
Abstract
The priority aim of this study is to investigate the effect of carbon footprint, which is an indicator of environmental degradation, on health expenditures for the USA. In the study, cointegration analysis was performed for the period 1970–2016 by using health expenditures, carbon footprint, gross domestic product per capita and life expectancy at birth variables. According to the results of standard cointegration analysis, only cointegration relationship between health expenditures and income was found. In the models with carbon footprint, no cointegration relationship was discovered between the original values of the variables. This result was approached with suspicion, and it was thought that there might be a hidden cointegration between healthcare expenditures and carbon footprint. For this purpose, the hidden cointegration analysis and crouching error correction model proposed by Granger and Yoon [18] were employed among the positive and negative components of the variables of healthcare expenditures and carbon footprint. The results of the hidden cointegration analysis revealed that there was a hidden cointegration relationship between the positive components of healthcare expenditures and the positive components of carbon footprint. Analysis results show that a 1% increase in carbon footprint will cause a 2.04% increase in healthcare expenditures in the long term in the USA. When the positive components of the variables were considered, it was concluded that there was a one-way long-term asymmetric causality relationship between carbon footprint and healthcare expenditures. As a result of the study, it was proposed that the carbon footprint should be diminished to prevent the increasing burden of the healthcare expenditures on the budget.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
There are serious problems in the human–environment relationship. Environmental pollution can be ignored since economic returns are usually prioritized. However, nature has mechanisms to improve itself within its own cycle. As the interest in climate change and global warming is intensified, the issue of the emission of carbon dioxide and other greenhouse gases also constitutes one of the focal points. In order to reduce the effects of climate change, it is aimed at decreasing the emission of these gases and preventing their damages on the environment as much as possible. In the studies conducted on this issue, carbon footprint has started to be mentioned increasingly [19, 33, 49]. Carbon footprint has been developed within the scope of the concept of ecological footprint. Although there are relevant studies, the number of which is rising, there are also criticisms that there is confusion about its definition. The common point of the researchers is that the carbon footprint is a measure of the emission of a certain amount of carbon dioxide or other greenhouse gases together with carbon dioxide resulting from human production or consumption [51]. Carbon footprint is also used as a method of measurement showing the amount of the emission of CO2 and other greenhouse gases directly or indirectly. However, carbon footprint, which is one of the indicators of the environmental damage caused by human activities, can also be expressed as a spatial indicator measured in hectares or square meters [19, 24]. Since the concept of footprint refers to a spatial size, carbon footprint can be described as the areal size needed to clean the carbon and greenhouse gas pollution led by human beings in nature.
Increasing surface temperatures and rapid warming of the climate are seen as a serious threat to the environment. With the Kyoto Protocol (1998), many countries have accepted and recorded that the climate system has started to warm up and the presence of climate change. Global climate change causes damages that are difficult to recover in natural resources, degradation in ecosystems and extra greenhouse gas emissions. In addition, it is predicted that it will lead to increases in hurricane, heatwave, infectious diseases, fire and floods that may occur suddenly. This shows that human health is in serious danger due to climate change [29, 32]. Increasingly CO2 and other greenhouse gas emissions are shown as the source of the global climate change threat [25]. When evaluated from this point of view, carbon footprint, which is considered as an important measure of climate change effects, is an ecological indicator that calculates the pollution caused by human and production processes and takes into account the greenhouse gases which are listed in the Kyoto Protocol (CO2, CH4, N2O, SF6, HFCs and PFCs) [31]. There are also criticisms about which ones CO2, carbon-based gases or other greenhouse gases should be used in calculating the carbon footprint. Should only CO2 be used in the calculation? Should CO be used, which can easily be converted into CO2 with the chemical reaction in the atmosphere? Or to what extent is it correct to limit the calculation to greenhouse gases only? There are also discussions such as [51]. There are also claims that it cannot be a comprehensive environmental indicator, as it only takes into account carbon-based gases or greenhouse gases, as it does not take into account other chemicals harmful to the environment and does not contain content that indicates the destruction of natural resources [31].
The environment has a significant effect on the health. This interaction can occur directly via exposure to harmful environmental products as well as indirectly by degrading ecosystems which maintain their own lifecycle. The effect of environmental quality on health is a topic which is seriously studied [1, 9, 42]. According to the World Health Organization, nine out of every ten people breathe polluted air and air pollution comes first in the environmental risk ranking in 2019. Lungs, heart and brain can be damaged due to the exposure to polluted air. Besides, approximately 7 million people die from diseases such as lung diseases, cancer and paralysis every year. Moreover, it is thought that 250 thousand additional deaths will possibly occur annually between 2030 and 2050 due to malnutrition, diarrhea, malaria and high temperatures with the effect of climate change, which is significantly affected by carbon and other greenhouse gas emissions [52]. It is difficult to make a definite judgment about the short- and long-term effects of environmental degradation on health, because the duration of exposure to polluted air, exposure to different gases and the additive results of these effects can be separate for each pollutant. Another spatial and temporal effect of environmental quality on health is the economic dimension. Whereas there are many studies conducted on the determinants of healthcare expenditures [10, 11, 16, 22, 23, 30, 36, 37, 43], there is a limited number of studies focusing on environmental quality and healthcare expenditures [2, 7, 8, 38].
Although there is an increasing number of studies on the determinants of health expenditures, the literature examining the relationship between environmental indicators and health expenditures is still very limited. One of the most striking points in the studies examining the relationship between health expenditures and environmental indicators is that the studies in this field have started to gain new momentum [2, 6, 53]. For example, Apergis [2] reports that his recent study (in 2018) was the first study to examine the short and long-term effects of CO2 emissions on health expenditures for the United States. Especially the predictions that the effects of climate change are beginning to appear and that these effects will gradually increase in the future [15, 29, 44] show why these studies are given importance. In the studies that examine the relationship between health expenditures and environmental indicators, although CO2 or various greenhouse gases are considered as environmental indicators, no studies directly investigating the relationship between carbon footprint and healthcare expenditures have been encountered. The novelty of this study is that it is the first study to directly examine the relationship between health expenditures and carbon footprint, which can be considered as one of the important indicators of climate change. Another novelty of the study is that it is the first study to investigate the idea that there may be a hidden relationship between health expenditures and carbon footprint and their positive and negative components.
The aim of this study is to examine the long- and short-term relationship between healthcare expenditures and carbon footprint for the USA. Therefore, the hidden cointegration analysis and crouching error correction model were used. The reason for choosing these methods for the analysis is the possibility that a relationship which is perhaps invisible between the normal values of the variables may exist between the positive or negative components of the variables. In other words, it is aimed to put forward the hidden relationship, if available, between the relevant variables. The rest of this study is structured as follows: The next section presents a literature review of healthcare expenditures and environmental indicators. Followed by this section describes the data and methodological scope and the next section states the empirical results. The last section sets forth the conclusion and recommendations.
Literature review
There are numerous studies on healthcare expenditures available in the literature. Similarly, there are many studies assessing the effects of the environmental indicators. The studies investigating the relationship between healthcare expenditures and environmental indicators are in a limited number, however, they have started to gain momentum recently. Apergis et al. [2] state that the studies investigating the relationship between healthcare expenditures and CO2 emissions in the long and short terms for the USA are the first studies executed on this subject. In this study, the effect of the CO2 emissions on healthcare expenditures was examined via the panel quantile method by using the data of 1966–2009 for the USA. The results of the study indicate that CO2 emissions have a stronger effect on healthcare expenditures of the states which have higher expenditures on health. For the USA, researchers claim that policies for reducing carbon emissions will have a positive effect on decreasing healthcare expenditures. Likewise, Azad et al. [4] researched the effect of carbon emissions on healthcare expenditures in their study. For the countries of the South Asian Association for Regional Cooperation (SAARC), an analysis was performed through the panel quantile test and FMOLS and DOLS methods by using the data of 1995–2014. The results of the study point at a long-term positive relationship between per capita healthcare expenditures and carbon emissions.
In their study, Narayan and Narayan [38] analyzed eight OECD member countries using the data of 1980–1999. In this study, the long- and short-term relationship between per capita healthcare expenditures and per capita income and some environmental quality indicators was examined via the panel cointegration method. Carbon monoxide, sulfur oxide and nitrogen oxide emissions were taken into account as environmental quality indicators, and thus, they were found to be cointegrated with per capita healthcare expenditures and per capita income in the long term. Researchers concluded that per capita income and carbon monoxide emissions had a positive effect on healthcare expenditures in the short term. In a similar study, Yazdi et al. [54] researched the effect of the environmental quality indicators and income on healthcare expenditures. In the study where the ARDL method was used, the data of 1967–2010 were used for Iran. According to the results of the research, sulfur oxide and carbon monoxide emissions were found to have a positive effect on healthcare expenditures. Mehrara et al. [34] focused on the variables related to the environmental quality and investigated their relationship with healthcare expenditures and income. In the research, the data of 1995–2007 were used for more than 114 countries, and the panel cointegration method and error correction model were employed. The results of the research revealed that there was a direct relationship between healthcare expenditures and environmental quality indicators both in the long term and in the short term.
Jerrett et al. [26] examined the relationship between environmental variables and healthcare expenditures for 49 provinces of Ontario, Canada. In this study, the effect of total toxic pollution and municipal environmental expenditures on healthcare expenditures was analyzed through a two-stage regression model. According to the results obtained in the study, healthcare expenditures per capita were also found high in places with a high level of pollution. Besides, it was concluded that healthcare expenditures were lower in places where investment in public health and protection of the environmental quality was at a high level.
Wang et al. [50] examined the dynamic relationship between healthcare expenditures, CO2 emissions and economic growth. In the study, an analysis was performed with the ARDL method by using the data of 1995–2017 for Pakistan. According to the results of the study, for Pakistan, there is a short-term causality relationship between healthcare expenditures, CO2 emissions and economic growth. Moreover, a two-way causality was discovered between healthcare expenditures and CO2 emissions. In the short term, a one-way causality was identified from carbon emissions towards healthcare expenditures.
Zaidi and Saidi [55] researched the relationship between healthcare expenditures, environmental pollution and economic growth by using the data of 1990–2010 for Sub-Saharan African countries. In the study, the methods of ARDL and Granger causality analysis were used. Contrary to other studies in the literature, the results of the research revealed that the increase in CO2 and nitrous oxide emissions caused a decrease in healthcare expenditures. Additionally, a two-way causality relationship was discovered between CO2 emissions and healthcare expenditures.
In their study, Chaabouni and Saidi [7] investigated the causality relationship between CO2 emissions, healthcare expenditures and the GDP. The researchers reviewed 51 countries in the analysis and classified them in three groups: those with low incomes, those with below-moderate incomes and those with above-moderate incomes. According to the results of the analysis, a causality was found between the three variables examined. Besides, it was concluded that CO2 emissions led to healthcare expenditures for the countries other than those with low incomes.
In a study, Siti Khalijah [47] investigated the effect of Malaysia's environmental quality indicators and socioeconomic factors on healthcare expenditures for the period of 1970–2013. In the study, Carbon Dioxide (CO2), Nitrogen Dioxide (NO2) and Sulfur Dioxide (SO2) emissions were considered as environmental quality variables. In the study, the ARDL method was used to determine the short- and long-term effects. The results obtained in the study revealed that SO2, fertility and infant mortality rates significantly affected the healthcare expenditures of the country.
In the literature review, emissions of the gases such as carbon dioxide (CO2), nitrogen dioxide (NO2) and sulfur dioxide (SO2), carbon monoxide (CO), sulfur oxide (SO) and nitric oxide (NO) as environmental quality indicators or the sum of these as total toxic pollution were considered as variables. No studies directly investigating the effect of carbon footprint on healthcare expenditures were encountered. In this sense, this will be the first study directly investigating the relationship between healthcare expenditures and carbon footprint.
Materials and methods
Hidden cointegration
The analysis of the existence of a long-term relationship between the series is performed through the cointegration tests. The analysis of the long-term relationship for equally stable series can be tested via Engle-Granger cointegration analysis [14]. The absence of the standard cointegration relationship between the series indicates the absence of a long-term relationship between them. In this case, modeling of nonstationary series can be done with VAR by taking the first differences. But cointegration degrees may differ. Therefore, focusing on the relationship between the original states of the series may cause loss of information. However, what if there is a cointegration relationship between the positive and negative components of the series? In this case, it is concluded that there is hidden cointegration between the series. On the basis of the standard Engle-Granger cointegration test, it is possible to examine the long-term relationship between the positive and negative components of the series through the hidden cointegration analysis proposed by Granger and Yoon [18]. In this aspect, hidden cointegration is an example of nonlinear cointegration [18]. As stated in Beveridge and Nelson [5], any I(1) series of ARIMA (p, 1, q) representation includes a random walk component. Taking this into account, Granger and Yoon [18] shows the series X and Y in Eqs. 1 and 2 as two series with a random walk process.
In Eqs. 1 and 2, X0 and Y0 show the initial values. t = 1, 2,…, T and ε and η refer to the error terms having the white noise process with a mean of 0. Here, the variables for which the cointegration relationship is sought are not Xt and Yt, but their positive and negative components. Thus, for achieving hidden cointegration, the negative and positive components stated in Eqs. 3 and 4 must be defined.
Considering Eqs. 3 and 4, the error terms can be written as ε = ε+ + ε− and η = η+ + η−. Accordingly, Eqs. 1 and 2 can be written as in Eqs. 5 and 6.
Hence, Xt and Yt series can be arranged as in Eqs. 7 and 8:
Positive components in Eqs. 7 and 8 were assumed as \({X}_{t}^{+}=\sum_{i=1}^{t}{\varepsilon }_{i}^{+}\) and \({Y}_{t}^{+}=\sum_{i=1}^{t}{\eta }_{i}^{+}\), and negative components were assumed as \({X}_{t}^{-}=\sum_{i=1}^{t}{\varepsilon }_{i}^{-}\) and \({Y}_{t}^{-}=\sum_{i=1}^{t}{\eta }_{i}^{-}\). The change in positive and negative components are \(\Delta {X}_{t}^{+}={\varepsilon }_{i}^{+}\), \({\Delta Y}_{t}^{+}={\eta }_{i}^{+}\), \({\Delta X}_{t}^{-}={\varepsilon }_{i}^{-}\) and \({\Delta Y}_{t}^{-}={\eta }_{i}^{-}\). When Engle-Granger [14] cointegration analysis is implemented for the positive and negative components obtained, Granger-Yoon [18] hidden cointegration analysis will have been executed.
Crouching error correction models
When the hidden cointegration relationship was detected, crouching error correction models were proposed by Granger and Yoon [18]. When the existence of a cointegration is accepted between Xt and Yt, the crouching error correction models are written as in Eqs. 9 and 10:
Here \(lags\left({\varepsilon }_{t-1}^{+},{\eta }_{t-1}^{+}\right)\) is the various lags of \({\varepsilon }_{t-1}^{+} \,{\text{and}}\, {\eta }_{t-1}^{+}\), which is the remnant of the long-term forecast. Thus, the terms \(\Delta {X}_{t}^{+}\) and \(\Delta {Y}_{t}^{+}\) are formed as in Eqs. 11 and 12:
Here, \({\gamma }_{1}\) and \({\delta }_{1}\) are error correction coefficients. The dependent variable in the equation whose error correction coefficient is insignificant is defined as permanent component in the system [35].
Many studies were conducted after Granger and Yoon [18] suggested that the idea that there may be hidden cointegration between their positive and negative components, though not among the original states of the series. Hatemi and Irandoust [21] examined the hidden cointegration with the method of Johansen cointegration. Hatemi‐J [20] has extended the hidden cointegration analysis for panel data. Schorderet and Shin et al. [45, 46] used the Nonlinear ARDL Framework asymmetric cointegration method. Hidden cointegration studies are expanding. Further studies are possible to expand with studies such as the fractionally cointegrated vector autoregressive (FCVAR) method [27, 28], where the degree of integration can be fractional, and Fourier cointegration [48] that taking into account multiple structural breaks.
Data
In this research, hidden cointegration between the variables of health expenditures, carbon footprint, gross domestic product per capita and life expectancy at birth was investigated by using the data of 1970–2016 for the USA. The data of healthcare expenditure (HE) was obtained from the OECD database as % of the GDP. The healthcare expenditure variable measures the expenditures made for health care services including the curative care, rehabilitation care, long-term care, ancillary services, medical products, prevention, public health services and health management, excluding healthcare investments. The healthcare expenditures variable included in the research was considered as the sum of government expenditures and compulsory and voluntary health insurance expenditures [40]. In Fig. 1, the graph of the USA for healthcare expenditures between 1970 and 2016 is presented.

Source: OECD Health Statistics Database
Healthcare expenditures of the USA (1970–2016, % of the GDP).
As seen in Fig. 1, healthcare expenditures have a tendency to increase continuously as a share in the GDP of the USA. Whereas the share of healthcare expenditures in the GDP was 6% in the 1970s, it approached 18% in 2016. The increase between 1970 and 2016 appears about threefold. This means that more resources should be allocated to healthcare expenditures for the United States.
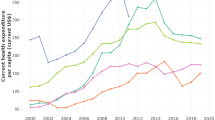
The carbon footprint variable used in this study was taken from the Global Footprint Network, which provides open access and calculates the ecological footprint showing the human demand and the capacity of nature to fulfill this demand. Carbon footprint is the amount of the area included in the calculation of the ecological footprint and required for the absorption of CO2 emitted into nature. The carbon footprint variable was measured in respect of global hectares (gha) per capita (ConsPerCap) of consumption. The footprint of consumption is the amount of the area needed to produce the consumed products and absorb the emerging CO2 emission. The global hectare is a biologically productive 1-ha area that indicates the average biological productivity in the world in a certain year [17]. In Fig. 2, the carbon footprint graph of the USA is shown for 1970–2016.

Source: Global Footprint Network
Carbon footprint of the USA (1970–2016, EFConsPerCap).
When Fig. 2 is reviewed, the carbon footprint of the USA is about 8 gha from the 1970s until the 1980s. From 1980 to 2006, it was determined as approximately 7 gha per capita. It decreases down to 5 gha after 2006. These data reveal that the USA tried to keep its carbon footprint within a certain range between 1970 and 2016. Especially after 2006, it is understood that it has been attempted to reduce the environmental effect of carbon emissions.
The gross domestic product per capita (GDPPC) and life expectancy at birth (LEX) variables were obtained from World Bank’s World Development Indicators. In this study, natural logarithmic states of the variables were used and analyzes were performed with Eviews 9.5 program.
Empirical results
The presence of a long-term relationship between healthcare expenditures and carbon footprint may not be seen when it is only examined between the normal values of these variables. Probably, there is a relationship between the hidden components of these variables. The hidden cointegration analysis was executed to reveal it. To execute cointegration analysis, the variables must be integrated at I(1) level. The unit root test was carried out to specify the stationary levels of the variables. For healthcare expenditures (HE) and carbon footprint (CF) variables, Augmented Dickey Fuller (ADF) [13] and Phillips-Perron (PP) [41] unit root tests were conducted for the conditions with fixed-term, conditions with fixed term and trend, conditions without fixed term and trend, and the results of the unit root test are shown in Table 1.
The results in Table 1 indicate that the Healthcare Expenditures (HE) and Carbon Footprint (CF) variables are I(1) according to ADF and PP tests. These results mean that the cointegration relationship can be sought between these variables. Engle-Granger cointegration analysis was carried out to research the presence of the long-term relationship between variables, and the results are given in Table 2.
The results acquired in Table 2 are the results of the cointegration analysis obtained for the intercept term model. According to these results, no cointegration relationship was discovered between healthcare expenditures and carbon footprint. With the idea that a cointegration relationship might exist between the positive and negative components of these variables, it was decided to implement the hidden cointegration analysis. For this, the positive and negative components of the healthcare expenditures and carbon footprint variables were first obtained, and then the unit root tests were carried out. Since the intercept term model was preferred in the cointegration analysis, the ADF intercept term unit root test results for these components are presented in Table 3.
According to the results of the unit root test stated in Table 3, it is observed that the positive and negative cumulative shocks of the healthcare expenditures (HE) and carbon footprint (CF) variables are I(1) for the intercept term model. According to these results, hidden cointegration analysis can be conducted between the variables. In Table 4, the results of Granger and Yoon [18] hidden cointegration tests are presented.
The results in Table 4 indicate that the finding in Table 2 showing that there is no cointegration relationship between the healthcare expenditures and carbon footprint variables (HE–CF) is unreliable, because, in Table 4, the existence of a long-term relationship is observed between the cumulative positive shocks of healthcare expenditures and cumulative positive shocks of carbon footprint (HE+–CF+). According to this result, healthcare expenditures and carbon footprint react at shocks in a different way in the USA. It is observed that a positive shock in carbon footprint acts with the effect of a positive shock in healthcare expenditures. The long-term equilibrium equation is shown in Eq. 13 based on the existence of the long-term relationship between the cumulative positive shocks of healthcare expenditures and cumulative positive shocks of carbon footprint (HE+–CF+).
In the long-term equation given in Eq. 13, the coefficients were found statistically significant. According to the coefficients, a positive shock of 1% that will occur in the carbon footprint will cause an increase of 2.04% in healthcare expenditures. On the basis of the long-term equation, crouching error correction models are presented in Eqs. 14 and 15.
Crouching error correction models were obtained through Stepwise regression method by using maximum 10 lagged variables. In the models given in Eqs. 14 and 15, it is observed that all the coefficients are significant. Moreover, the negative and significant error correction coefficient (εt-1) in Eq. 14 signifies that the system will reach the long-term equilibrium. The error correction coefficient shows that the short-term disequilibriums will be improved within approximately 7 years. In the model given in Eq. 15, the positive error correction coefficient (εt-1) means that the crouching error correction model does not function for this equation. These results reveal that the CF+ variable is a permanent component and the HE+ variable is a transitory variable. In other words, the long-term dynamics are determined by the carbon footprint. A positive shock in the carbon footprint influences both itself and the increase in healthcare expenditures in the long term, which ensures the long-term equilibrium. Besides, a positive shock in healthcare expenditures is not permanent in the long term; it causes a temporary effect. So, it can be said that the CF+ variable is the long-term asymmetric cause of the HE+ variable. In other words, the increase in carbon footprint is the cause of the increase in healthcare expenditures in the long term. The opposite case is not possible. That is, the HE+ variable is not the long-term asymmetric cause of the CF+ variable. Considering the positive components, there is a one-way long-term asymmetric causality relationship between carbon footprint and healthcare expenditures.
In the model, which was established among the positive components of healthcare expenditures and carbon footprint, has also investigated whether there were structural breaks. Least Squares with Breaks Bai–Perron break type method was used to determine the structural break periods and coefficients of these periods. The results are shown in Eqs. 16 and 17.
When Eqs. 16 and 17 are examined, it is seen that a break has occurred in the model in 1981. In the model, constant terms were not significant for both periods. In the structural break model, it is observed that the effect of carbon footprint on health expenditures was higher after 1981. This can be explained by the fact that the effects of climate change are becoming increasingly apparent since this period.
Although the study focuses on especially health expenditures and carbon footprint variables, it is also aimed to investigate whether there is a cointegration relationship between the original states and their positive and negative components of the variables by adding different variables to the model. Gdp, age and population come to the forefront as the most important variables in the studies of health expenditure for USA, Canada and some developed countries [11, 23, 37, 43]. Therefore, analysis was made again by adding Gross Domestic Product Per Capita (GDPPC) and Life Expectancy at Birth (LEX) variables. Unit root test results of the added variables in Table 5 are shown. When the graph of GDPPC and LEX variables is examined, the unit root test was performed as a trend and intercept since a clear trend effect was seen.
The results in Table 5 indicate that the GDPPC, LEX and their positive and negative components are I(1) according to ADF and PP tests. These results mean that the cointegration relationship can be sought between these variables. First of all, the cointegration relationship between HE, CF, GDPPC and LEX was examined by the Engle-Granger [14] cointegration analysis. Then, the hidden cointegration relationship between their positive and negative components was investigated by Granger and Yoon [18] hidden cointegration method. The results are shown in Table 6.
According to these results, no cointegration relationship was discovered between healthcare expenditures, carbon footprint, gross domestic product per capita and life expectancy at birth and their positive and negative components. Besides, only cointegration between health expenditures and income has been observed. This result is compatible with other studies [12, 37, 39, 53] showing that income has a significant impact on health expenditures.
Conclusion
The damage given to the environment by human beings appears in various forms. This happens sometimes directly and sometimes indirectly. Since economic returns are prioritized, the environment is degrading increasingly. The results do not emerge only as the environmental damage. Health is also influenced at a significant level. This study examines the effect of environmental degradation on human health in terms of carbon footprint, which is a measure of environmental degradation, and healthcare expenditure variables. In the study, it was researched whether there was a relationship between healthcare expenditures and carbon footprint in the long term. According to the results of the cointegration analysis, no cointegration relationship was discovered between the original values of the variables. This result was approached with suspicion, and it was thought that there might be a hidden cointegration between healthcare expenditures and carbon footprint. For this purpose, the hidden cointegration analysis proposed by Granger and Yoon [18] was conducted between the positive and negative components of the healthcare expenditures and carbon footprint variables. The results of the hidden cointegration analysis show that there is a hidden cointegration relationship between the positive components of healthcare expenditures and the positive components of carbon footprint.
The coefficients were found statistically significant in the long-term equation between the variables. According to the coefficients calculated, a positive shock of 1% that will occur in the carbon footprint will cause an increase of 2.04% in healthcare expenditures in the long term. When this result is evaluated in terms of the impact of various environmental indicators on health expenditures, it supports the following studies: The study examining low, low-middle, upper-middle, high-income countries conducted by Apergis et al. [3] stated that the decrease in carbon emissions will reduce health expenditures. The study implemented by Yahaya et al. [53] stating that the increase in air pollutants in developing countries has an effect on increasing health expenditures. In their study, Apergis [2] concluded that US states with higher CO2 emissions have more health expenditures. In their study, Narayan and Narayan [38] have reached the conclusion that environmental quality indicators in eight OECD countries have a positive impact on health expenditures in the short and long term. Jerrett et al. [26] showed that in areas of Canada's states with high pollution, per capita health expenditures are also high. Unlike these results, in the study conducted by Zaidi and Saidi [55], it was revealed that the increase in CO2 and Nitrous oxide emissions for Sub-Saharan African countries caused a decrease in health expenditures.
The crouching error correction models were also calculated on the basis of the long-term equation for the positive components of the variables of healthcare expenditures and carbon footprint. The error correction coefficient showed that the short-term disequilibriums will be improved within approximately 7 years. The results obtained from the error correction model indicate that the positive component of the carbon footprint is the permanent component. It is stated that the reason behind the increase in healthcare expenditures is the increase in the carbon footprint in this long term. The opposite case is not possible. That is, it is not right to show the increase in healthcare expenditures as the reason behind the increase in carbon footprint. Hence, when positive components are regarded, it can be concluded that there is a one-way long-term asymmetric causality relationship between carbon footprint and healthcare expenditures. When this result is evaluated in terms of causality between environmental indicators and health expenditures, it is supported by the Chaabouni and Saidi's [7] study, which has been concluded that in upper-middle income countries, CO2 emissions are the cause of health expenditures. However, it differs from the result of Wang et al. [50] and Zaidi and Saidi [55], who found a bidirectional causality relationship between CO2 emissions and healthcare expenditures. In the model, has also investigated whether there were structural breaks for the positive components of healthcare expenditures and carbon footprint. It was observed that there was a break in 1981. In the structural break model, the effect of the carbon footprint on health expenditures is higher after 1981. This can be explained by the increasingly visible effects of climate change. In addition, Gross Domestic Product Per Capita and Life Expectancy at Birth variables were added to the model and it was re-investigated whether there is a cointegration relationship between the original states and the positive and negative components of the variables. Apart from health expenditures and income, there was no cointegration relationship between other variables and their components.
The United States has encountered several consequences of climate change in the near past. In the future, it is estimated that they will face similar situations frequently. Knowlton et al. [29] investigated the cost on the health of natural disasters such as hurricanes, heat waves, floods, infectious disease outbreaks, river floods and fires caused by climate change in the USA between 2000 and 2009. While the cost of health was estimated at $740 million in this period, these costs exceeded $14 billion as a result of these events. Health problems caused by climate change include diseases caused by water pollution, pollen allergies and food-borne diseases that increase due to increased carbon emissions. Despite these serious threats, the idea that the cost to be undertaken to reduce greenhouse gas emissions is high stands as an obstacle to taking steps in this direction. However, problems arising from climate change will put serious pressure on the public budget. In the 1970s, the share of healthcare expenditures in the GDP in the USA was around 6%, however, it was approximately 18% in 2016. Within this time frame, the share of healthcare expenditures in the GDP was tripled. This forms a serious budget burden for the USA. It should not be ignored that the share of the healthcare expenditures in the GDP may increase over time. In this study, it was discovered that the increase in carbon footprint was the cause of the increase in healthcare expenditures, and a 1% increase in carbon footprint would lead to a 2.04% increase in healthcare expenditures in the long term. These rates take into account the period data investigated in this study and reflect the current situation. It shows that the carbon footprint as a measure of the possible effects of climate change, in the future, may affect health expenditures above the rate determined in this study. According to the results of the study, policy makers in the USA should take precautions to decrease their carbon footprint if they do not want healthcare expenditures to constitute an increasing burden on the budget. It should be known that delay in taking action against the negative effects of climate change will have very expensive consequences [15, 29, 44]. To this end, the policy proposal to mitigate the inevitable impacts of climate change is to set up urgent action priorities with a comprehensive national planning. The most important share in the increase in greenhouse gas emissions is fossil fuel use and deforestation. Therefore, it is important to consider the plans as a priority in order to ensure more use of clean and renewable energy resources, to maintain researches aiming at increasing energy efficiency and to increase forest areas.
Change history
21 October 2020
The author would like to correct the errors in the publication of the original article.
References
Ahmad, M., Ur Rahman, Z., Hong, L., Khan, S., Khan, Z., Naeem Khan, M.: Impact of environmental quality variables and socio-economic factors on human health: empirical evidence from China. Pollution 4(4), 571–579 (2018)
Apergis, N., Gupta, R., Lau, C.K.M., Mukherjee, Z.: US state-level carbon dioxide emissions: Does it affect health care expenditure? Renew. Sustain. Energy Rev. 91, 521–530 (2018)
Apergis, N., Bhattacharya, M., Hadhri, W.: Health care expenditure and environmental pollution: a cross-country comparison across different income groups. Environ. Sci. Pollut. Res. 27(12), 1–15 (2020)
Azad, A.K., Abdullah, S.M., Fariha, T.R.: Does carbon emission matter for health care expenditure? Evidence from SAARC region using panel cointegration. J. Polit. Econ. Polit. 34(1), 611–634 (2018)
Beveridge, S., Nelson, C.R.: A new approach to decomposition of economic time series into permanent and transitory components with particular attention to measurement of the “business cycle”. J. Monet. Econ. 7, 151–174 (1981)
Blázquez-Fernández, C., Cantarero-Prieto, D., Pascual-Sáez, M.: On the nexus of air pollution and health expenditures: new empirical evidence. Gac. Sanit. 33, 389–394 (2019)
Chaabouni, S., Saidi, K.: The dynamic links between carbon dioxide (CO2) emissions, health spending and GDP growth: a case study for 51 countries. Environ. Res. 158, 137–144 (2017)
Chen, L., Zhuo, Y., Xu, Z., Xu, X., Gao, X.: Is carbon dioxide (CO2) emission an important factor affecting healthcare expenditure? Evidence from China, 2005–2016. Int. J. Environ. Res. Public Health 16(20), 3995 (2019)
Corvalán, C., Kjellström, T., Smith, K.: Health, environment and sustainable development: identifying links and indicators to promote action. Epidemiology 10(5), 656–660 (1999)
Crémieux, P.Y., Ouellette, P., Pilon, C.: Health care spending as determinants of health outcomes. Health Econ. 8(7), 627–639 (1999)
Di Matteo, L.: The determinants of the public–private mix in Canadian health care expenditures: 1975–1996. Health Policy 52(2), 87–112 (2000)
Di Matteo, L., Di Matteo, R.: Evidence on the determinants of Canadian provincial government health expenditures: 1965–1991. J. Health Econ. 17(2), 211–228 (1998)
Dickey, D.A., Fuller, W.A.: Distribution of the estimators for autoregressive time series with a unit root. J. Am. Stat. Assoc. 74(366a), 427–431 (1979)
Engle, R.F., Granger, C.W.J.: Cointegration and error correction: representation, estimation, and testing. Econometrica 55, 251–276 (1987)
Epstein, P.R., Mills, E.: Climate change futures: health, ecological and economic dimensions. The Center for Health and the Global Environment, Harvard Medical School (2005)
Gbesemete, K.P., Gerdtham, U.G.: Determinants of health care expenditure in Africa: a cross-sectional study. World Dev. 20(2), 303–308 (1992)
Global Footprint Network: Carbon footprint https://www.footprintnetwork.org/resources/glossary/, Accessed 12 November 2019 (2019)
Granger, C.W., Yoon, G.: Hidden cointegration. U of California, Economics Working Paper, (2002–02) (2002)
Hammond, G.: Time to give due weight to the “carbon footprint” issue. Nature 445(7125), 256 (2007)
Hatemi‐J, A.: Hidden panel cointegration. Munich Personal RePEc Archive Paper No. 31604 (2011)
Hatemi-J, A., Irandoust, M.: Asymmetric interaction between government spending and terms of trade volatility: New evidence from hidden cointegration technique. J. Econ. Stud. 39(3), 368–378 (2012)
Hazra, N.C., Rudisill, C., Gulliford, M.C.: Determinants of health care costs in the senior elderly: age, comorbidity, impairment, or proximity to death? Eur. J. Health Econ. 19(6), 831–842 (2018)
Hitiris, T., Posnett, J.: The determinants and effects of health expenditure in developed countries. J. Health Econ. 11(2), 173–181 (1992)
Hua, H., Pan, Y., Yang, X., Wang, S., Shi, Y.: Dynamic relations between Energy carbon footprint and economic growth in ethnic minority autonomous regions China. Energy Proc. 17, 273–278 (2012)
Huddart, K.E., Krahn, H., Krogman, N.T.: Are we counting what counts? A closer look at environmental concern, pro-environmental behaviour, and carbon footprint. Local Environ. 20(2), 220–236 (2015)
Jerrett, M., Eyles, J., Dufournaud, C., Birch, S.: Environmental influences on healthcare expenditures: an exploratory analysis from Ontario, Canada. J. Epidemiol. Commun. Health 57(5), 334–338 (2003)
Johansen, S., Nielsen, M.O.: Likelihood inference for a nonstationary fractional autoregressive model. J. Econ. 158, 51–66 (2010)
Johansen, S., Nielsen, M.O.: Likelihood inference for a fractionally cointegrated vector autoregressive model. Econometrica 80, 2667–2732 (2012)
Knowlton, K., Rotkin-Ellman, M., Geballe, L., Max, W., Solomon, G.M.: Six climate change–related events in the United States accounted for about $14 billion in lost lives and health costs. Health Aff. 30(11), 2167–2176 (2011)
Kumara, A.S., Samaratunge, R.: Patterns and determinants of out-of-pocket health care expenditure in Sri Lanka: evidence from household surveys. Health Policy Plann. 31(8), 970–983 (2016)
Laurent, A., Olsen, S.I., Hauschild, M.Z.: Carbon footprint as environmental performance indicator for the manufacturing industry. CIRP Ann. 59(1), 37–40 (2010)
Lee, K., Cheong, I.: Measuring a carbon footprint and environmental practice: the case of Hyundai Motors Co. (HMC). Ind. Manag. Data Syst. 111(6), 961–978 (2011)
Matthews, H.S., Hendrickson, C.T., Weber, C.L.: The importance of carbon footprint estimation boundaries. Environ Sci Technol. 42(16), 5839–5842 (2008)
Mehrara, M., Sharzei, G., Mohaghegh, M.: The relationship between health expenditure and environmental quality in developing countries. J. Health Admin. 14, 46 (2011)
Mert, M., Çağlar, A.E.: Eviews ve Gauss Uygulamalı Zaman Serileri Analizi [Eviews and Gauss Applied Time Series Analysis], Detay Yayıncılık, Ankara, ISBN: 978-605-254-126-5 (2019)
Murthy, V.N., Okunade, A.A.: Determinants of US health expenditure: evidence from autoregressive distributed lag (ARDL) approach to cointegration. Econ. Model. 59, 67–73 (2016)
Murthy, N.V., Ukpolo, V.: Aggregate health care expenditure in the United States: evidence from cointegration tests. Appl. Econ. 26(8), 797–802 (1994)
Narayan, P.K., Narayan, S.: Does environmental quality influence health expenditures? Empirical evidence from a panel of selected OECD countries. Ecol. Econ. 65(2), 367–374 (2008)
Newhouse, J.P.: Medical-care expenditure: a cross-national survey. J. Hum. Resour. 12(1), 115–125 (1977)
OECD: Health spending (indicator), OECD Health Statistics (database), https://doi.org/10.1787/8643de7e-en. Accessed 30 Nov 2019 (2019)
Phillips, P.C., Perron, P.: Testing for a unit root in time series regression. Biometrika 75(2), 335–346 (1988)
Remoundou, K., Koundouri, P.: Environmental effects on public health: An economic perspective. Int J Environ Res Public Health 6(8), 2160–2178 (2009)
Roberts, J.: Spurious regression problems in the determinants of health care expenditure: A comment on Hitiris (1997). Appl. Econ. Lett. 7(5), 279–283 (2000)
Ruth, M., Coelho, D., Karetnikov, D.: The US economic impacts of climate change and the costs of inaction: A review and assessment by the Center for Integrative Environmental Research (CIER) at the University of Maryland (2007).
Schorderet, Y.: A nonlinear generalization of cointegration: A note on hidden cointegration. Université de Genève/Faculté des sciences économiques et sociales, No 2002.03 (2002)
Shin, Y., Yu, B., Greenwood-Nimmo, M.: Modelling asymmetric cointegration and dynamic multipliers in a nonlinear ARDL framework. In: Sickles, R., Horrace, W. (eds.) Festschrift in Honor of Peter Schmidt. Springer, New York (2014)
Siti Khalijah, Z.: The impact of environmental quality on public health expenditure in Malaysia (Doctoral dissertation, Universiti Utara Malaysia) (2015)
Tsong, C.C., Lee, C.F., Tsai, L.J., Hu, T.C.: The fourier approximation and testing for the null of cointegration. Empiric. Econ. 51(3), 1085–1113 (2016)
Uddin, G.A., Salahuddin, M., Alam, K., Gow, J.: Ecological footprint and real income: panel data evidence from the 27 highest emitting countries. Ecol. Ind. 77, 166–175 (2017)
Wang, Z., Asghar, M.M., Zaidi, S.A.H., Wang, B.: Dynamic linkages among CO2 emissions, health expenditures, and economic growth: empirical evidence from Pakistan. Environ. Sci. Pollut. Res. 26(15), 15285–15299 (2019)
Wiedmann, T., Minx, J.: A definition of 'carbon footprint'. In: C. C. Pertsova, Ecological Economics Research Trends: Chapter 1, pp. 1–11, Nova Science Publishers, Hauppauge NY, USA. https://www.novapublishers.com/catalog/product_info.php?products_id=5999 (2008)
World Health Organization (WHO): Ten threats to global health in 2019, https://www.who.int/vietnam/news/feature-stories/detail/ten-threats-to-global-health-in-2019. Accessed 26 Nov 2019 (2019)
Yahaya, A., Nor, N.M., Habibullah, M.S., Ghani, J.A., Noor, Z.M.: How relevant is environmental quality to per capita health expenditures? Empirical evidence from panel of developing countries. Springer Plus 5(1), 925 (2016)
Yazdi, S., Zahra, T., Nikos, M.: Public healthcare expenditure and environmental quality in Iran. In Recent Advances in Applied Economics. https://www.wseas.us/e-library/conferences/2014/Lisbon/AEBD/AEBD-17.pdf. Accessed 05 Oct 2019 (2014)
Zaidi, S., Saidi, K.: Environmental pollution, health expenditure and economic growth in the Sub-Saharan Africa countries: Panel ARDL approach. Sust. Cities Soc. 41, 833–840 (2018)
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gündüz, M. Healthcare expenditure and carbon footprint in the USA: evidence from hidden cointegration approach. Eur J Health Econ 21, 801–811 (2020). https://doi.org/10.1007/s10198-020-01174-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10198-020-01174-z
Keywords
- Healthcare expenditure
- Carbon footprint
- Carbon emissions
- Environmental quality
- Hidden cointegration
- Crouching error correction