
Abstract
Monitoring the health status of patients has become a major activity in rehabilitation research in recent years. As a result, various self-assessment instruments have been developed, adapted or improved with the aim of measuring patient-reported outcomes and predictors. Among these are international instruments, such as the NHP or the SF-36, as well as those developed in Germany, such as the IRES, the FREM-17 or the SPE-scale. Some of the widely used international instruments, such as the NHP and SF-36, have been translated into German for application in Germany. All of these instruments have been thoroughly tested and validated in several studies. Current trends in statistical methods (e.g. responsiveness, Rasch scaling) as well as classical test-theoretical standards were taken into consideration in the development of these instruments. In this article, we provide a comprehensive review of five important assessment fields of rehabilitation research in Germany: health-related quality of life (generic, disease-specific, children and adolescents, preference-based), evaluation of specific therapy and education programs, motivation, screening for vocational problems and screening for comorbid disorders. The questionnaires are critically discussed, and perspectives for further research are specified. Although assessment instruments as the IRES or the SF-36 are well-established in rehabilitation research studies, there is still a need for further research to determine the best choice of instruments for a given purpose. The limitations of the questionnaires with respect to health care studies are also discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Assessing patient-reported outcomes is an essential element of health care evaluation in rehabilitation research. In 1998, the German Federal Ministry of Education and Research (BMBF) and the German pension insurance scheme established a funding program for rehabilitation research projects. The German Research Funding Program “Rehabilitation Sciences” contains eight research networks and maintains working groups across all of these research networks (URL:http://www.reha-verbund.de). Various self-administered instruments were developed in order to measure patient-reported outcomes and predictors, all adapted or improved within the framework of this funding program.
These instruments assist in the inclusion of the patients’ perspective in the area of rehabilitation research, diagnostics and therapy. A personal perception of overall health status as well as a feeling of well-being in physical, mental and social domains are substantial factors in coping and health-related behavior. Therefore, patient-reported outcomes are a matter of particular interest.
Methods
In this paper, a comprehensive review is given in five important assessment fields of rehabilitation research in Germany: health-related quality of life (HRQoL), evaluation of specific therapy and education programs, motivation, screening for vocational problems and screening for comorbid mental disorders. The purpose of this review is to provide researchers and clinicians with current developments and practical information regarding the instruments reviewed.
Results
Health-related HRQoL
Current questionnaires measuring HRQoL can be classified into psychometric measures, which are rooted in classical measurement theory, and preference-based measures, which are derived from decision and utility theories. In the traditions of both types of instruments, health is considered to be a multidimensional concept, but the two approaches differ in several aspects. The development of psychometric measures is based on the specific scale’s objectivity, validity, reliability, and responsiveness to each health domain. This is achieved by developing multi-item scales to measure each domain. In contrast, the goal of instruments measuring HRQoL for use in economic evaluations is to obtain a single summary index expressing peoples’ preferences for different health states. Such measures determine various aspects of health on a single summary scale from zero (dead) to unity (healthy).
In addition, HRQoL questionnaires can be further subclassified into generic and disease-specific instruments. Generic instruments are able to compare outcomes across different populations and interventions, while disease-specific measures assess the specific health status and concerns of certain diagnostic groups. Unlike generic instruments, the latter seem to be especially sensitive for detecting changes over time, which is an important feature for clinicians and patients.
Generic HRQoL questionnaires
At the present time, two generic HRQoL instruments are commonly used in German rehabilitation research: the questionnaire “Indicators of Rehabilitation Status” (IRES; Bührlen et al. 2005) and the “Short Form-36 Health Survey” (SF-36; Bullinger and Kirchberger 1998; Ware and Sherbourne 1992). Short versions of the IRES (IRES-24) and the SF-36 (SF-12) are also available. Both instruments are often used in combination of one long version and one short version in German rehabilitation research projects. Measurement instruments which are much less frequently used are the “Sickness Impact Profile” (SIP; Bergner et al. 1981) and the “Nottingham Health Profile” (NHP; Hunt et al. 1981). Table 1 provides the content areas covered by these four HRQoL instruments.
Indicators of Rehabilitation Status (IRES) questionnaire
The IRES was developed and validated in Germany as a generic instrument assessing HRQoL in rehabilitation research studies (Gerdes and Jäckel 1995). Theoretical considerations as well as re-analyses of extensive datasets have recently provided the necessary support for a major revision of the items and scales (e.g. Zwingmann 2004). The revised version IRES-3 (Bührlen et al. 2005) is based on a theoretical model of rehabilitation following the guidelines of the ICF (International Classification of Functioning, Disability, and Health). In addition, the results of expert panels on the definition of treatment goals in medical rehabilitation are implemented. The IRES-3 questionnaire consists of eight dimensions with a varying number of items. Response levels range from five to seven. The scale classification is based on theoretical considerations with regard to exploratory and confirmatory factor analyses (Bührlen et al. 2005). The IRES-3 questionnaire is available in three different versions. The baseline version includes 144 items, thereby assessing additional information about treatment strategy, normal daily activities and vocational life. The end of treatment version comprises 75 items, the follow-up version 123 items. The IRES-3 was thoroughly tested in a sample of rehabilitation patients of seven diagnostic groups (n=453). Comparisons of the IRES-3 with the SF-36 and a German version of the “Hospital Anxiety and Depression Scale” (HADS-D) revealed convergent validity. The analyses also showed satisfactory results with respect to item difficulties, missing values, ceiling and floor effects, internal consistencies and test-retest-reliability. Pearson correlations between IRES-3 and SF-36 scales of the same domain were moderate to strong, thus demonstrating good practicability in comparison with another generic measurement. All dimensions of the IRES-3 showed higher responsiveness than the SF-36. The German version of the IRES-3 is available online (URL:http://www.hri.de).
A short version of the IRES-3 (IRES-24) was derived which is based on Mixture Distribution Rasch Models (Wirtz et al. 2005). The IRES-24 describes four dimensions: subjective health, functionality in everyday life, physical health and pain, and is a short, economic, and practicable tool for assessing indicators relevant for treatment strategy and the evaluation of clinical rehabilitation.
Short Form-36 Health Survey (SF-36/SF-12)
At the international level, the SF-36 is currently one of the most widely used HRQoL instruments. In its early stages, the SF-36 was developed to assess the HRQoL in clinical practice and research, health policy evaluations and general population surveys (Ware and Sherbourne 1992). Since its development it has also been established in rehabilitation outcome research studies. The SF-36 consists of 36 items measuring health across eight domains. Responses are transformed into a score ranging from 0 (bad health) to 100 (good health). Additionally, the eight dimensions can be summarized to two broad scales: physical health and mental health. In recent years, several rehabilitation research studies have shown that the SF-36 is a feasible instrument by which to measure HRQoL in samples of rehabilitation patients (Bullinger et al. 2003; Maurischat and Krüger-Bödecker 2004). A short version (SF-12) is also available which contains 12 items that describe HRQoL on the same two broad domains as the original: physical health and mental health.
Disease-specific instruments
In contrast to generic measurements, disease-specific instruments assess HRQoL for certain interventions or in certain subpopulations. In general, disease-specific instruments seem to be more sensitive to changes in patients’ health status than generic HRQoL measures. Several disease-specific instruments have developed or adapted to measure HRQoL in rehabilitation. In this review we describe two instruments in more detail: the “Quality of Life Questionnaire Asthma and Chronic Obstructive Pulmonary Disease” (FLAC; Mühlig et al. 2000) and the German version of the “Short Musculoskeletal Function Assessment Questionnaire” (SMFA; Swiontkowski et al. 1999).
FLAC
The aim of FLAC was to facilitate the evaluation of HRQoL in samples of patients with chronic respiratory diseases. FLAC consists of 14 Likert-scaled items, each belonging to one of four subscales: physical well-being and functioning (four items), social well-being and functioning (four items), mental well-being and functioning (four items) and treatment satisfaction and disease management (two items). The questionnaire was tested and validated in a sample of patients with asthma and chronic obstructive pulmonary disease, respectively (n=143). Results have shown that the FLAC is highly accepted and feasible in samples of patients with chronic respiratory diseases.
SMFA
The SMFA was originally developed in the United States as a disease-specific HRQoL measure for use in community-based outcome studies and in clinical studies of patients with musculo-skeletal disorders (Swiontkowski et al. 1999). The questionnaire consists of two parts with a total of 46 items. Part one – the function index (34 items) – assesses patient function, and part two – the bother index (12 items) – describes whether patients are bothered by functional problems. Disease-specific instruments, such as the SMFA, cover a broad range of musculo-skeletal diseases of the extremities (i.e. degenerative, inflammatory or traumatic diseases). The German adaptation (SMFA-D) has been tested in several patient samples treated operatively for osteoarthritis of the knee and hip, rotator cuff tears and rheumatoid arthritis with regard to practicability, psychometric properties and distributional characteristics (e.g. König et al. 2000, Kirschner et al. 2003, Glatzel et al. 2004, Wollmerstedt et al. 2004). It seems to be a valid, reliable and responsive instrument by which to assess changes in functional status concerning patients with musculo-skeletal diseases of the extremities.
In addition, a short version (XSMFA-D) containing 16 items has been developed (Wollmerstedt et al. 2003). The XSMFA-D was evaluated in a sample of patients with primary osteoarthritis of the knee and hip undergoing a total joint replacement. Analyses with respect to internal consistency, test-retest-reliability as well as construct and criterion validity yielded moderate to high coefficients. However, further studies evaluating the feasibility of the XSMFA-D in samples of patients with moderate musculo-skeletal disorders are needed. Currently, a population-based study with the SMFA-D and XSMFA-D, respectively, is planned for assessing norms of the general population.
Children and adolescents
Concomitant with the growing number of structured treatment programs for children and adolescents in rehabilitation is the growing interest in indicators of subjective health and quality of life in this research field. While there is evidence that HRQoL measures are valuable instruments in adult samples, the assessment of HRQoL in children and adolescents has remained a scientific challenge. In German rehabilitation research studies on children and adolescents with chronic health conditions, the revised version of the KINDL, the KINDL-R (URL:http://www.kindl.org), is often used (Ravens-Sieberer et al. 2005).
KINDL-R
The KINDL-R represents a German-language instrument, which is also available in English and a number of other languages. Three self-report versions exist, each applicable for a different age group: Kiddy-KINDL-R, for children aged 4–7 years; Kid-KINDL-R, for children aged 8–12 years, Kiddo-KINDL-R, for children aged 13–16 years. Additionally, two proxy versions for parents are available: for parents with children aged 4–7 years and for those with children aged 8–16 years. The KINDL-R core set consists of 24 Likert-scaled items assessing six dimensions based on four items each: physical well-being, emotional well-being, self-esteem, family, friends and everyday functioning (school or nursery school). The subscales can be combined to a total score. All versions of the KINDL-R contain an additional module entitled “Disease”. This module consists of a filter question and six items measuring the HRQoL addressing the children’s illness. Existing disease-specific modules are obesity, bronchial asthma, atopic dermatitis and diabetes. The practicability and psychometric properties of the KINDL-R have been evaluated in a sample of children and adolescents (n=1020; 8–17 years) with diagnoses of obesity, asthma or atopic dermatitis. Participants filled in the KINDL-R core set plus the relevant disease-specific module at the beginning and the end of an inpatient rehabilitation treatment as well as at 3 and 12 months after treatment. The results demonstrated good psychometric properties. Additionally, gender-, age- and diagnosis-specific impairments were found, particularly for children with obesity and for those with the highest degree of obesity, respectively. In sum, the results suggest that the KINDL-R is a feasible and valid instrument for assessing HRQoL in children and adolescents with chronic disorders in inpatient rehabilitation settings.
Furthermore, the KIDSCREEN project (Ravens-Sieberer et al. 2001; URL:http://www.kidscreen.org) funded by the European Union should be mentioned. The aim of the KIDSCREEN project is the cross-national development of a questionnaire measuring HRQoL in children aged from 8 to 18 years. Three versions are currently available: the KIDSCREEN-52 (long version), the KIDSCREEN-27 (short version) and the KIDSCREEN-10 index, all of which offer a global HRQoL score. The three questionnaires assess HRQoL from a child’s perspective in terms of physical, mental and social well-being. However, further research is needed to evaluate the benefit of these HRQoL instruments in pediatric rehabilitation.
Preference-based HRQoL measurements
The generic instruments described above measure quality of life as a health profile, focusing on the evaluation of several domains. In contrast, the aim of instruments for use in economic evaluations is to obtain a single index score that reflects peoples’ preferences of different health states (Froberg and Kane 1989). Increasing numbers of health economic evaluation studies on medical treatments have been carried out in recent years. Currently, several preference-based instruments are available in the German language: EQ-5D, Short Form-6 Dimensions (SF-6D), Health Utilities Index Mark 2 (HUI Mark 2), 15D-questionnaire and the Quality of Well-Being-Self-Administered (QWB-SA). These instruments are described here and in Table 2.
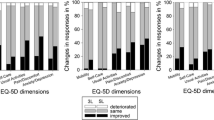
EQ-5D
The EQ-5D consists of five dimensions, each with three items. The descriptive system allows for 243 discrete health states. In addition, a visual analogue scale (EQ-VAS) measures participants’ current health on a scale, anchored by worst (0) and best (100) imaginable health state. As the only preference-based measure which has been thoroughly tested and validated in Germany (Schulenburg et al. 1998), the EQ-5D is to date the most frequently used and the one recommended for the utility-oriented assessment of patient outcomes (Hessel et al. 1999; Krauth et al. 2003). In a study on rehabilitation inpatients with chronic low back pain, the EQ-5D was demonstrated to be a useful instrument in rehabilitation research (Seitz et al. 2001).
SF-6D
The aim of the SF-6D was to extract utility values from the profile instrument SF-36 (Brazier et al. 2002). The SF-6D consists of six dimensions derived from 11 items of the SF-36. The number of levels per item ranges between four and six. The SF-6D utility score is based on a representative sample of the general population from the United Kingdom. The SF-6D can also be used as an independent instrument.
Health Utilities Index Mark 2 (HUI Mark 2)
The HUI Mark 2 is the second version of the Canadian HUI questionnaire family (Torrance et al. 1996) and describes six ‘plus one’ dimensions of sensory and communication abilities. The questionnaire comprises 15 items with three to five response categories. The HUI Mark 2 preference scores were estimated in a sample of parents in Hamilton, Ontario. The translation into German and the validation was carried out in a sample of childhood cancer survivors by Felder-Puig et al. (2000).
Quality of well-being scale-self-administered (QWB-SA)
The QWB-SA is based on the interviewer version of a questionnaire (Kaplan et al. 1976, 1997) and includes five sections of HRQoL (Sieber et al. 2004). Chronic symptoms or problems are assessed as present or absent, while all other symptoms and problems are evaluated only for the last 3 days preceding the interview. The German version was analyzed with respect to psychometric properties, validity, and reliability in clinical samples with current diagnosis of prostate cancer, benign prostatic hyperplasia, colon cancer and rectal cancer (Frosch et al. 2001).
15D
The 15D questionnaire was developed in Finland and consists of 15 items, each with five response levels (Sintonen 1994). Values for the 15D were derived from a sample of the Finnish population. The German translation was carried out by Arno Brandt (H. Sintonen, personal communication).
The psychometric properties and feasibility of the German versions from the EQ-5D, SF-6D, HUI Mark 2, 15D and QWB-SA were recently compared in a longitudinal study in rehabilitation inpatients with musculo-skeletal, cardiovascular or psychosomatic disorders (Moock et al. 2005). In terms of missing values, all instruments appeared to be highly acceptable. Ceiling effects were acceptable as well. However, comparisons of distributions and mean index scores demonstrated that results obtained with different preference-based measures were not equivalent. If small changes are expected in evaluative studies, the 15D or the SF-6D should be used.
Evaluation of specific therapy and education programs
The development of assessments to evaluate specific therapy and education programs of rehabilitation settings was a main focus in the German Research Funding Program “Rehabilitation Sciences” (Zwingmann et al. 2004). In the following, an instrument assessing the fear of illness progression in samples of patients with chronic disorders is presented, and a brief report on two other measurements evaluating educational programs in rehabilitation is given.
Fear of Progression Questionnaire (FoP-Q)
One of the most important aspects of psychological distress in patients with confirmed diseases (e.g. cancer, diabetes mellitus, and arthritis) is the fear of illness progression. As the fear of progression (FoP) may have a substantial impact on quality of life, specific treatment is appropriate. To develop treatments reducing FoP, questionnaires assessing patients’ distress related to FoP are necessary.
The “Fear of Progression Questionnaire” (FOP-Q) is a psychological questionnaire measuring FoP in patients with chronic diseases (Herschbach et al. 2005). The development of this questionnaire was undertaken in three stages. The initial questionnaire with 87 items was psychometrically tested in a sample of rehabilitation inpatients (n=411). On the basis of these results, 43 items were selected to describe five subscales: affective reaction (13 items), partnership/family (seven items), occupation (seven items), loss of autonomy (seven items) and coping with anxiety (nine items). The FoP-Q was subsequently adopted in a new sample of rehabilitation inpatients with chronic diseases (n=439) to evaluate convergent and discriminative validity. The correlation coefficients of the FoP-Q total score and other psychiatric measurements (HADS depression, HADS anxiety, SCL-90-R anxiety, SCL-90-R phobic anxiety and SF-12 physical and mental sub-scales) were moderate and ranged between 0.51 and 0.66. Within defined subgroups of patients with varying disease duration the discriminative power of the FoP-Q was found to be suitable. In sum, the results demonstrated that the FoP-Q is a questionnaire which is independent from other anxiety and depression scales and which is suited to discriminate within patient groups. As a well-accepted, short and economic instrument it can be used to assess FoP in samples of rehabilitation patients with chronic diseases. The FoP-Q is also available in English language. However, only the German version has been tested at the present time for its psychometrical properties.
Two additional instruments were developed for evaluating educational programs. The first is the “Bath Ankylosing Spondylitis Disease Activity Index” (BASDAI; Garrett et al. 1994), which defines the disease status in rehabilitation patients with ankylosing spondylitis (AS) and related diseases. It was translated into German and validated in a sample of rehabilitation inpatients with AS and other spondarthropathies at the beginning and the end of treatment (n=318; Bönisch and Ehlebrecht-König 2003). The BASDAI consists of six 10-cm horizontal visual analogue scales measuring severity of fatigue, spinal and peripheral joint pain, tenderness and morning stiffness. In conclusion, the BASDAI-D is a valid and reliable instruments for patients with AS. As a result of its good feasibility and practicability, the BASDAI-D is suggested for use in medical rehabilitation research.
The second is the “Self-efficacy Scale for Parents of Pre-schoolers with Atopic Dermatitis” (SEND), which is a disease-specific instrument. This questionnaire consists of nine items with six levels each (Buchholz et al. 2003). Psychometric analyses in a sample of parents (primarily mothers) of pre-schoolers with atopic dermatitis n=163), which obtained an intensive medical examination program, demonstrated that the SEND is an applicable and usable assessment for the evaluation of atopic dermatitis-specific interventions.
Motivation
The achievement of rehabilitation treatment depends on a patient’s individual motivation and compliance. However, the assessment of motivation with regard to methodological and content-specific aspects is complex. Nevertheless, several instruments assessing the motivation to participate in rehabilitation treatment have been developed in the last years. Two instruments are of particular interest in rehabilitation research and will be discussed here in some detail. An overview of various measurements evaluating motivation in psychotherapy is given by Zwerenz et al. (2005).
Questionnaire for Assessing Rehabilitational Motivation (FREM-17)
The “Questionnaire for Assessing Rehabilitational Motivation” (FREM-17; Deck et al. 1998) is a generic instrument based on the “expectancy-value theory” (Weiner 1992). The FREM-17 was developed to measure the expectation and motivation of inpatients within the framework of rehabilitation treatment. Further research revealed that it is sufficient to confine the questionnaire to the expectancy component (Deck 1999). The current version of the FREM-17 consists of 17 items representing four domains: regeneration (five items), health (four items), coping (four items) and retirement (four items). Practicability and psychometric properties were tested in a sample of rehabilitation inpatients with non-specific low back pain. The results suggest that the FREM-17 is a practicable, reliable and valid instrument by which to assess rehabilitation motivation. In addition, an economic short version, the FREM-8, is available.
Patient Questionnaire of Rehabilitation Motivation (PAREMO)
Yet another instrument assessing motivation is the “Patient Questionnaire of Rehabilitation Motivation” (PAREMO; Hafen et al. 2001). The PAREMO contains 46 items relating to six domains: need for assistance and psychological burden of suffering (eight items), restrictions in everyday life because of the physical burden of suffering (six items), reactions of significant others to the illness (six items), readiness to change in terms of preventive behavior (eight items), hopelessness and skepticism (four items) and initiative and knowledge (six items). The PAREMO was tested in five samples of rehabilitation inpatients with musculo-skeletal, cardiovascular, pulmonary, oncological or psychosomatic disorders and was found to be a practical, reliable and valid instrument. A short version, the PAREMO-20, is also available (Kriz et al. 2006). A manual of the PAREMO-20 in German is available online at (http://www.psychologie.uni-freiburg.de/abteilungen/Rehabilitationspsychologie/forschung1/downloads/PAREMO_20_Kurzmanual%201%20.pdf/).
With the FREM-17 and the PAREMO researchers have two highly accepted generic instruments for assessing rehabilitation motivations. In addition, a number of other instruments have been developed with the objective of measuring specific aspects of motivation. For example, the RELEIMO questionnaire was developed to measure rehabilitation-related activity motivation (Muthny et al. 2005), and the first results from a sample of rehabilitation inpatients with musculo-skeletal disorders showed that it has satisfactory psychometric properties. The HAMORE scale, which is based on the “Health Action Process Approach (HAPA)” (Schwarzer 1992), was developed to predict the degree of inpatients’ cooperation and willingness during rehabilitation treatment (Kühn et al. 2001). Finally, the FBTM (Fragebogen zur berufsbezogenen Therapiemotivation) assesses the motivation of rehabilitation patients with psychosomatic disorders for vocational reintegration (Zwerenz et al. 2005). It consists of 24 items describing four subscales: intention to change, wish for pension, negative treatment expectations and active coping. The FBTM was validated in a sample of rehabilitation inpatients with psychosomatic disorders (n=282). The results showed moderate to strong reliability coefficients and only small correlations between the four subscales. Ongoing studies address the sensitivity and predictive validity of the FBTM.
The motivation-related instruments mentioned above are based on the assumption that the motivation to participate actively in a rehabilitation treatment is a multidimensional construct. However, the questionnaires differ greatly in the domains that they cover and were designed as either generic or disease-specific tools. Further research projects comparing the questionnaires with respect to psychometric properties, feasibility and practicability are required.
Screening for vocational problems
The return to work and avoidance of early retirement are essential outcome parameters of rehabilitation. Accordingly, the development of instruments assessing the subjective likelihood for return to work is a fundamental challenge within the scientific community of rehabilitation research. Several instruments have been developed and validated during the past few years, and a comprehensive overview of these is given by Fiedler et al. (2005). The ISI questionnaire (Isnyer Rückkehr Inventar) measures the duration between the rehabilitation treatment and return to work (Dern and Rass 2002). It consists of ten gender-specific items. The AVEM (Arbeitsbezogenes Verhaltens- und Erlebensmuster) is a 66-item questionnaire with five response-levels each, and it assesses the return to work motivation (Schaarschmidt and Fischer 1997, 1998). The questionnaire was standardized and psychometrically tested in a sample of German schoolteachers (n=1589). The results addressing reliability, and convergent validity were substantial. The AVEM seems to be a highly accepted and economic instrument by which to assess the motivation to work. The SPE-scale is a short instrument (three items) assessing the subjective prognosis of the return to work (Mittag and Raspe 2003, Mittag et al. 2003a). Feasibility and psychometric properties were tested in a cohort of blue-collar workers (n=4279), and the results suggest that the SPE-scale can be recommended for use in rehabilitation research to assist the medical appraisal.
All of these instruments can assist in the adjustment and modification of interventions and treatment programs addressing individual requirements. However, further research is needed that compares the psychometric properties of questionnaires screening for vocational problems.
Screening for comorbid mental disorders
Comorbid mental disorders can affect the motivation and compliance of rehabilitation patients to participate in treatment programs. When comorbid mental disorders occur, patients are likely to require specific treatments. The identification and classification of comorbid mental disorders have major implications for rehabilitation. Therefore, valid screening instruments at the beginning of rehabilitation treatment are needed. In rehabilitation research studies, German adaptations of the General Health Questionnaire (GHQ-12, 12 items), the Hospital Anxiety and Depression Scale (HADS-D, 14 items) and a short version of the Patient Health Questionnaire (PHQ-D, Löwe et al. 2002) have been adopted for screening comorbid mental disorders in rehabilitation patients. The GHQ questionnaire was originally developed as a 60-item questionnaire (Goldberg and Blackwell 1970), and the shorter GHQ-12 was subsequently derived from longer versions. The GHQ-12 measures whether the respondent has experienced a particular symptom or behavior recently (Schmitz et al. 1999). The instrument has been thoroughly psychometrically tested and validated in several languages and compared to the longer versions of the GHQ (GHQ-30, GHQ-28 and GHQ-20). The results showed that the short version is a feasible instrument to screen for comorbid mental disorders.
The HADS is a widely used screening instrument assessing psychological distress. Several studies have demonstrated that the HADS is a valid instrument which provides clinicians with information on relevant comorbid mental disorders (Mykletun et al. 2001). The questionnaire is based on 14 items that describe two subscales: anxiety (seven items) and depression (seven items). In a German sample of rehabilitation inpatients with cardiovascular (n=213) or musculo-skeletal (n=206) disorders, the GHQ-12 and the HADS-D were compared with respect to discriminate validity (Wunsch et al. 2002). In both patient groups the HADS-D showed a better screening performance than the GHQ-12. However, the limitation in performance is the result of the different methodological approaches intrinsic to the instruments and the difficulties in screening for mental disorders in patients with physical disease. Thus, the authors recommend both questionnaires be used for the identification of comorbid mental disorders in samples of rehabilitation patients with cardiovascular or musculo-skeletal disorders.
The decision as to which screening instrument should be applied depends on several considerations (e.g. study design, and diagnostic group). Accordingly, a set of different assessment instruments aimed at assessing rehabilitation could be useful. Comprehensive proposals for rehabilitation patients with cardiovascular disorders are given by Mittag et al. (2004), and those for patients with chronic low back pain are given by Schreiber et al. (2004).
Discussion
Monitoring the health status of patients has become a major activity in rehabilitation research in recent years. Intensive research and controversial discussions within the scientific community have resulted in a paradigm shift in monitoring and evaluating health. In addition to conventional clinical endpoints and medical appraisals, patient-reported outcomes have gained importance as an outcome criterion.
During the past decades an increasing number of questionnaires have been developed in Germany, including, for example, the IRES, the FREM-17 and the SPE-scale. Additionally, widely used international instruments, such as the NHP or the SF-36, have been translated into the German language and adapted for use in Germany. These instruments have been thoroughly tested and validated in several studies. Current trends in statistical methods (e.g. responsiveness, Rasch scaling) as well as classical test-theoretical standards were considered. Thus, instruments assessing patient-reported outcomes in rehabilitation research achieve current psychometrical standards.
The ability to provide patient-reported assessments applicable in rehabilitation research projects has been one of the major aims of rehabilitation research during recent years. However, current projects attempt to contribute to the transfer of existing scientific knowledge on assessment instruments into practical rehabilitation applications. To alleviate the implementation of the datasets into existing questionnaire sets, several assessment instruments are available as short versions.
In summary, the contribution of questionnaires available in the field of rehabilitation research to other health care sectors exists at several levels: (1) to allocate various standardized instruments to routinely monitor subjective health, well-being and specific parameters of diseases; (2) to screen for and identify relevant impairments of physical and mental health; (3) to assess vocational impacts influencing health behavior; (4) to identify social and behavioral determinants of health which are relevant to patient participation in specific therapies or educational programs; (5) to screen for and observe comorbid disorders. However, there is still a need for further research to determine the best choice of instruments for a given purpose and the limitations of these tools in health care studies.
In conclusion, this review article provides an overview on patient-reported instruments in rehabilitation research. The Institute for Quality in Prevention and Rehabilitation (IPQR) provides an online database with descriptions of several assessments measuring patient-reported outcome (URL:http://www.assessment-info.de). An introduction to scoring methods for generic instruments in rehabilitation research is presented by Reusch (2002). Corresponding SPSS Syntax-files are provided on an enclosed CD-Rom. An extensive collection of SPSS Syntax-files that can be used to calculate scores of the instruments is available online (URL:http://www.rehawissenschaft.uni-wuerzburg.de/methodenberatung/assessment.html).
References
Bergner M, Bobitt RA, Carter WB (1981) The Sickness Impact Profile: development and final revision of a health status measure. Med Care 19:787–805
Bönisch A, Ehlebrecht-König I (2003) Der BASDAI-D-ein Fragebogen zur Erfassung der Krankheitsaktivität bei Spondylitis ankylosans und verwandten Erkrankungen. Z Rheumatol 62:251–263
Brazier J, Roberts J, Deverill M (2002) The estimation of a preference-based measure of health from the SF-36. J Health Econ 21:271–292
Buchholz HT, Warschburger P, von Schwerin AD, Petermann F (2003) SEND: Eine Skala zur Erhebung der spezifischen Selbstwirksamkeit für Eltern neurodermitiskranker Kinder. ZMP 12:63–68
Bührlen B, Gerdes N, Jäckel WH (2005) Entwicklung und psychometrische Testung eines Patientenfragebogens für die medizinische Rehabilitation (IRES-3). Rehabilitation 44:63–74
Bullinger M, Kirchberger I (1998) SF-36 Fragebogen zum Gesundheitszustand (SF-36). Handbuch für die deutschsprachige Fragebogenversion. Hogrefe, Göttingen
Bullinger M, Morfeld M, Kohlmann T, Nantke J, van den Bussche H, Dodt B, Dunkelberg S, Kirchberger I, Krüger-Bödecker A, Lachmann A, Lang K, Mathis C, Mittag O, Peters A, Raspe H, Schulz H (2003) Der SF-36 in der rehabilitationswissenschaftlichen Forschung-Ergebnisse aus dem Norddeutschen Verbund für Rehabilitationsforschung (NVRF) im Förderschwerpunkt Rehabilitationswissenschaften. Rehabilitation 42:218–225
Deck R (1999) Erwartungen und Motivationen in der medizinischen Rehabilitation. Ihre sozialmedizinische und gesundheitspolitische Bedeutung für den Rehabilitationserfolg. Jacobs, Lage
Deck R, Zimmermann M, Kohlmann T, Raspe H (1998) Rehabilitationsbezogene Erwartungen und Motivationen bei Patienten mit unspezifischen Rückenschmerzen. Rehabilitation 37:140–146
Dern W, Rass G (2002) Geschlechts-und statusspezifische Prädiktoren beeinflussen den Weg zurück zur Arbeit. DRV-Schriften 33:332–334
Felder-Puig R, Frey E, Sonnleithner G, Feeny D, Gadner H, Barr RD, Furlong W, Topf R (2000) German cross-cultural adaptation of the Health Utilities Index and its application to a sample of childhood cancer survivors. Eur J Pediatr 159:283–288
Fiedler RG, Ranft A, Greitemann B, Heuft G (2005) Arbeitmotivation - Diagnostikinstrumente und ihre Relevanz in der Patientenversorgung. Zum Stand arbeitsbezogener Motivationsdiagnostik. Psychother Psych Med 55:469–475
Froberg DG, Kane RL (1989) Methodology for measuring health-state preferences I: measurement strategies. J Clin Epidemiol 42:345–354
Frosch D, Porzsolt F, Heicappell R, Kleinschmidt K, Schatz M, Weinknecht S, Kaplan RM (2001) Comparison of German language versions of the QWB-SA and SF-36 evaluating outcomes for patients with prostate disease. Qual Life Res 10:165–173
Garrett S, Jenkinson T, Kennedy GL, Whitelock H, Gaisford P, Calin A (1994) A new approach to defining disease status in ankylosing spondylitis: the bath ankylosing spondylitis disease activity index. J Rheum 21:2286–2291
Gerdes N, Jäckel WH (1995) Der IRES-Fragebogen für Klinik und Forschung. Rehabilitation 34:13–24
Glatzel M, Wollmerstedt N, Doesch M, Kirschner S, Matzer M, Faller H, König A (2004) Reliabilitäts-, Validitäts und änderungssensitivitätsprüfung des Funktionsfragebogen Bewegungsapparat (SMFA-D) bei operierten Patienten mit rheumatoider Arthritis. Aktuel Rheumatol 29:17–23
Goldberg DP, Blackwell B (1970) Psychiatric illness in general practice. A detailed study using a new method of case identification. Br Med J 1:439–443
Hafen K, Jastrebow J, Nübling R, Bengel J (2001) Entwicklung eines Patientenfragebogens zur Erfassung der Reha-Motivation (PAREMO). Rehabilitation 40:3–11
Herschbach P, Berg P, Dankert A, Duran G, Engst-Hastreiter U, Waadt S, Keller M, Ukat R, Henrich G (2005) Psychometric properties of the Fear of Progression Questionnaire. J Psychosom Res 58:505–511
Hessel F, Kohlmann T, Krauth C, Nowy R, Seitz R, Siebert U, Wasem J (1999) Gesundheitsökonomische Evaluation in der Rehabilitation. Teil 1: Prinzipien und Empfehlungen für die Leistungserfassung. In: Verband Deutscher Rentenversicherungsträger (ed) Förderschwerpunkt “Rehabilitationswissenschaften”. “Empfehlungen der Arbeitsgruppen Generische Methoden”, “Routinedaten” und “Reha-ökonomie”. DRV-Schriften 16:106–193
Hunt SM, McKenna SP, McEwen J, Williams J, Papp E (1981) The Nottingham Health Profile: Subjective health status and medical consultations. Social Sci Med 15:221–229
Kaplan RM, Bush JW, Berry CC (1976) Health status: types of validity and the index of well-being. Health Serv Res 11:478–507
Kaplan RM, Sieber WJ, Ganiats TG (1997) The Quality of Well-Being Scale: Comparison of the interviewer-administered version with a self-administered questionnaire. Psychol Health 12:783–791
Kirschner S, Walther M, Boehm D, Matzer M, Heesen T, Faller H, König A (2003) German short musculoskeletal function assessment questionnaire (SMFA-D): comparison with the SF-36 and WOMAC in a prospective evaluation in patients with primary osteoarthrits undergoing total knee arthroplasty. Rheumatol Int 23:15–20
König A, Kirschner S, Walther M, Böhm D, Faller H (2000) I. Kulturelle Adaptation, Praktikabilitäts- und Reliabilitätsprüfung des Funktionsfragebogen Bewegungsapparat (SMFA-D). Z Orthop 138:295–301
Krauth C, Rieger J, Mellert C, Schwartz FW (2003) Das Gesundheitsheitökonomische Querprojekt Q3: überblick über die Konzeption der reha-ökonomischen Evaluation. In: Petermann F (ed) Prädiktion, Verfahrensoptimierung und Kosten in der medizinischen Rehabilitation. Roderer, Regensburg, pp 47–60
Kriz D, Nübling R, Herwig JE, Fuchs S, Bengel J (2006) Normierung des PAREMO-20-Patientenfragebogen zur Erfassung der Rehabilitationsmotivation. DRV-Schriften 64:161–162
Kühn A, Pannicke L, Mohs A, Schneider H (2001) Entwicklung eines Fragebogens zur Erfassung motivationaler Bedingungen zur Vorhersage der Therapiemitarbeit von LVA-Versicherten während stationärer medizinischer Rehabilitation - Erste Ergebnisse der Skalenentwicklung. Rehabilitation 40:165–174
Löwe B, Spitzer RL, Zipfel S, Herzog W (2002) PHQ-D. Gesundheitsfragebogen für Patienten. Pfizer, Karlsruhe
Maurischat C, Krüger-Bödecker A (2004) Analysen zum Strukturmodell des SF-36/SF-12-eine übersicht. In: Maurischat C, Morfeld M, Kohlmann T, Bullinger M (ed) Lebensqualität. Nützlichkeit und Psychometrie des Health Survey SF-36/SF-12 in der medizinischen Rehabilitation. Pabst, Lengerich, pp 29–48
Mittag O, Raspe H (2003) Eine kurze Skala zur Messung der subjektiven Prognose der Erwerbstätigkeit: Ergebnisse einer Untersuchung an 4279 Mitgliedern der gesetzlichen Rentenversicherung zu Reliabilität (Guttman-Skalierung) und Validität der Skala. Rehabilitation 42:169–174
Mittag O, Glaser-Möller N, Ekkernkamp M, Matthis C, Hèon-Klein V, Raspe A, Raspe H (2003a) Prädiktive Validität einer kurzen Skala zur subjektiven Prognose der Erwerbstätigkeit (SPE-Skala) in einer Kohorte von LVA-Versicherten mit schweren Rückenschmerzen oder funktionellen Beschwerden der Inneren Medizin. Soz Praventivmed 48:361–369
Mittag O, Budde HG, Eisenriegler E, Engel S, Herrmann-Lingen C, Jokiel R, Langosch W, Lueger S, Mai B, Niehues U, Schoel M, Maurischat C (2004) Ein Fragebogenset zur Erfassung (Screening) psychischer Störungen und sozialer Probleme von Patienten in der kardiologischen Rehabilitation. Rehabilitation 43:375–383
Moock J, Kohlmann T, Besch D, Drüner K (2005) Nutzentheoretische Lebensqualitätsmessinstrumente in der medizinischen Rehabilitation: Ein anwendungsbezogener Vergleich. ZMP 14:25–32
Mühlig S, Teeling H, Petermann F (2000) FLAC-Der Fragebogen zur Lebensqualität bei Asthma und Chronisch-obstruktiver Bronchitis. In: Schumacher J, Klaiberg A, Brähler E (ed) Diagnostische Verfahren zu Lebensqualität und Wohlbefinden. Hogrefe, Göttingen pp 135–140
Muthny FA, Fiedler R, Wiedebusch S (2005) Leistungsmotivation als Teilaspekt der Reha-Motivation und Einflussgröße auf den Reha-Erfolg-neue Skalen und empirische Ergebnisse. DRV-Schriften 59:203–204
Mykletun A, Stordal E, Dahl AA (2001) Hospital Anxiety and Depression (HAD) scale: factor structure, item analyses and internal consistency in a large population. Br J Psychiatr 179:540–544
Ravens-Sieberer U, Gosch A, Abel T, Auquier P, Bellach B-M, Bruil J, Dür W, Power M, Rajmil L, KIDSCREEN Group (2001) Quality of life in children and adolescents: A European public health perspective. Soz Praventivmed 46:294–302
Ravens-Sieberer U, Redegeld M, Bauer CP, Mayer H, Stachow R, Kiosz D, van Egmond-Fröhlich B, Rempis R, Kraft D, Bullinger M (2005) Lebensqualität chronisch kranker Kinder und Jugendlicher in der Rehabilitation. ZMP 14:5–12
Reusch A (2002) Skalenberechnung ausgewählter Instrumente. In: Reusch A, Zwingmann C, Faller H (ed) Empfehlungen zum Umgang mit Daten in der rehabilitationsforschung. Roderer, Regensburg pp 37–60
Seitz R, Schweikert B, Jacobi E, Tschirdewahn B, Leidl R (2001) ökonomisches Rehabilitations-management bei chronischen Rückenschmerzen. Der Schmerz 15:448–452
Schaarschmidt U, Fischer AW (1997) AVEM - ein diagnostisches Instrument zur Differenzierung von Typen gesundheitsrelevanten Verhaltens und Erlebens gegenüber der Arbeit. Zeitschrift für Differentielle und Diagnostische Psychologie 18:151–163
Schaarschmidt U, Fischer A (1998) Diagnostik interindividueller Unterschiede in der psychischen Gesundheit von Lehrerinnen und Lehrern zum Zwecke einer differentiellen Gesundheitsförderung. In: Bamberg E, Ducki A, Metz AM (ed) Handbuch Betriebliche Gesundheitsförderung. Verlag für Angewandte Psychologie, Göttingen
Schmitz N, Kruse J, Tress W (1999) Psychometric properties of the General Health Questionnaire (GHQ-12) in a German primary care. Acta Psychiatr Scand 100:462–468
Schreiber B, Bandemer-Greulich U, Uhlemann K, Müller K, Müller-Pfeil J, Kreutzfeldt A, Fikentscher E, Bahrke U (2004) Behandlungsspezifik beim chronischen Rückenschmerz: Ist die optimierte Rehabilitationszuweisung ausreichend? Rehabilitation 43:142–151
Schulenburg J-M, Graf von der, Claes C, Greiner W, Uber A (1998) Die deutsche Version des EuroQol-Fragebogens. Z Gesundheitswissenschaft 6:3–20
Schwarzer R (1992) Self-efficacy in the adoption and maintenance of health behaviors: Theoretical approaches and a new model. In: Schwarzer (ed) Self-efficacy: Thought control of action. Hemiphere, Washington D.C., pp 217–242
Sieber WJ, Groessl EJ, David KD, Ganiats TG, Kaplan RM (2004) Quality of Well-Being Self-Administered (QWB-SA) Scale. User’s Manual. Online Available: http://medicine.ucsd.edu/fpm/hoap/QWB_SA.pdf
Sintonen H (1994) The 15D-Measure of health-related quality of life. II Feasibility, reliability and validity of valuation system. National Health and Medical Research Council (National Centre for Health Program Evaluation) Working Paper 42, Melbourne, Australia
Swiontkowski MF, Engelberg R, Martin DP, Agel J (1999) Short Musculoskeletal Function Assessment Questionnaire: Reliability, validity and responsiveness. J Bone Joint Surg 81:1245–1260
Torrance GW, Feeny DH, Furlong WJ, Barr RD, Zhang Y, Wang Q (1996) Multiattribute utility function for a comprehensive health status classification system – Health Utilities Index Mark 2. Medical Care 34:702–722
Ware JE, Sherbourne CD (1992) The MOS 36-item Short-Form Health Survey (SF-36): I. Conceptual framework and item selection. Medical Care 30:473–483
Weiner B (1992) Expectancy-value theories. In: Weiner B (ed) Human motivation. Metaphors, theories, and research. Sage, Newsbury Park, pp 159–220
Wirtz M, Farin E, Bengel J, Jäckel WH, Hämmerer D, Gerdes N (2005) IRES-24 Patientenfragebogen – Entwicklung der Kurzform eines Assessmentinstrumentes in der Rehabilitation mittels Mixed-Rasch-Analyse. Diagnostica 51:75–87
Wollmerstedt N, Kirschner S, Böhm D, Faller H, König A (2003) Entwicklung und Evaluierung der Kurzversion des Funktionsfragebogens Bewegungsapparat XSMFA-D. Z Orthop 141:718–724
Wollmerstedt N, Kirschner S, Wolz Th, Ellßel J, Beyer W, Faller H, König A (2004) Validitäts- und änderungssensitivitätsprüfung des Funktionsfragebogens Bewegungsapparat (SMFA-D) in der stationären Rehabilitation von Patienten mit konservativ behandelter Coxarthrose. Rehabilitation 43:233–240
Wunsch A, Rundel M, Härter M, Bengel J (2002) Screening psychischer Störungen in der kardiologischen und orthopädischen Rehabilitation. Rehabilitation 41:375–381
Zwerenz R, Knickenberg RJ, Schattenburg L, Beutel ME (2005) Motivation zur psychosomatisch-psychotherapeutischen Bearbeitung von beruflichen Belastungen-Entwicklung und Validierung eines Fragebogens. Rehabilitation 44:14–23
Zwingmann C, Buschmann-Steinhage R, Gerwinn H, Klosterhuis H (2004) Förderschwerpunkt “Rehabilitationswissenschaften”: Ergebnisse - Umsetzung - Erfolge und Perspektiven. Rehabilitation 43:260–270
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Moock, J., Kohlmann, T. & Zwingmann, C. Patient-reported outcomes in rehabilitation research: instruments and current developments in Germany. J Public Health 14, 333–342 (2006). https://doi.org/10.1007/s10389-006-0065-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-006-0065-1