
Abstract
Malnutrition among under five children in Nigeria remains a major public health burden. It has been shown to be one of the leading causes of childhood death and has permanent consequences for cognitive development, school attendance, economic productivity in adulthood and maternal reproductive outcome. Understanding the associated risk factors of malnutrition is critical for developing appropriate interventions because its determinants interact at different degrees to affect these children. Thus, it is important, for programmatic purposes, to continue to identify the important risk factors and geographical variations especially in a country with massive variations in cultural belief and socioeconomic status of its populace. A multilevel structured additive regression, based on cumulative probit link function was adopted to explore the spatio-temporal variations on severity of three anthropometric indices among children in Nigeria using the Nigeria Demographic and Health Survey data from 2003 to 2018. Within a Bayesian context, appropriate priors were assigned on all functions and parameters. Evidently, strong and significant spatial variations was found to exist on severity of malnutrition among under five children in Nigeria showing a north–south divide. We found young age at first marriage, episodes of child illnesses, child birth weight, religion, mother’s education and household wealth to be associated with undernutrition. Findings will guide in developing effective strategies to combat the devastating effect of child malnutrition in Nigeria. Consequently, there can be hope of attaining the relevant sustainable development goals.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
The nutritional status of a child is an integral part of his physical and mental well-being (Idris et al. 2013). The nutritional status of children is particularly important because it has both short and long-term effects on the well-being of the populations and the socio-economic development of the society. Severe malnutrition in early childhood often leads to deficient in cognitive development, school achievement, economic productivity in adulthood, maternal reproductive outcome and undue pressure on health care system (De Onis and Branca 2016; Dewey and Begum 2011; Black et al. 2013).
Malnutrition among children is one of the most important causes of morbidity and mortality in the world. Nearly half of all deaths in children under 5 are attributed to under nutrition (UNICEF 2018). Previous studies revealed that under nutrition in the aggregate including fetal growth restriction, stunting, wasting and deficiencies of vitamin and zinc along with suboptimum breastfeeding is a cause of 3.1 million child deaths annually or 45% of all child deaths in 2011 (Black et al. 2013). Report by World Health Organisation (WHO) revealed that 47 million children under 5 years of age are wasted, 14.3 million are severely wasted and 14.4 million are severely stunted, while 38.3 million are obese (WHO 2021). In Nigeria, an estimated 2 million children suffer from severe acute malnutrition (SAM) in 2018 (UNICEF 2018). Moreover, Nigerian has the second highest burden of stunted children in the world, with a national prevalence rate of 32% of children under five (UNICEF 2018).
Understanding the severity of child nutritional status permits appropriate and adequate interventions in management of and addressing the issue of child malnutrition. According to WHO (WHO, 2020), malnutrition is a group of conditions in children and adults generally related to poor quality or insufficient quantity of nutrient intake, absorption or utilization. Generally, malnutrition is classified into protein-energy malnutrition resulting from deficiencies in any or all nutrients; and micronutrient deficiency resulting from a deficiency of specific micronutrients. Protein-energy malnutrition in children comes in three forms: (i) Chronic malnutrition which is a measure of height-for-age otherwise known as stunting (too short for height), (ii) Acute malnutrition which is a measure of weight-for-height known as wasting (too thing for height), and (iii) Chronic and/or acute malnutrition referred to as underweight (too thing for age) which is a measure of weight-for-age. Stunting has been found to be as a result of inadequate nutrition over a long period of time leading to retardation in linear growth. On the other hand, acute malnutrition was found to be associated with inadequate nutrition leading to rapid weight loss or failure to gain weight proportionately to height (LSHTM 2009). This has also been linked to recent episodes of some common diseases such as diarrhoea, cough, fever and acute respiratory infection among children under five especially in developing countries and in sub-Saharan Africa in particular. On the other hand, underweight is believed to result from either stunting or wasting or even both.
A number of risk factors including infection, poor environmental condition, food insecurity, recurrent acute illness, birth order, family size, demography and socio-economic factors have been previously shown to be associated with malnutrition (Ansuya et al. 2018; Ajao et al. 2010; Balogun and Yakubu 2014; Abidoye and Ihebuzor 2001; Akombi et al. 2017b). Malnutrition was found to be higher among children living in households with more sibling and inappropriate feeding practices (Abidoye and Ihebuzor 2001; Ajao et al. 2010; Balogun and Yakubu 2014). Low birth weight (LWB) is another predictive factor that is found to be associated with malnutrition (Ansuya et al. 2018). In their study, Fagbamigbe et al. (2020) showed that children with LBW and male infants are more likely to have severe acute malnutrition. A LBW baby is prone to growth failure during infancy and early childhood. Linear growth retardation in young children, on the other hand, is an indicator of chronic under nutrition and it provides an accurate marker of inequality in human development (De Onis and Branca 2016).
Although the prevalence of child malnutrition is relatively well documented, evidence on the geographical variation, bio-demographic factors affecting children malnutrition in Nigeria is limited especially considering the severity of the three anthropometric indices. Moreover, estimates derived from survey data can be affected by sample sizes taken from the different locations, and the effects of explanatory variables have not been taken into account. Model-based estimation however has a mechanism of borrowing strength from neigbouring locations to improve local estimates especially in places with relatively few observations. Previous efforts in predicting malnutrition in Nigeria have focused on ecological and areal data analysis (Balogun and Yakubu 2014; Abidoye and Ihebuzor 2001; Ajao et al. 2010). These methods give mean estimates at district level but do not capture the variability of prevalence that occurs within regions. For few that have used the Nigeria Demography Health Survey (NDHS) data, spatial effects among regions were not considered (Adekanmbi et al. 2013; Akombi et al. 2017a, b). In this study, we used Bayesian multilevel structured geo-additive models to determine how well background characteristics, socio demographic and bio-demographic covariates, as well as, trend in years determine the nutritional status of children in Nigerian. The multilevel modelling technique accounts for the hierarchical structure of the data and correct the estimated standard errors to allow for clustering of individuals within areas (Goldstein 2003).
Data and methods are presented in Sect. 2 while Sect. 3 presents the Statistical analysis with Data Analysis presented in Sect. 4. Results and discussions are presented in Sect. 5 with some concluding remarks.
2 Data and methods
Variables of interest were extracted from the Child Recode data of the 2003, 2008, 2013 and 2018 Nigeria Demographic and Health Survey (NDHS). Demographic and Health Survey (DHS) is conducted in many developing countries by The DHS Program (www.dhsprogram.com) to provide cross-sectional information on demographic and health indicators including information about maternal and child health (including their nutritional status), fertility and family planning; knowledge and current use of contraceptive methods as well as sexually transmitted diseases. The survey is designed to provide this information at national and regional level; urban and rural areas and also at state (district) level. The standard methodology with which the surveys are being carried out permits comparisons of indicators across years and the countries where it is conducted. The datasets used in this study allow us to examine trend in child nutrition in Nigeria between 2003 and 2018. (NPC [Nigeria] and ORC Macro 2004; NPC [Nigeria] and ICF Macro 2009, 2014; NPC [Nigeria] and ICF 2019). Understanding trend on child nutritional status has become an important tool that can aid the achievement of the relevant Sustainable Development Goal indicators.
The sampling frame used for the surveys were based on the Population and Housing Census of the Federal Republic of Nigeria conducted in 1991 and 2006. The primary sampling unit (PSU) referred to as cluster for the survey was defined on the basis of enumeration areas (EAs) from the census frames. The NDHS samples were based on a two-stage stratified design. At the first stage, a number of clusters were selected from the list of enumeration areas while households to participate in the survey were selected at the second stage. One of the eligibility criteria for women component of the survey is that female respondents must be in the age range 15–49 years. The response rates from the eligible women were 95.4, 96.5, 97.7 and 99.3% in 2003, 2008, 2013 and 2018 respectively. Of these women, questions on child health, morbidity and mortality were asked from those who have given birth in the five years preceding each survey years. In 2003, data were obtained on 6029 children, 2008 on 28,647 children, 2013 on 31,482 children and 2018 on 33,924 children from their mothers.
Three anthropometric indicators: height-for-age, weight-for-height and weight-for-age are commonly used in measuring child nutritional status. These can be expressed in standard deviation units (Z-scores) from the median of the reference population in accordance with the WHO Child Growth Standards (WHO Multicentre Growth Reference Study Group 2006). A child with a Z-score (from any of these three anthropometric indices) lower than \(-\)2.0 is considered to be malnourished.
2.1 Dependent variables
Stunting or short height-for-age is a sign of chronic undernutrition that reflects failure to receive adequate nutrition over a long period of time. The underlying causes of stunting are inadequate nutrition from food with nutrients that can promote growth. It could also be a possibility of recurrent infections or chronic diseases that can cause poor nutrient intake and absorption. Wasting on the other hand is referred to as low weight-for-height, a measure of acute undernutrition and represents the failure to receive adequate nutrition in the period immediately before the survey. Wasting may result from inadequate intake of food or from a recent episode of illness or infection causing weight loss. Severity of malnourishment goes a long way to depict the health outcome among under five children and their mothers.
Analysing data on nutritional status of children under five can indeed be motivated by taking cognizance of the fact that such outcomes can be classified based on the level of severity in accordance with the WHO standard definition. In this paper, the analyses considered ordinal categorical outcomes for stunting, wasting and underweight based on severity of the nutritional status in accordance with WHO definition of anthropometric indices (AI) of \(< -3.0\) (severe stunting/severe wasting/severe underweight), \(-3.0 \le\) Z-score \(< -2.0\) (as moderate stunting/wasting/underweight) and Z-score \(\ge 2.0\) (as normal). This can be represented through the variable \(Y_{ik}\) as follows:
The same holds for wasting and underweight. A model that takes cognizance of this ordering is desirable. Interestingly, modelling children nutritional status rarely consider severity of malnourishment using the ordinal level outcome variable at a complex level that accounts for trend, linear fixed effects, spatial variations, nonlinear effects of metrical covariates and incorporation of random effect model which accounts for any possible unobserved heterogeneity that may exist in the data. Our approach takes credence from the flexibility of the Markov chain Monte Carlo (MCMC) sampling techniques that are incorporated into BayesX – a software for structured additive regression models (Belitz et al. 2015).
2.2 Independent variables
The independent variables explored in this study are classified under three broad categories. These are background characteristics, socio-demographics and bio-demographics (which are health related). Also, dummy variables were created that indicate the year of the surveys in order to measure any possible trend between 2003 and 2018 during which the four waves of NDHS were conducted. Table 1 presents details of the covariates explored.
3 Statistical analysis
3.1 Modelling
Suppose \(Y_{ik}\) is a random variable that indicates the nutritional status of a child as described in Eq. 1. The subscripts i and k indicate the response from the ith child living in the kth state. Consider the regression problem with \(Y_{ik}\) as outcome variable on a set of covariates of different nature given as \((Y_{ik}, X_i, Z_i, S_i, V_i)\). The intention is to explore the dependence of \(Y_{ik}\) being an ordinal categorical variable on \(X_i\) as metrical covariates consisting of mother’s age at birth of child, age of mother at first marriage/cohabitation, body mass index (BMI) of mother, and the current age of child; \({Z_i}\) as a vector of all categorical covariates; \({S_i}\) as the spatial covariate \(S_i \in \{1,2, \cdots , 37 \}\) and a further component \(V_i\) as random effects for cluster and household number where the child lived. The random effects are to explore any unobservable covariate and incorporated to assess the hierarchical nature of the data. As described in Fahrmeir and Tutz (2001), such a multi-categorical regression model can be motivated through latent variables such that the response variable y (for simplicity) is observed as an ordered categories \(1, \cdots , k\). It is postulated that y is a categorized version of a latent variable
obtained through the threshold mechanism
with thresholds \(-\infty = \theta _0< \cdots < \theta _k =\infty\). The error term \(\varepsilon\) is assumed to have a distribution function F, and hence, it follows that y obeys a cumulative model
where \(\eta\) is the multilevel structured additive predictor which can be specified for a particular child i as
From Eq. 4, \(f(x_i)\), \(f_{spat}(S_i)\), \(\beta\) and \(v_i\) represent the unknown smooth nonlinear effects of vector of metrical covariates X, the spatial effect, vector of the linear parameters for the categorical covariates and \(v_i\) is the component for the random effects respectively. To enhance identifiability, functions are centred about zero, and by implication the linear parameters includes an intercept term \(\beta _0\).
In assessing the severity of the nutritional status of the children as in our case study, each of the three AIs indicators is considered to have a three-level ordered categorical version of the latent continuous variable U described in Eq. 2. Consequently, \(\varepsilon\) is assumed to have a standard normal distribution function, that is,
thus, yielding a cumulative probit model. Taking credence from Edwards and Thurstone (1952), cumulative models based on category boundaries or threshold techniques are well used in ordinal regression. The use of this approach for ordered outcome was documented in Adebayo (2004) in exploring geographical variations in childhood breastfeeding initiation in Nigeria.
3.2 Bayesian inference
Parameter estimation was based on Bayesian techniques that rely on MCMC samples. Consequently, all the unknown functions and parameters were considered as random variables and assigned appropriate prior distributions as follows: Non-informative independent diffuse priors were assigned to the parameters of the linear fixed effects of the categorical variables so that the estimation can be data driven like in the classical approach. For the nonlinear effect of the metrical covariates, Bayesian P-splines prior as discussed in Lang and Brezger (2004) and Brezger and Lang (2006) was assumed. This entails the estimation of the function f as a linear combination of B-splines basis function
where \(B_i(Z)\) are B-splines. The coefficients \(\alpha _i\) are defined to follow a first or second order Gaussian random walk smoothness priors. A Gaussian Markov random field prior as proposed by Besag et al. (1991) and Fahrmeir and Lang (2001) was assumed for the geographical effects \(f_{spat}(s), s=1, \cdots , 37\). This is an extension of first-order random walk prior to two dimensional spatial arrays as discussed in (Rue and Held 2005). A possibility is to split the spatial effect into structured and unstructured as shown in these applications. In that case, Eq. 4 becomes
The unstructured term together with the random component, \(v_i\) are considered as independent and identically distributed. The amount of smoothness in the nonlinear and spatial effects are controlled by some variance parameter for example, \(\zeta ^2\), which can be simultaneously estimated with all the unknown smooth functions by assigning a highly dispersed but proper hyperprior such that \(\zeta ^2\sim IG(a,b)\). Commonly considered hyperparameters are \(a=1\) and \(b=0.005\) or \(a=b=0.001\) (Brezger et al. 2008). However, in addition to the above, we performed some sensitivity analysis by varying the choices using \(\hbox {a}=0.001\), \(\hbox {b}=0.001\); \(\hbox {a}=0.0001\), \(\hbox {b}=0.0001\); \(\hbox {a}=0.01\), \(\hbox {b}=0.01\). The results show indistinguishable differences.
Posterior samples are drawn from the full conditionals of single or block of parameters given the rest and the data through the efficient MCMC simulations. Additional parameters U of the continuous latent variable are included in the posterior analysis of the cumulative probit model.
For the cumulative probit models, the posteriors can be based on
Details of the sampling schemes are discussed in the manual of BayesX (Brezger et al. 2008). The end results of the posterior given in Eq. 5 have unknown distributions which permits the use of a Gibbs sampling procedure for the MCMC simulations with efficiency guaranteed by Cholesky decomposition for band matrices (Rue 2001).
4 Data analysis and results
4.1 Data analyses
Data analyses were carried out in line with WHO indicators for measuring child nutritional status. In order to be able to explore any possible trend in child nutritional status for Nigeria, a merged dataset was created from 2003, 2008, 2013 and 2018 NDHS. In total, 57,897 children with complete information on the variables of interest were included in data analyses from the four waves of the surveys after data cleaning. In line with Eq. 4, models with predictor \(\eta\) were fitted for each of the three AIs. The variables were included in phases from simple to complex ones in order to assess the gains of modelling based on subsets of the variables. The complete model was specified as follows:
The variables \(time_{2008}\), \(time_{2013}\) and \(time_{2018}\) are dummies created for the years 2008, 2013 and 2018 respectively with 2003 set as the reference category.
Further information on the modeling technique and other possible terms that can be considered beyond those included in this study are explained in Fahrmeir et al. (2013) In general, our model building was based on the following concepts:
The interaction term in \(M_6\) is a form of a geographically weighted term that allows to assess the varying effect of living in an urban area across the states.
4.2 Results
Based on the DIC as shown in Table 4, model with the predictor \(M_6\) turns out to be the best parsimonious; hence findings based on this model shall be presented and discussed. However, we shall compare the results of the spatial effects for model \(M_1\) with the aim of understanding how much of the spatial effects can be accounted for by the inclusion of different sets of covariates. First, results of the bivariate analysis are presented in Table 2. From the bivariate analyses, findings show a significant association between chronic malnutrition (i.e. stunting) and year of study. A reasonable decline in severe chronic malnutrition from 19 percent to 13 percent between 2003 and 2018 was significantly evident. There seems to be no significant drop in moderate chronic malnutrition during the same time frame. Regarding severe acute malnutrition (wasting), findings show significant association with year of study. Findings on combination underweight (chronic and acute malnutrition) also exhibit a significant decline across the study time frame. Mother’s age at birth, literacy status, educational attainment of mothers, household wealth status and geographical locations are significantly associated with the child’s nutritional status. Children of fifth birth order, from multiple births, born to mothers who did not receive assistance at birth and delivered at somewhere different from hospital are more likely to be severely stunted, wasted or underweight. Astonishingly, both chronic and acute malnutrition (and in turn both i.e. weight–for–age) are associated with underweight mothers.
Results for the linear fixed effects with predictor in model \(M_6\) are presented in Table 3. The Table presents estimates of the posterior means and the corresponding 95% credible intervals. Theta 1 and Theta 2 included in the Table are the threshold parameters of the ordinal response variable that represents the cut-off points for the severity of malnutrition (Brezger et al. 2008). In interpreting the estimates from the cumulative probit model, positive estimates imply the AI indicator for the children tends towards the normal category and hence, the children would be less likely to have suffered from malnutrition but the reverse is the case for negative estimates. The findings indicate that compared with the base year, i.e. 2003, the children were less likely to have been stunted in 2013 and in 2018 and the estimates are significant. Male children were more likely to have been stunted when compared with female children. Children whose mothers attained at least primary level of education and those from at least poorer households were less likely to have been stunted when compared with those whose mothers had no education and from the poorest households respectively. Children from households that source water from protected sources, those with improved toilet facilities, those from Christian religious groups, those whose deliveries took place in hospital, whose mothers were working at the time of the survey, and those who were of large size at birth were less likely to have been stunted when compared with their respective reference categories. However, children from the North West region, those of first or second to fourth birth order, those whose mothers had at least one ante natal care attendance, those who were of small size at birth and those that had diarrhoea in the two weeks before the survey were more likely to have been stunted. Estimates for the other categories are not significant.
Estimates for wasting in Table 3 shows that compared with year 2003, the chances of being wasted were higher in 2008 and in 2013 but significantly lower in 2018. Children whose mothers attained higher level of education were less likely to have been stunted when compared with those who mothers had no education but estimates for the other levels of education are not significant. Children of first or second to fourth birth and those who were of large size at birth were less likely to have been wasted when compared with their respective reference categories. On the other hand, children who reside in urban areas, those from the North West region, those whose mothers attended ante natal care only once, and those who had fever in the two weeks before the survey were more likely to have been wasted. Regarding underweight, children whose mothers attained at least primary level of education, those of Islamic or Christian religion, those from at least poorer households, those whose mothers had hospital delivery and those who were of large size at birth were less likely to have been underweight but male children, those from the North West region, those whose mothers were assisted during birth, those whose mothers had at least one ante natal care attendance, children who were of small size at birth and those who had diarrhoea or fever in the two weeks before the survey were more likely to have been underweight. All other estimates are not significant.
Findings on the nonlinear effects of the metrical covariates of mother’s age at marriage and mother’s age at birth (reported in years), mother’s BMI, and child’s age reported in months on stunting, wasting and underweight for model \(M_6\) are presented in Figs. 1, 2 and 3. The estimated nonlinear effects of the metrical covariates for stunting are presented in Fig. 1a–1d. The findings for age at marriage indicate that the children became more stunted with mother’s age at marriage up to around age 18 years from where the likelihood of being stunted reduces till around age 34 years at marriage. For mother’s BMI, the results show that the likelihood that children would be stunted reduces with increase in mother’s BMI. The same holds for mother’s age at birth of the child though the decline in this case was not as sharp as the case of BMI. As for the age of the child, the results show that from age 0 to around age 20 months, the children became stunted as they grow older after which a somehow sinusoidal pattern was observed. Regarding wasting (Fig. 2a–2d), the findings indicate that the likelihood that a child will be wasted increases with advancement in mother’s age at first marriage but reduces with mother’s BMI up to around 40 kg/m2 from where the chances increase. Child’s age presents a U shape in the first two years of life indicating that between birth and age 15 months, the children had high chances of being wasted but this reduces afterward. Mother’s age at birth of the child shows that the children born to women below age 20 years have less chances of being wasted followed by a kind of stable pattern till around age 40 years. Estimates for underweight (Fig. 3a–3d) shows that with mother’s age at marriage, the chances of the child being underweight are some who stable through the ages while, like for wasting, underweight reduces with mother’s BMI up to around 40 kg/m2. The result for child’s age follows the pattern obtained for stunting revealing that the level of underweight increases sharply with advancement in age but with a flat pattern between ages 13 and 27 months followed by a slight rise. Mother’s age at birth shows that up to around age 20 months, the chances of being underweight reduces followed by a flatten pattern till around age 30 months.

Nonlinear effects of a Respondent’s age at marriage, b Respondent’s Body Mass Index, c Child’s Age and d Mother’s age at the birth of child for Height-for-Age (Stunting)

Nonlinear effects of a Respondent’s age at marriage, b Respondent’s Body Mass Index, c Child’s Age and d Mother’s age at the birth of child for Weight-for-Height (Wasting)

Nonlinear effects of a Respondent’s age at marriage, b Respondent’s Body Mass Index, c Child’s Age and d Mother’s age at the birth of child for Weight-for-Age (Underweight)

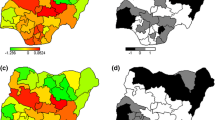
Maps of Nigeria showing the estimates of the spatial effects for height-for-age (Stunting) from \(M_1\) indicating: a Unstructured effect, b its location of the corresponding 95% credible intervals, c structured effect, d its location of the corresponding 95% credible intervals, e sum of structured and unstructured, and f its location of the corresponding 95% credible intervals

Maps of Nigeria showing the estimates of the spatial effects for weight-for-height (wasting) from \(M_1\) indicating: a Unstructured effect, b its location of the corresponding 95% credible intervals, c structured effect, d its location of the corresponding 95% credible intervals, e sum of structured and unstructured, and f its location of the corresponding 95% credible intervals

Maps of Nigeria showing the estimates of the spatial effects for weight-for-age (underweight) from \(M_1\) indicating: a Unstructured effect, b its location of the corresponding 95% credible intervals, c structured effect, d its location of the corresponding 95% credible intervals, e sum of structured and unstructured, and f its location of the corresponding 95% credible intervals
Results of the spatial effects for the three indicators obtained from model with predictor M1 are presented in Figs. 4, 5 and 6. The coloured maps are the posterior spatial effects while the maps in white, gray and black are those for the locations of the 95% credible intervals which are used in deciding the significance of the spatial effects. White colour signifies significantly higher estimate (the 95% credible interval strictly lie on the positive side), black colour signifies significantly lower estimate (the 95% credible interval strictly lie on the negative side), while estimates for states shaded in gray colour are not significant (the 95% credible interval include zero). The left panels for all the plots are the unstructured random effects while the structured spatial effects are presented in the right panels. Whereas the estimates for the unstructured random effects are not significant for all the indicators, the structured effects that take the neighbourhood structure of the states into account present a north–south divide for the three indicators. For stunting, lower estimates were obtained virtually in all the northern states; indicating that children from such states have significantly higher chances of being stunted. It is noteworthy that none of the states in any of the three southern regions has significantly higher chances of the children being stunted. Specifically, children from all the states in the North West geopolitical zone (Sokoto, Kebbi, Zamfara, Kaduna, Kano, Jigawa, and Katsina); in Borno, Yobe, Bauchi, Gombe, and Taraba in the North East zone; Niger, and Plateau in the North Central were more likely to have been stunted. On the other hand, except for Adamawa, Kwara, Nasarawa and Oyo states whose estimates are not significant, children from all the other states were less likely to have been stunted.
Estimates of spatial effects for wasting (Fig. 5c and 5d)) show that children from Kebbi, Sokoto, Borno, Yobe, Adamawa, Bauchi, Jigawa, Kano, Katsina and Kaduna were more likely to have been stunted but those from Ondo, Ekiti, Kogi, Benue, Enugu, Ebonyi, Abia, Bayelsa and Rivers were less likely. Results for underweight are similar to those for stunting showing that except for Taraba, Plateau, Nasarawa and Kwara (in the north), and Oyo and Ogun states where the estimates are not significant, children from all the other northern states were more likely to have been underweight but those from the other southern states were less likely.

Maps of Nigeria showing the estimates of the spatial effects for height-for-age (stunting) from \(M_6\) indicating: a Unstructured effect, b its location of the corresponding 95% credible intervals, c structured effect, d its location of the corresponding 95% credible intervals, e sum of structured and unstructured, and f its location of the corresponding 95% credible intervals

Maps of Nigeria showing the estimates of the spatial effects for weight-for-height (wasting) from \(M_6\) indicating: a Unstructured effect, b its location of the corresponding 95% credible intervals, c structured effect, d its location of the corresponding 95% credible intervals, e sum of structured and unstructured, and f its location of the corresponding 95% credible intervals

Maps of Nigeria showing the estimates of the spatial effects for weight-for-age (underweight) from \(M_6\) indicating: a Unstructured effect, b its location of the corresponding 95% credible intervals, c structured effect, d its location of the corresponding 95% credible intervals, (e) sum of structured and unstructured, and f its location of the corresponding 95% credible intervals

Map of spatially varying effect of urban based on model \(M_6\) for a stunting b its location of the 95% credible intervals; c wasting d its location of the 95% credible intervals; e stunting f its location of the 95% credible intervals
In comparison to model \(M_1\), estimates of the spatial effects of model \(M_6\) which is the model with the least DIC and supposedly the most parsimonious one, findings of the spatial effects show considerable difference compared with model \(M_1\) (Figs. 7, 8 and 9). By implication, adjusting for the sets of covariates as described earlier has helped in explaining some geographical variations in child malnutrition in Nigeria. For instance, Kwara state that has insignificant spatial variations in model \(M_1\) now turns out to be significantly associated to be stunted. Again, under five children Sokoto, Zamfara and Adamawa states that were associated to be stunted are now significantly associated with better height-for-age (normal). Apart from Kebbi state in North West and Bauchi, Gombe and Yobe states in North East that are still significantly associated with stunted children even after controlling for various covariates, the significantly negative effects that was obvious in model \(M_1\) have now become insignificant. On wasting, inclusion of different sets of covariates in model\(M_6\) has reduced the geographical variations in estimates of wasting. While Zamfara state with insignificant spatial variation in model \(M_1\) became positively significant, the negatively significant effect in model \(M_1\) are now insignificant in Sokoto, Katsina, Kaduna and Jigawa states in North West, Adamawa and Gombe states in North East. The findings show insignificant estimates in all the states in southern part apart from Bayelsa and Ebonyi states with significantly better nourished children according to weight-for-height. The results of spatial effects for underweight as presented in Fig. 9 for model \(M_6\) compared with that in Fig. 6 for model \(M_1\) present a somewhat different results. Taraba state with insignificant spatial effect in model \(M_1\) is now associated with improved child malnutrition status based on weight-for-age index. Similarly Zamfara state with significantly poor nutritional status based on weight-for-age index now has significantly improved status. Only children from Bauchi and Yobe states in North East, and Kebbi in North West as well as Niger state in North Central are still significantly associated with poor nutritional status according to weight-for-age.
Findings from the geographically weighted component of model \(M_6\) reveal no spatial variability in children height-for-age but for weight-for-height and weight-for-age. Figure 10a–f presents findings on geographically varying effect of urbanization. Generally urbanization has negative impact on children’s weight-for-height in the country but only in Oyo and Kano states with regards to child’s nutritional status based on underweight.
5 Discussion of results and conclusion
5.1 Discussion
Malnutrition has continued to remain a major public health issue in Nigeria and young children remain the major victims. Its determinants interact at different degrees to affect these children. Understanding the severity of malnutrition in children will to a large extent assist policy makers in designing appropriate intervention strategies. Policies premised on this will also enhance effective utilization of the scarce resources especially in the era of economic meltdown and global pandemic of corona virus that has raged devastating effect on the global communities. Benefits of proper and appropriate infant and youth feeding practices include but not limited to immune boosting to be able to fight several infectious diseases including the dreaded corona virus. Thus, it is important, for programmatic purposes, to continue to identify the important risk factors and geographical variations especially in a country with massive variations in cultural belief and socioeconomic status of its populace. This study, therefore, analyses undernutrition indicators among young children in Nigeria pooling data from four waves of the NDHS. The rationale was to identify spatial locations with high and low risks of malnutrition and to quantify the variations among important determinants in Nigeria. Using a cumulative probit model that extends the predictor to account for different categories of variables, the study identified striking north–south divide in the three nutritional indicators indicating that children from virtually all the northern states of Nigeria have higher chances of suffering from malnutrition. A programme to address the nutritional imbalance needs to take to account the wide variations in its design.
Evidently, significant spatial variations and trend were noticed on the three anthropometric indices among under five children in Nigeria. While some of these variations can be explained by the included covariates, it is still obvious that there are some residual spatial variations. The observed variations in the malnutrition indicators point to the existence of other important factors not covered by the survey that drive the nutritional status of children at different locations in the country. For instance, studies have revealed that there are cultural and religious beliefs in parts of the country that limit the freedom of women, who are the major care givers for children, on issues that have to do with taking decisions regarding their health and those of their children (Babalola and Fatusi 2009; Gayawan 2014). A 2015 report has it that two out of every three cases of acute malnutrition in northern Nigeria are unable to access treatment (ACF International and Nigeria 2015). Further, management services of acute malnutrition are unevenly spread across the country with some states offering the services in only half of the Local Government Areas particularly those concentrated in urban areas while the rural areas, where the majority of the populace reside, are left without the services (ACF International and Nigeria 2015). Also, a decomposition analysis of some determinants of malnutrition among young children in northern Nigeria and other parts of the country found that the effects of the same determinants act in different form in accelerating or retarding the linear growth of the young children thus highlighting the heterogeneous impact of the determinants (Amare et al. 2018). Consequently, a local solution that fits the specific needs of each part of the country needs to be designed in addressing the issue of malnutrition among children as, with existing evidence, solutions that work on southern part of the country, for instance, may not be appropriate if replicated in northern states.
It is not a gainsaying that maternal educational attainment plays a vital role in enhancing both maternal and child’s health as obtained from the three indicators considered. Educated women would understand the proper preventive and curative measures for their children, and where the needs arises, they would be in better position to express the needs of their children to medical experts than the uneducated women would do. This findings show consistency with several studies from other developing countries (Yadav et al. 2015; Pongou et al. 2006). Fagbamigbe et al. (2020) emphasized the effect of decomposition of educational inequalities in their study on severe acute malnutrition. The same explanation could hold for children from wealthy households as this offers adequate resources to cater for the needs of the children even though our findings show that children from wealthy households are associated with improved nutritional status of height-for-age and weight-for-age but not for weight-for-height. We also found children of working-women to be less likely to be stunted. These findings strengthen the need for women empowerment as a means of ensuring the wellbeing of their children since they are the ones often in custodians of their kids.
While the positive effect of parity or birth order was significant on wasting, reverse is the case for stunting and underweight. Multiple children at birth are negatively associated with the three anthropometric indices. Direct association was evident on child’s weight at birth with stunting. While children born as larger than average at birth are associated with improved nutritional status, their counterparts born as smaller than average are known to have worse nutritional status or malnourished. Analysis of DHS data from Zimbabwe and Malawi has provided evidence that the growth of low birth weight babies are well behind those of normal weight babies and that significant length difference are obvious at about twelve months of age (Mbuya et al. 2010; Ntenda 2019). In Indonesia, low birth weight was found to be the most dominant predictor associated with stunting (Aryastami et al. 2007). Episodes of diarrhoea and fever two weeks prior the survey are negatively and significantly associated with nutritional status. While children with diarrhoea are more likely to be stunted and underweight, those who had fever within the same time frame are likely to be wasted and underweight. Episode of illnesses definitely affects nutritional intake of children. The synergies between illnesses and nutrition are such that appetite for nutrition is supressed when a child suffers from an illness and nutritional deficiency, on the other hand, increases the child’s susceptibility to illness. Thus, preventive measures such as immunization and sanitation need to be reinforced in the country while health institutions are strengthened throughout the country to be able to cater for the needs of the populace particularly young children and pregnant women.
The study found younger age at marriage/cohabitation particularly below 18 years of age to be associated with stunted children. This finding might be expected because young mothers often lack the requisite knowledge of child care practices. A study in Ghana found that children of teenage mothers were about 8 times more likely to be stunted and 13 times more likely to be underweight when compared with those of adult mothers (Wemakor et al. 2018). Thus, it is imperative to reinforce the implementation of Child Right Act in order to further prevent teenage childbearing while children of teen mothers should be identified and assisted with nutritional and health interventions. The deteriorating nutritional status of the children as the advance in age could be associated with weaning and introduction of supplementary foods. Some of these foods are prepared in unhygienic conditions and since the immune systems of these children are still tender, they tend to be susceptible to various infections which subsequently reduce their food intake (Gayawan et al. 2019).
5.2 Conclusion
We employed multilevel structured additive regression to model the severity of malnutrition in Nigeria with the aim of understanding possible associated risk factors. Data from the Nigeria Demographic and Health Survey of 2003, 2008, 2013 and 2018 are used with the aim of understanding any spatio-temporal variations that may be present. The multilevel approach revealed that there are still some unexplained heterogeneity in understanding child nutritional issues in Nigeria. Findings from this study show that there are some puzzles to be unravelled as regards child malnutrition in Nigeria especially as the variations across the states persist after accounting for some observed variables. It is anticipated that further research beyond cross-sectional study may be employed to unravel the puzzle. Nigeria needs to intensify its efforts at ensuring that the SDGs 2 and 3 on child nutrition and health are accomplished. Knowing fully that malnutrition is one of the leading causes of childhood death and has permanent consequences for cognitive development, school attendance, economic productivity in adulthood and maternal reproductive outcome. Developing state-specific interventions should be given consideration since there still exists strong spatial correlations of associated risk factors of under five malnutrition. This can assist in prudent utilization of the scarce resources more importantly that the country depends mostly on donor-funded projects.
References
Abidoye R, Ihebuzor N (2001) Assessment of nutritional status using anthropometric methods on 1–4 year old children in an urban ghetto in Lagos, Nigeria. Nutrition and Health 15(1):29–39
ACF International, Nigeria A (2015) Severe acute malnutrition management in Nigeria: challenges, lessons & the road ahead
Adebayo SB (2004) Bayesian geoadditive modelling of breastfeeding initiation in Nigeria. J Appl Economet 19(2):267–281
Adekanmbi VT, Kayode GA, Uthman OA (2013) Individual and contextual factors associated with childhood stunting in Nigeria: a multilevel analysis. Matern Child Nutr 9(2):244–259
Ajao K, Ojofeitim E, Adebayo A, Fatusi A, Afolabi O (2010) Influence of family size, household food security status, and child care practices on the nutritional status of under-five children in Ile-Ife, Nigeria. Afr J Reprod Health 14(4):117–26
Akombi BJ, Agho K, Hall JJ, Meron D, Astell-Burt T, Renzaho AM (2017a) Stunting and severe stunting among children under- 5 years in Nigeria: a multilevel analysis. BMC Prediatrics 17(1):15
Akombi B, Agho K, Merom D, Hall J, Renzaho A (2017b) A multilevel analysis of factor associated with wasting and underweight among children under-five years in Nigeria. Nutrients 9(1):44
Amare M, Benson T, Fadare O, Oye M (2018) Study of the determinants of chronic malnutrition in Northern Nigeria: quantitative evidence from the Nigeria demographic and health surveys international food policy research institute (IFPRI) working paper 45 (September 2017). Food Nutr Bull 39(2):296–314
Ansuya BS, Nayak BU, George A, Shashidhara YN, Mundkur SC, Guddattu V (2018) Risk factors for malnutrition among preschool children in rural Karnataka: a case-control study. BMC Public Health 18:283
Aryastami NK, Shankar A, Kusumawardani N, Besral B, Jahari AB, Achadi E (2007) Low birth weight was the most dominant predictor associated with stunting among children aged 12–23 months in Indonesia. BMC Nutr 3(16):1–6
Babalola S, Fatusi A (2009) Determinants of use of maternal health services in Nigeria - Looking beyond individual and household factors. BMC Pregnancy Childbirth 9(43):1–13. https://doi.org/10.1186/1471-2393-9-43
Balogun TB, Yakubu AM (2014) Recent illness, feeding practices and father’s education as determinants of nutritional status among preschool children in a rural Nigeria community. J Trop Paediatr 61(2):92–99
Belitz C, Brezger A, Klein N, Kneib T, Lang S, Umlauf N (2015) BayesX - Bayesian inference in structured additive regression models. http://www.uni-goettingen.de/de/bayesx/550513.html. Accessed 20 March, 2016
Besag J, York Y, Mollie A (1991) Bayesian image restoration with two applications in spatial statistics (with discussion). Ann Inst Stat Math 43:1–59
Black RE, Victora CG, Walker SP, Bhutta ZA, Christain P, De Onis M, Ezzat M, Grantham-McGregor S, Katz J, Martorell R, Uauy R (2013) Maternal and child under nutrition and overweight in low-income and middle-income countries. Lancet 382(9890):427–451
Brezger A, Lang S (2006) Generalized structured additive regression based on Bayesian P-splines. Comput Stat Data Anal 50:967–991
Brezger A, Kneib T, Lang S (2008) BayesX - Software for Bayesian inference based o Markov Chain Monte Carlo simulation techniques. Available at http://www.stat.uni-muenchen.de/BayesX
De Onis M, Branca F (2016) Childhood stunting: a global perspective. Matern Child Nutr 12:12–26
Dewey K (2016) Reducing stunting by improving maternal, infant and young child nutrition in regions such as South Asia: evidence, challenges and opportunities. Matern Child Nutr 12(Suppl 1):27–38
Dewey K, Begum K (2011) Long-term consequences of stunting in early life. Matern Child Nutr 7:5–18
Edwards D, Thurstone L (1952) An internal consistency check for scale values determined by the method of successive intervals. Psychometrika 17:169–180
Fagbami AF, Kandala NB, Uthman OA (2020) Severe acute malnutrition among under 5 children in low-and middle-income countries: a hierarchical analysis of associated risk factors. Nutrition 75–76:110768. https://doi.org/10.1016/j.nut.2020.110768. (Epub 2020 Feb 14 PMID:32320941)
Fagbamigbe AF, Kandala NB, Uthman OA (2020) Decomposing the educational inequalities in the factors associated with severe acute malnutrition among under-five children in low- and middle-income countries. BMC Public Health 20(555):1–14
Fahrmeir L, Lang S (2001) Bayesian inference for generalized additive mixed models based on Markov random field priors. J R Stat Soc (Series C) 50:201–220
Fahrmeir L, Tutz G (2001) Multivariate statistical modelling based on generalized linear models. Springer-Verlag, New York
Fahrmeir L, Kneib T, Lang S, Marx B (2013) Regression: methods, methods and application. Springer, Berlin
Gayawan E (2014) Spatial analysis of choice of place of delivery in Nigeria. Sex Reprod Healthcare 5:59–67
Gayawan E, Aladeniyi OB, Oladuti OM, Olopha P, Adebayo SB (2019) Investigating the spatial patterns of common childhood morbidity in six neighboring west African countries. J Epidemiol Global Health 9(4):315–323
Ghosh-Jerath S, Singh A, Magsumbol MS, Kamboj P, Goldberg G (2016) Exploring the Potential of Indigenous Foodds to address hidden hunger: nutritive value of indigenous foods of Santhal tribal community of Jharkhand, India. J Hunger Environ Nutr 11:548–568
Goldstein H (2003) Multilevel statistical methods. England, Arnold, London
Idris SH, Popoola-Zakariya B, Sambo MN, Sufyan MB, Abubakar A (2013) Nutritional status and pattern of infant feeding practices among children under five in rural community of North western Nigeria. Int Q Commun Health Educ 33(1):83–94 (2012-2013)
Kothari M, Adferrahim N (2010) Nutrition update 2010. ICF Macro, Calverton, Maryland
Lang S, Brezger A (2004) Bayesian P-splines. J Comput Graph Stat 13:183–212
London School of Hygiene and Tropical Medicine (2009) The use of Epidemiological tools in conflict-affected populations: open Access Educational Resources for Policy-Makers
Mbuya M, Chideme M, Chasekwa B, Mishra V (2010) Biological, social, and environmental determinants of low birth weight and stunting among infants and young children in Zimbabwe, in Zimbabwe. (Vol. DHS Working Paper No. 7). Calverton ICF Macro
Mukuku O, Mishika PL, Mudisu LK, Tshibanda KN, Augustin M, Mutombo AM et al (2019) Factors associated with the time to breast feeding cessation among children aged one to four years in a Rural area in Democratic Republic of Congo. Global J Nutr Food Sci 2(2):1–15. https://doi.org/10.33552/GJNFS.2019.02.000533
National Population Commission (NPC) [Nigeria] and ICF (2019) Nigeria Demographic and Health Survey 2018. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF
National Population Commission (NPC) [Nigeria] and ICF Macro (2009) Nigeria Demographic and Health Survey 2008. Abuja, Nigeria: National Population Commission and ICF Macro
National Population Commission (NPC) [Nigeria] and ICF Macro (2014) Nigeria Demographic and Health Survey 2013. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International
National Population Commission (NPC) [Nigeria] and ORC Macro (2004) Nigeria Demographic and Health Survey 2003. Calverton, Maryland: National Population Commission ORC Macro
Ntenda PAM (2019) Association of low birth weight with undernutrition in preschool-aged children in Malawi. Nutr J 18(51):1–15
Pongou R, Ezzati M, Salomon JA (2006) Household and community socioeconomic and environmental determinants of child nutritional status in Cameroon. BMC Public Health 9:1–19
Rue H (2001) Fast sampling of Gaussian Markov random fields with applications. J R Stat Soc (Series B) 63:325–338
Rue H, Held L (2005) Gaussian Markov random fields. Theory and applications. Chapman & Hall/CRC, Boca Raton
UNICEF (2018) Infant and young child feeding: exclusive breastfeeding, predominant breastfeeding. In: UNICEF Data: Monitoring the Situation of Children and Women. https://data.unicef.org/tp[ic/nutrition/infant-and-young-child-feeding
Wemakor A, Garti H, Azongo T, Garti H, Atosona A (2018) Young maternal age is a risk factor for child undernutrition in Tamale Metropolis Ghana. BMC Res Notes 11(877):1–5
WHO Multicentre Growth Reference Study Group (2006) WHO child growth standards: Length/height-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. World Health Organization, Geneva
World Health Organization (2020) Fact sheets on malnutrition. https://www.who.int/news-room/factsheets/detail/malnutrition
WHO (2021) Joint child malnutrition estimates. https://www.who.int/data/gho/data/themes/topics/joint-child-malnutrition-estimates-unicef-who-wb. Accessed 21 July 2023
Yadav A, Ladusingh L, Gayawan E (2015) Does a geographical context explain regional variation in child malnutrition in India? J Public Health 23(5):277–287. https://doi.org/10.1007/s10389-015-0677-4
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ukwajunor, E.E., Adebayo, S.B. & Gayawan, E. Spatio-temporal modelling of severity of malnutrition and its associated risk factors among under five children in Nigeria between 2003 and 2018: Bayesian multilevel structured additive regressions. Stat Methods Appl 32, 1743–1777 (2023). https://doi.org/10.1007/s10260-023-00711-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10260-023-00711-3