF et al (2002) Melanocortin-1 receptor polymorphisms and risk of melanoma: is the association explained solely by pigmentation phenotype? Am J Hum Genet 66:176–186. https://doi.org/10.1086/302711
Rastrelli M, Tropea S, Rossi CR, Alaibac M (2014) Melanoma: epidemiology, risk factors, pathogenesis, diagnosis and classification. In Vivo 28:1005–1011
Rigel DS, Carucci JA (2000) Malignant melanoma: prevention, early detection, and treatment in the 21st century. CA Cancer J Clin 50:215–236
Rodolfo M, Daniotti M, Vallacchi V (2004) Genetic progression of metastatic melanoma. Cancer Lett 214:133–147. https://doi.org/10.1016/j.canlet.2004.06.049
Schottenfeld D, Fraumeni JF (2006) Cancer epidemiology and prevention, 3rd edn. Oxford University Press, New York
Sidorchuk A, Agardh EE, Aremu O et al (2009) Socioeconomic differences in lung cancer incidence: a systematic review and meta-analysis. Cancer Causes Control 20:459–471. https://doi.org/10.1007/s10552-009-9300-8
Situm M, Buljan M, Bulić SO, Simić D (2007) The mechanisms of UV radiation in the development of malignant melanoma. Coll Antropol 31(Suppl 1):13–16
Smith KJ, Skelton HG, Yeager J, Angritt P, Wagner KF (1993) Cutaneous neoplasms in a military population of HIV-1-positive patients. J Am Acad Dermatol 29:400–406
Statistics Canada (2020) Table 17-10-0009-01. Population estimates, quarterly. https://doi.org/10.25318/1710000901-eng
Swedlow AJ, English J, MacKie RM et al (1986) Benign melanocytic naevi as a risk factor for malignant melanoma. Br Med J (Clin Res Ed) 292:1555–1559. https://doi.org/10.1136/bmj.292.6535.1555
Tucker MA, Goldstein AM (2003) Melanoma etiology: where are we? Oncogene 22:3042–3052. https://doi.org/10.1038/sj.onc.1206444
Volkovova K, Bilanicova D, Bartonova A et al (2012) Associations between environmental factors and incidence of cutaneous melanoma. Review. Environ Health 11:S12. https://doi.org/10.1186/1476-069X-11-S1-S12
Wagstaff A, Paci P, van Doorslaer E (1991) On the measurement of inequalities in health. Soc Sci Med 33:545–557. https://doi.org/10.1016/0277-9536(91)90212-U
White E, Kirkpatrick CS, Lee JA (1994) Case-control study of malignant melanoma in Washington State. I. Constitutional factors and sun exposure. Am J Epidemiol 139:858–868. https://doi.org/10.1093/oxfordjournals.aje.a117092
World Bank (2019) Quantitative techniques for health equity analysis: the concentration index. http://citeseerx.ist.psu.edu/viewdoc/summary?doi=10.1.1.634.5222
Acknowledgements
The analyses for this paper were conducted at the Statistics Canada’s Atlantic Research Data Centre (ARDC) at Dalhousie University, which is part of the Canadian Research Data Centre Network (CRDCN). The authors would like to thank the CRDCN for facilitating the access to the Canadian Cancer Registry, Canadian Census of Population, and the National Household Survey, and the ARDC analyst Heather Hobson for her support and assistance. We also thank Min Hu for his research assistance.
Funding
Marie Charles received the Dalhousie Faculty of Medicine Sandy Murray Research in Medicine (RIM) Studentship for research in dermatology (2019) and Mohammad Hajizadeh acknowledges the Research Development Grant Faculty of Health, Dalhousie University (2017).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics statement
The data files used for this study, the Canadian Cancer Registry (CCR), the Canadian Census of Population (CCP), and the National Household Survey (NHS), are available at the Statistics Canada’s Research Data Centre Network (RDCN). Data were accessed in the Atlantic Research Data Centre (ARDC) located at Dalhousie University. Data obtained through the ARDC are exempt from research ethics board review based on the Tri-council policy statement: Ethical conduct for research involving humans (TCPS2) article 2.2 (a).
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Charles, M., Hajizadeh, M. Trends in socioeconomic inequalities in the incidence of cutaneous melanoma in Canada from 1992 to 2010. J Public Health (Berl.) 29, 1215–1224 (2021). https://doi.org/10.1007/s10389-020-01232-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-020-01232-z