
Abstract
Purpose
To report 4 cases undergoing 25-gauge endoscopic vitrectomy for the treatment of proliferative vitreoretinopathy with severe corneal opacity in which a transpupillary view of the fundus was not possible.
Study Design
A retrospective interventional case series.
Methods
The main outcomes measured were postoperative anatomic status of the retina and subjective improvement of vision. Results: Postoperative reattachment of the retina and subjective improvement of vision were achieved in all 4 eyes.
Conclusion
Twenty five-gauge endoscopic vitrectomy provides a clear view making it possible conduct pars plana vitrectomy in order to reattach the retina in cases of proliferative vitreoretinopathy with severe corneal opacity.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Recent technological advances in vitreous surgery systems including the use of a wide-angle viewing system have helped enlarge the indication of microincision vitrectomy surgery not only for uncomplicated retinal detachment but also for proliferative vitreoretinopathy. However, cases of severe corneal opacity make it impossible to perform vitrectomy with a transpupillary view when using a wide-angle viewing system.
We report 4 cases undergoing 25-gauge endoscopic vitrectomy for the treatment of proliferative vitreoretinopathy with severe corneal opacity in which a transpupillary view of the fundus was not possible.
Materials and methods
This retrospective, interventional case series examined 4 eyes of 4 patients who underwent 25-gauge endoscopic pars plana vitrectomy for proliferative vitreoretinopathy with severe corneal opacity at the National Hospital Organization Kyoto Medical Center, Kyoto, Japan between July 2014 and June 2016. This study was approved by the Institutional Review Board of the National Hospital Organization Kyoto Medical Center, and followed the tenets of the Declaration of Helsinki. Informed consent was obtained from each patient for all of the treatments.
All 4 patients were referred to our hospital due to suspected proliferative vitreoretinopathy after undergoing B-scan ultrasonography (Fig. 1). All 4 eyes had severe corneal opacity that prevented direct visualization of the fundus.

Anterior segment view of patient #2 showing severe corneal opacity (Left). B-scan ultrasound revealed a closed funnel proliferative vitreoretinopathy in the same case (Right)
Table 1 presents the demographic data of the patients. Three eyes had microcornea and horizontal nystagmus, and were diagnosed as developmental/congenital glaucoma. In each of these three cases, B-scan ultrasonography OU indicated a long axial length in the affected eye. In case 4, the patient had undergone pars plana vitrectomy for rhegmatogenous retinal detachment with perfluorocarbon liquid (PFCL) and heavy/conventional silicone oil 4 times since 2013. Case 4 was pseudophakic, while all of the other eyes were aphakic.
Surgical procedures for reattachment of the retina
A single surgeon (MK) who has been performing endoscope-assisted vitrectomy for over 25 years conducted the 25-gauge three port pars plana vitrectomy with a 25-gauge ophthalmic endoscope with 6,000 pixels (Fiber Tech Co., Ltd) under sub-Tenon anesthesia or, in the case of nystagmus retrobulbar anesthesia.
During the first step, in order to observe the fundus in aphakic eyes, a small amount of viscoelastic material was injected into the anterior vitreous cavity through a limbal wound made with a 20-gauge microvitreoretinal blade to create an opaque-free space for the endoscopy. In the pseudophakic eye case, instead of a limbal wound, one 25-gauge transconjunctival sclerotomy port was created 3.5 mm posterior to the limbus.
The other 25-gauge transconjunctival scleral ports were all created under endoscopic observation. Subsequently, 27-gauge twin light fibers (DORC) were placed 3.5 mm posterior to the limbus at the 4:30 and 7:30 position.
After the core vitrectomy, membranotomy and/or membranectomy was performed with microforceps and a vitreous cutter, with the reattachment of the retina achieved by using PFCL. Endolaser and cryoretinopexy were conducted under PFCL (Fig. 2; cf. supplemental Video). The PFCL was removed prior to the fluid/air exchange. After performing the peripheral iridectomy at the 6:00 position, silicone oil was injected.

Intraoperative view of patient #2 when using a 25-gauge endoscope. All photos are taken in surgeon’s view, where 12:00 of the photo indicates inferior fundus of the patient. Endoscopy revealed proliferative vitreoretinopathy with a closed funnel (arrow head) without a view of the optic disc (a), which is consistent with the B-scan ultrasound preoperative findings. Microforceps (arrow) were used to grasp the proliferative membrane over the funnel (a, b, e) and then pull by substituting the optic disc (c), ora serrata (d), and PFCL (f) with the 2nd forceps in order to stabilize the detached retina. Proliferative membrane (star) are gradually removed without making iatrogenic retinal breaks (a-f). Endolaser was applied under PFCL (g). After removing the PFCL, fluid/air exchange was subsequently performed (h)
Endoscopic examination of case 4 revealed several large retinal breaks at the equator area, subretinal emulsified silicone oil, a massive mixture complex of silicone oil and perfluorocarbon liquid, and anterior proliferative vitreoretinopathy. As a result, endoscopic manipulation, which included retinotomy, was performed under the silicone oil to flatten the retina.
A subsequent endoscopic fundus examination through limbus was performed a few months after the first endoscopic vitrectomy in order to confirm the retina attached prior to silicone oil removal in another few months.
Results
Endoscopy revealed proliferative vitreoretinopathy in all 4 eyes. Table 2 presents the clinical features of the cases. Retinal breaks were identified at the periphery of all cases under the endoscope. At the end of the first endoscopic vitrectomy in all 4 eyes, successful reattachment of the retina was achieved with the use of silicone oil tamponade.
There was no difficulty in terms of the illumination intensity, visual field, movability of the tool, and resolution of the image in performing a 25-gauge endoscope system compared to 20- or 23-gauge system.
A subsequent endoscopic fundus examination performed a few months after the first endoscopic vitrectomy confirmed the reattachment of retina under the silicone oil in 3 eyes. The silicone oil was then successfully removed in all 3 eyes under endoscopy. Keratoplasty is planned for these eyes. As endoscopic examination in case 3 revealed proliferative membrane and retinal detachment at the peripheral area of the inferior quadrant, membranotomy and membranectomy were added in order to flatten the retina. Silicone oil tamponade remained 8 months after the second vitrectomy in accordance with the patient’s wishes.
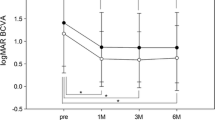
There was improvement in the postoperative visual acuity in one eye, with subjective improvement in the vision achieved in all eyes.
Discussion
We have previously reported a two-step procedure of 23-gauge endoscope-assisted vitrectomy followed by corneal transplantation used in a case of severe penetrating corneal injury [1]. In that case, we performed a vitrectomy in conjunction with an endoscope and a wide-angle viewing system; advantageous, because in addition to the endoscopic view, the wide-angle viewing system made it possible to observe the fundus through the localized, less-damaged corneal portion. Thus, the use of a hybrid operation consisting of an endoscope and a wide-angle viewing system appears to be less invasive, provides improved visualization, and minimizes the risk of early intervention in traumatic cases.
The use of temporary keratoprosthesis during pars plana vitrectomy followed by keratoplasty is reported to be beneficial in cases where a wide-angle viewing system cannot be used due to the opaque portions [2,3,4], similar to the 4 cases in our current study that had severe diffuse corneal opacity. However, the use of combined pars plana vitrectomy and simultaneous keratoplasty could lead to intraoperative complications such as suprachoroidal hemorrhage, especially in high myopic eyes, and corneal graft failure, especially in eyes with silicone oil tamponade [4, 5]. Furthermore, one problem that needs to be addressed in these cases is the urgency of the treatment for retinal detachment.
Endoscopy allowed us to observe the fundus directly and bypass the corneal opacity, thereby making it possible to identify the retinal breaks and perform intraocular manipulation to flatten the retina [6,7,8]. Recent studies demonstrate the efficacy of endoscopic vitrectomy in eyes with media opacities [1, 9,10,11,12].
The 3 cases in our current study had microcornea with a long ocular axial length, and these morphological features prevented the identification of the peripheral retinal lesion through the pupil despite there being a clear cornea in which endoscopy would normally be able to determine retinal breaks [12]. Here too, the use of high magnification with endoscopy is a useful tool for identifying tiny retinal breaks, especially in pseudophakic and aphakic eyes [6].
It should be noted, however, there are several disadvantages to endoscopic vitrectomy for retinal detachment or proliferative vitreoretinopathy. First, the use of a bimanual technique is not possible, as one hand is required for the surgeon to manipulate the endoscope. Thus, the procedure can be difficult in surgery for severe proliferative vitreoretinopathy. Several reports recommend that endoscopes only be used in uncomplicated cases [7, 11]. To overcome this problem, we used the optic disc, ora serrata, and PFCL substituting for forceps in the left hand to stabilize the detached retina. In addition, the direction in which the proliferative membrane or vitreous adhesion to the retina needs to be pulled has to be carefully considered in order to prevent making retinal breaks, and in order to effectively remove the membrane and adhesion.
The second disadvantage is that in endoscopy it is hard to deal with the border of the phases. For example, an endoscope cannot visualize the border of the silicone oil when the tip of the endoscope is located within the silicone oil. To avoid this, we did not perform manipulations using 4 phases such as PFCL, silicone oil, water and air, but rather conducted the procedure using only 2 phases such as water and air, water and PFCL, or air and silicone oil.
Another disadvantage is that an endoscope only provides a monocular view and thus, the shadowing is eliminated as the illumination and image fibers are located in the same axis. To overcome this, we placed twin chandelier light fibers in all our cases without using the transpupillary view to create shadows that made the endoscopic maneuver considerably easier.
The problem of this procedure is the difficulty in postoperative follow-up. In silicone oil-filled eyes, ultrasonographic evaluation is not accurate. Ophthalmoscopic fundus examination through the clearer parts of the cornea is limited. So the first endoscopic fundus examination was performed only a few months after endoscopic vitrectomy, prior to silicone oil removal in another few months.
Chun at al. report that endoscopic vitrectomy can be performed in ocular traumatic eyes with opaque cornea as safely as vitrectomy with a temporary keratoprosthesis, and thereby achieve a similar visual and anatomic outcomes [11]. Similarly, we used 25-gauge endoscopic vitrectomy and successfully achieved reattachment of the retina in 4 cases of proliferative vitreoretinopathy with non-traumatic opaque cornea.
In conclusion, 25-gauge endoscopic vitrectomy can be successfully used to provide a clear enough view in order to conduct pars plana vitrectomy and achieve reattachment of the retina in cases of proliferative vitreoretinopathy with severe corneal opacity. Endoscopic 25-gauge vitrectomy proved to be safe and effective in cases of proliferative vitreoretinopathy with corneal opacity in which a transpupillary view of the fundus is not possible.
References
Morishita S, Kita M, Yoshitake S, Hirose M, Oh H. 23-gauge vitrectomy assisted by combined endoscopy and a wide-angle viewing system for retinal detachment with severe penetrating corneal injury: a case report. Clin Ophthalmol. 2011;5:1767–70.
Eckardt C. A new temporary keratoprosthesis for pars plan vitrectomy. Retina. 1987;7:34–7.
Koenig SB, McDonald HR, Williams GA, Abrams GW. Penetrating keratoplasty after placement of a temporary ketatoprosthesis during pars plana vitrectomy. Am J Ophthalmol. 1986;102:45–9.
Garcia-Valenzuela E, Blair NP, Shapiro MJ, Gieser JP, Resnick KI, Solomon MJ, et al. Outcome of vitreoretinal surgery and penetrating keratoplasty using temporary keratoprosthesis. Retina. 1999;19:424–9.
Roters S, Szuman P, Hermes S, Thumann G, Bartz-Schmidt KU, Kirchhof B. Outcome of combined penetrating keratoplasty with vitreoretinal surgery for management of severe ocular injuries. Retina. 2003;23:48–56.
Kita M, Yoshimura N. Endoscope-assisted vitrectomy in the management of pseudophakic and aphakic retinal detachments with undetected retinal breaks. Retina. 2011;31:1347–51.
Marra KV, Yonekawa Y, Papakostas TD, Arroyo JG. Indications and techniques of endoscope assisted vitrectomy. J Ophthalmic Vis Res. 2013;8:282–90.
Pappuru RRR, Tyagi M, Paulose RM, Paulose RM, Dave VP, Das T, et al. Role of diagnostic endoscopy in posterior segment evaluation for definitive prognostication in eyes with corneal opacification. Am J Ophthalmol. 2017;176:9–14.
de Smet MD, Mura M. Minimally invasive surgery-endoscopic retinal detachment repair in patients with media opacities. Eye. 2008;22:662.
Sabiti KA, Raizada S. Endoscope-assisted pars plana vitrectomy in severe ocular trauma. Br J Ophthalmol. 2012;96:1399–403.
Chun DW, Colyer MH, Wroblewski KJ. Visual and anatomic outcomes of vitectomy with temporary keratoprosthesis or endoscopy in ocular trauma with opaque cornea. Ophthalmic Surg Lasers Imaging. 2012;43:302–10.
Yoshitake S, Oh H, Kita M. Endoscope-assisted vitrectomy for retinal detachment in an eye with microcornea. Jpn J Ophthalmol. 2012;56:613–6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
M. Kita, Grant (Alcon Novartis, HOYA, Kowa, Santen, Wakamoto); Y. Fujii, None; S. Hama, None.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplemental video Intraoperative view of patient #2 with a 25-gauge endoscope. Endoscopy revealed proliferative vitreoretinopathy with closed funnel without view of the optic disc, which is consistent with preoperative findings of B-scan ultrasound. Microforceps were used to grasp the proliferative membrane over the funnel and then pull by substituting the optic disc, ora serrata, and PFCL with the 2nd forceps in order to stabilize the detached retina. Endolaser was applied under PFCL. The original tiny retinal break at 6:00 portion of periphery was identified. After removing PFCL, fluid/air exchange and internal drainage of residual subretinal fluid through the intentional retinotomy site was subsequently performed. Then silicone oil was injected, followed by confirming the reattachment of the retina with an endoscope. (WMV 34585 kb)
About this article

Cite this article
Kita, M., Fujii, Y. & Hama, S. Twenty five-gauge endoscopic vitrectomy for proliferative vitreoretinopathy with severe corneal opacity. Jpn J Ophthalmol 62, 302–306 (2018). https://doi.org/10.1007/s10384-018-0578-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10384-018-0578-5