
Abstract
Purpose
Few studies report the prevalence and types of strabismus, or average of stereopsis in Japanese adults. We performed ophthalmological evaluation including motility and stereopsis during medical examinations at cooperative companies.
Methods
We studies 1214 volunteers. The average age was 41.2 ± 12.6 (range 20–86) years. Examinations were carried out using their customary eyewear, evaluating alternate prism cover test (APCT), and Titmus stereo test (TST).
Results
The mean horizontal angle at near distance (1/3 m) was 8.1 ± 6.0 Prism Diopter (PD), and vertical angle was 0.09 ± 1.0 PD. The total number of cases who had intermittent or constant tropia was 44 (3.6%), and the ratio of exotopia to esotropia (XT:ET ratio) was 18.5:1. The mean horizontal angle at far distance (5 m) was 3.9 ± 3.7 PD, and vertical angle was 0.09 ± 1.7 PD. The total number of cases who had intermittent or constant tropia was 21 (1.7%), and the XT:ET ratio was 7:1. The average TST was 50.1 ± 1.6 arcsec. 7.3% (n = 89) of the cases did not reach 100 arcsec.
Conclusions
We report detailed strabismus and stereopsis in Japanese adults. The XT:ET ratio was 18.5:1 in near distance, 7:1 in far distance. In our study, more than 60% of the cases of exotropia were convergence insufficiency type, and this may be a characteristic in Japanese adults.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Various studies report the prevalence of strabismus [1–10], and there are many reports on the different types of strabismus and ratio of exotropia and esotropia [1–11]. However, most of these studies examined infants and children, with very few studies on adults. The statistics on adults are usually of adult-onset strabismus [12] in patients presenting for hospital screening [10, 11]. The data on adults were not taken from medical examinations and there are no reports targeting normal examinees. Data from Japanese population is important as the prevalence of strabismus is affected by ethnicity [1–3]. Moreover, no detailed studies on stereopsis in Japanese adults are available, an unfortunate omission in our increasingly three-dimensional (3D) technological environment. Therefore, we performed an ophthalmological medical evaluation including ocular motility and stereopsis during medical examinations at cooperative companies, and report the results of strabismus prevalence, strabismus types, and stereopsis.
Subject and methods
Participants were 1214 volunteers who were examined at medical checkups during company medical examinations after giving informed consent. This study has obtained the approval of the Kitasato University B Ethics Committee (11-82) and the Kitasato University Medical Center Ethics Committee (25-10). There were 672 participants from Kitasato University Hospital in 2012, 400 from Kitasato University Medical Center in 2013, and 142 from Kitasato Medical Service in 2013. All subjects were Japanese. There were 402 men (33.1%), 809 women (66.6%), and 3 of indeterminate gender (0.2%). 280 participants were aged 20–29 years old (23.1%), 293 were 30–39 years old (24.1%), 316 were 40–49 years old (26.0%), 220 were 50–59 years old (18.1%), and 105 were 60 years old and over (8.6%). The average age was 41.2 ± 12.6 years (20–86 years old, Fig. 1).

Age frequency distributions
Volunteers were examined using their regular eyewear. The examinations included 5 m far vision (OS, OD), alternate prism cover test (APCT) at 1/3 and 5 m, and Titmus stereo test (TST: circle). Landolt C was used to measure visual acuity (VA) from 0.1 to 1.5 at 5 m (CA-100, Tomey). Those who were unable to see at 0.1 were excluded. The average VA was changed from decimal into Log MAR and calculated. The statistics of the results of APCT were collected at absolute values. Cases of poor VA in one eye and participants unable to alternate their fixation were excluded from the data of APCT. TST requires cross-polarized filters (worn over prescription glasses). The averages of TST were derived by converting into logarithm and averaging. Cases of no stereopsis were excluded when calculating the average. All examinations were carried out by three orthoptists having experience of five years or more. Data were processed using the IBM SPSS Statistics, Version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
-
1.
Correction condition in examination
Five hundred and forty-six participants did not wear glasses (45.0%) (8 of them having had refractive surgery), 396 wore glasses (32.6%), 270 wore contact lenses (22.2%), with 2 omissions in entry (0.2%).
-
2.
Visual acuity
The average decimal VA (mean) was 1.09 (n = 1212) OD and 1.04 (n = 1208) OS.
A VA of 1.0 or above was established in 53.6% OD (n = 651) and in 61.1% OS (n = 742); 82.3% had a VA of 0.7 OD (n = 999) and 84.8% OS (n = 1030). A VA of 0.1 or below OD was established in 0.9% (n = 11) and in 1.6% OS (n = 19) (Fig. 2); 0.24% (n = 3) eyes had a VA of 0.1 or below OU.

Decimal visual acuity frequency distributions
-
3.
APCT (near distance at 1/3 m)
Horizontal angles were between −85 and +20 PD, and the average was 8.1 ± 6.0 PD (mean ± standard deviation) (Fig. 3). Figure 4 shows details of strabismus types. The vast majority of eyes 93.3% (n = 1133) had exophoria. In 4.5% (n = 55) of participants the horizontal angle was 20 PD or more: 1 with constant exotropia (45 PD), 19 with intermittent exotropia (20–40 PD), and 35 with exophoria (20–85 PD).

Strabismus magnitude in horizontal angles

Strabismus subtypes in horizontal angles. ET constant esotropia, E(T) intermittent esotropia, E esophoria, ortho orthophoria. X exophoria, X(T) intermittent exotropia, XT constant exotropia
The maximum vertical angle was 20 PD, and the average was 0.09 ± 1.0 PD (mean ± standard deviation). Vertical deviation was not observed in 98.4% (n = 1195), vertical heterophoria in 0.7% (n = 8) and vertical intermittent tropia in 0.4% (n = 5). In 0.3% (n = 4) participants the vertical deviation was more than 10 PD: 1 with vertical constant tropia (14 PD), 2 with vertical intermittent tropia (10, 20 PD) and 1 with vertical heterophoria (20 PD).
There was intermittent or constant tropia in 3.6% (n = 44) of subjects: horizontal tropia (both esoshift and exoshift) in 3.2% (n = 39), vertical tropia in 0.6% (n = 7) and comorbid horizontal and vertical tropia in 0.2% (n = 2). The exotopia: esotropia (XT:ET) ratio was 18.5:1. Figure 5 displays the ratio by age for strabismus prevalence. There were no significant difference in strabismus prevalence rate as a function of age by Chi square tests (p = 0.51: horizontal, p = 0.49: vertical).

Strabismus prevalence rate by age. Top prevalence of strabismus at near distance (1/3 m), Left horizontal angle, Right vertical angle. Bottom prevalence of strabismus at far distance (5 m), Left horizontal angle, Right vertical angle
-
4.
APCT (far distance at 5 m)
Horizontal angles were between −68 and +14 PD, with an average of 3.9 ± 3.7 PD (mean ± standard deviation) (Fig. 3). Figure 4 shows details of strabismus types. The vast majority of subjects’ eyes had exophoria 96.3% (n = 1169). In 1.1% (n = 13) of participants the horizontal angles were 20 PD or more: 2 with constant exotropia (25 PD), 5 with intermittent exotropia (20–35 PD), and 6 with exophoria (20–68 PD).
The maximum vertical angle was 25 PD, with an average of 0.09 ± 1.7 PD (mean ± standard deviation). The vertical ocular positions showed orthophoria in 98.6% (n = 1197), hyperphoria in 0.4% (n = 5), intermittent hypertropia in 0.4% (n = 5) and hypertropia in 0.2% (n = 2). In 0.4% (n = 5) participants vertical angles of 10 PD or above were established: 2 with vertical constant tropia (10 PD, 12 PD), 2 with vertical intermittent tropia (16 PD, 20 PD) and 1 with vertical heterophoria (25 PD).
There was intermittent or constant tropia in 1.7% (n = 21) of subjects: 1.3% (n = 16) with horizontal tropia (both esoshift and exoshift), 0.6% (n = 7) with vertical tropia was and 0.2% (n = 2) with comorbid horizontal and vertical tropia. The XT:ET ratio was 7:1. The ratio by age for strabismus prevalence is shown in Fig. 5. There were no significant difference of strabismus prevalence rate per age in Chi square tests (p = 0.62: horizontal, p = 0.59: vertical).
-
5.
APCT (comparing the distances 1/3 and 5 m)
At 5 m 14 subjects (37.8%) presented exotropia as well as exotropia at 1/3 m. However, 23 subjects (62.1%) presented exotropia at 1/3 m but not at 5 m. We did not observe any cases were a subject presented exotropia at 5 m but not at 1/3 m, which means that more than half of the cases of exotropia displayed convergence insufficiency.
-
6.
TST (circle)
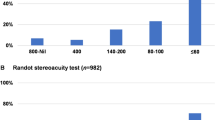
The average of stereopsis was 50.1 ± 1.6 arcsec (Fig. 6). In 92.6% (n = 1124) of the cases stereopsis was 100 arcsec or better, and 7.3% (n = 89) of the cases did not reach 100 arcsec. Of 89 cases that did not reach 100 arcsec, 9 cases recognized strabismus with APCT at 1/3 m (3 intermittent exotropia, 4 constant exotropia, and 2 constant esotropia), and 14 cases recognized poor VA (VA of 0.3 or below in one or both eyes).

TST frequency distributions
Discussion
There are three previous reports that compare strabismus prevalence and the ratio of exotropia and esotropia (EX:ET ratio), targeting infants ages 6–72 months old of different ethnicities in the United States [1–3] (Table 1). Within these reports, significant difference was observed in the XT:ET ratio and there were many cases of exotropia and fewer cases of esotropia in Asians compared to non-Hispanic whites. From these findings, it is evident that the prevalence in strabismus type is ethnically dependent.
In Japan, there are some reports of children in elementary and junior schools from about 50 years ago [4–6]. In these studies, the strabismus prevalence was 0.058–2.3% and the XT:ET ratio was 1.2–2.3:1. In recent years, Matsuo et al. published a number of reports. In the report on 1.5-year-olds [7], the strabismus prevalence was 0.01–0.12% and the XT:ET ratio was 2.4:1. In the report on 3-year-olds [7], strabismus prevalence was 0.20–0.34% and the XT:ET ratio was 4.4:1. In the reports on 6–12 years old [8, 9], the prevalence was 0.99–1.28% and the XT:ET ratio was 2.5–2.8:1. From the above, we can say that in Japanese children the average strabismus prevalence is 0.058–2.3%, the XT:ET ratio is 1.2–4.4:1, and the ratio of exotropia tends to be higher in Japanese compared to other ethnic groups. According to our study, the strabismus prevalence is 3.6% and the XT:ET ratio is 18.5:1 at near distance, and at far distance the prevalence is 1.7% and the XT:ET ratio is 7:1. This indicates that in adults both the prevalence and exotropia tend to increase compared to esotropia when compared to cases that targeted children.
Exotropia increases significantly especially at near distance vision, and in our study more than 60% of the cases with exotropia were convergence insufficiency. Tompson et al. [12] report that convergence insufficiency, 15.7% of total cases, is the secondary cause of strabismus development in adults (the first is paralytic). From the above, we can assume that exotropia of near distance vision tends to increase with aging.
There are few reports that focus on strabismus prevalence in adults. Stidwill [11] in the United Kingdom selected 3075 subjects with strabismus, decompensated heterophoria, nystagmus, accommodative or vergence anomalies. That study included adults although the target age is not indicated. About half of them, 1562 subjects (50.8%) had esotropia and 464 subjects (29.7%) had exotropia; the XT:ET ratio was 1:3.7. Matsumura et al. [10] in Japan performed cover-uncover tests on 685 subjects, who visited an ophthalmology clinic and had only mild refractive errors, cataracts, or allergic conjunctivitis and no eye diseases. In that group, the strabismus prevalence was 3.0% and the XT:ET ratio was 6:1. There is some bias in the two studies above as the subjects selected were from patients who had visited hospitals. Based on these studies, we can say that esotropia is more prevalent in Caucasians while exotropia is more prevalent in Asians, this prevalence is the same in children and adults. Exotropia was also significant in Japanese in our study of adults.
Sagging eye syndrome [13] is known to be caused by fragile orbital pulley [14] and develops with aging. However, in our study there was no tendency of strabismus increasing with aging at any age over 20 years old. It is not clear whether this is due to insufficient sampling or other factors affecting middle age, or whether it is due to characteristics of Japanese. This issue needs to be evaluated more carefully with more samples.
Stereopsis was poorer than 100 arcsec 7.3% (n = 89) of cases by circle testing. The causes of 74.2% (n = 66/89) cases were not explainable by VA or strabismus, so we would like to elucidate the causes. Of 89 cases that did not reach 100 arcsecs, the causes for 9 cases were identified as strabismus and 14 cases were identified as poor VA. There are other two possible causes. The first is TST sensitivity: the sensitivity of TST is reported to be about 75% [15], so false-negative cases may have been included. As for the second possible cause, as, depending on the correction method, TST tested at near distance may sometimes generate false results in those accompanied by presbyopia.
In conclusion, as this test is limited to adults examined during medical checkups at companies in the areas around Tokyo the results may slightly differ from the statistics of the entire Japanese population, however, this is the first strabismus and stereopsis study report targeting Japanese adults. Moreover, over 60% of the cases of exotropia were convergence insufficiency as a characteristic in Japanese adults. In the future, we believe such findings will be valuable basic data for studies on strabismus.
References
Multi-ethnic Pediatric Eye Disease Study Group. Prevalence of amblyopia and strabismus in African American and Hispanic children ages 6 to 72 months the multi-ethnic pediatric eye disease study. Ophthalmology. 2008;115:1229–36.
Friedman DS, Repka MX, Katz J, Giordano L, Ibironke J, Hawse P, et al. Prevalence of amblyopia and strabismus in white and African-American children aged 6 through 71 months: the Baltimore Pediatric Eye Disease Study. Ophthalmology. 2009;116:2128–34.
McKean-Cowdin R, Cotter SA, Tarczy-Hornoch K, Wen G, Kim J, Borchert M, Multi-Ethnic Pediatric Eye Disease Study Group, et al. Prevalence of amblyopia or strabismus in asian and non-Hispanic white preschool children: multi-ethnic pediatric eye disease study. Ophthalmology. 2013;120:2117–24.
Makiuchi S, Yamaji R, Kozaki M. On the investigations of amblyopic children and students in compulsory course in Osaka-fu. Rinsho Ganka (Jpn J Clin Ophthalmol). 1962;16:151–65 (in Japanese).
Yazawa K. Ocular examination on 10,000 school children. Rinsho Ganka (Jpn J Clin Ophthalmol). 1973;27:557–69 (in Japanese).
Maruo T, Kubota N, Arimoto H. The results of examinations for strabismus and amblyopia in elementary and secondary school pupils. Ganka Rinsho Iho (Jpn Rev Clin Ophthalmol). 1977;71:712–4 (in Japanese).
Matsuo T, Matsuo C, Matsuoka H, Kio K. Detection of strabismus and amblyopia at 1.5- and 3-year-old children by preschool vision-screening program in Japan. Acta Med Okayama. 2007;61:9–16.
Matsuo T, Matsuo C. The prevalence of strabismus and amblyopia in Japanese elementary school children. Ophthalmic Epidemiol. 2005;12:31–6.
Matsuo T, Matsuo C. Comparison of prevalence rates of strabismus and amblyopia in Japanese elementary school children between the years 2003 and 2005. Acta Med Okayama. 2007;61:329–34.
Matsumura M, Arimatsu J, Utsumi R, Utumi T, Nakamura K. Physiological exophoria at near distance 1. Frequency and distribution of exophoria. Jpn Orthopt J. 1991;19:111–5 (in Japanese).
Stidwill D. Epidemiology of strabismus. Ophthal Physiol Opt. 1997;17:536–9.
Martinez-Thompson JM, Diehl NN, Holmes JM, Mohney BG. Incidence, types, and lifetime risk of adult-onset strabismus. Ophthalmology. 2014;121:877–82.
Chaudhuri Z, Demer JL. Sagging eye syndrome. JAMA Ophthalmol. 2013;131:619–25.
Kono R, Okanobu H, Ohtsuki H, Demer JL. Displacement of the rectus muscle pulleys simulating superior oblique palsy. Jpn J Ophthalmol. 2008;52:36–43.
Moganeswari D, Thomas J, Srinivasan K, Jacob GP. Test re-test reliability and validity of different visual acuity and stereoacuity charts used in preschool children. J Clin Diagn Res. 2015;9:NC01-5.
Acknowledgements
We would like to thank Prof. Dr. Joseph L.Demer of the Jules Stein Eye Institute for comments that greatly improved the manuscript. We are also grateful to Ms. Etuko Ohta for assistance with analyze data, and Mr. Benjamin Abbott for checking the English. This research was partially supported by the Ministry of Education, Science, Sports and Culture, Grant-in-Aid for Young Scientists (B), 2011–2012(23792001, Toshiaki Goseki) and 2013–2014 (25861648, Toshiaki Goseki). This study was presented at 12th Meeting of the International Strabismological Association (ISA) in Kyoto, Japan on Dec. 1-4, 2014.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
T. Goseki, None; H. Ishikawa, None.
About this article

Cite this article
Goseki, T., Ishikawa, H. The prevalence and types of strabismus, and average of stereopsis in Japanese adults. Jpn J Ophthalmol 61, 280–285 (2017). https://doi.org/10.1007/s10384-017-0505-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10384-017-0505-1