
Abstract
Purpose
To compare the distance of the medial rectus muscle insertion to the limbus (DMIL) between patients with acute acquired comitant esotropia (AACE) associated with excessive digital device usage (EDDU) and exotropic patients.
Study design
Retrospective study.
Methods
The medical records of 72 eyes of 44 patients with EDDU were retrospectively analyzed. The DMIL was measured from the anterior part at the midpoint of the medial rectus muscle insertion into the anterior limbus using a caliper after dissecting the medial rectus muscle with two control sutures at 12 o’clock and 6 o’clock. The DMIL in the non-fixation eye was compared between 44 patients with AACE and 23 patients with exotropia.
Results
The mean daily EDDU was 6.5 ± 3.1 h. The mean cycloplegic refractive errors (spherical equivalent: SE) were − 3.18 ± 2.52 diopters (D) OD and − 3.03 ± 2.42 D OS. The mean DMIL in the 72 eyes of 44 patients with AACE associated with EDDU was 4.30 ± 0.66 mm. The difference in DMIL of non-fixation eyes between 44 AACE patients and 23 exotropic patients was significant (4.28 ± 0.65 mm vs. 5.28 ± 0.50 mm, p < 0.0001). However, the SE in 44 non-dominant eyes of AACE was − 3.08 ± 2.56 D, significantly stronger than − 1.22 ± 1.93 D in the 23 exotropic eyes (p = 0.008).
Conclusion
DMIL in patients with AACE associated with EDDU was significantly shorter. This anatomical anomaly may be an etiology of AACE associated with EDDU.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute acquired comitant esotropia (AACE) is a special subtype of esotropia characterized by acute onset in younger children with diplopia and equal deviation in all gaze directions. AACE is historically classified into three types according to its clinical characteristics and etiologies: (1) Swan type, disruption of fusion resulting from monocular occlusion or visual loss; (2) Franceschetti type, an acutely large angle of deviation caused by psychological stress or associated with small hyperopia with or without an accommodative element; (3) Bielschowsky type, uncorrected moderate myopia, mostly in adolescents and adults [1,2,3,4].
Recently, a new entity of AACE associated with excessive digital device usage (EDDU), which includes the use of smartphones, tablets, and computers for near work activities involving screen time, including internet browsing in everyday life, has increasingly been reported [5,6,7,8,9,10,11]. In most reports, EDDU is defined as usage exceeding 5 h per day [5,6,7, 11]. However, from a Japanese national survey on Internet usage among youth in 2021 by the cabinet office of the government of Japan (https://www8.cao.go.jp/youth/kankyou/internet_torikumi/tyousa/r03/net-jittai/pdf-index.html. In Japanese), the average Internet usage among youth aged 6–18 years is 4.4 h per day. In relation to this survey, the usage for more than 5 h per day in previous reports of AACE associated with EDDU may not be excessive. Therefore, there may be other risk factors for the development of AACE in addition to EDDU.
In 2019, Cai et al. reported that the distance from the medial rectus muscle insertion to the limbus (DMIL) in 43 patients with AACE was significantly shorter than in 50 patients with exotropia (4.8 ± 0.4 mm vs. 5.4 ± 0.4 mm, p < 0.001) [12]. Lekskul et al. also argue that the shorter DMIL in patients with AACE, augmented the amount of recession on Parks’ standard surgical number by 0.5–1.0 mm; moreover, DMIL in infantile esotropia is shorter, and this abnormal distance may be an etiology of esodeviation [13]. In 2022, Abdelhafez et al. reported similar findings. However, these 3 studies do not provide detailed explanations as to how the DMIL was measured. In 1989, Keech and et al. reported that DMIL varied during different stages of medial rectus recessions for infantile esotropia, with a maximum difference of 1.0 mm or more between four different stages [14]. Therefore, standardizing the methods to measure DMIL is crucial to avoid unintentional errors in the results of comparative data, including those from the three studies mentioned [12, 13, 15]. In this study, we investigated the differences in DMIL between 72 eyes of 44 patients with AACE associated with EDDU and 25 eyes of 23 patients with exotropia, following the detailed methods for measuring DMIL described in two previous studies [16, 17].
Materials and methods
Among the surgically aligned 71 cases diagnosed with AACE between 2015 and 2023, cases of the three historical types (Swan, Franceschetti, and Bielschowsky) were excluded after careful confirmation of a lack of history leading to these three types. Additionally, cases showing a tendency towards these historical types were also excluded from this study. Patients with a history of accommodative esotropia, strabismus surgery, neurological disorders, or amblyopia treatment with occlusion were also excluded. Using digital devices (DDs) ≥ 4 h per day before or at symptoms’ onset was defined as prolonged or excessive use of DDs, according to previous reports [5,6,7,8, 11, 12]. Finally, 44 patients with AACE associated with the prolonged use of DDs were retrospectively included in this study based on the definition of acute onset identified after interviewing about the sudden onset diplopia or esotropia.
At the initial visit, all patients underwent ophthalmic and orthoptic examinations, and diagnostic imaging with cranial and orbital computed tomography or magnetic resonance imaging to rule out paretic strabismus or other AACE caused by intracranial diseases. Cycloplegic refraction was performed after administering 1% atropine sulfate eye drops once daily for 3–5 days to eliminate accommodative effects, and the spherical equivalent (SE) of refractive error was calculated. Ocular motility was evaluated clinically using the Hess red-green test under prism neutralization to confirm concomitant esodeviation. Deviation was measured using the alternate prism cover test in all nine gaze positions with full refractive correction at distance and near. Binocular near and distance responses were evaluated using Bagolini-striated lenses. Near stereoacuity was assessed using the Randot stereo test (Stereo Optical) or the Titmus Stereo Test (Stereo Optical).
All surgery was performed under general anesthesia in patients < 15 years old and local anesthesia for those ≥ 15 years old by a single experienced surgeon (TY). The surgical procedure details for the 44 patients were: unilateral medial rectus recession (UMRR), 16 patients; bilateral medial rectus recession (BMRR), 27 patients; and BMRR with unilateral lateral rectus resection, one patient. The UMRR procedure was performed on the non-dominant eye. All strabismus surgery was performed with the limbal incision. DMIL measurements were made from the anterior part at the midpoint of the medial rectus muscle insertion to the anterior limbus, defined as the transition from the clear cornea to gray, with a caliper after dissecting the medial rectus muscle with two control sutures at 12 o’clock and 6 o’clock by a single surgeon (TY) (Fig. 1). In a comparative analysis, the DMIL in 25 eyes of 23 exotropic patients prospectively undergoing unilateral lateral rectus recession and medial rectus resection between 2020 and 2023 was measured in the same manner.

Measurement of the distance from the medial rectus muscle insertion to the limbus (DMIL). Measurement of DMIL were made from the anterior part at the midpoint of the medial rectus muscle insertion to the anterior limbus defined as the transition from a clear cornea to gray with a caliper after dissecting the medial rectus muscle with two control sutures at 12 o’clock and 6 o’clock (solid arrow)
This study was conducted in accordance with the tenets of the Declaration of Helsinki and approved by the Clinical Research Ethics Committee of the Japan Community Health Care Organization Chukyo Hospital (approval no. 2021030). The study protocols and data collection procedures complied with all local laws, and informed consent was obtained from all patients or their guardians after all study details had been explained. Neither patients nor the public were directly involved in the design, conduct, reporting, or dissemination plans of our research.
Statistical analyses were performed using Microsoft Excel for Mac version 16 (Microsoft Corp.) and StatMate version 5 (ATMS). Numerical data are expressed as mean ± standard deviation (SD) and were compared using Student’s t-test or Welch’s test. The relationships between the DMIL and deviation angle near and at a distance were analyzed using Pearson’s correlation coefficient. Statistical significance was set at p < 0.05.
Results
The basic patient characteristics are summarized in Table 1. The study included 44 patients with AACE (28 men and 16 women). The mean age at the initial visit was 22.0 ± 8.7 years. The duration from onset to the first visit ranged from 1 month to 5 years (median 2.3 years). None of the patients had a family history of strabismus, trauma, or eye occlusion. The external and anterior segments were normal in all patients. Fundus examination results were normal in all patients. The mean daily DD use was 6.5 ± 3.1 h (range, 4–14 h). The cycloplegic refractive error (SE) was − 3.19 ± 2.52 diopters (D) OD and − 3.03 ± 2.42 D OS. The best-corrected logMAR visual acuity was − 0.08 ± 0.10 OD and − 0.08 ± 0.09 OS. The preoperative angle of deviation was 28.2 ± 13.0 prism diopter (PD) (range, 8–55 PD) at distance and 25.3 ± 16.8 PD (range, 2–60 PD) at near.
During esotropic surgery (mean age at surgery: 23.1 ± 8.7 years, ranging from 12 to 41 years), the DMIL was carefully measured. The mean DMIL in 72 eyes of 44 cases was 4.30 ± 0.66 mm (4.31 ± 0.65 mm in 28 dominant eyes and 4.28 ± 0.65 mm in 44 non-dominant eyes; p = 0.489), significantly shorter than the 5.28 ± 0.50 mm observed in 23 exotropic eyes (mean age at surgery: 42.5 ± 22.8 years, ranging from 10 to 77 years) (p < 0.001). The cycloplegic refractive error (SE) in 44 non-dominant eyes with AACE was − 3.08 ± 2.56 D, significantly stronger than − 1.22 ± 1.93 D in 23 exotropic eyes (Table 2).
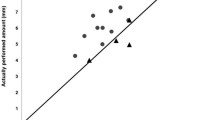
The correlation coefficients between the DMIL in the 44 non-dominant eyes and the deviation angle were found to be non-significant (at distance: r = -0.040, p = 0.808; at near: r = 0.047, p = 0.770). The correlation coefficients between DMIL in the 44 non-dominant eyes and the age at surgery were also not significantly different (r=-0.179, p = 0.245).
At the final visit, both binocular responses at near and distance were positive in all patients. Near stereoacuity was measurable in all patients, with a mean stereoacuity of 58.6 arc seconds (”) (ranging from 20” to 3,000”) and a mean log10 stereoacuity of 1.77 ± 0.44 (Table 1). The mean DMIL in 29 patients with fine stereoacuity (≤ 60”) was 4.38 ± 0.64 mm, and in 15 patients with coarse stereoacuity (60”<, ≤ 3000”) it was 4.10 ± 0.64 mm; the difference was not statistically significant (p = 0.858).
Discussion
AACE has been associated with accommodative spasms, myopia, hyperopia, intracranial diseases, or EDDU. However, the exact etiology remains unclear [18]. The average Internet usage among youth aged 6–18 years in Japan was 4.4 h per day in 2021, according to a national survey. This is nearly equivalent to the definition of EDDU in AACE. However, EDDU alone cannot be completely involved in the mechanism of the pathogenesis of this new entity [18]. In general, the principle of etiology and the natural history of a disease are essential for recognizing multiple contributing factors across any illness spectrum [19]. Therefore, other relevant factors in the development of AACE associated with EDDU should be investigated in detail.
Knowledge of the anatomic characteristics of the extraocular muscles, including muscle insertion, is important to understand the physiology of eye movements and clarify the etiology of strabismus. Several investigations of the DMIL in patients with infantile esotropia are reported [14,15,16,17,18]. In 1978, Helveston et al. reported that the mean DMIL was 4.4 mm (ranging from 3.0 to 6.0 mm) in 57 patients with infantile esotropia [16]. In 1990, Keech et al. reported a mean DMIL of 4.4 mm in 40 patients with infantile esotropia, using the same measurement method [14]. In 1995, Yoshida et al. compared the differences in DMIL between 58 eyes of 29 cases with infantile esotropia and with other esotropia in infancy employing the same measuring method used in this report and found a significantly shorter DMIL of 4.09 ± 0.85 mm in patients with infantile esotropia compared to 5.25 ± 0.27 mm (p < 0.01) in cases with partially accommodative esotropia and 4.90 ± 0.89 mm (p < 0.01) in cases with other esotropia in infancy [17]. However, these reports did not compare the DMIL between children with infantile esotropia and non-strabismic children. In 1980, Apt reported that the normal distance between the anterior limbus and the anterior edge of the insertion of the medial rectus muscle using 100 consecutive adult autopsy eyes was 5.3 ± 0.7 mm [20], almost equal to the normal distance of the medial rectus muscle (5.5 mm) in most textbooks and previous articles [21,22,23,24]. Compared to these values, it is assumed that the DMIL in patients with infantile esotropia is significantly shorter than in normal eyes. Although the etiology of infantile esotropia is unclear, it is assumed that one of the main factors responsible for infantile esotropia is the innervational imbalances between fusional convergence and divergence mechanisms. This abnormal innervation is strongly associated with a shorter DMIL.
There are only a few published reports regarding shorter DMIL in patients with AACE associated with EDDU, with one notable report by Cai et al. [12]. Their study included 45 patients, among whom 14 reported using smartphones or computers for more than 5 h per day before the onset of AACE. Although the DMIL measurement method is not explained in detail, they state that the mean DMIL in 43 patients with AACE (4.8 ± 0.4 mm) was significantly shorter than that of 50 patients with exotropia (5.4 ± 0.4 mm). In the present study, we also found a shorter DMIL in 44 eyes of 44 patients with AACE associated with EDDU compared to 23 eyes of 25 patients with exotropia (4.28 ± 0.64 mm vs. 5.28 ± 0.50 mm, p < 0.0001). As the mean DMIL in patients with exotropia in both studies was almost the same as in normal eyes, it can be concluded that patients with AACE associated with EDDU have a shorter DMIL than those with normal eyes. Although Bielschowsky thought that excessive near work produced unbalanced forces in the eyes for convergence and divergence as a cause of AACE despite uncorrected myopia [1], the etiology of AACE associated with EDDU remains unclear. However, Campos speculates that excessive near work with excessive accommodation followed by convergence spasms is a mechanism suggestive of AACE, and subsequent investigations support this speculation [25]. The mechanism of AACE associated with EDDU may be similar to that of Bielschowsky-type AACE, and EDDU may trigger AACE development whenever this mechanism is appropriate [26,27,28]. Ali et al. also suggest that patients with esophoria have enhanced divergence amplitudes to suppress manifest esotropia and that diplopia and manifest esotropia could occur in cases of failure of the divergence amplitude to overcome esophoria as an underlying mechanism of AACE [29]. In either case, esotropia may occur because of increased tonus of the medial rectus muscles, which can be stronger in the presence of a shorter DMIL. In addition to clinical results, Lekskul et al. also argue anatomically that a shorter DMIL in patients with AACE based on results of good outcomes in patients augments the amount of recession on Parks’ standard surgical number by 0.5–1.0 mm [13], and we adopted the same arrangement.
One of the essential aspects for comparing the results in this study with those in previous studies is the standardized method used to measure the DMIL. We measured the DMIL from the anterior part at the midpoint of the medial rectus muscle insertion to the anterior limbus with a caliper after dissecting the medial rectus muscle with two control sutures at 12 o’clock and 6 o’clock as recommended by Apt [20] and Keech et al. [17]. However, some previous studies do not provide detailed explanations for measuring the DMIL. Using 100 consecutive adult autopsied eyes, Apt reports that the distance between the anterior limbus, defined as the transition from a clear cornea to gray, and the posterior limbus, defined as the transition from the gray cornea to the white sclera, was 0.6 ± 0.1 mm, and that this width of the limbus can significantly influence comparisons of DMILs [20]. Keech et al. [17] and Apt [20] both recommend considering the normal distance between the anterior limbus and the anterior edge of the insertion of the medial rectus muscle as the DMIL. Pathologists, histologists, and ophthalmic surgeons define the limbus differently. The surgical limbus for ophthalmic surgeons is known as the gray zone, which spans a width of approximately 1.2 mm between the transparency of the cornea anteriorly and the white of the sclera posteriorly [30]. However, the anterior extent of the Tenon capsule and conjunctiva fuse with the episclera, and the exact position of the posterior limbus may be difficult to identify without a complete incision of the anterior extent of the Tenon capsule and conjunctiva [31]. Therefore, the anterior limbus is regarded as an easy landmark to identify. Recently, muscle insertion distance measurements using anterior segment optical coherence tomography (AS-OCT) have been reported [32, 33]. In these studies, the end of the cleft between the extraocular muscle and sclera was defined as the insertion of the rectus muscle. However, this position is not the anterior of insertion, which acts as the point of action of rotational force. Exact identification of the anterior edge of the medial rectus muscle insertion is crucial in the investigation of the relationship between DMIL and the mechanism of AACE associated with EDDU. Therefore, the muscle insertion distance measurements using AS-OCT should be more developed to identify the anterior edge of the rectus muscle insertion and the transitional point from the gray cornea to the white sclera.
Another factor that can influence the comparison of results is the variation in DMIL observed during muscle surgery for esotropia. Keech et al. compared DMILs during four different stages of BMRR for infantile esotropia to evaluate the variability of the DMIL: (1) before disinsertion of the muscle with the eye abducted by fixation forceps at the 12 o’clock and 6 o’clock meridian of the limbus, (2) before disinsertion of the muscle with the eye abducted by a muscle hook under the medial rectus muscle, (3) after disinsertion of the muscle with the eye abducted by fixation forceps at the 12 o’ clock and 6 o’clock meridian of the limbus, and (4) after disinsertion of the muscle with the eye abducted by fixation forceps at the superior and inferior poles of the muscle insertion site [17]. In measurements 1 and 2, the anterior part at the midpoint of the medial rectus muscle insertion was difficult to identify because of the presence of the muscular fascia, which is part of the fascial sheath (capsule of Tenon) before disinsertion of the muscle. In measurement 4, two fixation forceps at the superior and inferior poles of the muscle insertion site created a force to advance the insertion, which may be susceptible to measurement error. The limbus and insertion in measurement 3 were less influenced by the fixation forceps or traction sutures used to abduct the eyeball. Therefore, measurement 3 is thought to be the ideal method to measure the exact DMIL, and we recommend measurement 3 as the standard method for further studies.
In this study, comparisons were made between patients with AACE associated with EDDU and patients with exotropia. The SE in 44 non-dominant eyes with AACE was − 3.08 ± 2.56 D, significantly stronger than the − 1.22 ± 1.93 D observed in 23 exotropic eyes (Table 2). In general, the power of myopia and axial length are positively correlated. Based on the stronger SE observed in the 44 non-dominant eyes with AACE, it is presumed that the axial length in these eyes is longer. We believe that the stronger SE in esotropic eyes may not have an influence on the shorter DMIL.
This study had certain limitations. First, it is challenging to measure the DMIL in normal individuals with matched age and refraction, making it difficult to compare the DMIL in AACE associated with EDDU with that of normal participants. In patients with acquired esotropia, such as paralytic strabismus, the normal anatomical positions of the insertion of extraocular muscles are usually present before the onset of their disease. Therefore, their DMIL data can be considered comparatively normal. In this study, the correlation coefficients between DMIL in the 44 non-dominant eyes and the age at surgery (ranging from 12 to 41 years) were not significantly different. This indicates that abnormal DMIL in AACE associated with EDDU is not influenced by age. Therefore, we believe there is minimal risk of statistically significant differences arising from the younger mean age at surgery for AACE associated with EDDU compared to the control group. However, it is crucial to compare these findings with anatomically normal individuals. We started measuring the DMIL in all patients with paralytic esotropia after initiating this study. However, matching ages and refractions for statistical analysis is difficult, and we had a small number of DMIL measurements in patients with paralytic esotropia. In future, we plan to continue measuring the DMIL in normal participants for statistical comparisons between AACE associated with EDDU and comparative individuals to draw definite conclusions.
References
Bielschowsky A. Das Einwartfschien Der Myopia. Dtsch Ophthalmol Gesell. 1922;43:245–8. (in German).
Burian HM, Miller JE. Comitant convergent strabismus with acute onset. Am J Ophthalmol. 1958;45:55–64.
Clark AC, Nelson LB, Simon JW, Wagner R, Rubin SE. Acute acquired comitant esotropia. Br J Ophthalmol. 1989;73:636–8.
von Noorden GK, Campos EC. Acute acquired comitant esotropia: esodeviations. Binocular vision and ocular motility: theory and management of strabismus. 6th ed. St Louis: CV Mosby; 2002. pp. 338–40.
Lee HS, Park SW, Heo H. Acute acquired comitant esotropia related to excessive smartphone use. BMC Ophthalmol. 2016;16:37.
Yilmaz PT, Fatihoglu ÖU, Sener E. Acquired comitant esotropia in children and young adults: clinical characteristics, surgical outcomes, and association with presumed intensive near work with digital displays. J Pediatr Ophthalmol Strabismus. 2020;57:251–6.
Vagge A, Giannaccare G, Scarinci F, Cacciamani A, Pellegrini M, Bernabei F, et al. Acute acquired concomitant esotropia from excessive application of near vision during the COVID-19 lockdown. J Pediatr Ophthalmol Strabismus. 2020;57:e88–91.
Wu Y, Dai S, Liang F, Sun B. Excessive smartphone use may cause acute acquired comitant esotropia. J Ophthalmol Vis Res. 2020;2:1–6.
Mohan A, Sen P, Shah C, Jain E, Jain S. Prevalence and risk factor assessment of digital eye strain among children using online e-learning during the COVID-19 pandemic: Digital Eye strain among kids (DESK study-1). Indian J Ophthalmol. 2021;69:140–4.
Mohan A, Sen P, Mujumdar D, Shah D, Jain E. Series of cases of acute acquired comitant esotropia in children associated with excessive online classes on smartphone during COVID-19 pandemic; digital eye strain among kids (DESK) study-3. Strabismus. 2021;29:163–7.
Yagasaki T, Yokoyama Y, Yagasaki A, Eboshita R, Tagami K, Haga Y, et al. Surgical outcomes with and with prism adaptation of cases with acute acquired comitant esotropia related to prolonged digital device use. Clin Ophthalmol. 2023;17:807–16.
Cai C, Dai H, Shen Y. Clinical characteristics and surgical outcomes of acute acquired comitant esotropia. BMC Ophthalmol. 2019;19:173.
Lekskul A, Chotkajornkiat N, Wuthisiri W, Tangtammaruk P. Acute acquired comitant esotropia: etiology, clinical course, and management. Clin Ophthalmol. 2021;15:1567–72.
Keech RV, Scott WE, Baker JD. The medial rectus muscle insertion site in infantile esotropia. Am J Ophthalmol. 1990;109:79–84.
Abdelhafez MS, Sabahi S, Abdelhafez MM, Elamrousy D. Medial rectus insertion site in surgical candidate children with esotropia. J AAPOS. 2022;26:E12.
Helveston EM, Elis FD, Patterson JH, Weber J. Augmented recession of the medial recti. Ophthalmology. 1978;85:507–11.
Yoshida T, Yagasaki T, Sato M, Awaya S. Effects of Medial Rectus muscle insertion on Grading recession in Esotropia surgery. J Eye. 1995;12:1332–4. (in Japanese).
Iimori H, Suzuki H, Komori M, Hikoya A, Hotta Y, Sato M. Clinical findings of acute acquired comitant esotropia in young patients. Jpn J Ophthalmol. 2022;66:87–93.
Fialkowski A, Beasley TM, Tiwari HK. Multifactorial inheritance and complex diseases. In: Rimoin DL, Pyeritz RE, Korf B, editors. Emery and Rimoin’s principles and practice of medical genetics. 6th ed. Philadelphia: Elsevier Science; 2013. pp. 323–58.
Apt L. An anatomical reevaluation of rectus muscle insertion. Trans Am Ophthalmol Soc. 1980;78:365–75.
von Noorden GK, Campos EC. Rectal muscles, summary of the gross anatomy of the extraocular muscles. Binocular vision and ocular motility: theory and management of strabismus. 6th ed. St Louis: CV Mosby; 2002. pp. 39–41.
Bron AJ, Tripathi RC, Tripathi BJ. The anatomy of the eye and orbit: the extraocular muscles and ocular movements. Wolff EB ed. Wolff’s anatomy of the Eye and Orbit. 8th ed. Boca Raton: CRC; 1997. pp. 107–76.
Howe L. On the primary insertions of the ocular muscles. Trans Am Ophthalmol Soc. 1902;9:668–78.
Helveston EM. Surgical anatomy of the rectus muscles. Surgical management of strabismus. Oostende, Wayenborgh Publishing;; 2005. pp. 28–31.
Campos EC. Why do the eyes cross? A review and discussion of the nature and origin of essential infantile esotropia, microstrabismus, accommodative esotropia, and acute comitant esotropia. J AAPOS. 2008;12:326–31.
Hussaindeen JR, Mani R, Agarkar S, Ramani KK, Surendran TS. Acute adult onset comitant esotropia associated with accommodative spasm. Optom Vis Sci. 2014;91:46–51.
Kaur S, Sukhija J, Khanna R, Takkar A, Singh M. Diplopia after excessive smart phone usage. Neuroophthalmology. 2018;43:323–26.
Hayashi R, Hayashi S, Machida S. The effects of topical cycloplegics in acute acquired comitant esotropia induced by excessive digital device usage. BMC Ophthalmol. 2022;22:366.
Ali MH, Berry S, Qureshi A, Rattanalert N, Demer JL. Decompensated esophoria as a benign cause of acquired esotropia. Am J Ophthalmol. 2018;194:95–100.
Van Buskirk EM. The anatomy of the Limbus. Eye (Lond). 1989;3:101–8.
Jaggi GP, Laeng HR, Müntener M, Killer HE. The anatomy of the muscle insertion (scleromuscular junction) of the lateral and medial rectus muscle in humans. Invest Ophthalmol Vis Sci. 2005;46:2258–63.
Inagaki R, Suzuki H, Haseoka T, Arai S, Takagi Y, Hikoya A, et al. Effects of the gaze fixation position on AS-OCT measurements of the limbus and extraocular muscle insertion site distance. J Pediatr Ophthalmol Strabismus. 2021;58:28–33.
Kim EJ, Ganga A, Rana VK, Tanzer JR, Ronquillo YC, Moshirfar M. Reliability of time domain AS-OCT in measuring the extraocular rectus muscle insertion-limbus distances: a systematic review and meta-analysis. Clin Ophthalmol. 2022;16:2823–3.
Acknowledgements
We would like to thank all the orthopedists at Yagasaki Eye Clinic and Japan Community Healthcare Organization Chukyo Hospital. We would like to thank Editage (www.editage.com) for English language editing.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Yagasaki, None; T. Yagasaki, None; Y. Yokoyama, None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Yagasaki, A., Yagasaki, T. & Yokoyama, Y. Medial rectus insertion site in cases of acute acquired comitant esotropia associated with excessive digital device usage. Jpn J Ophthalmol (2024). https://doi.org/10.1007/s10384-024-01113-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10384-024-01113-y