
Abstract
B cell-activating factor (BAFF) promotes the survival, proliferation and maturation of B lymphocytes, which are key elements in the pathogenesis of systemic lupus erythematosus (SLE). This cytokine is encoded on TNFSF13B gene, and diverse single-nucleotide polymorphisms have been associated with susceptibility in different autoimmune disorders. In this study, the relationship of TNFSF13B gene rs9514827T>C, rs1041567T>A and rs9514828C>T polymorphisms, mRNA expression and soluble BAFF levels was investigated in 175 SLE patients and 208 healthy controls (HC). The TNFSF13B polymorphisms were evaluated by PCR–RFLP technique. The TNFSF13B gene expression was quantified through the RT-PCR assays. The soluble BAFF (sBAFF) levels were measured with ELISA test. There were no differences in genotype and allele frequencies for the three TNFSF13B polymorphisms, between SLE patients and HC. SLE patients showed 3.15-fold more TNFSF13B gene expression than HC. The patients who displayed most mRNA expression were those with active disease and the carriers of rs9514828 T variant allele. The sBAFF serum levels were higher in SLE patients compared to HC (2.083 vs. 0.742 ng/mL, p < 0.001). The SLE patients with active disease showed the higher sBAFF serum levels (2.403 ng/mL), mainly patients with lupus nephritis and hematological manifestations. In addition, a correlation of sBAFF with disease activity was found (r = 0.32, p < 0.001). In conclusion, the TNFSF13B gene polymorphisms were not found to be associated with SLE susceptibility in Mexican mestizos. Nevertheless, rs9514828C>T polymorphism seems to increase TNFSF13B gene expression. High BAFF expression is related to active disease, renal and hematological involvement; therefore, it could be considered as follow-up biomarker in SLE patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Systemic lupus erythematosus (SLE) is a prototype of autoimmune disease, characterized by loss of immune tolerance, overproduction of autoantibodies, immune complex deposition and a wide pool of clinical manifestations. SLE has highly heterogeneous physiopathology; however, B lymphocyte hyperactivity is a key element in the pathogenesis of SLE. B cell-activating factor (BAFF, also known as BLyS, TALL-1, THANK) belongs to the TNF superfamily [1]. This cytokine is implicated in survival, proliferation and maturation of B lymphocytes [2, 3] and T cell-independent antibodies class switching [4]. BAFF is encoded on TNFSF13B gene localized on chromosome 13q.32-34. The TNFSF13B gene is composed of 40,245 base pairs with six exons and seven introns [2, 5]. BAFF is a transmembranal protein expressed on myeloid lineage and some epithelial cells, through different stimuli such as IFN-γ, IFN-α, interleukin (IL)-10, Toll-like receptors (TLR)-3, TLR-4 and TLR-7 [5,6,7]. The soluble BAFF (sBAFF) form is obtained as consequence of proteolytic cleavage of transmembranal protein by a furin protease. It has been shown that under physiologic conditions sBAFF protein forms trimers, as well as oligomeric complexes [8, 9]. BAFF and their homologue a proliferation-inducing ligand (APRIL) which is another TNF superfamily member [10] can bind to the receptors transmembrane activator and calcium modulator and cyclophilin ligand interactor (TACI) and B cell maturation antigen (BCMA), with variable affinity based on stoichiometry [11, 12], while BAFF receptor (BR3) is specific to BAFF [13]. An excessive BAFF and APRIL production has been associated with development of autoimmune and clinical characteristics of SLE in murine models, as well as with others autoimmune diseases [13,14,15,16]. Multiple single-nucleotide polymorphisms (SNPs) in the TNFSF13B gene have been described and associated with different conditions, such as hepatic inflammation in hepatitis B virus infection [17], risk to develop mixed cryoglobulinemia in hepatitis C virus infection [18] and risk of cardiovascular disease in SLE [19]. Furthermore, TNFSF13B gene polymorphisms have been associated with susceptibility to develop different autoimmune diseases, such as immune thrombocytopenic purpura [20], rheumatoid arthritis and Sjögren’s syndrome [21,22,23,24]. The rs9514827T>C, rs1041567T>A and rs9514828C>T polymorphisms are localized in the promoter of TNFSF13B gene, and very little data have examined their association with mRNA expression in SLE. Therefore, the main objective of this study was to analyze the association between the TNFSF13B gene polymorphisms that includes the rs9514827T>C, rs1041567T>A and rs9514828C>T, and disease susceptibility, as well as the relationship with TNFSF13B gene expression, sBAFF serum levels and clinical parameters in SLE patients from western Mexico.
Materials and methods
Subjects
A total of 383 Mexican mestizos’ subjects were included in this study. The human ethics committee of West General Hospital approved the protocol under the next number 449/16. All the subjects signed an informed consent according to the Declaration of Helsinki [25] and Health Ministry of Mexico. One hundred seventy-five SLE patients were included in the study. All patients fulfilled the American College of Rheumatology 1997 classification criteria for SLE [26, 27]. The Mexican version of the Systemic Lupus Disease Activity Index (MexSLEDAI) [28] and Systemic Lupus International Collaborating Clinics (SLICC) damage index [29] was applied to all SLE patients at the enrollment of the study. Patients were classified according to the presence of disease activity in: inactive (MexSLEDAI < 2) and active (MexSLEDAI ≥ 2). A total of 208 Mexican mestizos were considered healthy controls (HC), recruited from the Department of Blood Transfusion Center from West General Hospital. The HC have no family history of autoimmune diseases.
DNA extraction and genotyping
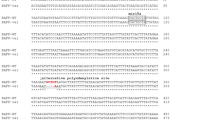
Genomic DNA was purified through peripheral blood leukocytes using the Miller’s technique [30]. To identify the rs9514827T>C, rs1041567T>A and rs9514828C>T genotypes, the polymerase chain reaction (PCR)–restriction fragment length polymorphisms (RFLP) technique was used. In rs9514827T>C and rs1041567T>A polymorphisms, the nucleotide sequence of the primers was: forward 5′ ATTCCCTGTCAGAATTTTCTCT3′ and reverse 5′CCTATAACTCCCACAATAAGGTGAC3′ [21], whereas in rs9514828C>T, the nucleotide sequence of primers was : forward 5′TTGTACACCGACCTGTTAGG 3′ and reverse 5′TGGAAGTAAGTCCACTGGGAAT3′ [21]. The PCR conditions were: initial denaturation cycle at 94 °C for 3 min; 35 cycles of denaturation for 30 s at 94 °C; annealing for 20 s at 57 °C; extension for 30 s at 72 °C; and final extension for 1 min at 72 °C. The 468-bp PCR product rs9514827T>C was digested with three units of Aci-I enzyme (New England BioLabs®, Ipswich, Massachusetts, USA) at 37 °C for 2 h. The digestion fragments were TT: 468 bp, TC: 468, 308 and 160 bp, and CC: 308 and 160 bp. The 468-bp PCR product rs1041567T>A was digested with three units of DpnII enzyme (New England BioLabs®, Ipswich, MA, USA) at 37 °C for 1 h. The digestion fragments were TT: 263 and 205 bp, TA: 263, 205, 169 and 94 bp, and AA: 205, 169 and 94 bp. Finally, the 398-bp PCR product rs9514828C>T was digested with three units of Aci-I enzyme (New England BioLabs®, Ipswich, MA, USA) at 37 °C 6 h. The digestion fragments were CC: 261 and 137 bp, CT: 398, 261 and 137 bp, and TT: 398 bp.
RNA extraction and reverse transcription
Total RNA was extracted from peripheral blood leukocytes using Trizol reagent (Invitrogen Life Technologies, Carlsbad, CA, USA) as per manufacturer’s protocol. The RNA concentration and OD260/280 were determined by spectrophotometry (NanoDrop lite, Thermo Scientific, USA), and the ratio was used to provide an estimate of the purity of the nucleic acid, in all samples ranged between 1.7 and 2.0. The RNA integrity was corroborated on 1X TBE agarose gel. The samples with low-quality or degraded RNA were excluded from the study. Complementary DNA (cDNA) was synthesized from 1 μg of total RNA using oligo-dT and GoScript™ Reverse Transcription System (Promega Corp., Madison, WI, USA) following the manufacturer’s protocol. The cDNA samples were stored at − 80 °C until the real-time PCR assays. The TNFSF13B mRNA expression was determined in forty SLE patients and fifteen HC carrying different genotypes for the rs9514827T>C, rs1041567T>A and rs9514828C>T TNFSF13B polymorphisms.
Quantitative PCR (qPCR)
The RT-qPCR followed the guidelines of the Minimum Information for Publication of Quantitative Real-Time PCR Experiments (MIQE) [31]. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used as a reference gene in order to determine relative quantification. The primers and hydrolysis probes were designed on the Roche Universal Probe Library software (TNFSF13B: probe cat. no. 4688988001, GAPDH: probe cat. no. 05190541001), and the primers were validated by gel electrophoresis. The TNFSF13B gene expression quantification (NM_006573.4) was performed by quantitative real-time PCR (qPCR) using the Nano Light Cycler 2.0 (Roche Applied Science, Penzberg, Germany). All samples were run as triplicates. After validation of PCR efficiencies for both genes, the obtained data were analyzed.
Serum BAFF levels
The sBAFF levels were quantified from sera of 101 HC and 167 SLE patients, with quantitative ELISA test (R&D systems®, Minneapolis, MN, USA) performed according to manufacturer’s recommendations. The samples were read at 450 nm by Multiskan™ Go Microplate Spectrophotometer (Thermo Fisher Scientific, Waltham, MA).
Statistical analysis
The data were analyzed using IBM SPSS statistics version 22 and GraphPad Prism version 6.0. The variables were expressed as median ± interquartile range (IQR) and frequencies according to the case. The frequencies of alleles and genotypes were compared using the Chi-square test and Fisher’s exact test, when appropriate. The haplotype inference was performed by EM algorithm using SHEsis software platform [32, 33]. A comparative threshold cycle (Ct) method with a cutoff of 40 cycles was used to determine TNFSF13B mRNA copy number relative to GAPDH based on 2−ΔΔCt method [34]. sBAFF serum levels were compared using Mann–Whitney U and Kruskall–Wallis tests according to the case. To analyze the relation of quantitative variables, Spearman’s correlation coefficient was used. p values < 0.05 were considered statistically significant.
Results
Demographic and clinical features
Two hundred eight HC, all women with a median age of 32 [interquartile range (IQR) 16–40] years old, and 175 SLE patients with a median age of 34 (IQR 24–44) years old (p = 0.449) were included. The SLE patients had 5 (IQR 2–11) years of disease evolution and 96% of them were women. The median of MexSLEDAI score was 2 (IQR 1–4, minimum 0, maximum 18), and SLICC damage score was 0 (IQR 0–1, minimum 0, maximum 7). The main clinical features of SLE patients were as follows: lymphopenia (54%), fatigue (27%), renal involvement (26%), which included active lupus nephritis (16%) and chronic kidney disease (10%), leukopenia (24%), arthritis (19%) and malar rash (17%). The less frequent affection was in the central nervous system (6%). The antinuclear antibody (ANA) was positive in 94% and anti-dsDNA antibody in 57% of SLE patients. The treatment of SLE patients at the time of the enrollment was prednisone in 72%, at median dose of 10 (IQR 5–20) mg/day, azathioprine in 58% and antimalarial in 54%.
Allele, genotype and haplotype frequencies of TNFSF13B gene polymorphisms
The control group was found in Hardy–Weinberg equilibrium for the three TNFSF13B gene polymorphisms. The allele and genotype frequencies for the rs9514827T>C polymorphism in the SLE patients were similar to HC (TT 64%, TC 34.3% and CC 1.7% vs. TT 63.9%, TC 33.7% and CC 2.4%, respectively), and no statistical difference was found (p > 0.05). Similarly, in rs1041567T>A polymorphism there were no differences in allele and genotype frequencies between groups (TT 1.7% TA 21.7% and AA 76.6% vs. TT 0.5%, TA 18.3% and AA 81.2%, respectively). In rs9514828C>T polymorphism, the allele and genotype frequencies were similar in SLE patients and HC (CC 51.4% CT 44% TT 4.6% vs. CC 55.2%, CT 39.1% and TT 5.7%, respectively). As result of haplotype analysis, moderate linkage disequilibrium was found (D′ = 0.737, p < 0.001, Fig. 1a). The distribution of all haplotype frequencies was similar in both HC and SLE patients (p > 0.05). Table 1 shows the allele, genotype and haplotype frequencies in both studied groups.

TNFSF13B gene expression and soluble BAFF levels. a Haplotype analysis of TNFSF13B gene polymorphisms (D′ = 0.737, p < 0.001). bTNFSF13B gene expression in HC and SLE patients. c sBAFF levels in HC and SLE patients. d sBAFF levels according to rs9514828C>T genotypes. eTNFSF13B gene expression in SLE patients according to dominant model of rs9514828C>T polymorphism, *p value was obtained by Mann–Whitney U test using quantitative gene expression data from 2−ΔCt method. f sBAFF levels in SLE patients according to dominant model of rs9514828C>T polymorphism. Qualitative gene expression data are shown through 2−ΔΔCt method. Mann–Whitney’s U test data are shown in median and IQR. HC, healthy controls; IQR, interquartile range; sBAFF, soluble BAFF; SLE, systemic lupus erythematosus
TNFSF13B gene expression and sBAFF serum levels
The TNFSF13B gene expression was 3.15-fold more in the SLE patients than HC (Fig. 1b). Likewise, the SLE patients had higher levels of sBAFF than HC (p < 0.001, Fig. 1c). When analyzed the sBAFF serum levels according to TNFSF13B gene SNPs, no differences were found (Fig. 1d). However, in SLE group the TNFSF13B gene expression was higher in carriers of rs9514828 T polymorphic allele compared to C/C homozygous genotype carriers (p < 0.05, Fig. 1e). Although those carriers of rs9514828 T variant allele showed higher TNFSF13B gene expression, differences in sBAFF serum levels were not found (p > 0.05, Fig. 1f). Furthermore, the higher TNFSF13B gene expression was observed in active patients that shown 2.94-fold more expression than inactive patients (Fig. 2a); similar to that observed with sBAFF serum levels.

BAFF expression and clinical disease activity in SLE patients. aTNFSF13B gene expression in inactive and active SLE patients. b sBAFF levels in inactive and active SLE patients. c Correlation between sBAFF levels and MexSLEDAI score in SLE patients. Qualitative gene expression analysis; data are shown through 2−ΔΔCt method. Kruskall–Wallis test, Dunn’s post hoc test; data are shown in median and IQR. Spearman’s correlation test. HC, healthy controls; IQR, interquartile range; sBAFF, soluble BAFF; SLE, systemic lupus erythematosus
sBAFF serum levels and SLE disease activity
The sBAFF serum levels were evaluated in SLE patients according to disease activity. The SLE patients with active and inactive disease had higher sBAFF serum levels in comparison with HC [2.403 (IQR 1.506–4.426, minimum 0.209, maximum 20.6) ng/mL and 1.707 (IQR 1.267–2.496, minimum 0.456 maximum 7.309) ng/mL vs. 0.742 (IQR 0.663–0.867, minimum 0.04, maximum 1.532) ng/mL, respectively, p < 0.001, Fig. 2b]. Likewise, the sBAFF serum levels were correlated with disease activity (r = 0.320, p < 0.001, Fig. 2c). Finally, the sBAFF serum levels were higher in SLE patients with lupus nephritis and hematological manifestations (p < 0.05) compared to those who did not have these clinical manifestations (Fig. 3).

Soluble BAFF levels according to SLE phenotypes. The sBAFF levels according to the main clinical manifestation in SLE patients are shown. Renal disorder included only active lupus nephritis (LN). Articular involvement (ART), included ≥ 2 joints with synovitis. Hematological disorder (HEM) included lymphopenia (< 1.4 × 103/uL), leukopenia (< 4.0 × 103/uL), hemolytic anemia and thrombocytopenia (< 100 × 103/uL). Mucocutaneous disorder (MUC) included malar rash, discoid lupus, mouth ulcers and alopecia. Mann–Whitney U test. Data are shown in median and IQR. ART, articular involvement; HEM, hematological disorder; IQR, interquartile range; LN, lupus nephritis; MUC, mucocutaneous; sBAFF, soluble BAFF
Discussion
Systemic lupus erythematosus is an autoimmune disease, characterized by autoantibodies production and the tissue immune complex deposition [35]. The physiopathology involves several factors; however, B lymphocyte hyperactivity plays a key role. Therefore, factors that promote B lymphocyte survival, proliferation and maturation could have relevance in onset or progression of the disease. Experimental studies have shown that BAFF is a critical B cell survival factor; BAFF absence or neutralization leads to reduced matured B cells, whereas excessive BAFF expression is associated with increased survival and expansion of autoreactive B cells [14, 36, 37].
Several studies have focused on TNFSF13B genetic variants as susceptibility markers in different autoimmune diseases. However, very little data have examined the TNFSF13B genetic variants in SLE, and there are no studies in Mexican population. In this study, three TNFSF13B gene polymorphisms (rs9514827T>C, rs1041567T>A and rs9514828C>T) were determined in SLE patients. In addition, the relationship between gene expression, sBAFF serum levels and clinical parameters was analyzed. There were no differences in the distribution of genotype and allele frequencies between SLE patients and HC, in the three evaluated TNFSF13B gene polymorphisms. Therefore, these genetic variants do not increase the risk of SLE development in western Mexican population. These TNFSF13B gene variants have been analyzed in Norwegian, Japanese and Greek SLE patients with different results [19, 22, 23, 38]. A recent study reported that TNFSF13B gene variants rs12583006T>A, rs9514828C>T and rs1041567T>A increase the susceptibility for SLE in Greek population [19]. However, similar to that found in this study, other reports have found no associations of TNFSF13B gene polymorphisms with the risk of SLE in Norwegian and Japan populations [23, 38].
In addition, the frequencies for the variant genotypes of rs9514827T>C and rs9514828C>T polymorphisms in western Mexico population were minor to those reported in European populations (rs9514827 CC genotype 2.4% vs. 11% and rs9514828 TT genotype 5.7% vs. 23%, respectively). It has been shown that western Mexican population is conformed mainly by European and Native American ancestry in 64.9 and 30.8% [39], which could explain these differences.
Furthermore, TNFSF13B TAC and CAT haplotypes were the most frequent in Mexican population, and no differences were observed between SLE patients and HC. Nossent et al. [24] reported that the CTAT and TTTT haplotypes of the TNFSF13B gene were associated with the increase in disease susceptibility and higher serum sBAFF levels, respectively, in Australian Sjögren’s syndrome patients. Interestingly, both haplotypes associated with these findings contained the rs9514828 T variant allele, which has been associated with increased TNFSF13B mRNA expression [23], higher sBAFF levels and autoantibodies in SLE and Sjögren’s syndrome [22, 24, 40]. In our study, SLE patients displayed 3.15-fold more TNFSF13B gene expression than HC. In addition, TNFSF13B gene expression was more significant in those SLE patients with active disease, as well as in carriers of rs9514828 T variant allele. In a previous study, the presence of rs9514828 T allele was associated with high TNFSF13B expression (2.6-fold) in a human promyelocytic cell line [41]. It has been suggested that the presence of rs9514828 T allele in a promoter consensus sequences could alter the binding of the transcription factor myeloid zinc finger protein (MZF1) and thus influence the TNFSF13B gene expression [42].
On the other hand, SLE patients with active disease displayed higher BAFF expression (2.94-fold more) compared with inactive SLE patients. Previously, it has been shown by Kawasaki et al, who found 11-fold more TNFSF13B gene expression in SLE patients in comparison with controls [23]; however, association with sBAFF levels was not observed. The relevant study by Zollar et al. reported that the BAFF transcript was associated with clinical and serological SLE activity. Also the high TNFSF13B expression would be predictive of disease activity over the ensuing year [43]. In this study, a relationship between high TNFSF13B gene expression and disease activity was found; however, it has no prospective data, which could be important to emphasize the use of mRNA expression, as disease biomarker.
The alterations in the BAFF/APRIL system have been described with development of autoimmune diseases. In murine models and humans, BAFF overproduction has been associated with development of autoimmunity with similar features of SLE [2]. Interestingly, in this study SLE patients had higher sBAFF levels (2.083 ng/mL) than HC (0.742 ng/mL). Even those SLE patients with inactive disease (1.707 ng/mL) displayed higher sBAFF levels than HC. In addition, sBAFF levels were correlated with disease activity (r = 0.32, p < 0.001). The sBAFF levels reported in healthy population is close to 0.9 ng/mL; it has been suggested that sBAFF levels could be useful for monitor disease activity in SLE patients [19, 38, 44,45,46,47]. Additionally, sBAFF levels have been associated with anti-DNA antibodies titers and SELENA-SLEDAI score; serum BAFF concentration ≥ 2 ng/mL has been proposed as a predictor of SLE flare [48, 49]. However, it must be considered that the sBAFF levels could be affected by treatment of SLE, mainly the use of the glucocorticoids [50], so the treatment must be taken into account when performing an evaluation of this cytokine. Furthermore, BAFF family has been associated with autoimmune disease. In a previous study by our group, SLE patients showed high BAFF and APRIL levels associated with disease activity and decreased BCMA expression on B cells. These findings suggest that the alterations in BAFF receptors expression lead to homeostasis deregulation and failures in control to excess of this cytokines in active SLE patients [51]. Moreover, the soluble BAFF and APRIL levels have been associated with clinical phenotypes of SLE, including arthritis, mouth ulcers, central nervous system involvement, hematological disorders, lupus nephritis, microalbuminuria and atherosclerosis related to lupus [19, 44, 45, 52, 53]. In this study, soluble BAFF levels were associated with active lupus nephritis and hematological disorder, as previously reported [51].
In conclusion, the rs9514827T>C, rs1041567T>A and rs9514828C>T polymorphisms in TNFSF13B gene are not associated with the high risk of SLE development in western Mexican population. Nevertheless, the rs9514828C>T polymorphism alters the TNFSF13B gene expression. The BAFF expression is associated with active disease, lupus nephritis and hematological affections. Therefore, BAFF expression can be considered as biomarker of disease activity in SLE. However, prospective studies in subgroups with specific phenotypes of disease are necessary to confirm these findings.
References
Moore PA, Belvedere O, Orr A, et al. BLyS: member of the tumor necrosis factor family and B lymphocyte stimulator. Science. 1999;285:260–3.
Schneider P, MacKay F, Steiner V, et al. BAFF, a novel ligand of the tumor necrosis factor family, stimulates B cell growth. J Exp Med. 1999;189:1747–56.
Mackay F, Browning JL. BAFF: a fundamental survival factor for B cells. Nat Rev Immunol. 2002;2:465–75.
Litinskiy MB, Nardelli B, Hilbert DM, et al. DCs induce CD40-independent immunoglobulin class switching through BLyS and APRIL. Nat Immunol. 2002;3:822–9.
MacKay F, Schneider P. Cracking the BAFF code. Nat Rev Immunol. 2009;9:491–502.
Sjöstrand M, Johansson A, Aqrawi L, et al. The expression of BAFF is controlled by IRF transcription factors. J Immunol. 2016;196:91–6.
Nardelli B, Belvedere O, Roschke V, et al. Synthesis and release of B-lymphocyte stimulator from myeloid cells. Blood. 2001;97:198–204.
Liu Y, Xu L, Opalka N, et al. Crystal structure of sTALL-1 reveals a virus-like assembly of TNF family ligands. Cell. 2002;108:383–94.
Cachero TG, Schwartz IM, Qian F, et al. Formation of virus-like clusters is an intrinsic property of the tumor necrosis factor family member BAFF (B cell activating factor). Biochemistry. 2006;45:2006–13.
Hahne M, Kataoka T, Schröter M, et al. APRIL, a new ligand of the tumor necrosis factor family, stimulates tumor cell growth. J Exp Med. 1998;188:1185–90.
Gross JA, Johnston J, Mudri S, et al. TACI and BCMA are receptors for a TNF homologue implicated in B-cell autoimmune disease. Nature. 2000;404:995–9.
Schuepbach-Mallepell S, Das D, Willen L, et al. Stoichiometry of heteromeric BAFF and April cytokines dictates their receptor binding and signaling properties. J Biol Chem. 2015;290:16330–42.
Vincent FB, Saulep-Easton D, Figgett WA, et al. The BAFF/APRIL system: emerging functions beyond B cell biology and autoimmunity. Cytokine Growth Factor Rev. 2013;24:203–15.
Mackay F, Woodcock SA, Lawton P, et al. Mice transgenic for BAFF develop lymphocytic disorders along with autoimmune manifestations. J Exp Med. 1999;190:1697–710.
Vincent FB, Morand EF, Schneider P, MacKay F. The BAFF/APRIL system in SLE pathogenesis. Nat Rev Rheumatol. 2014;10:365–73.
Thompson N, Isenberg DA, Jury EC, Ciurtin C. Exploring BAFF: its expression, receptors and contribution to the immunopathogenesis of Sjögren’s syndrome. Rheumatol Oxf. 2016;55:1548–55.
Han Q, Yang C, Li N, et al. Association of genetic variation in B-cell activating factor with chronic hepatitis B virus infection. Immunol Lett. 2017;188:53–8.
Ayad MW, Elbanna AA, Elneily DA, Sakr AS. Association of BAFF −871C/T promoter polymorphism with hepatitis C-related mixed cryoglobulinemia in a cohort of Egyptian patients. Mol Diagnosis Ther. 2015;19:99–106.
Theodorou E, Nezos A, Antypa E, et al. B-cell activating factor and related genetic variants in lupus related atherosclerosis. J Autoimmun. 2018;92:87.
Abdel-Hamid SM, Al-Lithy HN. B cell activating factor gene polymorphisms in patients with risk of idiopathic thrombocytopenic purpura. Am J Med Sci. 2011;342:9–14.
Zayed RA, Sheba HF, Abo Elazaem MAK, et al. B-cell activating factor promoter polymorphisms in Egyptian patients with systemic lupus erythematosus. Ann Clin Lab Sci. 2013;43:289–94.
Nezos A, Papageorgiou A, Fragoulis G, et al. B-cell activating factor genetic variants in lymphomagenesis associated with primary Sjogren’s syndrome. J Autoimmun. 2014;51:89–98.
Kawasaki A, Tsuchiya N, Fukazawa T, et al. Analysis on the association of human BLYS (BAFF, TNFSF13B) polymorphisms with systemic lupus erythematosus and rheumatoid arthritis. Genes Immun. 2002;3:424–9.
Nossent HC, Lester S, Zahra D, et al. Polymorphism in the 5′ regulatory region of the B-lymphocyte activating factor gene is associated with the Ro/La autoantibody response and serum BAFF levels in primary Sjögren’s syndrome. Rheumatology. 2008;47:1311–6.
World Medical Association. World Medical Association Declaration of Helsinki Ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–4.
Tan E, Cohen AS, Fries JF, et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982;25:1271–7.
Hochberg M. Updating the American College of Rheumatology. Arthritis Rheum. 1997;40:1997.
Guzman J, Cardiel MH, Arce-Salinas A, Sánchez-Guerrero J, Alarcón-Segovia D. Measurement of disease activity in systemic lupus erythematosus. Prospective validation of 3 clinical indices. J Rheumatol. 1992;19:1551–8.
Gladman D, Ginzler E, Goldsmith C, et al. The development and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for systemic lupus erythematosus. Arthritis Rheum. 1996;39:363–9.
Miller S, Dykes D, Polesky H. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988;16:1215.
Bustin SA, Vladimir B, Garson JA, et al. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin Chem. 2009;55:611–22.
Shi YY, He L. SHEsis, a powerful software platform for analyses of linkage disequilibrium, haplotype construction, and genetic association at polymorphism loci. Cell Res. 2005;15:97–8.
Li Z, Zhang Z, He Z, et al. A partition-ligation-combination-subdivision EM algorithm for haplotype inference with multiallelic markers: update of the SHEsis (http://analysis.bio-x.cn). Cell Res. 2009;19:519–23.
Livak KJ, Schmittegen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2−ΔΔCT method. Methods. 2001;25:402–8.
Tsokos GC, Lo MS, Reis PC, Sullivan KE. New insights into the immunopathogenesis of systemic lupus erythematosus. Nat Rev Rheumatol. 2016;12:716–30.
Schiemann B, Gommerman JL, Vora K, et al. An essential role for BAFF in the normal development of B cells through a BCMA-independent pathway. Science. 2001;293:2111–4.
Stohl W, Jacob N, Guo S, Morel L. Constitutive overexpression of BAFF in autoimmune-resistant mice drives only some aspects of systemic lupus erythematosus-like autoimmunity. Arthritis Rheum. 2010;62:2432–42.
Eilertsen G, Van Ghelue M, Strand H, Nossent JC. Increased levels of BAFF in patients with systemic lupus erythematosus are associated with acute-phase reactants, independent of BAFF genetics: a case-control study. Rheumatology. 2011;50:2197–205.
Martínez-Cortés G, Salazar-Flores J, Fernández-Rodríguez LG, et al. Admixture and population structure in Mexican-Mestizos based on paternal lineages. J Hum Genet. 2012;57:568–74.
Gottenberg J-E, Sellam J, Ittah M, et al. No evidence for an association between the −871 T/C promoter polymorphism in the B-cell-activating factor gene and primary Sjögren’s syndrome. Arthritis Res Ther. 2006;8:R30.
Novak AJ, Grote DM, Ziesmer SC, et al. Elevated serum B-lymphocyte stimulator levels in patients with familial lymphoproliferative disorders. J Clin Oncol. 2006;24:983–7.
Morris JF, Hromas R, Rauscher FJ. Characterization of the DNA-binding properties of the myeloid zinc finger protein MZF1: two independent DNA-binding domains recognize two DNA consensus sequences with a common G-rich core. Mol Cell Biol. 1994;14:1786–95.
Zollars E, Bienkowska J, Czerkowicz J, et al. BAFF (B cell activating factor) transcript level in peripheral blood of patients with SLE is associated with same-day disease activity as well as global activity over the next year. Lupus Sci Med. 2015;2:1–8.
Duan JH, Jiang Y, Mu H, Tang ZQ. Expression of BAFF and BR3 in patients with systemic lupus erythematosus. Braz J Med Biol Res. 2016;49:3–7.
Treamtrakanpon W, Tantivitayakul P, Benjachat T, et al. APRIL, a proliferation-inducing ligand, as a potential marker of lupus nephritis. Arthritis Res Ther. 2012;14:R252.
Morel J, Roubille C, Planelles L, et al. Serum levels of tumour necrosis factor family members a proliferation-inducing ligand (APRIL) and B lymphocyte stimulator (BLyS) are inversely correlated in systemic lupus erythematosus. Ann Rheum Dis. 2009;68:997–1002.
Elbirt D, Asher I, Mahlab-Guri K, et al. BlyS levels in sera of patients with systemic lupus erythematosus: clinical and serological correlation. Isr Med Assoc J. 2014;16:491–6.
Petri M, Stohl W, Chatham W, et al. Association of plasma B lymphocyte stimulator levels and disease activity in systemic lupus erythematosus. Arthritis Rheum. 2008;58:2453–9.
Petri MA, Van Vollenhoven RF, Buyon J, et al. Baseline predictors of systemic lupus erythematosus flares: data from the combined placebo groups in the phase III belimumab trials. Arthritis Rheum. 2013;65:2143–53.
Stohl W, Metyas S, Tan SM, et al. B lymphocyte stimulator overexpression in patients with systemic lupus erythematosus: longitudinal observations. Arthritis Rheum. 2003;48:3475–86.
Salazar-Camarena DC, Ortiz-Lazareno PC, Cruz A, et al. Association of BAFF, APRIL serum levels, BAFF-R, TACI and BCMA expression on peripheral B-cell subsets with clinical manifestations in systemic lupus erythematosus. Lupus. 2016;25:582–92.
Vincent FB, Northcott M, Hoi A, et al. Association of serum B cell activating factor from the tumour necrosis factor family (BAFF) and a proliferation-inducing ligand (APRIL) with central nervous system and renal disease in systemic lupus erythematosus. Lupus. 2013;22:873–84.
Phatak S, Chaurasia S, Mishra SK, et al. Urinary B cell activating factor (BAFF) and a proliferation-inducing ligand (APRIL): potential biomarkers of active lupus nephritis. Clin Exp Immunol. 2017;187:376–82.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Marín-Rosales, M., Cruz, A., Salazar-Camarena, D.C. et al. High BAFF expression associated with active disease in systemic lupus erythematosus and relationship with rs9514828C>T polymorphism in TNFSF13B gene. Clin Exp Med 19, 183–190 (2019). https://doi.org/10.1007/s10238-019-00549-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10238-019-00549-8